
Cell-Free DNA Screening for Sex Chromosome Abnormalities and Pregnancy Outcomes, 2018–2020: A Retrospective Analysis

Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
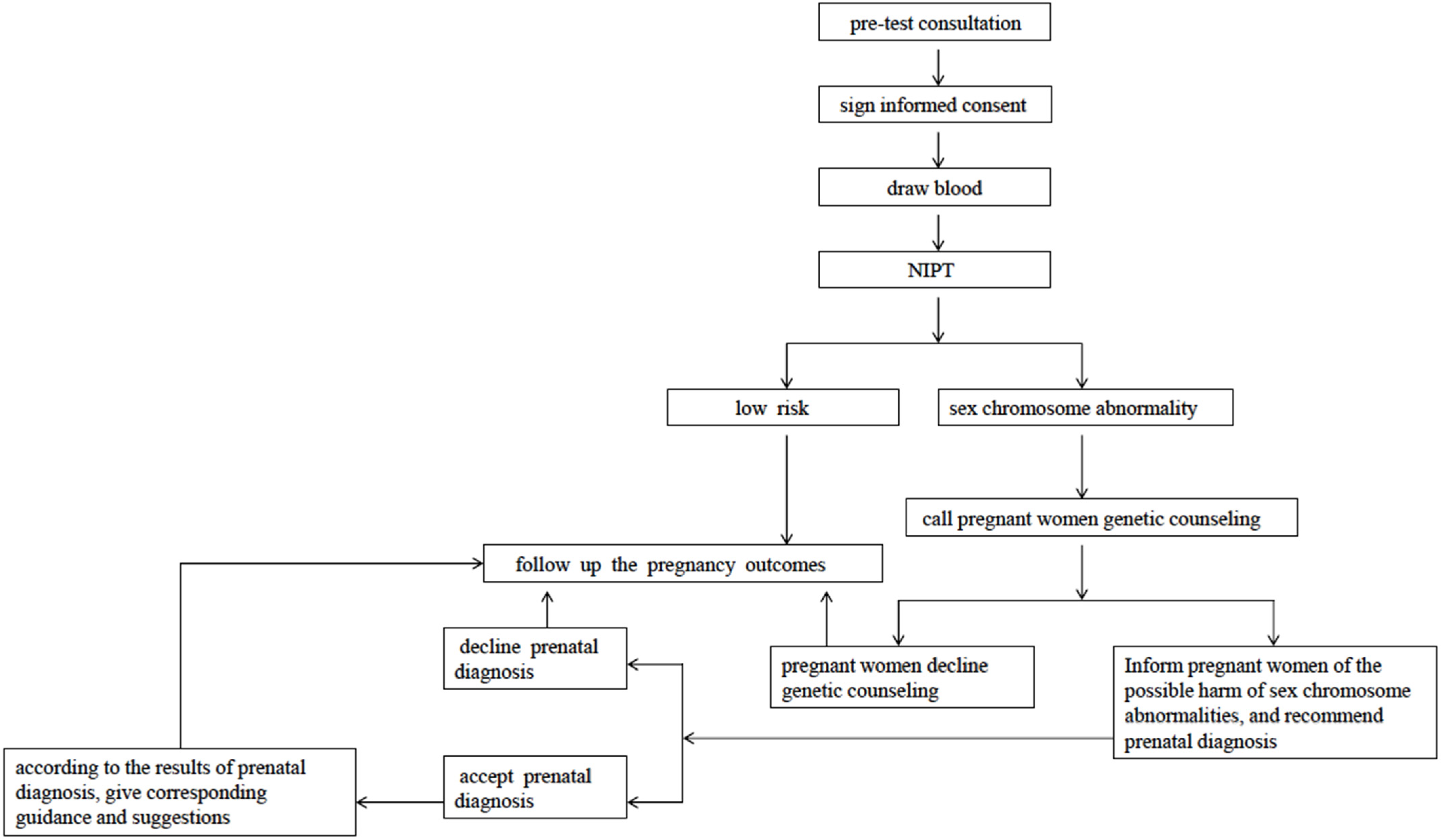
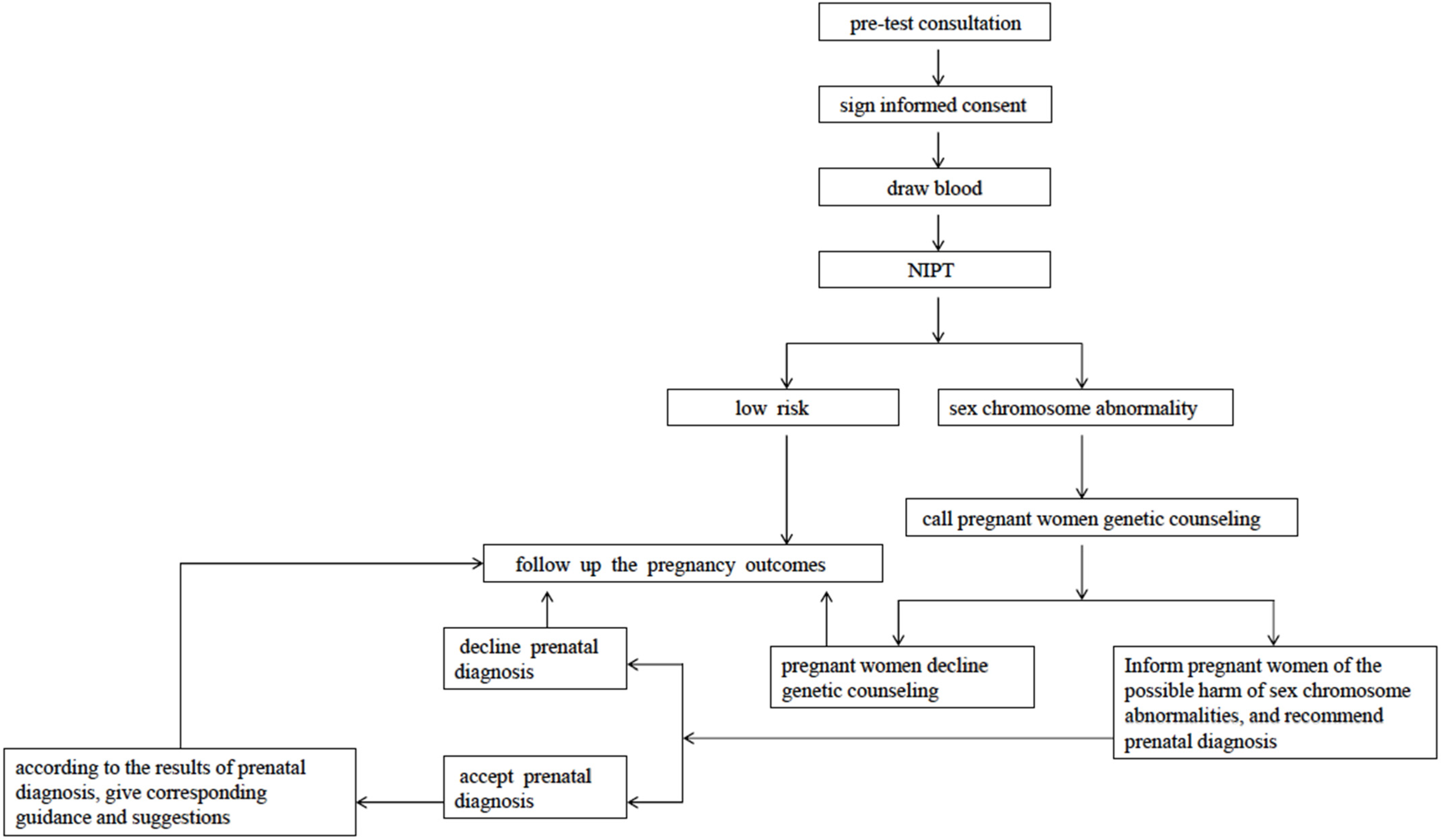
2.2. Methods
2.3. Experimental Methods
3. Results
3.1. NIPT, Prenatal Diagnosis Results, and Follow-Ups
3.2. Accuracy of NIPT in the Screening of Fetal Sex Chromosome Abnormalities
3.3. Comparison between Increased and Decreased Aneuploidy Groups Detected by NIPT
3.4. Comparison between True-Positive and False-Positive Cases, Number of Births, and TOP in the Cases of Sex Chromosome Aneuploidy Detected by NIPT
3.5. Pairwise Comparison between True-Positive and False-Positive Cases and between the Number of Births and TOP in the Cases of Sex Chromosome Aneuploidy Detected by NIPT
3.6. Mosaic Karyotype of Sex Chromosome Abnormalities
3.7. Changes in the Detection Rate of Sex Chromosome Abnormalities in Our Hospital after NIPT Was Performed
4. Discussion
4.1. Main Findings
4.2. Strengths and Limitations
4.3. Interpretation
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bianchi, D.W.; Wilkins-Haug, L. Integration of noninvasive DNA testing for aneuploidy into prenatal care: What has happened since the rubber met the road? Clin. Chem. 2014, 60, 78–87. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koumbaris, G.; Kypri, E.; Tsangaras, K.; Achilleos, A.; Mina, P.; Neofytou, M.; Velissariou, V.; Christopoulou, G.; Kallikas, I.; Gonzalez-Linan, A.; et al. Cell-Free DNA Analysis of Targeted Genomic Regions in Maternal Plasma for Non-Invasive Prenatal Testing of Trisomy 21, Trisomy 18, Trisomy 13, and Fetal Sex. Clin. Chem. 2016, 62, 848–855. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ellison, C.K.; Sun, Y.; Hogg, G.; Fox, J.; Tao, H.; McCarthy, E.; Sagoe, B.; Azab, M.A.; Mazloom, A.R.; Tynan, J.; et al. Using Targeted Sequencing of Paralogous Sequences for Noninvasive Detection of Selected Fetal Aneuploidies. Clin. Chem. 2016, 62, 1621–1629. [Google Scholar] [CrossRef]
