
Early Sensory Profile in Autism Spectrum Disorders Predicts Emotional and Behavioral Issues

 , , , , , , and
, , , , , , and  add
Show full author list
add
Show full author list
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Procedures
2.3. Data Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Johnson-Ecker, C.L.; Parham, L.D. The Evaluation of Sensory Processing: A Validity Study Using Contrasting Groups. Am. J. Occup. Ther. 2000, 54, 494–503. [Google Scholar] [CrossRef]
- Bundy, A.C.; Lane, S.J.; Murray, E.A. (Eds.) Sensory Integration: Theory and Practice, 2nd ed.; F.A. Davis: Philadelphia, PA, USA, 2002. [Google Scholar]
- Kranowitz, C.S. Screening for Sensory Integration Dysfunction. Caught Two, But One Got Away. Child Care Inf. Exch. 1998, 119, 80–83. [Google Scholar]
- Dunn, W. The sensations of everyday life: Empirical, theoretical, and pragmatic considerations. Am. J. Occup. Ther. 2001, 55, 608–620. [Google Scholar] [CrossRef]
- Ornitz, E.M.; Guthrie, D.; Farley, A.H. The early development of autistic children. J. Autism Child. Schizophr. 1977, 7, 207–229. [Google Scholar] [CrossRef]
- Kientz, M.A.; Dunn, W. A Comparison of the Performance of Children with and Without Autism on the Sensory Profile. Am. J. Occup. Ther. 1997, 51, 530–537. [Google Scholar] [CrossRef]
- Ornitz, E.M. Neurophysiologic studies of infantile autism. In Handbook of Autism and Pervasive Developmental Disorders; John Wiley & Sons: Hoboken, NJ, USA, 1987; pp. 148–165. [Google Scholar]
- Talay-Ongan, A.; Wood, K. Unusual Sensory Sensitivities in Autism: A possible crossroads. Int. J. Disabil. Dev. Educ. 2000, 47, 201–212. [Google Scholar] [CrossRef]
- Watling, R.L.; Deitz, J.; White, O. Comparison of Sensory Profile Scores of Young Children with and Without Autism Spectrum Disorders. Am. J. Occup. Ther. 2001, 55, 416–423. [Google Scholar] [CrossRef]
- Baranek, G.T.; David, F.J.; Poe, M.D.; Stone, W.L.; Watson, L.R. Sensory Experiences Questionnaire: Discriminating sensory features in young children with autism, developmental delays, and typical development. J. Child Psychol. Psychiatry 2006, 47, 591–601. [Google Scholar] [CrossRef]
- Tomchek, S.D.; Dunn, W. Sensory Processing in Children with and without Autism: A Comparative Study Using the Short Sensory Profile. Am. J. Occup. Ther. 2007, 61, 190–200. [Google Scholar] [CrossRef]
- Narzisi, A.; Fabbri-Destro, M.; Crifaci, G.; Scatigna, S.; Maugeri, F.; Berloffa, S.; Fantozzi, P.; Prato, A.; Muccio, R.; Valente, E.; et al. Sensory Profiles in School-Aged Children with Autism Spectrum Disorder: A Descriptive Study Using the Sensory Processing Measure-2 (SPM-2). J. Clin. Med. 2022, 11, 1668. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, S.; Waseem, H.; Sadaf, A.; Ashiq, R.; Basit, H.; Rose, S. Daily Living Tasks Affected by Sensory and Motor Problems in Children with Autism Aged 5–12 Years. J. Health Med. Nurs. 2021, 92, 7–12. [Google Scholar] [CrossRef]
