
Predictors of the CD24/CD11b Biomarker among Healthy Subjects


 and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Isolation of Peripheral Blood Leukocytes
2.3. Flow Cytometry
2.4. Statistics
3. Results
3.1. Demographics and Population Characteristics
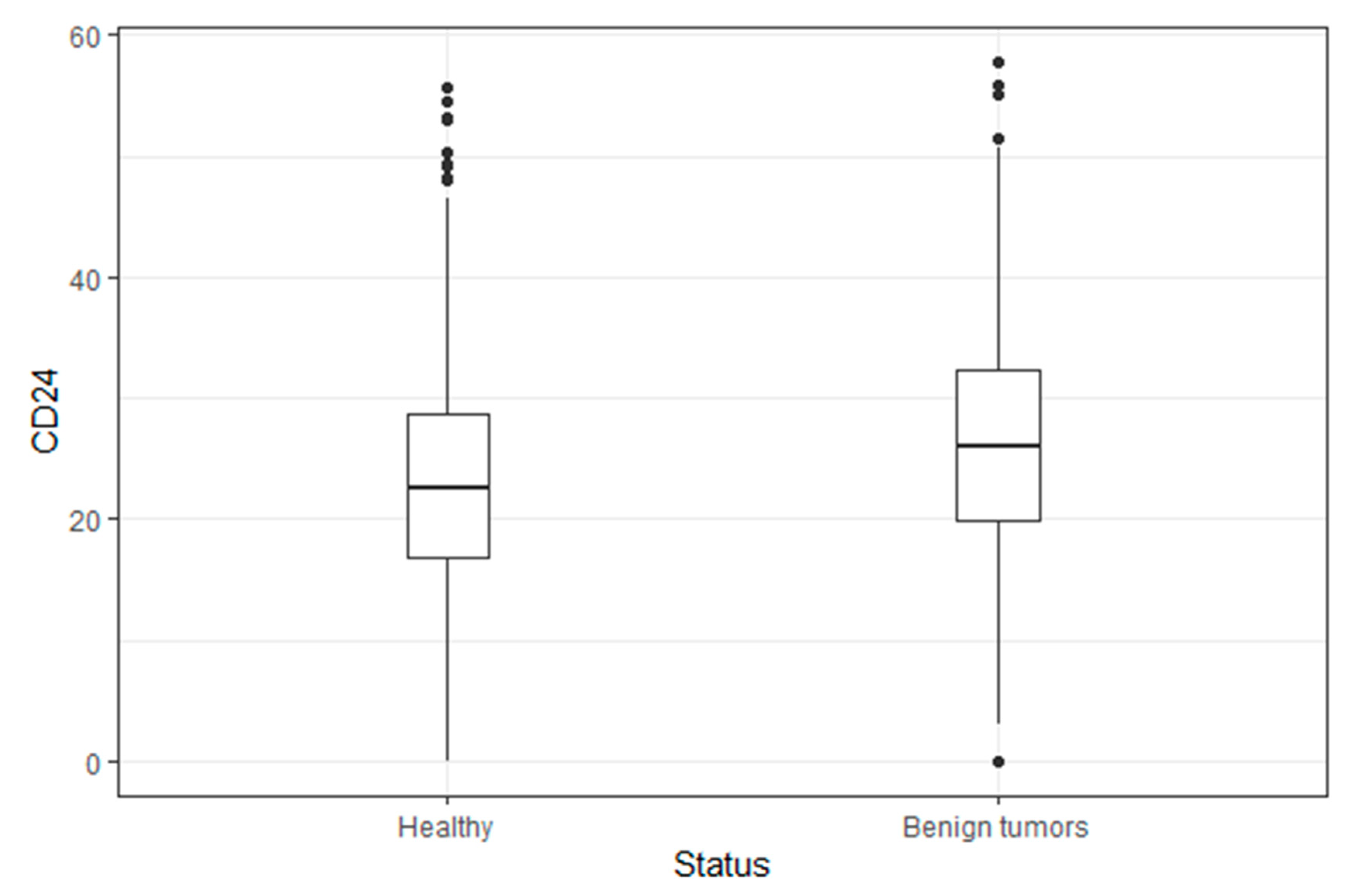
3.2. CD24 Levels in Subjects with Benign Tumors Compared to Healthy Subjects
3.3. Association between Participants’ Characteristics and CD24 Levels Univariate and Multivariate Analysis
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Duffy, M.J. Tumor Markers in Clinical Practice: A Review Focusing on Common Solid Cancers. Med. Princ. Pr. 2013, 22, 4–11. [Google Scholar] [CrossRef]
- Kraus, S.; Shapira, S.; Kazanov, D.; Naumov, I.; Moshkowitz, M.; Santo, E.; Galazan, L.; Geva, R.; Shmueli, E.; Hallack, A.; et al. Predictive Levels of CD24 in Peripheral Blood Leukocytes for the Early Detection of Colorectal Adenomas and Adenocarcinomas. Dis. Markers 2015, 2015, 1–9. [Google Scholar] [CrossRef]
- Sagiv, E.; Memeo, L.; Karin, A.; Kazanov, D.; Jacob–Hirsch, J.; Mansukhani, M.; Rechavi, G.; Hibshoosh, H.; Arber, N. CD24 Is a New Oncogene, Early at the Multistep Process of Colorectal Cancer Carcinogenesis. Gastroenterology 2006, 131, 630–639. [Google Scholar] [CrossRef]
- Shamai, S.; Nabiochtchikov, I.; Kraus, S.; Zigdon, S.; Kazanov, D.; Itzhak-Klutch, M.; Eizner, C.; Arber, N.; Geva, R. CD24 and APC Genetic Polymorphisms in Pancreatic Cancers as Potential Biomarkers for Clinical Outcome. PLoS ONE 2015, 10, e0134469. [Google Scholar] [CrossRef]
- Shapira, S.; Kazanov, D.; Mdah, F.; Yaakobi, H.; Herishanu, Y.; Perry, C.; Avivi, I.; Itchaki, G.; Shacham-Abulafia, A.; Raanani, P.; et al. Feasibly of CD24/CD11b as a Screening Test for Hematological Malignancies. J. Pers. Med. 2021, 11, 724. [Google Scholar] [CrossRef] [PubMed]
- Baumann, P.; Cremers, N.; Kroese, F.; Orend, G.; Chiquet-Ehrismann, R.; Uede, T.; Yagita, H.; Sleeman, J.P. CD24 expression causes the acquisition of multiple cellular properties associated with tumor growth and metastasis. Cancer Res. 2005, 65, 10783–10793. [Google Scholar] [CrossRef]
- Fang, X.; Zheng, P.; Tang, J.; Liu, Y. CD24: From A to Z. Cell. Mol. Immunol. 2010, 7, 100–103. [Google Scholar] [CrossRef]
- Sagiv, E.; Arber, N. The novel oncogeneCD24and its arising role in the carcinogenesis of the GI tract: From research to therapy. Expert Rev. Gastroenterol. Hepatol. 2008, 2, 125–133. [Google Scholar] [CrossRef]
- Kristiansen, G.; Denkert, C.; Schlüns, K.; Dahl, E.; Pilarsky, C.; Hauptmann, S. CD24 Is Expressed in Ovarian Cancer and Is a New Independent Prognostic Marker of Patient Survival. Am. J. Pathol. 2002, 161, 1215–1221. [Google Scholar] [CrossRef]