- Xu, L.; Huang, H.; Lin, N.; Wang, Y.; He, D.; Zhang, M.; Chen, M.; Chen, L.; Lin, Y. Non-invasive cell-free fetal DNA testing for aneuploidy: Multicenter study of 31 515 singleton pregnancies in southeastern China. Ultrasound Obstet. Gynecol. 2020, 55, 242–247. [Google Scholar] [CrossRef]
- Skotko, B.G.; Allyse, M.A.; Bajaj, K.; Best, R.G.; Klugman, S.; Leach, M.; Meredith, S.; Michie, M.; Stoll, K.; Gregg, A.R. Adherence of cell-free DNA noninvasive prenatal screens to ACMG recommendations. Genet. Med. 2019, 21, 2285–2292. [Google Scholar] [CrossRef] [PubMed]
- Liang, D.; Cram, D.S.; Tan, H.; Linpeng, S.; Liu, Y.; Sun, H.; Zhang, Y.; Tian, F.; Zhu, H.; Xu, M.; et al. Clinical utility of noninvasive prenatal screening for expanded chromosome disease syndromes. Genet. Med. 2019, 21, 1998–2006. [Google Scholar] [CrossRef]
- Sund, K.L.; Khattar, D.; Boomer, T.; Caldwell, S.; Dyer, L.; Hopkin, R.J.; Smolarek, T.A. Confirmatory testing illustrates additional risks for structural sex chromosome abnormalities in fetuses with a non-invasive prenatal screen positive for monosomy X. Am. J. Med. Genet. C Semin. Med. Genet. 2020, 184, 294–301. [Google Scholar] [CrossRef] [PubMed]
- Lalatta, F.; Tint, G.S. Counseling parents before prenatal diagnosis: Do we need to say more about the sex chromosome aneuploidies? Am. J. Med. Genet. A 2013, 161A, 2873–2879. [Google Scholar] [CrossRef] [PubMed]
- Hens, K. Chromosome Screening Using Noninvasive Prenatal Testing Beyond Trisomy-21: What to Screen for and Why It Matters. J. Med. Philos. 2018, 43, 8–21. [Google Scholar] [CrossRef] [PubMed]
- Benn, P. Expanding non-invasive prenatal testing beyond chromosomes 21, 18, 13, X and Y. Clin. Genet. 2016, 90, 477–485. [Google Scholar] [CrossRef] [PubMed]
- Petersen, A.K.; Cheung, S.W.; Smith, J.L.; Bi, W.; Ward, P.A.; Peacock, S.; Braxton, A.; Van Den Veyver, I.B.; Breman, A.M. Positive predictive value estimates for cell-free noninvasive prenatal screening from data of a large referral genetic diagnostic laboratory. Am. J. Obstet. Gynecol. 2017, 217, 691.e1–691.e6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, B.; Lu, B.Y.; Yu, B.; Zheng, F.X.; Zhou, Q.; Chen, Y.P.; Zhang, X.Q. Noninvasive prenatal screening for fetal common sex chromosome aneuploidies from maternal blood. J. Int. Med. Res. 2017, 45, 621–630. [Google Scholar] [CrossRef]