- Yela-González, N.; Santamaría-Vázquez, M.; Ortiz-Huerta, J.H. Activities of Daily Living, Playfulness and Sensory Processing in Children with Autism Spectrum Disorder: A Spanish Study. Children 2021, 8, 61. [Google Scholar] [CrossRef] [PubMed]
- Harrison, J.; Hare, D.J. Brief Report: Assessment of Sensory Abnormalities in People with Autistic Spectrum Disorders. J. Autism Dev. Disord. 2004, 34, 727–730. [Google Scholar] [CrossRef] [PubMed]
- Rogers, S.J. Neuropsychology of autism in young children and its implications for early intervention. Ment. Retard. Dev. Disabil. Res. Rev. 1998, 4, 104–112. [Google Scholar] [CrossRef]
- Baranek, G.T. Efficacy of Sensory and Motor Interventions for Children with Autism. J. Autism Dev. Disord. 2002, 32, 397–422. [Google Scholar] [CrossRef] [PubMed]
- Ben-Sasson, A.; Cermak, S.A.; Orsmond, G.I.; Tager-Flusberg, H.; Kadlec, M.B.; Carter, A.S. Sensory clusters of toddlers with autism spectrum disorders: Differences in affective symptoms. J. Child Psychol. Psychiatry 2008, 49, 817–825. [Google Scholar] [CrossRef] [PubMed]
- Ermer, J.; Dunn, W. The Sensory Profile: A Discriminant Analysis of Children with and Without Disabilities. Am. J. Occup. Ther. 1998, 52, 283–290. [Google Scholar] [CrossRef]
- Rogers, S.J.; Hepburn, S.; Wehner, E. Parent Reports of Sensory Symptoms in Toddlers with Autism and Those with Other Developmental Disorders. J. Autism Dev. Disord. 2003, 33, 631–642. [Google Scholar] [CrossRef] [PubMed]
- Lord, C. Follow-up of two-year-olds referred for possible autism. J. Child Psychol. Psychiatry 1995, 36, 1365–1382. [Google Scholar] [CrossRef]
- Stone, W.L.; Hogan, K.L. A structured parent interview for identifying young children with autism. J. Autism Dev. Disord. 1993, 23, 639–652. [Google Scholar] [CrossRef] [PubMed]
- Baranek, G.T.; Foster, L.G.; Berkson, G. Tactile Defensiveness and Stereotyped Behaviors. Am. J. Occup. Ther. 1997, 51, 91–95. [Google Scholar] [CrossRef] [PubMed]
- Nelson, D.L. Children with Autism and Other Pervasive Disorders of Development and Behavior: Therapy Through Activities; SLACK Inc.: Thorofare, NJ, USA, 1984. [Google Scholar]
- Paluszny, M. Therapy of psychic trauma resulting from attempted filicide. Psychother. Theory Res. Pract. 1979, 16, 107–115. [Google Scholar] [CrossRef]
- Green, S.A.; Ben-Sasson, A. Anxiety disorders and sensory over-responsivity in children with autism spectrum disorders: Is there a causal relationship? J. Autism Dev. Disord. 2010, 40, 1495–1504. [Google Scholar] [PubMed]
- Wigham, S.; Rodgers, J.; South, M.; McConachie, H.; Freeston, M. The Interplay Between Sensory Processing Abnormalities, Intolerance of Uncertainty, Anxiety and Restricted and Repetitive Behaviours in Autism Spectrum Disorder. J. Autism Dev. Disord. 2015, 45, 943–952. [Google Scholar] [CrossRef]
