Cardiopulmonary Exercise Testing in Childhood in Late Preterms: Comparison to Early Preterms and Term-Born Controls

 , , ,
, , ,
Abstract
1. Introduction
2. Methods
2.1. Design
2.2. Subjects
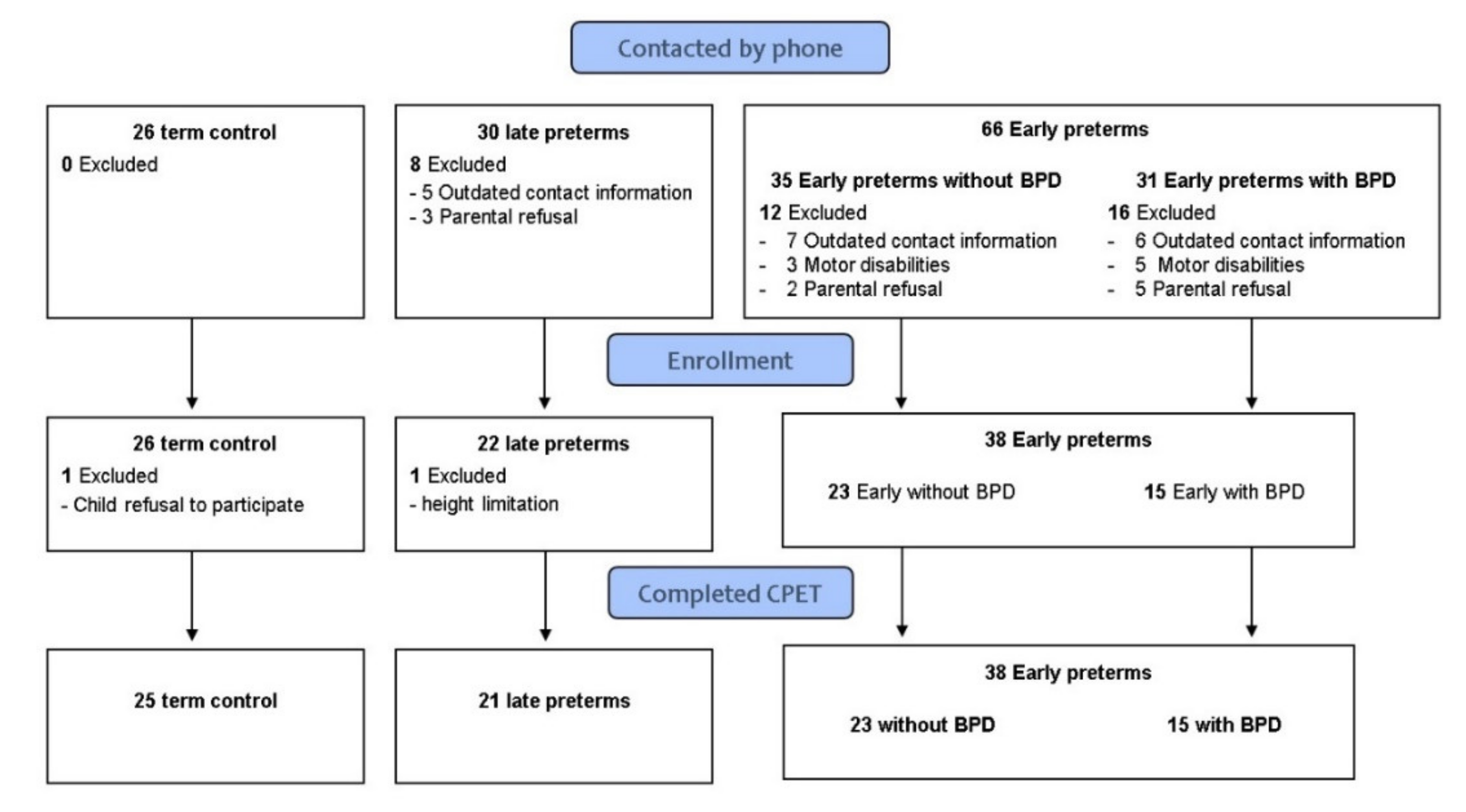
2.3. Participants’ Recruitment
2.4. Data Collection and Cardio-Pulmonary-Exercise-Testing (CPET)
2.4.1. Anthropometric and Disease Measures
2.4.2. Spirometry
2.4.3. Exercise Testing with CPET
2.5. Statistical Analysis
3. Results
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| EP | Early preterm |
| TC | Term healthy |
| LP | Late preterm |
| FEV1 | Forced expiratory volume in one second |
| CPET | Cardiopulmonary exercise test |
| V̇O2 | Oxygen uptake |
| BPD | Bronchopulmonary dysplasia |
| PFT | Pulmonary function tests |
References
- Blencowe, H.; Cousens, S.; Oestergaard, M.Z.; Chou, D.; Moller, A.-B.; Narwal, R.; Adler, A.; Vera Garcia, C.; Rohde, S.; Say, L.; et al. National, Regional, and Worldwide Estimates of Preterm Birth Rates in the Year 2010 with Time Trends since 1990 for Selected Countries: A Systematic Analysis and Implications. Lancet 2012, 379, 2162–2172. [Google Scholar] [CrossRef]
- Karnati, S.; Kollikonda, S.; Abu-Shaweesh, J. Late Preterm Infants—Changing Trends and Continuing Challenges. Int. J. Pediatr. Adolesc. Med. 2020, 7, 36–44. [Google Scholar] [CrossRef]
- Howson, C.P.; Kinney, M.V.; McDougall, L.; Lawn, J.E. Born Too Soon: Preterm Birth Matters. Reprod. Health 2013, 10, S1. [Google Scholar] [CrossRef]
- Manar, M.H.; Brown, M.R.; Gauthier, T.W.; Brown, L.A.S. Association of Glutathione-S-Transferase-P1 (GST-P1) Polymorphisms with Bronchopulmonary Dysplasia. J. Perinatol. 2004, 24, 30–35. [Google Scholar] [CrossRef]
- Teune, M.J.; Bakhuizen, S.; Bannerman, C.G.; Opmeer, B.C.; Van Kaam, A.H.; Van Wassenaer, A.G.; Morris, J.M.; Mol, B.W.J. A Systematic Review of Severe Morbidity in Infants Born Late Preterm. Am. J. Obstet. Gynecol. 2011, 205, 374.e1–374.e9. [Google Scholar] [CrossRef]
- Engle, W.A.; Tomashek, K.M.; Wallman, C.; Stark, A.R.; Adamkin, D.H.; Batton, D.G.; Bell, E.F.; Bhutani, V.K.; Denson, S.E.; Martin, G.I.; et al. “Late-Preterm” Infants: A Population at Risk. Pediatrics 2007, 120, 1390–1401. [Google Scholar] [CrossRef]