- Ortiz-Montero, P.; Liu-Bordes, W.-Y.; Londoño-Vallejo, A.; Vernot, J.-P. CD24 expression and stem-associated features define tumor cell heterogeneity and tumorigenic capacities in a model of carcinogenesis. Cancer Manag. Res. 2018, 10, 5767–5784. [Google Scholar] [CrossRef]
- Farid, R.M.; Sammour, S.A.E.-M.; El-Din, Z.A.E.-K.S.; Salman, M.I.; Omran, T.I. Expression of CD133 and CD24 and their different phenotypes in urinary bladder carcinoma. Cancer Manag. Res. 2019, 11, 4677–4690. [Google Scholar] [CrossRef] [PubMed]
- Kristiansen, G.; Sammar, M.; Altevogt, P. Tumour Biological Aspects of CD24, A Mucin-Like Adhesion Molecule. J. Mol. Histol. 2003, 35, 255–262. [Google Scholar] [CrossRef]
- Altevogt, P.; Sammar, M.; Hüser, L.; Kristiansen, G. Novel insights into the function of CD24: A driving force in cancer. Int. J. Cancer 2020, 148, 546–559. [Google Scholar] [CrossRef]
- Jing, X.; Cui, X.; Liang, H.; Hao, C.; Yang, Z.; Li, X.; Yang, X.; Han, C. CD24 is a Potential Biomarker for Prognosis in Human Breast Carcinoma. Cell. Physiol. Biochem. 2018, 48, 111–119. [Google Scholar] [CrossRef]
- Jaggupilli, A.; Elkord, E. Significance of CD44 and CD24 as Cancer Stem Cell Markers: An Enduring Ambiguity. Clin. Dev. Immunol. 2012, 2012, 1–11. [Google Scholar] [CrossRef]
- Kwon, M.J.; Han, J.; Seo, J.H.; Song, K.; Jeong, H.M.; Choi, J.-S.; Kim, Y.J.; Lee, S.-H.; Choi, Y.-L.; Shin, Y.K. CD24 Overexpression Is Associated with Poor Prognosis in Luminal A and Triple-Negative Breast Cancer. PLoS ONE 2015, 10, e0139112. [Google Scholar] [CrossRef]
- Kristiansen, G.; Winzer, K.-J.; Mayordomo, E.; Bellach, J.; Schlüns, K.; Denkert, C.; Dahl, E.; Pilarsky, C.; Altevogt, P.; Guski, H.; et al. CD24 expression is a new prognostic marker in breast cancer. Clin. Cancer Res. 2003, 9, 4906–4913. [Google Scholar]
- Zhang, P.; Zheng, P.; Liu, Y. Amplification of the CD24 Gene Is an Independent Predictor for Poor Prognosis of Breast Cancer. Front. Genet. 2019, 10, 560. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, T.; Terai, Y.; Kogata, Y.; Ashihara, K.; Maeda, K.; Fujiwara, S.; Yoo, S.; Tanaka, Y.; Tsunetoh, S.; Sasaki, H.; et al. CD24 expression as a marker for predicting clinical outcome and invasive activity in uterine cervical cancer. Oncol. Rep. 2015, 34, 2282–2288. [Google Scholar] [CrossRef]
- Copeland, K.A.F. Applied Linear Statistical Models; McGraw-Hill/Irwin: New York, NY, USA, 1997; Volume 29, ISBN 0072386886. [Google Scholar]