- Palser, E.R.; Fotopoulou, A.; Pellicano, E.; Kilner, J.M. The link between interoceptive processing and anxiety in children diagnosed with autism spectrum disorder: Extending adult findings into a developmental sample. Biol. Psychol. 2018, 136, 13–21. [Google Scholar] [CrossRef]
- Baranek, G.T.; Wakeford, L.; David, F.J. Understanding, Assessing and Treating Sensory-Motor Issues. In Autism Spectrum Disorders in Infants and Toddlers: Diagnosis, Assessment and Treatment; Guilford Press: New York, NY, USA, 2010; pp. 104–140. [Google Scholar]
- Dunn, K.; Rydzewska, E.; Fleming, M.; Cooper, S.-A. Prevalence of mental health conditions, sensory impairments and physical disability in people with co-occurring intellectual disabilities and autism compared with other people: A cross-sectional total population study in Scotland. BMJ Open 2020, 10, e035280. [Google Scholar] [CrossRef]
- Ecker, C.; Marquand, A.; Mourão-Miranda, J.; Johnston, P.; Daly, E.M.; Brammer, M.J.; Maltezos, S.; Murphy, C.M.; Robertson, D.; Williams, S.; et al. Describing the Brain in Autism in Five Dimensions--Magnetic Resonance Imaging-Assisted Diagnosis of Autism Spectrum Disorder Using a Multiparameter Classification Approach. J. Neurosci. 2010, 30, 10612–10623. [Google Scholar] [CrossRef]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders: DSM-5, 5th ed.; American Psychiatric Publishing Inc.: Arlington, VA, USA, 2013. [Google Scholar]
- Lord, C.; Rutter, M.; DiLavore, P.C.; Risi, S.; Gotham, K.; Bishop, S. Autism Diagnostic Observation Schedule 2; Western Psychological Services: Torrance, CA, USA, 2012. [Google Scholar]
- Schopler, E.; Reichler, R.J.; Renner, B.R. The Childhood Autism Rating Scale (CARS): For Diagnostic Screening and Classification of Autism; Irvington: New York, NY, USA, 1986. [Google Scholar]
- Rutter, M.; Le Couteur, A.; Lord, C. Autism Diagnostic Interview-Revised; Western Psychological Services: Los Angeles, CA, USA, 2003; Volume 29, p. 30. [Google Scholar]
- Miller Kuhaneck, H.; Ecker, C.; Parham, L.D.; Henry, D.A.; Glennon, T.J. Sensory Processing Measure—Preschool (SPM-P): Manual; Western Psychological Services: Los Angeles, CA, USA, 2010. [Google Scholar]
- Achenbach, T.M.; Rescorla, L.A. Manual for the ASEBA Preschool Forms and Profiles; University of Vermont, Research Center for Children, Youth & Families: Burlington, VT, USA, 2000; Volume 30. [Google Scholar]
- Frigerio, E.; Burt, D.M.; Gagliardi, C.; Cioffi, G.; Martelli, S.; Perrett, D.I.; Borgatti, R. Is everybody always my friend? Perception of approachability in Williams syndrome. Neuropsychologia 2006, 44, 254–259. [Google Scholar] [CrossRef]
- Kern, J.K.; Garver, C.R.; Carmody, T.; Andrews, A.A.; Mehta, J.A.; Trivedi, M.H. Examining sensory modulation in individuals with autism as compared to community controls. Res. Autism Spectr. Disord. 2008, 2, 85–94. [Google Scholar] [CrossRef]