- Duke, J.W.; Lovering, A.T. Respiratory and Cardiopulmonary Limitations to Aerobic Exercise Capacity in Adults Born Preterm. J. Appl. Physiol. (1985) 2020, 129, 718–724. [Google Scholar] [CrossRef]
- Kugelman, A.; Colin, A.A. Late Preterm Infants: Near Term but Still in a Critical Developmental Time Period. Pediatrics 2013, 132, 741–751. [Google Scholar] [CrossRef]
- McEvoy, C.; Venigalla, S.; Schilling, D.; Clay, N.; Spitale, P.; Nguyen, T. Respiratory Function in Healthy Late Preterm Infants Delivered at 33–36 Weeks of Gestation. J. Pediatr. 2013, 162, 464–469. [Google Scholar] [CrossRef][Green Version]
- Kotecha, S.J.; Watkins, W.J.; Paranjothy, S.; Dunstan, F.D.; Henderson, A.J.; Kotecha, S. Effect of Late Preterm Birth on Longitudinal Lung Spirometry in School Age Children and Adolescents. Thorax 2012, 67, 54–61. [Google Scholar] [CrossRef]
- Yaacoby-Bianu, K.; Plonsky, M.T.; Gur, M.; Bar-Yoseph, R.; Kugelman, A.; Bentur, L. Effect of Late Preterm Birth on Lung Clearance Index and Respiratory Physiology in School-Age Children. Pediatr. Pulmonol. 2019, 54, 1250–1256. [Google Scholar] [CrossRef] [PubMed]
- Engan, M.; Engeseth, M.S.; Fevang, S.; Vollsæter, M.; Eide, G.E.; Røksund, O.D.; Halvorsen, T.; Clemm, H. Predicting Physical Activity in a National Cohort of Children Born Extremely Preterm. Early Hum. Dev. 2020, 145, 105037. [Google Scholar] [CrossRef]
- Burns, Y.R.; Danks, M.; O’Callaghan, M.J.; Gray, P.H.; Cooper, D.; Poulsen, L.; Watter, P. Motor Coordination Difficulties and Physical Fitness of Extremely-Low-Birthweight Children. Dev. Med. Child. Neurol. 2009, 51, 136–142. [Google Scholar] [CrossRef]
- Rogers, M.; Fay, T.B.; Whitfield, M.F.; Tomlinson, J.; Grunau, R.E. Aerobic Capacity, Strength, Flexibility, and Activity Level in Unimpaired Extremely Low Birth Weight (≤800 g) Survivors at 17 Years of Age Compared with Term-Born Control Subjects. Pediatrics 2005, 116, e58–e65. [Google Scholar] [CrossRef]
- Welsh, L.; Kirkby, J.; Lum, S.; Odendaal, D.; Marlow, N.; Derrick, G.; Stocks, J. The EPICure Study: Maximal Exercise and Physical Activity in School Children Born Extremely Preterm. Thorax 2010, 65, 165–172. [Google Scholar] [CrossRef] [PubMed]