- Cheung, S.W.; Patel, A.; Leung, T.Y. Accurate description of DNA-based noninvasive prenatal screening. N. Engl. J. Med. 2015, 372, 1675–1677. [Google Scholar] [CrossRef] [PubMed]
- Song, J.P.; Jiang, Y.F.; Gao, T.X.; Yao, Y.Y.; Liu, L.J.; Xu, R.H.; Yi, M.Q.; Yu, C.J.; Wang, W.P.; Li, H. Performance of non-invasive prenatal screening for sex chromosome aneuploidies and parental decision-making. Chin. Med. J. 2020, 133, 1617–1619. [Google Scholar] [CrossRef] [PubMed]
- Xu, Y.; Chen, L.; Liu, Y.; Hao, Y.; Xu, Z.; Deng, L.; Xie, J. Screening, prenatal diagnosis, and prenatal decision for sex chromosome aneuploidy. Expert Rev. Mol. Diagn. 2019, 19, 537–542. [Google Scholar] [CrossRef] [PubMed]
- Jeppesen, L.D.; Hatt, L.; Singh, R.; Schelde, P.; Andreasen, L.; Markholt, S.; Lildballe, D.L.; Vogel, I. Screening for Fetal Aneuploidy and Sex Chromosomal Anomalies in a Pregnant Woman with Mosaicism for Turner Syndrome-Applications and Advantages of Cell-Based NIPT. Front. Genet. 2021, 12, 741752. [Google Scholar] [CrossRef] [PubMed]
- Lin, A.E.; Santoro, S.; High, F.A.; Goldenberg, P.; Gutmark-Little, I. Congenital heart defects associated with aneuploidy syndromes: New insights into familiar associations. Am. J. Med. Genet. C Semin. Med. Genet. 2020, 184, 53–63. [Google Scholar] [CrossRef] [PubMed]
- Ataman, E.; Cogulu, O.; Durmaz, A.; Karaca, E.; Durmaz, B.; Akin, H.; Ozkinay, F. The rate of sex chromosome aneuploidies in prenatal diagnosis and subsequent decisions in Western Turkey. Genet. Test. Mol. Biomark. 2012, 16, 150–153. [Google Scholar] [CrossRef]
- Nishiyama, M.; Sekizawa, A.; Ogawa, K.; Sawai, H.; Nakamura, H.; Samura, O.; Suzumori, N.; Nakayama, S.; Yamada, T.; Ogawa, M.; et al. Factors affecting parental decisions to terminate pregnancy in the presence of chromosome abnormalities: A Japanese multicenter study. Prenat. Diagn. 2016, 36, 1121–1126. [Google Scholar] [CrossRef]
- So, P.L.; Cheng, K.Y.Y.; Cheuk, K.Y.; Chiu, W.K.; Mak, S.L.; Mok, S.L.; Lo, T.K.; Yung, W.K.; Lo, F.M.; Chung, H.Y.B.; et al. Parental decisions following prenatal diagnosis of sex chromosome aneuploidy in Hong Kong. J. Obstet. Gynaecol. Res. 2017, 43, 1821–1829. [Google Scholar] [CrossRef]