- Crane, L.; Goddard, L.; Pring, L. Sensory processing and coping in adults with autism spectrum disorder. Autism 2009, 13, 215–218. [Google Scholar] [CrossRef]
- Cheung, P.P.; Siu, A.M.H. A comparison of patterns of sensory processing in children with and without developmental disabilities. Res. Dev. Disabil. 2009, 30, 1468–1480. [Google Scholar] [CrossRef] [PubMed]
- Balasco, L.; Provenzano, G.; Bozzi, Y. Sensory Abnormalities in Autism Spectrum Disorders: A Focus on the Tactile Domain, From Genetic Mouse Models to the Clinic. Front. Psychiatry 2020, 10, 1016. [Google Scholar] [CrossRef]
- Will, E.A.; Daunhauer, L.A.; Fidler, D.J.; Raitano Lee, N.; Rosenberg, C.R.; Hepburn, S.L. Sensory Processing and Maladaptive Behavior: Profiles Within the Down Syndrome Phenotype. Phys. Occup. Ther. Pediatr. 2019, 39, 461–476. [Google Scholar] [CrossRef]
- Georgiou, N.; Spanoudis, G. Developmental Language Disorder and Autism: Commonalities and Differences on Language. Brain Sci. 2021, 11, 589. [Google Scholar] [CrossRef] [PubMed]
- Bishop, D.V.M. Uncommon Understanding: Development and Disorders of Language Comprehension in Children; Psychology Press: Hove, UK, 1997; p. 278. [Google Scholar]
- Norbury, C.F.; Vamvakas, G.; Gooch, D.; Baird, G.; Charman, T.; Simonoff, E.; Pickles, A. Language growth in children with heterogeneous language disorders: A population study. J. Child Psychol. Psychiatry 2017, 58, 1092–1105. [Google Scholar] [CrossRef] [PubMed]
- Gizzonio, V.; Bazzini, M.C.; Marsella, C.; Papangelo, P.; Rizzolatti, G.; Fabbri-Destro, M. Supporting preschoolers’ cognitive development: Short-and mid-term effects of fluid reasoning, visuospatial, and motor training. Child Dev. 2022, 93, 134–149. [Google Scholar] [CrossRef]
- Piccardi, E.S.; Begum Ali, J.; Jones, E.J.; Mason, L.; Charman, T.; Johnson, M.H.; Gliga, T. Behavioural and neural markers of tactile sensory processing in infants at elevated likelihood of autism spectrum disorder and/or attention deficit hyperactivity disorder. J. Neurodev. Disord. 2021, 13, 1. [Google Scholar] [CrossRef]
- Cascio, C.; McGlone, F.; Folger, S.; Tannan, V.; Baranek, G.; Pelphrey, K.A.; Essick, G. Tactile Perception in Adults with Autism: A Multidimensional Psychophysical Study. J. Autism Dev. Disord. 2008, 38, 127–137. [Google Scholar] [CrossRef]
- Mailloux, Z.; Mulligan, S.; Roley, S.S.; Blanche, E.; Cermak, S.; Coleman, G.G.; Bodison, S.; Lane, C.J. Verification and Clarification of Patterns of Sensory Integrative Dysfunction. Am. J. Occup. Ther. 2011, 65, 143–151. [Google Scholar] [CrossRef]
- Tomchek, S.D.; Huebner, R.A.; Dunn, W. Patterns of sensory processing in children with an autism spectrum disorder. Res. Autism Spectr. Disord. 2014, 8, 1214–1224. [Google Scholar] [CrossRef]