- Vrijlandt, E.J.L.E.; Gerritsen, J.; Boezen, H.M.; Grevink, R.G.; Duiverman, E.J. Lung Function and Exercise Capacity in Young Adults Born Prematurely. Am. J. Respir. Crit. Care Med. 2006, 173, 890–896. [Google Scholar] [CrossRef]
- Haraldsdottir, K.; Watson, A.M.; Beshish, A.G.; Pegelow, D.F.; Palta, M.; Tetri, L.H.; Brix, M.D.; Centanni, R.M.; Goss, K.N.; Eldridge, M.W. Heart Rate Recovery after Maximal Exercise Is Impaired in Healthy Young Adults Born Preterm. Eur. J. Appl. Physiol. 2019, 119, 857–866. [Google Scholar] [CrossRef]
- MacLean, J.E.; DeHaan, K.; Fuhr, D.; Hariharan, S.; Kamstra, B.; Hendson, L.; Adatia, I.; Majaesic, C.; Lovering, A.T.; Thompson, R.B.; et al. Altered Breathing Mechanics and Ventilatory Response during Exercise in Children Born Extremely Preterm. Thorax 2016, 71, 1012–1019. [Google Scholar] [CrossRef]
- Landry, J.S.; Chan, T.; Lands, L.; Menzies, D. Long-Term Impact of Bronchopulmonary Dysplasia on Pulmonary Function. Can. Respir. J. 2011, 18, 265–270. [Google Scholar] [CrossRef]
- Mitchell, S.H.; Teague, W.G.; Robinson, A. Reduced Gas Transfer at Rest and during Exercise in School-Age Survivors of Bronchopulmonary Dysplasia. Am. J. Respir. Crit. Care Med. 1998, 157, 1406–1412. [Google Scholar] [CrossRef]
- Tikanmäki, M.; Tammelin, T.; Sipola-Leppänen, M.; Kaseva, N.; Matinolli, H.-M.; Miettola, S.; Eriksson, J.G.; Järvelin, M.-R.; Vääräsmäki, M.; Kajantie, E. Physical Fitness in Young Adults Born Preterm. Pediatrics 2016, 137, e20151289. [Google Scholar] [CrossRef]
- Jensen, E.A.; Dysart, K.; Gantz, M.G.; McDonald, S.; Bamat, N.A.; Keszler, M.; Kirpalani, H.; Laughon, M.M.; Poindexter, B.B.; Duncan, A.F.; et al. The Diagnosis of Bronchopulmonary Dysplasia in Very Preterm Infants. An Evidence-Based Approach. Am. J. Respir. Crit. Care Med. 2019, 200, 751–759. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention (CDC) about Child & Teen BMI. Available online: https://www.cdc.gov/healthyweight/assessing/bmi/childrens_bmi/about_childrens_bmi.html (accessed on 6 August 2022).