- Green, T.; Flash, S.; Reiss, A.L. Sex differences in psychiatric disorders: What we can learn from sex chromosome aneuploidies. Neuropsychopharmacology 2019, 44, 9–21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mennuti, M.T.; Chandrasekaran, S.; Khalek, N.; Dugoff, L. Cell-free DNA screening and sex chromosome aneuploidies. Prenat. Diagn. 2015, 35, 980–985. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Linden, M.G.; Bender, B.G.; Robinson, A. Intrauterine diagnosis of sex chromosome aneuploidy. Obstet. Gynecol. 1996, 87, 468–475. [Google Scholar] [CrossRef]
- Berglund, A.; Stochholm, K.; Gravholt, C.H. Morbidity in 47,XYY syndrome: A nationwide epidemiological study of hospital diagnoses and medication use. Genet. Med. 2020, 22, 1542–1551. [Google Scholar] [CrossRef] [PubMed]
- Brady, P.; Brison, N.; Van Den Bogaert, K.; de Ravel, T.; Peeters, H.; Van Esch, H.; Devriendt, K.; Legius, E.; Vermeesch, J.R. Clinical implementation of NIPT—Technical and biological challenges. Clin. Genet. 2016, 89, 523–530. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Charactristics | Cases (n) | Percentage (%) |
|---|---|---|
| Maternal age (years old) | ||
| <35 | 566 | 88.58 |
| ≥35 | 73 | 11.42 |
| BMI (kg/m2) | ||
| <18.5 | 56 | 8.76 |
| 18.5–23.9 | 408 | 63.85 |
| 24–27.9 | 148 | 23.16 |
| ≥28 | 27 | 4.23 |
| Gestational age (Weeks) | ||
| 9–13 | 29 | 4.54 |
| 13 +1—14 +6 | 19 | 2.97 |
| 15–20 | 544 | 85.13 |
| ≥20 +1 | 47 | 7.36 |
| Number of fetus | ||
| Singleton | 639 | 100 |
| Twins | 0 | 0 |
| History of adverse pregnancy and childbirth | ||
| Yes | 146 | 22.85 |
| No | 493 | 77.15 |
| Method of conception | ||
| Natural conception | 622 | 97.34 |
| Assisted reproduction | 17 | 2.66 |
| Mid term Down’s serological screening results | ||
| AFP-MoM | ||
| <0.7 | 72 | 11.27 |
| 0.7–2.5 | 507 | 79.34 |
| >2.5 | 4 | 0.63 |
| HCG-MoM | ||
| <0.5 | 48 | 7.51 |
| 0.5–2.0 | 437 | 68.39 |
| >2.0 | 98 | 15.34 |
| High risk (cut-off: T21 > 1/270, T18 > 1/270) | T21:59/T18:4 | T21:9.23/T18:0.63 |
