
Long COVID Syndrome Presenting as Neuropsychiatric Exacerbations in Autism Spectrum Disorder: Insights for Treatment



{kind=link}
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Subjects
2.2. Monocyte Cytokine Profiles
3. Results
3.1. Case Presentation
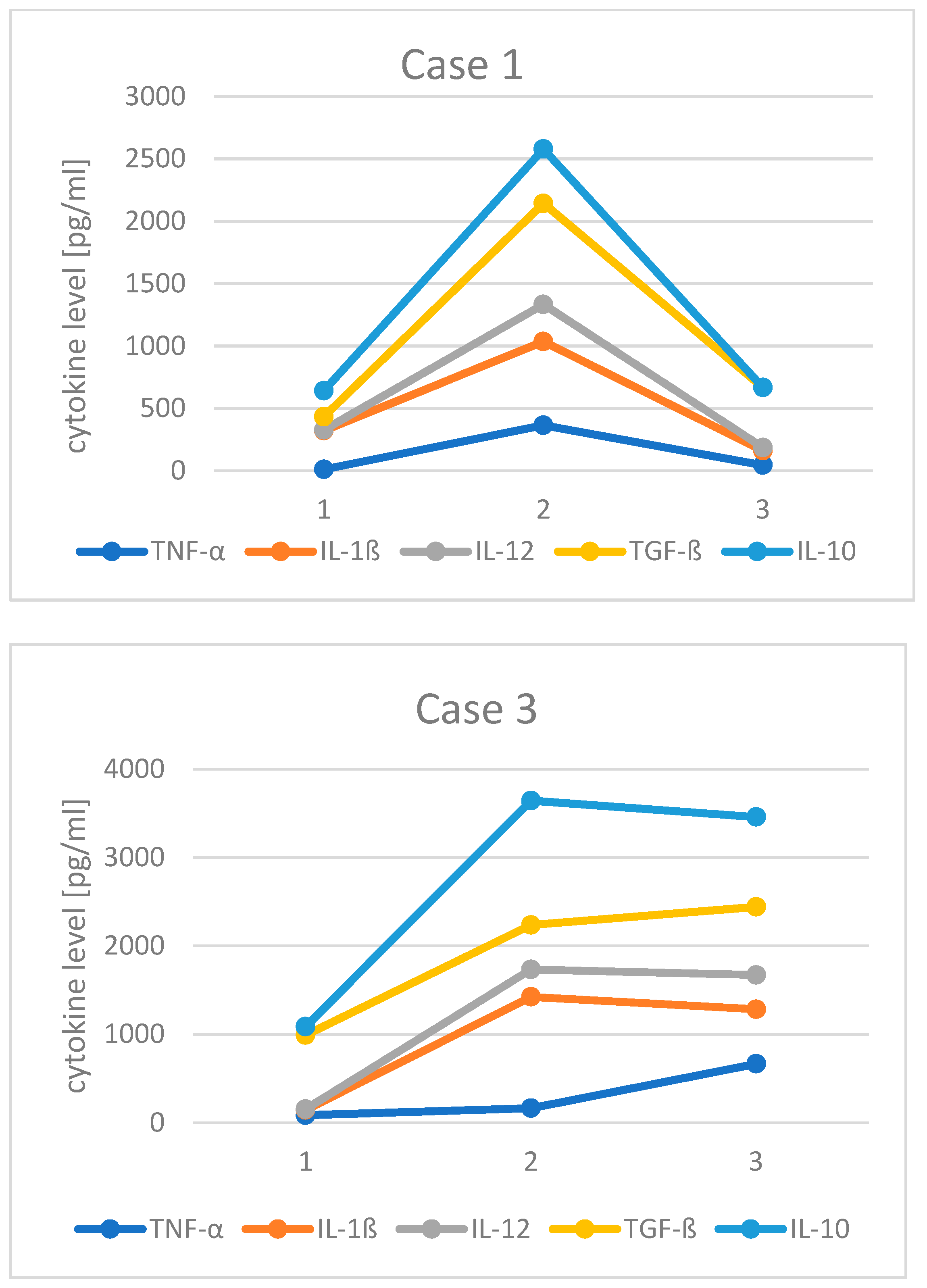
3.2. Changes in Monocyte Cytokine Profile before and after COVID-19
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations Used:
| AE: | autoimmune encephalitis |
| AEDs: | anti-epileptic drugs |
| ASD: | autism spectrum disorders |
| CFS: | chronic fatigue syndrome |
| COVID-19: | coronavirus disease 2019 |
| CRCI: | cancer-therapy-related cognitive impairment |
| CVID: | common variable immunodeficiency |
| IDO: | indoleamine 2,3-dioxygenase |
| Ig: | immunoglobulin |
| IL: | interleukin |
| IVIg: | intravenous immunoglobulin |
| JAK: | Janus kinase |
| LPS: | lipopolysahhcaride |
| mTOR: | mammalian target of rapamycin |
| NSAIDs: | non-steroidal anti-inflammatory drugs |
| OCD: | obsessive compulsive disorder |
| PB Mo: | peripheral blood monocytes |
| QOL: | quality of life |
| SARS-CoV-2: | severe acute respiratory syndrome coronavirus 2 |
| SQ: | subcutaneous |
| SPUH: | Saint Peter’s University Hospital |
| TGF: | transforming growth factor |
| TNF: | tumor necrosis factor |
| WES: | whole exome sequencing |
| WGS: | whole genome sequencing |
References
- Brussow, H. COVID-19 and children: Medical impact and collateral damage. Microb. Biotechnol. 2022, 15, 1035–1049. [Google Scholar] [CrossRef]
- Lunsky, Y.; Jahoda, A.; Navas, P.; Campanella, S.; Havercamp, S.M. The mental health and well-being of adults with intellectual disability during the COVID-19 pandemic: A narrative review. J. Policy Pract. Intellect. Disabil. 2022, 19, 35–47. [Google Scholar] [CrossRef]
- Siberry, V.G.R.; Rowe, P.C. Pediatric long COVID and myalgic encephalomyelitis/chronic fatigue syndrome: Overlaps and opportunities. Pediatr. Infect. Dis. J. 2022, 41, 139–141. [Google Scholar] [CrossRef]
- Soriano, J.B.; Murthy, S.; Marshall, J.C.; Relan, P.; Diaz, J.V. A clinical case definition of post-COVID-19 condition by a Delphi consensus. Lancet Infect. Dis. 2022, 22, 102–107. [Google Scholar] [CrossRef]
- Zimmermann, P.; Pittet, L.F.; Curtis, N. How common is long COVID in children and adolescents? Pediatr. Infect. Dis. J. 2021, 40, 482–487. [Google Scholar] [CrossRef]