- Imms, C. Review of the Children’s Assessment of Participation and Enjoyment and the Preferences for Activity of Children. Phys. Occup. Ther. Pediatr. 2008, 28, 389–404. [Google Scholar] [CrossRef] [PubMed]
- Miller, M.R. Standardisation of Spirometry. Eur. Respir. J. 2005, 26, 319–338. [Google Scholar] [CrossRef]
- Quanjer, P.H.; Borsboom, G.J.J.M.; Brunekreef, B.; Zach, M.; Forche, G.; Cotes, J.E.; Sanchis, J.; Paoletti, P. Spirometric Reference Values for White European Children and Adolescents: Polgar Revisited. Pediatr. Pulmonol. 1995, 19, 135–142. [Google Scholar] [CrossRef] [PubMed]
- Weisman, I.M.; Marciniuk, D.; Martinez, F.J.; Testing Measurements Frank Sciurba, E.; Sue, D.; Myers Bruce Johnson, J.; Whipp, B.; Zeballos, J.; Beck, K.; Mahler, D.; et al. ATS/ACCP Statement on Cardiopulmonary Exercise Testing. Am. J. Respir. Crit. Care Med. 2003, 167, 211–277. [Google Scholar] [CrossRef]
- Cooper, D.M.; Weiler-Ravell, D.; Whipp, B.J.; Wasserman, K. Aerobic Parameters of Exercise as a Function of Body Size during Growth in Children. J. Appl. Physiol. Respir. Environ. Exerc. Physiol. 1984, 56, 628–634. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, H.; Monahan, K.D.; Seals, D.R. Age-Predicted Maximal Heart Rate Revisited. J. Am. Coll Cardiol. 2001, 37, 153–156. [Google Scholar] [CrossRef]
- Rowland, T.; Hagenbuch, S.; Pober, D.; Garrison, A. Exercise Tolerance and Thermoregulatory Responses during Cycling in Boys and Men. Med. Sci. Sports Exerc. 2008, 40, 282–287. [Google Scholar] [CrossRef] [PubMed]
- Wasserman, K.; Hansen, J.E.; Sue, D.Y.; Stringer, W.W.; Sietsema, K.E.; Sun, X.G.; Brian, J. Whipp. Principles of Exercise Testing and Interpretation, 5th ed.; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2012. [Google Scholar]
- Svedenkrans, J.; Henckel, E.; Kowalski, J.; Norman, M.; Bohlin, K. Long-Term Impact of Preterm Birth on Exercise Capacity in Healthy Young Men: A National Population-Based Cohort Study. PLoS ONE 2013, 8, e80869. [Google Scholar] [CrossRef]
- Tikanmäki, M.; Kaseva, N.; Tammelin, T.; Sipola-Leppänen, M.; Matinolli, H.M.; Eriksson, J.G.; Järvelin, M.R.; Vääräsmäki, M.; Kajantie, E. Leisure Time Physical Activity in Young Adults Born Preterm. J. Pediatrics 2017, 189, 135–142.e2. [Google Scholar] [CrossRef] [PubMed]
- Tamai, K.; Matsumoto, N.; Takeuchi, A.; Nakamura, M.; Nakamura, K.; Kageyama, M.; Washio, Y.; Tsukahara, H.; Yorifuji, T. Sports Participation and Preterm Birth: A Nationwide Birth Cohort in Japan. Pediatr. Res. 2021, 1–8. [Google Scholar] [CrossRef]
- Lowe, J.; Cousins, M.; Kotecha, S.J.; Kotecha, S. Physical Activity Outcomes Following Preterm Birth. Paediatr. Respir. Rev. 2017, 22, 76–82. [Google Scholar] [CrossRef]