| Medium risk (cut-off: T21:1/270-1/1000, T18:1/300-1/1000) | T21:87/T18:15 | T21:13.62/T18:2.35 |
| Low risk (cut-off: T21 < 1/270, T18 < 1/300) | T21:437/T18:564 | T21:68.39/T18:88.26 |
| Not performed | 56 | 8.76 |
| Types of Sex Chromosome Abnormalities | NIPT (n) | Prenatal Diagnosis (n) | With Karyotype Analysis Results | PPV | Pregnancy Outcomes | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| Accepted (n) | Refused (n) | Accordance (n) | Discordance (n) | Followed-Up (n) | Births (n) | TOP (n) | Loss to Follow-Up (n) | |||
| 45, X | 255 | 204 | 46 | 37 | 167 | 18.14% | 250 | 213 | 38 | 4 |
| 47, XXX | 75 | 63 | 12 | 37 | 26 | 58.73% | 75 | 58 | 17 | 0 |
| 47, XXY | 158 | 137 | 21 | 110 | 26 | 80.29% | 158 | 57 | 101 | 0 |
| 47, XYY | 74 | 59 | 15 | 42 | 17 | 71.19% | 74 | 63 | 11 | 0 |
| X(increased)-M | 45 | 33 | 12 | 2 | 31 | 6.06% | 45 | 44 | 1 | 0 |
| X(decreased)-M | 28 | 19 | 9 | 0 | 19 | 0 | 28 | 27 | 1 | 0 |
| Other complex for X | 2 | 2 | 0 | 0 | 2 | 0 | 2 | 2 | 0 | 0 |
| Del/Dup(X/Y) | 2 | 1 | 1 | 1 | 1 | 50.00% | 2 | 1 | 0 | 1 |
| Total | 639 | 518 | 116 | 229 | 289 | 44.21% | 634 | 465 | 169 | 5 |
| Karyotype Results | NIPT | Maternal Age(Years Old) | Gestational Age (Weeks *) | BMI (kg/m2) | Number of Fetus | IVF (Yes/No) | History of Adverse Pregnancy and Childbirth | Abnormal Serological Screening Results | Follow Up |
|---|---|---|---|---|---|---|---|---|---|
| 46, X, der(X) t(X; Y)(q23; q11.2) | XXY | 27 | 19 +1 | 23.74 | Singleton | No | — | — | TOP |
| 46, X,i(X)(q10) | XO | 30 | 17 +5 | 18.73 | Singleton | No | — | Mid pregnancy: HCG-MoM:0.32 | TOP |
| 46, XYqh-(Y = 22) | XYY | 31 | 19 +3 | 25.91 | Singleton | No | — | Mid pregnancy:HCG-MoM:3.00, T21:1/531 | Male, no obvious abnormality in birth appearance |
| 46, Xi(Y) (p10) | XO | 28 | 13 +6 | 17.78 | Singleton | No | — | Mid pregnancy: HCG-MoM:0.43 | TOP |
| 46, X, del(X) q(21.3) | XO | 32 | 17 +1 | 22.89 | Singleton | No | — | Mid pregnancy: HCG-MoM:0.27, T18:1/357 | TOP |
| 46, X, del(X) (q22) | del (Xq22.3-q28,46.57M)-M | 32 | 16 | 25.65 | Singleton | No | — | — | Female, no obvious abnormality in birth appearance, accordance with her mother’s karyotype of peripheral blood |
