
Granulomatosis with Polyangiitis-Mimicking Advanced Gynecological Cancer: A Case Report and Systematic Review of the Literature

 ,
,
Abstract
1. Introduction
Case Report
2. Materials and Methods
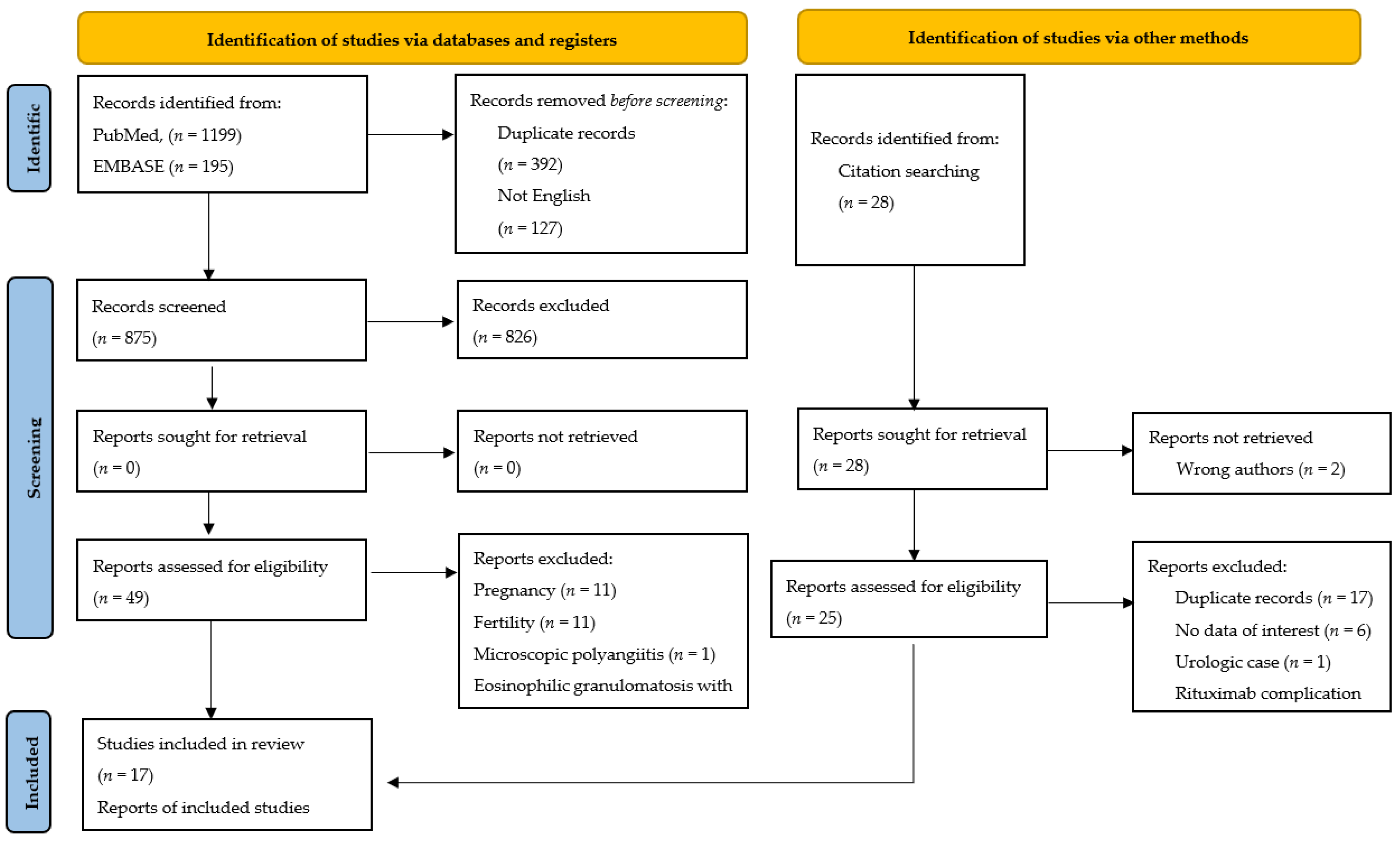
2.1. Search Strategy
2.2. Selection Criteria
2.3. Data Collection and Analysis
2.4. Definitions
3. Results
3.1. Main Findings
3.2. Therapy for GPA
3.3. Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Falk, R.J.; Gross, W.L.; Guillevin, L.; Hoffman, G.S.; Jayne, D.R.; Jennette, J.C.; Kallenberg, C.G.; Luqmani, R.; Mahr, A.D.; Matteson, E.L.; et al. American College of Rheumatology; American Society of Nephrology; European League Against Rheumatism. Granulomatosis with polyangiitis (Wegener’s): An alternative name for Wegener’s granulomatosis. Arthritis Rheum. 2011, 63, 863–864. [Google Scholar] [CrossRef]
- Available online: https://www.orpha.net/consor/cgi-bin/Disease_Search.php?lng=EN&data_id=759&Disease_Disease_Search_diseaseGroup=Wegener&Disease_Disease_Search_diseaseType=Pat&Disease(s)/group%20of%20diseases=Granulomatosis-with-polyangiitis&title=Granulomatosis%20with%20polyangiitis&search=Disease_Search_Simple (accessed on 14 September 2021).