- Ahmed, M.A.H.; Al-Attar, A.; Kim, J.; Watson, N.F.S.; Scholefield, J.H.; Durrant, L.G.; Ilyas, M. CD24 shows early upregulation and nuclear expression but is not a prognostic marker in colorectal cancer. J. Clin. Pathol. 2009, 62, 1117–1122. [Google Scholar] [CrossRef] [PubMed]
- Huang, H.; Hsu, H. Cloning and Expression of CD24 Gene in Human Hepatocellular Carcinoma: A Potential Early Tumor Marker Gene Correlates with p53 Mutation and Tumor Differentiation. Cancer Res. 1995, 55, 4717–4721. [Google Scholar]
- Rostoker, R.; Abelson, S.; Genkin, I.; Ben-Shmuel, S.; Sachidanandam, R.; Scheinman, E.J.; Bitton-Worms, K.; Orr, Z.S.; Caspi, A.; Tzukerman, M.; et al. CD24(+) cells fuel rapid tumor growth and display high metastatic capacity. Breast Cancer Res. 2015, 17, 1–14. [Google Scholar] [CrossRef]
- Zhou, Z.; Li, Y.; Kuang, M.; Wang, X.; Jia, Q.; Cao, J.; Hu, J.; Wu, S.; Wang, Z.; Xiao, J. The CD24+ cell subset promotes invasion and metastasis in human osteosarcoma. eBioMedicine 2020, 51, 102598. [Google Scholar] [CrossRef]
- Lee, K.W.; Castilho, A.; Cheung, V.C.H.; Tang, K.H.; Ma, S.K.Y.; Ng, I.O.-L. CD24+ Liver Tumor-Initiating Cells Drive Self-Renewal and Tumor Initiation through STAT3-Mediated NANOG Regulation. Cell Stem Cell 2011, 9, 50–63. [Google Scholar] [CrossRef]
- Hüser, L.; Altevogt, P.; Utikal, J. Role of STAT3 dependent SOX2 and CD24 expression in melanoma cell adaptive resistance towards targeted therapies. Oncotarget 2019, 10, 1662–1663. [Google Scholar] [CrossRef] [PubMed]
- Li, O.; Zheng, P.; Liu, Y. CD24 Expression on T Cells Is Required for Optimal T Cell Proliferation in Lymphopenic Host. J. Exp. Med. 2004, 200, 1083–1089. [Google Scholar] [CrossRef] [PubMed]
- Lee, K.-M.; Ju, J.-H.; Jang, K.; Yang, W.; Yi, J.Y.; Noh, N.Y.; Shin, I. CD24 regulates cell proliferation and transforming growth factor β-induced epithelial to mesenchymal transition through modulation of integrin β1 stability. Cell. Signal. 2012, 24, 2132–2142. [Google Scholar] [CrossRef] [PubMed]
- Ma, Z.L.; Chen, Y.P.; Song, J.L.; Wang, Y.Q. Knockdown of CD24 inhibits proliferation, invasion and sensitizes breast cancer MCF-7 cells to tamoxifen in vitro. Eur. Rev. Med. Pharmacol. Sci. 2015, 19, 2394–2399. [Google Scholar]
- Folkman, J. What Is the Evidence That Tumors Are Angiogenesis Dependent? J. Natl. Cancer Inst. 1990, 82, 4–7. [Google Scholar] [CrossRef]
- Abulafia, O.; Sherer, D.M. Angiogenesis of the ovary. Am. J. Obstet. Gynecol. 2000, 182, 240–246. [Google Scholar] [CrossRef]