- Ludvigsson, J.F. Case report and systematic review suggest that children may experience similar long-term effects to adults after clinical COVID-19. Acta. Paediatr. 2021, 110, 914–921. [Google Scholar] [CrossRef]
- Ceban, F.; Ling, S.; Lui, L.M.W.; Lee, Y.; Gill, H.; Teopiz, K.M.; Rodrigues, N.B.; Subramaniapillai, M.; Vincenzo, J.D.D.; Cao, B.; et al. Fatigue and cognitive impairment in post-COVID-19 Syndrome: A systematic review and meta-analysis. Brain Behav. Immun. 2022, 101, 93–135. [Google Scholar] [CrossRef]
- Nasserie, T.; Hittle, M.; Goodman, S.N. Assessment of the frequency and variety of persistent symptoms among patients with COVID-19: A systematic review. JAMA. Netw. Open. 2021, 4, e2111417. [Google Scholar] [CrossRef]
- Gibson, E.M.; Monje, M. Microglia in cancer therapy-related cognitive impairment. Trends. Neurosci. 2021, 44, 441–451. [Google Scholar] [CrossRef]
- Wong, T.L.; Weitzer, D. Long COVID and myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS)-a systemic review and comparison of clinical presentation and symptomatology. Medicina 2021, 57, 418. [Google Scholar] [CrossRef]
- Gibson, E.M.; Monje, M. Emerging mechanistic underpinnings and therapeutic targets for chemotherapy-related cognitive impairment. Curr. Opin. Oncol. 2019, 31, 531–539. [Google Scholar] [CrossRef]
- Gibson, E.M.; Nagaraja, S.; Ocampo, A.; Tam, L.T.; Wood, L.S.; Pallegar, P.N.; Greene, J.J.; Geraghty, A.C.; Goldstein, A.K.; Ni, L.; et al. Methotrexate chemotherapy induces persistent tri-glial dysregulation that underlies chemotherapy-related cognitive impairment. Cell 2019, 176, 43–55.e13. [Google Scholar] [CrossRef] [PubMed]
- Wen, X.; Ren, J.; Li, X.; Li, J.; Chen, S. Parents’ personality, parenting stress, and problem behaviors of children with special needs in China before and during the COVID-19 pandemic. Curr. Psychol. 2022, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Polónyiová, K.; Rašková, B.; Ostatníková, D. Changes in mental health during three waves of the COVID-19 pandemic in Slovakia: Neurotypical children versus children with autism spectrum disorder and their parents. Int. J. Environ. Res. Public Health. 2022, 19, 11849. [Google Scholar] [CrossRef] [PubMed]
- Rosen, N.E.; Lord, C.; Volkmar, F.R. The diagnosis of autism: From Kanner to DSM-III to DSM-5 and beyond. J. Autism Dev. Disord. 2021, 51, 4253–4270. [Google Scholar] [CrossRef] [PubMed]