- Hoffman, G.S.; Kerr, G.S.; Leavitt, R.Y.; Hallahan, C.W.; Lebovics, R.S.; Travis, W.D.; Rottem, M.; Fauci, A.S. Wegener granulomatosis: An analysis of 158 patients. Ann. Intern. Med. 1992, 116, 488–498. [Google Scholar] [CrossRef]
- Sowida, M. Granulomatosis polyangiitis. BMJ Case Rep. 2019, 12, e228693. [Google Scholar] [CrossRef] [PubMed]
- Comarmond, C.; Cacoub, P. Granulomatosis with polyangiitis (Wegener): Clinical aspects and treatment. Autoimmun. Rev. 2014, 13, 1121–1125. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 29, 372:n71. [Google Scholar]
- Gran, J.T.; Berner, A.; Kloster-Jensen, A.; Bostad, L. Microscopic polyangiitis diagnosed at hysterectomy. Clin. Exp. Rheumatol. 1999, 17, 611–613. [Google Scholar]
- von Maltzahn, M.; Kinloch, M.; Truchan, M.; Taylor-Gjevre, R.M. Vasculitic adnexal involvement in eosinophilic granulomatosis with polyangiitis (Churg-Strauss angiitis). J. Clin. Rheumatol. 2014, 20, 341–342. [Google Scholar] [CrossRef]
- Sukhdeo, A.; Bertouch, J. Gynecological involvement in eosinophilic granulomatosis with polyangiitis. Int. J. Rheum. Dis. 2016, 19, 932–935. [Google Scholar] [CrossRef]
- Famokunwa, B.; Ockrim, J.; Manson, J.J. Eosinophilic granulomatosis with polyangiitis presenting with a vesicovaginal fistula. Rheumatology 2017, 56, 1080. [Google Scholar] [CrossRef][Green Version]
- Swain, C.A.; Sherry, T.R.; Tyson, N. Childhood-Onset Eosinophilic Granulomatosis with Polyangiitis with a Vulvar Granuloma: A Case Report and Review of the Literature. J. Pediatr. Adolesc. Gynecol. 2019, 32, 425–428. [Google Scholar] [CrossRef]
- Stone, J.H.; Millward, C.L.; Criswell, L.A. Two genitourinary manifestations of Wegener’s granulomatosis. J. Rheumatol. 1997, 24, 1846–1848. [Google Scholar] [PubMed]
- Hendrix, Y.; Wuite-Eversdijk, M.P.; Meijer, J.W.; Kraayenbrink, A.A.; Richter, C. An unusual case of vaginal blood loss. Eur. J. Obstet. Gynecol. Reprod. Biol. 2009, 147, 236–237. [Google Scholar] [CrossRef] [PubMed]
- Oladipo, A.; Sathiyathasan, S.; Thomas, S.; Jeyanthan, K.; Hakeem-Habeeb, Y. An unusual presentation of Wegener disease of the cervix: Presenting as cervical cancer. J. Low. Genit. Tract Dis. 2011, 15, 328–330. [Google Scholar] [CrossRef] [PubMed]
- Nan, S.I.; Li, W.Y.; Xu, C.B.; Song, C.L. Granulomatosis with polyangiitis accompanied by manifestations of ovarian and cervical lesions. Am. J. Med. Sci. 2014, 348, 352–353. [Google Scholar] [CrossRef] [PubMed]
- Caron, F.; Michaud, R.; Gariépy, G.; Bourré-Tessier, J. Involvement of uterine cervix as the first manifestation of granulomatosis with polyangiitis. J. Clin. Rheumatol. 2014, 20, 458–459. [Google Scholar] [CrossRef]
- Campochiaro, C.; Scotti, R.; Margari, S.; Giorgione, V.; Mellone, R.; Mangili, G.; Maschio, A.D.; Tresoldi, M. A case of granulomatosis with polyangiitis: Rheumatoid arthritis overlap syndrome presenting as cervical cancer successfully treated with rituximab. Intern. Med. J. 2016, 46, 745–746. [Google Scholar] [CrossRef]
- Fallahi, M.J.; Shenavandeh, S.; Mokhtari, M.; Sajedianfard, S. Granulomatosis with polyangiitis presenting with pelvic mass leading to total hysterectomy: A case-letter. Jt. Bone Spine 2017, 84, 99–101. [Google Scholar] [CrossRef]