- Clemm, H.; Røksund, O.; Thorsen, E.; Eide, G.E.; Markestad, T.; Halvorsen, T. Aerobic Capacity and Exercise Performance in Young People Born Extremely Preterm. Pediatrics 2012, 129, e97–e105. [Google Scholar] [CrossRef]
- Priante, E.; Moschino, L.; Mardegan, V.; Manzoni, P.; Salvadori, S.; Baraldi, E. Respiratory Outcome after Preterm Birth: A Long and Difficult Journey. Am. J. Perinatol. 2016, 33, 1040–1042. [Google Scholar] [CrossRef]
- Kotecha, S.J.; Edwards, M.O.; Watkins, W.J.; Henderson, A.J.; Paranjothy, S.; Dunstan, F.D.; Kotecha, S. Effect of Preterm Birth on Later FEV 1: A Systematic Review and Meta-Analysis. Thorax 2013, 68, 760–766. [Google Scholar] [CrossRef]
- Edwards, M.O.; Kotecha, S.J.; Lowe, J.; Watkins, W.J.; Henderson, A.J.; Kotecha, S. Effect of Preterm Birth on Exercise Capacity: A Systematic Review and Meta-Analysis. Pediatr. Pulmonol. 2015, 50, 293–301. [Google Scholar] [CrossRef]
- Kaplan, E.; Bar-Yishay, E.; Prais, D.; Klinger, G.; Mei-Zahav, M.; Mussaffi, H.; Steuer, G.; Hananya, S.; Matyashuk, Y.; Gabarra, N.; et al. Encouraging Pulmonary Outcome for Surviving, Neurologically Intact, Extremely Premature Infants in the Postsurfactant Era. Chest 2012, 142, 725–733. [Google Scholar] [CrossRef]
- Amitai, N.; Stafler, P.; Blau, H.; Kaplan, E.; Mussaffi, H.; Levine, H.; Steuer, G.; Bar-Yishay, E.; Klinger, G.; Mei-Zahav, M.; et al. Palivizumab Following Extremely Premature Birth Does Not Affect Pulmonary Outcomes in Adolescence. Chest 2020, 158, 660–669. [Google Scholar] [CrossRef]
- Vrijlandt, E.J.L.E.; Reijneveld, S.A.; Aris-Meijer, J.L.; Bos, A.F. Respiratory Health in Adolescents Born Moderately-Late Preterm in a Community-Based Cohort. J. Pediatr. 2018, 203, 429–436. [Google Scholar] [CrossRef]
- Crump, C.; Winkleby, M.A.; Sundquist, J.; Sundquist, K. Risk of Asthma in Young Adults Who Were Born Preterm: A Swedish National Cohort Study. Pediatrics 2011, 127, e913–e920. [Google Scholar] [CrossRef] [PubMed]
- Flahault, A.; Oliveira Fernandes, R.; De Meulemeester, J.; Ravizzoni Dartora, D.; Cloutier, A.; Gyger, G.; El-Jalbout, R.; Bigras, J.-L.; Luu, T.M.; Nuyt, A.M. Arterial Structure and Stiffness Are Altered in Young Adults Born Preterm. Arterioscler. Thromb. Vasc. Biol. 2020, 40, 2548–2556. [Google Scholar] [CrossRef] [PubMed]
- Lewandowski, A.J.; Bradlow, W.M.; Augustine, D.; Davis, E.F.; Francis, J.; Singhal, A.; Lucas, A.; Neubauer, S.; McCormick, K.; Leeson, P. Right Ventricular Systolic Dysfunction in Young Adults Born Preterm. Circulation 2013, 128, 713–720. [Google Scholar] [CrossRef] [PubMed]