- Islam, S.; Akhtar, M.M.; Ciavattini, A.; Giannubilo, S.R.; Protic, O.; Janjusevic, M.; Procopio, A.D.; Segars, J.H.; Castellucci, M.; Ciarmela, P. Use of dietary phytochemicals to target inflammation, fibrosis, proliferation, and angiogenesis in uterine tissues: Promising options for prevention and treatment of uterine fibroids? Mol. Nutr. Food Res. 2014, 58, 1667–1684. [Google Scholar] [CrossRef] [PubMed]
- Guo, X.; Xu, T.; Zheng, J.; Cui, X.; Li, M.; Wang, K.; Su, M.; Zhang, H.; Zheng, K.; Sun, C.; et al. Accumulation of synovial fluid CD19+CD24hiCD27+ B cells was associated with bone destruction in rheumatoid arthritis. Sci. Rep. 2020, 10, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, M.A.; Jackson, D.; Seth, R.; Robins, A.; Lobo, D.N.; Tomlinson, I.P.; Ilyas, M. CD24 is upregulated in inflammatory bowel disease and stimulates cell motility and colony formation. Inflamm. Bowel Dis. 2010, 16, 795–803. [Google Scholar] [CrossRef]
- Braliou, G.G.; Pantavou, K.G.; Kontou, P.I.; Bagos, P.G. Polymorphismsof the CD24 Gene Are Associated with Risk of Multiple Sclerosis: A Meta-Analysis. Int. J. Mol. Sci. 2015, 16, 12368–12381. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Li, B.; Zhang, X.; Sonpavde, G.P.; Jiao, K.; Zhang, A.; Zhang, G.; Sun, M.; Chu, C.; Li, F.; et al. CD24 is a genetic modifier for risk and progression of prostate cancer. Mol. Carcinog. 2016, 56, 641–650. [Google Scholar] [CrossRef] [PubMed]
- Dowling, P.C.; Cook, S.D. Disease Markers in Acute Multiple Sclerosis. Arch. Neurol. 1976, 33, 668–670. [Google Scholar] [CrossRef]
- Shadick, N.A.; Cook, N.R.; Karlson, E.W.; Ridker, P.M.; Maher, N.E.; Manson, J.E.; Buring, J.E.; Lee, I.-M. C-Reactive Protein in the Prediction of Rheumatoid Arthritis in Women. Arch. Intern. Med. 2006, 166, 2490–2494. [Google Scholar] [CrossRef]
- Pope, J.E.; Choy, E.H. C-reactive protein and implications in rheumatoid arthritis and associated comorbidities. Semin. Arthritis Rheum. 2020, 51, 219–229. [Google Scholar] [CrossRef] [PubMed]
- Vermeire, S.; Van Assche, G.; Rutgeerts, P. C-Reactive Protein as a Marker for Inflammatory Bowel Disease. Inflamm. Bowel Dis. 2004, 10, 661–665. [Google Scholar] [CrossRef]
- Vermeire, S.; Van Assche, G.; Rutgeerts, P. Laboratory markers in IBD: Useful, magic, or unnecessary toys? Gut 2006, 55, 426–431. [Google Scholar] [CrossRef]
- Chen, P.; Zhou, G.; Lin, J.; Li, L.; Zeng, Z.; Chen, M.; Zhang, S. Serum Biomarkers for Inflammatory Bowel Disease. Front. Med. 2020, 7, 123. [Google Scholar] [CrossRef] [PubMed]