- Soro Marín, S.; Júdez Navarro, E.; Sianes Fernández, M.; Sánchez Nievas, G.; Romero, J.G. An unusual presentation of limited granulomatosis with polyangiitis involving vagina and urethra. Case Rep. Rheumatol. 2017, 2017, 9407675. [Google Scholar] [CrossRef]
- Bielejewska, A.; Bociek, A.; Bociek, M.; Jaroszyński, A. A unique case of ovarian manifestation of systemic vasculitis that mimics ovarian cancer. Sarcoidosis Vasc. Diffus. Lung Dis. 2020, 37, 179–183. [Google Scholar]
- Friedmann, I. the pathology of midline granuloma. Proc. R. Soc Med. 1964, 57, 289–297. [Google Scholar]
- Malamou-Mitsi, V.D.; Pappa, L.S.; Paraskevaidis, E.; Paschopoulos, M.; Drosos, A.A. Uterine cervical involvement in a patient with Wegener’s granulomatosis. Am. J. Med. 2000, 109, 74–75. [Google Scholar] [CrossRef]
- Lewis, F.M. Vulvar involvement in Wegener’s granulomatosis. A case report. J. Reprod. Med. 2002, 47, 725–727. [Google Scholar] [PubMed]
- Ahson, G.Z.; Parkin, D.E.; Gulliford, C.; Ashok, P.W. A rare case of postmenopausal bleeding due to Wegener’s granulomatosis. Acta Obstet. Gynecol. Scand. 2002, 81, 1086–1087. [Google Scholar] [CrossRef] [PubMed]
- Bean, S.M.; Conner, M.G. Wegener’s granulomatosis of the uterine cervix: A case report and review of the literature. Int. J. Gynecol. Pathol. 2007, 26, 95–98. [Google Scholar] [CrossRef] [PubMed]
- Maina, W.C.; Crocker, S.G.; Scott, D.; Ali, A. Postmenopausal bleeding due to cervical involvement with Wegener’s granulomatosis. J. Obstet. Gynaecol. 2009, 29, 167–169. [Google Scholar] [CrossRef]
- Mukherjee, S.; Al-Utayem, W.; Bergin, L.; Bevan, J.R.; Hull, R. Wegener’s granulomatosis presenting as intermenstrual bleeding. J. Obstet. Gynaecol. 2011, 31, 191–192. [Google Scholar] [CrossRef] [PubMed]
- Bastone, P.; Squifflet, J.L.; Marbaix, E.; Houssiau, F. Successful treatment of gynaecological involvement of granulomatosis with polyangiitis (Wegener’s granulomatosis) by rituximab. Clin. Exp. Rheumatol. 2015, 33, S142–S144. [Google Scholar]
- Vikse, J.; Rygh, A.; Kaisen, K.; Omdal, R. Life-threatening rituximab- induced pyoderma gangrenosum successfully treated with intravenous immunoglobulin. Scand. J. Rheumatol. 2017, 46, 413–414. [Google Scholar] [CrossRef]
- Bachmayer, K.; Ludwig, H.; Radaszkiewicz, T. Eine 60jährige Patientin mit Sialadenitis, Lungenrundherden und Ulcus vulvae A 60-year-old patient with sialadenitis, pulmonary round foci and vulvar ulcer. Wien. Klin. Wochenschr. 1984, 96, 289–294. [Google Scholar]
- Miyahara, H.; Sato, T.; Ueda, G.; Okudaira, Y. A case of Wegener’s granulomatosis with cancers of the thyroid gland and the cervix uteri (author’s transl). Nippon. Jibiinkoka Gakkai Kaiho 1976, 79, 1368–1374. [Google Scholar] [CrossRef][Green Version]


{kind=link}
| Authors | Age, yr | Clinical Evolution | Initial Presentation of Symptoms | ORL Symptoms | Lung Findings | Urological Symptoms | Gynecologic Symptoms | Examination Findings | Diagnosis Delay |
|---|---|---|---|---|---|---|---|---|---|