- Dissanayake, H.U.; McMullan, R.L.; Kong, Y.; Caterson, I.D.; Celermajer, D.S.; Phang, M.; Raynes-Greenow, C.; Polson, J.W.; Gordon, A.; Skilton, M.R. Cardiac and Vascular Health in Late Preterm Infants. J. Dev. Orig. Health Dis. 2021, 13, 128–134. [Google Scholar] [CrossRef] [PubMed]
- Karvonen, R.; Sipola, M.; Kiviniemi, A.; Tikanmäki, M.; Järvelin, M.-R.; Eriksson, J.G.; Tulppo, M.; Vääräsmäki, M.; Kajantie, E. Cardiac Autonomic Function in Adults Born Preterm. J. Pediatr 2019, 208, 96–103.e4. [Google Scholar] [CrossRef]
- Yang, J.; Epton, M.J.; Harris, S.L.; Horwood, J.; Kingsford, R.A.; Troughton, R.; Greer, C.; Darlow, B.A. Reduced Exercise Capacity in Adults Born Very Low Birth Weight: A Population-Based Cohort Study. Am. J. Respir. Crit. Care Med. 2021, 205, 88–98. [Google Scholar] [CrossRef]
- Robič Pikel, T.; Starc, G.; Strel, J.; Kovač, M.; Babnik, J.; Golja, P. Impact of Prematurity on Exercise Capacity and Agility of Children and Youth Aged 8 to 18. Early Hum. Dev. 2017, 110, 39–45. [Google Scholar] [CrossRef]
- Vrselja, A.; Pillow, J.J.; Black, M.J. Effect of Preterm Birth on Cardiac and Cardiomyocyte Growth and the Consequences of Antenatal and Postnatal Glucocorticoid Treatment. J. Clin. Med. 2021, 10, 3896. [Google Scholar] [CrossRef]


{kind=link}
| GA = 34–36.6 Weeks (Late Preterm) n = 21 1 | GA ≤ 30 Weeks (Early Preterm) n = 38 2 | Healthy Control Born at Term n = 25 3 | p-Value * | |
|---|---|---|---|---|
| Age (years) | 9.94 ± 0.87 | 9.63 ± 1.20 | 8.84 ± 0.93 | p2 < 0.001 p 3 = 0.014 |
| Male (%) | 12 (57%) | 19 (50%) | 13 (52%) | p = 0.87 |
| Gestational Age (weeks) | 34.9 ± 1.05 | 28.44 ± 1.5 | 39.5 ± 1.4 | p1,2,3 < 0.0001 |
| Birth Weight (gr) | 2373 ± 473 | 1105 ± 280 | 3315 ± 469 | p1,2,3 < 0.0001 |
| Oxygen Supplementation (days) median 25–75 | 0 [0–1] | 38 [8.5–67.50] | 0 [0–0] | p1,3 < 0.001 |
| Ventilation (days) median (25–75 quartile) | 0 [0–0] | 6 [3–30] | 0 [0–0] | p1,3 < 0.001 |
| Height (cm) | 137.4 ± 7.7 | 134.6 ± 9.7 | 133.3 ± 6.5 | p = 0.25 |
| Weight (kg) | 32.6 ± 6.4 | 33.2 ± 12.9 | 30.9 ± 7.6 | p = 0.66 |
| BMI | 17.1 ± 2.2 | 17.9 ± 4.5 | 17.2 ± 2.8 | p = 0.62 |
| BMI percentiles | 49.5 ± 29.3 | 53.7 ± 32.7 | 55.5 ± 31.5 | p = 0.81 |
| BMI z score median (25–75) | 0.12 [(−0.84)–(0.73)] | 0.11 [(−0.81)–(0.93)] | 0.28 [(−0.55)–(1.09)] | p = 0.75 |
| FEV1 (L/s) | 1.73 ± 0.38 | 1.57 ± 0.38 | 1.65 ± 0.32 | p = 0.28 |
| FEV1 (% predicted) | 87.5 ± 16.9 | 82.9 ± 14.6 | 91.04 ± 11.7 | p = 0.095 |
| FVC (L) | 2.02 ± 0.4 | 1.87 ± 0.42 | 1.89 ± 0.37 | p = 0.17 |
| FVC (% predicted) | 94.09 ± 13.6 | 88.9 ± 13.04 | 95.5 ± 11.6 | p = 0.11 |
| GA = 34–36.6 Weeks (Late Preterm) n = 21 1 | GA ≤ 30 Weeks (Early Preterm) n = 38 2 | Healthy Control Born at Term n = 25 3 | p-Value * | |