| Mosaic Chromosome Karyotype Results | NIPT | Maternal Age (Years Old) | Gestational Age (Weeks *) | BMI (kg/m2) | Number of Fetus | IVF (Yes/No) | History of Adverse Pregnancy and Childbirth | Abnormal Serological Screening Results | Follow Up |
|---|---|---|---|---|---|---|---|---|---|
| 45, X[26]/46, XX[54] | XO | 26 | 19 +4 | 26.23 | Singleton | No | — | — | TOP |
| 45, X[11]/46, XX[81] | XO | 25 | 17 +3 | 20.83 | Singleton | No | — | PAPPA-MoM:3.39 | TOP |
| 47, XXX[18]/46, XX[37] | XO | 28 | 16 +3 | 17.04 | Singleton | No | — | — | Female, no obvious abnormality in birth appearance |
| 45, X[4]/46, XX[46] | XO | 24 | 19 | 23.93 | Singleton | No | — | second-trimester screening: HCG-MoM:2.31 | Female, no obvious abnormality in birth appearance |
| 45, X[15]/46, XX[86] | XO | 32 | 12 +6 | 26.35 | Singleton | No | — | — | Female, no obvious abnormality in birth appearance |
| 45, X[4]/46, XX[50] | XO | 27 | 17 +2 | 25.85 | Singleton | No | — | — | Female, no obvious abnormality in birth appearance |
| 45, X[8]/46, XX[92] | XO | 29 | 18 +5 | 27.27 | Singleton | No | — | — | TOP, normal karyotype of peripheral blood with both husband and wife |
| 47, XXX[33]/46, XX[62] | XXX | 26 | 17 +4 | 23.93 | Singleton | No | — | — | Female, no obvious abnormality in birth appearance |
| 45, X[30]/46, XY[70] | XO | 40 | 17 +1 | 24.14 | Singleton | No | Spontaneous abortion three times | second-trimester screening: T21:1/400, T18:1/991 | Male, no obvious abnormality in birth appearance |
| 47, XYY[52]/46, XY[10] | XYY | 30 | 16 +1 | 26.45 | Singleton | Yes | Spontaneous abortion once | PAPPA-MoM:2.18 | Male, no obvious abnormality in birth appearance |
| 45, X[15]/46, XX[65] | XO | 25 | 16 +1 | 19.72 | Singleton | No | — | first-trimester screening: HCG-MoM:6.27, T21:1/61; second-trimester screening: HCG-MoM:5.36, T21:1/33 | TOP |
| 47, XYY[60]/46, XY[8] | XYY | 23 | 17 +5 | 20.7 | Singleton | No | — | second-trimester screening: HCG-MoM:0.29 | Male, no obvious abnormality in birth appearance |