| Stone et al., 1997 [12] | 55 | First symptoms: mild-1970s First consultation: 1982 Diagnosis: 1996 | Saddle nose and upper respiratory tract | Yes | No | No | Vaginal bleeding | Nodular lesions in cervix and vagina | 21 yr |
| Hendrix et al., 2009 [13] | 82 | Four yr-history of symptoms First consultation and diagnosis at the same time after 4 yr | Vaginal blood loss. Cervix then lung | No | Yes | No | Vaginal bleeding and purulent dischage | Cervical necrotizing granulomatous inflammation and vaginal ulcer | 48 mo + |
| Oladipo et al., 2011 [14] | 71 | 1 yr-history of symptoms Diagnosis was made 2 months after vault granuloma excision | Postmenopausal bleeding | No | No | No | Postmenopausal bleeding | Exophytic growth on the cervix with contact bleeding | 12 mo + |
| Nan et al., 2014 [15] | 58 | First symptoms: September 2012 On day 30: GPA suspected On day 37: Diagnosis. | Abnormal vaginal bleeding and compromise of multiple organs and systems | Yes | Yes | Yes | Vaginal bleeding | Partial hysterectomy, 9 yr before. Nodular lesions in cervix and ovarian cysts with purulent spillage | 37 d |
| Caron et al., 2014 [16] | 48 | One yr-history of symptoms First consultation and diagnosis at the same time after 1 yr | Abnormal cervix and ENT | Yes | Yes | No | Bleeding after sexual intercourse | Soft and friable mass that replaced the cervix | 12 mo |
| Campochiaro et al., 2016 [17] | 55 | Two mo-history of symptoms Diagnosis was made two weeks later of initial symptoms | Exophytic cervical lesion then synovitis, purpura, and red papules | No | Yes | Yes | Metrorrhagia | Necrotic cervical mass extending to the lower third vaginal wall. | 2 mo (First work up +) |
| Fallahi et al., 2017 [18] | 33 | Two mo-history of symptoms First consultation: May 2015 Diagnosis was made during admission | Lower abdominal pain, and abnormal uterine bleeding | Yes | Yes | Yes | Abnormal uterine bleeding | Uterine mass and cervical necrotizing vasculitis | 2 mo + |
| Soro et al., 2017 [19] | 62 | Three mo-history of symptoms Diagnosis was made during admission | Vesical tenesmus and vaginal bleeding and low-grade fever | No | No | Yes | Vaginal bleeding | Hysterectomy, BSO 12 yr before. Irregular hardening of anterior vagina encompassing urethra | 3 mo |
| Bielejewska et al., 2020 [20] | 48 | Diagnosis was made during hospitalization | Lumbosacral pain, left hydronephrosis, then nasal ulcer | Yes | No | Yes | Pelvic pain | Necrotizing and granulomatous inflammatory tumour left ovary | No |
| Pereira et al., (present case) | 75 | One-year history of symptoms | Pelvic pain, intermittent hematuria, vaginal bleeding, and pelvic mass | No | No | Yes | Pelvic pain and postmenopausal bleeding | Hysterectomy, BSO 36 yr before. Ulcerative, exophytic vaginal mass with contact bleeding | 12 mo |
| Authors | Age, yr | Clinical Evolution | Initial Presentation of Symptoms | ORL Symptoms | Lung Findings | Urological Symptoms | Gynecologic Symptoms | Examination Findings | Diagnosis Delay |
|---|---|---|---|---|---|---|---|---|---|
| Fridman et al., 1964 [21] | 61 | First consultation: July 1958 Diagnosis: November 1960 First recurrence: September 1961 Second recurrence: 1962 | ENT | Yes | No | No | Gynecological complaint | Uterine cervix and vaginal granuloma | 28 mo (Undisclosed +) |