|---|---|---|---|---|
| PeakV̇O2 Absolute (mL/min) | 1206 ± 248 | 1146 ± 348 | 1380 ± 260 | p2 = 0.02 p 3 = 0.014 |
| PeakV̇O2 Specific (mL/kg/min) | 37.6 ± 6.8 | 36.4 ± 11.4 | 45.2 ± 7.4 | p 2 = 0.038 p 3 = 0.002 |
| PeakV̇O2 (%Pred) | 90.2 ± 15.1 | 90.08 ± 23.19 | 112.4 ± 16.9 | p 2,3 < 0.001 |
| Peak HR (bpm) | 193.4 ± 7 | 190.08 ± 10.65 | 191.8 ± 9.8 | p = 0.46 |
| Peak HR (%pred) | 96.1 ± 3.9 | 94.4 ± 5.39 | 95.0 ± 5.0 | p = 0.44 |
| V̇E/V̇CO2 Slope | 34.4 ± 5.6 | 35.91 ± 6.36 | 34.4 ± 4.3 | p = 0.52 |
| Peak O2 pulse (%pred) | 94.1 ± 15.4 | 95.5 ± 23.01 | 118.8 ± 19.1 | p 2,3 < 0.001 |
| Peak O2 pulse (V̇O2/HR) | 6.2 ± 1.1 | 6.0 ± 1.71 | 7.2 ± 1.4 | p 2 = 0.031 p 3 = 0.008 |
| Sat. O2 Pre | 98.7 ± 1.05 | 99.03 ± 0.91 | 99.1 ± 1.0 | p = 0.40 |
| Sat. O2 Post | 98.5 ± 1.4 | 98.71 ± 1.31 | 99.1 ± 1.1 | p = 0.27 |
| Peak V̇E (L/min) | 48.8 ± 12.4 | 42.4 ± 11.78 | 47.5 ± 9.3 | p = 0.076 |
| BR (L) | 20.4 ± 11.0 | 19.77 ± 13.38 | 20.6 ± 12.0 | p = 0.97 |
| BR (%) | 28.7 ± 13.5 | 30.18 ± 17.61 | 29.3 ± 12.9 | p = 0.94 |
| Breathing limitation Low Normal | 9 (43%) 12 (57%) | 11 (29%) 27 (71%) | 3 (12%) 21 (88%) | p 2 = 0.02 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hochwald, O.; Bentur, L.; Haddad, Y.; Hanna, M.; Zucker-Toledano, M.; Mainzer, G.; Haddad, J.; Gur, M.; Borenstein-Levin, L.; Kugelman, A.; et al. Cardiopulmonary Exercise Testing in Childhood in Late Preterms: Comparison to Early Preterms and Term-Born Controls. J. Pers. Med. 2022, 12, 1547. https://doi.org/10.3390/jpm12101547
Hochwald O, Bentur L, Haddad Y, Hanna M, Zucker-Toledano M, Mainzer G, Haddad J, Gur M, Borenstein-Levin L, Kugelman A, et al. Cardiopulmonary Exercise Testing in Childhood in Late Preterms: Comparison to Early Preterms and Term-Born Controls. Journal of Personalized Medicine. 2022; 12(10):1547. https://doi.org/10.3390/jpm12101547
Chicago/Turabian StyleHochwald, Ori, Lea Bentur, Yara Haddad, Moneera Hanna, Merav Zucker-Toledano, Gur Mainzer, Julie Haddad, Michal Gur, Liron Borenstein-Levin, Amir Kugelman, and et al. 2022. "Cardiopulmonary Exercise Testing in Childhood in Late Preterms: Comparison to Early Preterms and Term-Born Controls" Journal of Personalized Medicine 12, no. 10: 1547. https://doi.org/10.3390/jpm12101547
APA StyleHochwald, O., Bentur, L., Haddad, Y., Hanna, M., Zucker-Toledano, M., Mainzer, G., Haddad, J., Gur, M., Borenstein-Levin, L., Kugelman, A., & Bar-Yoseph, R. (2022). Cardiopulmonary Exercise Testing in Childhood in Late Preterms: Comparison to Early Preterms and Term-Born Controls. Journal of Personalized Medicine, 12(10), 1547. https://doi.org/10.3390/jpm12101547