- Greuter, T.; Vavricka, S.; König, A.O.; Beaugerie, L.; Scharl, M. Malignancies in Inflammatory Bowel Disease. Digestion 2020, 101, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Axelrad, J.; Lichtiger, S.; Yajnik, V. Inflammatory bowel disease and cancer: The role of inflammation, immunosuppression, and cancer treatment. World J. Gastroenterol. 2016, 22, 4794–4801. [Google Scholar] [CrossRef] [PubMed]
- Klein, A.; Polliack, A.; Gafter-Gvili, A. Rheumatoid arthritis and lymphoma: Incidence, pathogenesis, biology, and outcome. Hematol. Oncol. 2018, 36, 733–739. [Google Scholar] [CrossRef]
- Yadlapati, S.; Efthimiou, P. Autoimmune/Inflammatory Arthritis Associated Lymphomas: Who Is at Risk? BioMed. Res. Int. 2016, 2016, 1–11. [Google Scholar] [CrossRef]
- Hart, P.C.; Rajab, I.M.; Alebraheem, M.; Potempa, L.A. C-Reactive Protein and Cancer—Diagnostic and Therapeutic Insights. Front. Immunol. 2020, 11, 1–17. [Google Scholar] [CrossRef]
- Sproston, N.R.; Ashworth, J.J. Role of C-reactive protein at sites of inflammation and infection. Front. Immunol. 2018, 9, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Vetter, M.L.; Gewurz, H.; Hansen, B.; James, K.; Baum, L.L. Effects of C-reactive protein on human lymphocyte responsiveness. J. Immunol. 1983, 130, 2121–2126. [Google Scholar]
- Singh, S.D.; Henley, S.J.; Ryerson, A.B. Surveillance for Cancer Incidence and Mortality—United States, 2012. MMWR. Morb. Mortal. Wkly. Rep. 2016, 63, 17–58. [Google Scholar] [CrossRef][Green Version]
- Franceschi, C.; Campisi, J. Chronic Inflammation (Inflammaging) and Its Potential Contribution to Age-Associated Diseases. J. Gerontol. Ser. A Boil. Sci. Med. Sci. 2014, 69, S4–S9. [Google Scholar] [CrossRef]
- Duggal, N.A.; Upton, J.; Whittaker, A.; Sapey, E.; Lord, J.M. An age-related numerical and functional deficit in CD19+CD24hiCD38hiB cells is associated with an increase in systemic autoimmunity. Aging Cell 2013, 12, 873–881. [Google Scholar] [CrossRef]
- Watad, A.; Bragazzi, N.L.; Adawi, M.; Amital, H.; Toubi, E.; Porat, B.-S.; Shoenfeld, Y. Autoimmunity in the Elderly: Insights from Basic Science and Clinics—A Mini-Review. Gerontology 2017, 63, 515–523. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Characteristic | Study Population N (%) or Mean (SD) | |
|---|---|---|
| Age At Visit | 48.7 (12.3) | |
| Gender (%) | Female | 668 (44.8%) |
| Male | 822 (55.2%) | |
| Smoking (%) | No | 939 (75.2%) |
| Yes | 310 (24.8%) | |
| Overweight (%) | No | 993 (83.0%) |
| Yes | 203 (17.0%) | |
| Background Disease (%) | With | 1147 (77.0%) |
| Without | 343 (23.0) | |
| Family History of Cancer | Without | 626 (45.8) |
| With | 742 (54.2) | |
| Physical Activity (%) | No | 333 (28.0%) |
| Yes | 858 (72.0%) | |
| CRP Levels (mg/mL) | <10 | 1209 (90.0) |