| Stone et al., 1997 [12] | 67 | First symptoms: 1988 Diagnosis: 1993 Recurrence: 1995 | Nose and lungs | Yes | Yes | Yes | Vaginal discharge | Nodular lesions on the cervix and vaginal wall | 60 mo |
| Malamou-Mitsi et al., 2000 [22] | 45 | Fifteen-year history of GPA Diagnosis of recurrence was made during admission | Unspecified | No | No | No | Vaginal bleeding | Necrotic and easily bleeding ectocervix mass with abnormal vessels | Undisclosed + |
| Lewis et al., 2002 [23] | 54 | The diagnosis was made after 2 wk-history of symptoms. Recurrence 1 yr later | Iritis left eye. Deep ulceration of the heart palate then vulva | Yes | No | No | Vulvar soreness and contact bleeding | Vasculitic lesions on both labia minora | <2 wk |
| Ahson et al., 2002 [24] | 80 | Three-year history of GPA Diagnosis of recurrence was made after 10 mo-history of symptoms | Kidneys, end-stage renal disease | No | No | Yes | Postmenopausal bleeding | Cervical necrosis and contact bleeding | 16 mo + |
| Bean and Conner 2007 [25] | 32 | Past medical history of GPA Diagnosis: 1999 One yr-history of symptoms before recurrence | Sinuses, nose, lungs | Yes | Yes | Yes | Vaginal bleeding | Cervical necrosis andcontact bleeding | 12 mo + |
| Maina et al., 2009 [26] | 64 | Ten-year history of GPA 2004: first recurrence January 2008: Diagnosis of second recurrence was made after 3 wk-history of symptoms: | Ear, eye, and renal involvement | Yes | No | Yes | Postmenopausal bleeding | Highly vascular and irregular cervical mass involving 50% of ectocervix | 3 wk + |
| Mukherjee et al., 2011 [27] | 42 | First consultation: 2003 Diagnosis: 2005 First recurrence: March 2008 Second recurrence: May 2008? persist | ENT and irregular and inflamed cervix | Yes | No | No | Intermenstrual and postcoital bleeding | Large friable vascular area and necrotizing granulomata in cervix | 24 mo (5 yr +) |
| Bastone et al., 2015 [28] | 34 | Diagnosis: March 2008 First recurrence: March 2011 Second recurrence: July 2014 | Skin, joints, sinus | Yes | No | No | Metrorrhagia | Uterine cervix and upper vagina | 19 mo + |
| Authors | Treatment | Outcome | Time | First Recurrence | Interval | Second Recurrence | Interval | Patient Status | Follow-Up |
|---|---|---|---|---|---|---|---|---|---|
| Stone et al., 1997 [12] | No treatment until diagnosis in 1996:
| CR * | 1 mo | - | - | - | - | Alive | 1 mo * |
| Hendrix et al., 2009 [13] | Treatment from diagnosis:
| Fast clinical recovery * | - | - | - | - | - | Alive | - |
| Oladipo et al., 2011 [14] | After 1 yr-history of symptoms
| CR * | 6 mo | - | - | - | - | Alive | 12 mo * |
| Nan et al., 2014 [15] | On day 30:
| The patient fell into a coma and died the following day | 43 d | - | - | - | - | Died Unknown cause | 44 d |
| Caron et al., 2014 [16] | Treatment started without delay:
| CR * | 1 mo | - | - | - | - | Alive | 1 mo * |
| Campochiaro et al., 2016 [17] | After 2-mo history of symptoms:
| CR * | 3 mo | - | - | - | - | Alive | 3 mo * |
| Fallahi et al., 2017 [18] | After first consultation: May 2015.