| 47, XXY[14]/46, XX[4]/46, XY[91] | XXY | 37 | 17 +3 | 20.34 | Singleton | No | — | second-trimester screening: HCG-MoM:3.04, T21:1/80 | Male, no obvious abnormality in birth appearance |
| 48, XXXX[44]/47, XXX[6] | X(increased)-M | 44 | 16 +2 | 19.53 | Singleton | No | — | second-trimester screening: AFP-MoM:2.37, T21:1/217, T18:1/812 | Female, no obvious abnormality in birth appearance |
| 45, X[19]/47, XXX[1]/46, XX[62] | XO | 23 | 16 +6 | 17.19 | Singleton | No | — | second-trimester screening: HCG-MoM:5.7, T21:1/62 | TOP |
| 45, X[40]/46, XX[55] | XO | 39 | 15 +5 | 24.03 | Singleton | No | Spontaneous abortion three times | first-trimester screening: T21:1/214; second-trimester screening: T21:1/145 | TOP |
| 45, X[50]/46, XY[50] | XO | 31 | 12 +5 | 22.67 | Singleton | Yes | — | second-trimester screening: HCG-MoM:3.19, T21:1/65 | TOP |
| 45, X[6]/46, XX[94] | XO | 37 | 19 +6 | 22.03 | Singleton | No | — | second-trimester screening: T21:1/205 | Female, no obvious abnormality in birth appearance |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lu, Y.; Zhou, S.; Linpeng, S.; Ding, S.; Li, S.; Li, Y.; Shi, L.; He, J.; Liu, Y. Cell-Free DNA Screening for Sex Chromosome Abnormalities and Pregnancy Outcomes, 2018–2020: A Retrospective Analysis. J. Pers. Med. 2022, 12, 48. https://doi.org/10.3390/jpm12010048
Lu Y, Zhou S, Linpeng S, Ding S, Li S, Li Y, Shi L, He J, Liu Y. Cell-Free DNA Screening for Sex Chromosome Abnormalities and Pregnancy Outcomes, 2018–2020: A Retrospective Analysis. Journal of Personalized Medicine. 2022; 12(1):48. https://doi.org/10.3390/jpm12010048
Chicago/Turabian StyleLu, Yanmei, Shihao Zhou, Siyuan Linpeng, Siyi Ding, Shihong Li, Yujiao Li, Liangcheng Shi, Jun He, and Yalan Liu. 2022. "Cell-Free DNA Screening for Sex Chromosome Abnormalities and Pregnancy Outcomes, 2018–2020: A Retrospective Analysis" Journal of Personalized Medicine 12, no. 1: 48. https://doi.org/10.3390/jpm12010048
APA StyleLu, Y., Zhou, S., Linpeng, S., Ding, S., Li, S., Li, Y., Shi, L., He, J., & Liu, Y. (2022). Cell-Free DNA Screening for Sex Chromosome Abnormalities and Pregnancy Outcomes, 2018–2020: A Retrospective Analysis. Journal of Personalized Medicine, 12(1), 48. https://doi.org/10.3390/jpm12010048