- Jyonouchi, H.; Geng, L. Associations between monocyte and T cell cytokine profiles in autism spectrum disorders: Effects of dysregulated innate immune responses on adaptive responses to recall antigens in a subset of ASD children. Int. J. Mol. Sci. 2019, 20, 4731. [Google Scholar] [CrossRef]
- Eom, T.H.; Lee, H.S.; Jang, P.S.; Kim, Y.H. Valproate-induced panhypogammaglobulinemia. Neurol Sci. 2013, 34, 1003–1004. [Google Scholar] [CrossRef]
- Goldstein, H.E.; Hauptman, J.S. The putative role of mTOR inhibitors in non-tuberous sclerosis complex-related epilepsy. Front Neurol. 2021, 12, 639319. [Google Scholar] [CrossRef]
- Steinman, G.; Mankuta, D. Antepartum COVID-19 and postpartum autism. Austin J. Clin. Neurol. 2021, 8, 1149. [Google Scholar]
- Premraj, L.; Kannapadi, N.V.; Briggs, J.; Seal, S.M.; Battaglini, D.; Fanning, J.; Suen, J.; Robba, C.; Fraser, J.; Cho, S.M. Mid and long-term neurological and neuropsychiatric manifestations of post-COVID-19 syndrome: A meta-analysis. J. Neurol Sci. 2022, 434, 120162. [Google Scholar] [CrossRef]
- Savino, R.; Carotenuto, M.; Polito, A.N.; Noia, S.D.; Albenzio, M.; Scarinci, A.; Ambrosi, A.; Sessa, F.; Tartaglia, N.; Messina, G. Analyzing the potential biological determinants of autism spectrum disorder: From neuroinflammation to the kynurenine pathway. Brain. Sci. 2020, 10, 631. [Google Scholar] [CrossRef] [PubMed]
- Komada, M.; Nishimura, Y. Epigenetics and neuroinflammation associated with neurodevelopmental disorders: A microglial perspective. Front Cell Dev. Biol. 2022, 10, 852752. [Google Scholar] [CrossRef] [PubMed]
- Fernandez-Castaneda, A.; Lu, P.; Geraghty, A.C.; Song, E.; Lee, M.H.; Wood, J.; O’Dea, M.R.; Dutton, S.; Shamardani, K.; Nwangwu, K.; et al. Mild respiratory COVID can cause multi-lineage neural cell and myelin dysregulation. Cell 2022, 185, 2452–2468.e16. [Google Scholar] [CrossRef] [PubMed]
- Sefik, E.; Qu, R.; Junqueira, C.; Kaffe, E.; Mirza, H.; Zhao, J.; Brewer, J.R.; Han, A.; Steach, H.R.; Israelow, B.; et al. Inflammasome activation in infected macrophages drives COVID-19 pathology. Nature 2022, 606, 585–593. [Google Scholar] [CrossRef] [PubMed]
- Ryan, F.J.; Hope, C.M.; Masavuli, M.G.; Lynn, M.A.; Mekonnen, Z.A.; Yeow, A.E.L.; Garcia-Valtanen, P.; Al-Delfi, Z.; Gummow, J.; Ferguson, C.; et al. Long-term perturbation of the peripheral immune system months after SARS-CoV-2 infection. BMC Med. 2022, 20, 26. [Google Scholar] [CrossRef]