| PR * | 6 mo | - | - | - | - | Alive | 6 mo * |
| Soro et al., 2017 [19] | After 3 mo-history of symptoms
| Sustained remission * | - | - | - | - | - | Alive | 60 mo |
| Vagino-urethral fistula ** | 2 yr ** | ||||||||
| CR *** | 5 yr *** | ||||||||
| Bielejewska et al., 2020 [20] | Treatment started during first hospitalization:
| Progression of GPA * | Later | - | - | - | - | Alive | 12 mo |
| Improvement without recovering renal function ** | - | ||||||||
| General good condition *** | - | ||||||||
| Kidney transplant | 1 yr | ||||||||
| Pereira et al. (present case) | After 1-year history of symptoms
| CR * | 6 mo | - | - | - | - | Alive | 53 mo |
| Authors | Treatment | Outcome | Time | First Recurrence | Interval | Second Recurrence | Interval | Patient Status | Follow-Up |
|---|---|---|---|---|---|---|---|---|---|
| Fridman et al., 1964 [21] | No treatment until 1962. Treatment since recurrence:
| Dramatic improvement * | - | Turbinate | 10 mo | Cervix-vagina | 18 mo | Died Unknown cause | Treatment: 1 mo * Total:5 yr |
| Stone et al., 1997 [12] | First treatment: 1988
| CR * Well ** CR *** | 16 mo * 13 mo ** 2 wk *** | Vulva Urethra | 24 mo | - | - | Alive | Treatment: 38 mo
|
| Malamou-Mitsi al., 2000 [22] | 15-yr history of GPA treated with cyclophosphamide Treatment since recurrence:
| CR * | 3 mo * | Cervix | 180 mo | - | - | Alive | Treatment: 12 mo Total: 15 yr |
| Lewis et al., 2002 [23] | Diagnosis after <1 mo of initial symptoms
| Resolved * | Rapidly * | Skin | 12 mo | - | - | Alive | Treatment: 12 mo *
|
| Ahson et al., 2002 [24] | Treatment from 1989 until July 2001
| Died 1 day after hysteroscopy | - | Cervix | 36 mo | - | - | Died Unknown cause | Treatment: 12 yr * Total: 12.5 yr |
| Bean and Conner 2007 [25] | Treatment after diagnosis 1999:
| Not provided | - | Cervix-vagina | 84 mo | - | - | Alive | Treatment: Lost * Total: 1 yr |
| Maina et al., 2009 [26] | 10-yr history of GPA treated with methotrexate * Treatment first recurrence: 2004 Treatment second recurrence: 2008
| Not provided* | - | Sclera | 48 mo | Cervix Thraquea | 96 mo | Alive | Treatment: Lost ** Total: 10 yr |
| Mukherjee et al., 2011 [27] | First treatment: January 2006
| Immediate improvement * | 6 mo * | Cervix | 23 mo | Upper airway | 25 mo | Alive | Treatment: 29 mo
|
| Definitive improvement in cervix, but upper airway not controlled ** | 3 mo ** | ||||||||
| Bastone et al., 2015 [28] | Treatment since March 2008
| Promptly achieved * | - | Cervix-vagina | 36 mo | Cervix-vagina | 55 mo | Alive | Treatment: 50 mo
|
| No remission ** | 20 mo ** | ||||||||
| PR *** | 6 mo *** |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pereira, A.; Magrina, J.F.; Magtibay, P.M.; Stamps, B.G.; Muñoz-Nuñez, E.; Perez-Medina, T. Granulomatosis with Polyangiitis-Mimicking Advanced Gynecological Cancer: A Case Report and Systematic Review of the Literature. J. Pers. Med. 2022, 12, 289. https://doi.org/10.3390/jpm12020289
Pereira A, Magrina JF, Magtibay PM, Stamps BG, Muñoz-Nuñez E, Perez-Medina T. Granulomatosis with Polyangiitis-Mimicking Advanced Gynecological Cancer: A Case Report and Systematic Review of the Literature. Journal of Personalized Medicine. 2022; 12(2):289. https://doi.org/10.3390/jpm12020289
Chicago/Turabian StylePereira, Augusto, Javier F. Magrina, Paul M. Magtibay, Beatriz G. Stamps, Elena Muñoz-Nuñez, and Tirso Perez-Medina. 2022. "Granulomatosis with Polyangiitis-Mimicking Advanced Gynecological Cancer: A Case Report and Systematic Review of the Literature" Journal of Personalized Medicine 12, no. 2: 289. https://doi.org/10.3390/jpm12020289
APA StylePereira, A., Magrina, J. F., Magtibay, P. M., Stamps, B. G., Muñoz-Nuñez, E., & Perez-Medina, T. (2022). Granulomatosis with Polyangiitis-Mimicking Advanced Gynecological Cancer: A Case Report and Systematic Review of the Literature. Journal of Personalized Medicine, 12(2), 289. https://doi.org/10.3390/jpm12020289