- Hess, E.B. DIR®/Floortime™: Evidence based practice towards the treatment of autism and sensory processing disorder in children and adolescents. Int. J. Child Health Hum. Dev. 2013, 6, 267–274. [Google Scholar]
- Ayres, A.J. Sensory Integration and the Child; Western Psychological Services: Los Angeles, NV, USA, 1979. [Google Scholar]
- Fulceri, F.; Grossi, E.; Contaldo, A.; Narzisi, A.; Apicella, F.; Parrini, I.; Tancredi, R.; Calderoni, S.; Muratori, F. Motor Skills as Moderators of Core Symptoms in Autism Spectrum Disorders: Preliminary Data from an Exploratory Analysis with Artificial Neural Networks. Front Psychol. 2019, 9, 2683. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
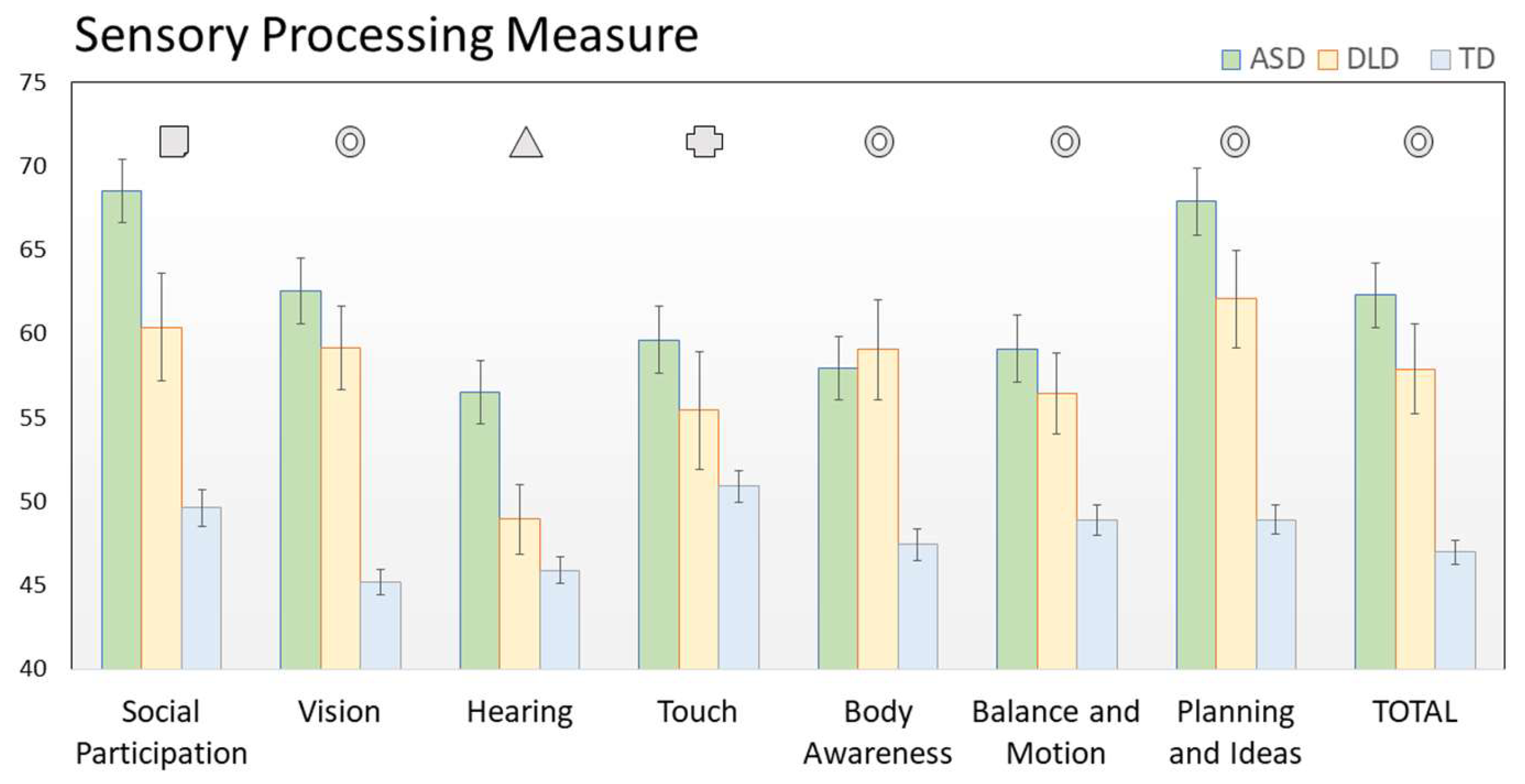
| SPM Subscale | ASD | DLD | TD | ASD vs. TD | ASD vs. DLD | DLD vs. TD |
|---|---|---|---|---|---|---|
| Social Participation | 68.55 | 60.39 | 49.64 | p< 0.001 | p =0.024 | p <0.001 |
| Vision | 62.57 | 59.17 | 45.23 | p <0.001 | p = 0.617 | p <0.001 |
| Hearing | 56.52 | 48.94 | 45.91 | p <0.001 | p =0.011 | p = 0.663 |
| Touch | 59.64 | 55.44 | 50.91 | p <0.001 | p = 0.518 | p = 0.378 |
| Body Awareness | 57.95 | 59.06 | 47.43 | p <0.001 | p = 1.000 | p <0.001 |
| Balance and Motion | 59.12 | 56.44 | 48.93 | p< 0.001 | p = 1.000 | p =0.019 |
| Planning And Ideas | 67.91 | 62.11 | 48.93 | p <0.001 | p = 0.140 | p <0.001 |
| Total | 62.31 | 57.89 | 46.98 | p <0.001 | p = 0.307 | p< 0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fabbri-Destro, M.; Maugeri, F.; Ianni, C.; Corsini, S.; Di Stefano, E.; Scatigna, S.; Crifaci, G.; Bruzzi, G.; Berloffa, S.; Fantozzi, P.; et al. Early Sensory Profile in Autism Spectrum Disorders Predicts Emotional and Behavioral Issues. J. Pers. Med. 2022, 12, 1593. https://doi.org/10.3390/jpm12101593
Fabbri-Destro M, Maugeri F, Ianni C, Corsini S, Di Stefano E, Scatigna S, Crifaci G, Bruzzi G, Berloffa S, Fantozzi P, et al. Early Sensory Profile in Autism Spectrum Disorders Predicts Emotional and Behavioral Issues. Journal of Personalized Medicine. 2022; 12(10):1593. https://doi.org/10.3390/jpm12101593
Chicago/Turabian StyleFabbri-Destro, Maddalena, Federica Maugeri, Carolina Ianni, Sofia Corsini, Erica Di Stefano, Stefano Scatigna, Giulia Crifaci, Gianina Bruzzi, Stefano Berloffa, Pamela Fantozzi, and et al. 2022. "Early Sensory Profile in Autism Spectrum Disorders Predicts Emotional and Behavioral Issues" Journal of Personalized Medicine 12, no. 10: 1593. https://doi.org/10.3390/jpm12101593
APA StyleFabbri-Destro, M., Maugeri, F., Ianni, C., Corsini, S., Di Stefano, E., Scatigna, S., Crifaci, G., Bruzzi, G., Berloffa, S., Fantozzi, P., Prato, A., Muccio, R., Valente, E., Pelagatti, S., Pecchini, E., Zulli, F., Rizzo, R., Milone, A., Viglione, V., ... Narzisi, A. (2022). Early Sensory Profile in Autism Spectrum Disorders Predicts Emotional and Behavioral Issues. Journal of Personalized Medicine, 12(10), 1593. https://doi.org/10.3390/jpm12101593