| ≥10 | 134 (10.0) | |
| Past Cancer (%) | No | 1404 (94.2%) |
| Yes | 86 (5.8%) |
| Characteristic | CD24/CD11b Levels Mean (SD) | |
|---|---|---|
| Age | (19–85) | 22.9 (9.4) |
| Gender (%) | Female | 22.4 (9.6) |
| Male | 23.2 (9.3) | |
| Smoking (%) | No | 22.4 (9.3) |
| Yes | 22.7 (9.7) | |
| Overweight (%) | No | 23.8 (9.0) |
| Yes | 22.2 (9.3) | |
| Background Disease (%) | With | 24.7 (9.4) |
| Without | 22.5 (9.4) | |
| Family History of Cancer | Without | 22.4 (9.5) |
| With | 22.7 (9.1) | |
| Physical Activity (%) | No | 23.4 (10.0) |
| Yes | 22.0 (9.1) | |
| CRP Levels (mg/mL) | <10 | 22.3 (9.3) |
| ≥10 | 27.2 (9.8) | |
| Past Cancer (%) | No | 22.6 (9.4) |
| Yes | 26.6 (10.0) |
| CD24/CD11b Levels | ||||
|---|---|---|---|---|
| Participants’ Characteristics | Univariable Analysis | Multivariable Analysis | ||
| β | p | β | p | |
| Age | 0.07 | 0.002 | 0.04 | 0.130 |
| Gender (Female vs. Male) | 0.75 | 0.147 | 0.91 | 0.104 |
| Smoking (Smoking vs. Non-Smoking) | 0.29 | 0.651 | 0.19 | 0.783 |
| Overweight (Yes vs. No) | 1.63 | 0.027 | 0.85 | 0.295 |
| Background Disease | 2.25 | <0.001 | 0.30 | 0.716 |
| Family History of Cancer (Yes vs. No) | 0.34 | 0.517 | 0.56 | 0.313 |
| Physical Activity (%) | −1.36 | 0.028 | −1.09 | 0.097 |
| CRP (Normal vs. Elevated) | 4.91 | <0.001 | 3.97 | 0.001 |
| Past Cancer (%) | 4.00 | <0.001 | 0.79 | 0.655 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shapira, S.; Aiger, G.; Ohayon, A.; Kazanov, D.; Mdah, F.; Shimon, M.B.; Hay-Levy, M.; Banon, L.; Laskov, I.; Mashiah, J.; et al. Predictors of the CD24/CD11b Biomarker among Healthy Subjects. J. Pers. Med. 2021, 11, 939. https://doi.org/10.3390/jpm11090939
Shapira S, Aiger G, Ohayon A, Kazanov D, Mdah F, Shimon MB, Hay-Levy M, Banon L, Laskov I, Mashiah J, et al. Predictors of the CD24/CD11b Biomarker among Healthy Subjects. Journal of Personalized Medicine. 2021; 11(9):939. https://doi.org/10.3390/jpm11090939
Chicago/Turabian StyleShapira, Shiran, Gal Aiger, Amitay Ohayon, Dina Kazanov, Fatin Mdah, Marina Ben Shimon, Mori Hay-Levy, Lian Banon, Ido Laskov, Jacob Mashiah, and et al. 2021. "Predictors of the CD24/CD11b Biomarker among Healthy Subjects" Journal of Personalized Medicine 11, no. 9: 939. https://doi.org/10.3390/jpm11090939
APA StyleShapira, S., Aiger, G., Ohayon, A., Kazanov, D., Mdah, F., Shimon, M. B., Hay-Levy, M., Banon, L., Laskov, I., Mashiah, J., Lev-Ari, S., & Arber, N. (2021). Predictors of the CD24/CD11b Biomarker among Healthy Subjects. Journal of Personalized Medicine, 11(9), 939. https://doi.org/10.3390/jpm11090939