- Mehandru, S.; Merad, M. Pathological sequelae of long-haul COVID. Nature Immunology. 2022, 23, 194–202. [Google Scholar] [CrossRef]
- Toro-Huamanchumo, C.J.; Benites-Meza, J.K.; Mamani-Garcia, C.S.; Bustamante-Paytan, D.; Garcia-Ramos, A.E.; Diaz-Vélez, C.; Baroza, J.J. Efficacy of colchicine in the treatment of COVID-19 patients: A systematic review and meta-analysis. J. Clin. Med. 2022, 11, 2615. [Google Scholar] [CrossRef]
- Bonaventura, A.; Vecchié, A.; Dagna, L.; Tangianu, F.; Abbate, A.; Dentali, F. Colchicine for COVID-19: Targeting NLRP3 inflammasome to blunt hyperinflammation. Inflamm. Res. 2022, 71, 293–307. [Google Scholar] [CrossRef]
- Mansouri, N.; Marjani, M.; Tabarsi, P.; von Garnier, C.; Mansouri, D. Successful treatment of Covid-19 associated cytokine release syndrome with colchicine. A case report and review of literature. Immunol. Investig. 2021, 50, 884–890. [Google Scholar] [CrossRef]
- Naik, R.R.; Shakya, A.K.; Aladwan, S.M.; Eltanani, M. Kinase inhibitors as potential therapeutic agents in the treatment of COVID-19. Front. Pharmacol. 2022, 13, 806568. [Google Scholar] [CrossRef]
- Chatterjee, B.; Thakur, S.S. Remdesivir and its combination with repurposed drugs as COVID-19 therapeutics. Front. Immunol. 2022, 13, 830990. [Google Scholar] [CrossRef] [PubMed]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jyonouchi, H.; Geng, L.; Rossignol, D.A.; Frye, R.E. Long COVID Syndrome Presenting as Neuropsychiatric Exacerbations in Autism Spectrum Disorder: Insights for Treatment. J. Pers. Med. 2022, 12, 1815. https://doi.org/10.3390/jpm12111815
Jyonouchi H, Geng L, Rossignol DA, Frye RE. Long COVID Syndrome Presenting as Neuropsychiatric Exacerbations in Autism Spectrum Disorder: Insights for Treatment. Journal of Personalized Medicine. 2022; 12(11):1815. https://doi.org/10.3390/jpm12111815
Chicago/Turabian StyleJyonouchi, Harumi, Lee Geng, Daniel A. Rossignol, and Richard E. Frye. 2022. "Long COVID Syndrome Presenting as Neuropsychiatric Exacerbations in Autism Spectrum Disorder: Insights for Treatment" Journal of Personalized Medicine 12, no. 11: 1815. https://doi.org/10.3390/jpm12111815
APA StyleJyonouchi, H., Geng, L., Rossignol, D. A., & Frye, R. E. (2022). Long COVID Syndrome Presenting as Neuropsychiatric Exacerbations in Autism Spectrum Disorder: Insights for Treatment. Journal of Personalized Medicine, 12(11), 1815. https://doi.org/10.3390/jpm12111815