
Lower Ratio of Liver Volume and Body Weight Is a Negative Predictor of Survival after Transjugular Intrahepatic Portosystemic Shunt

 ,
,  , , , , , and
, , , , , and 
Abstract
1. Introduction
2. Results
2.1. Patient Characteristics
2.2. Development of Liver Function and Liver Volume following TIPS Insertion
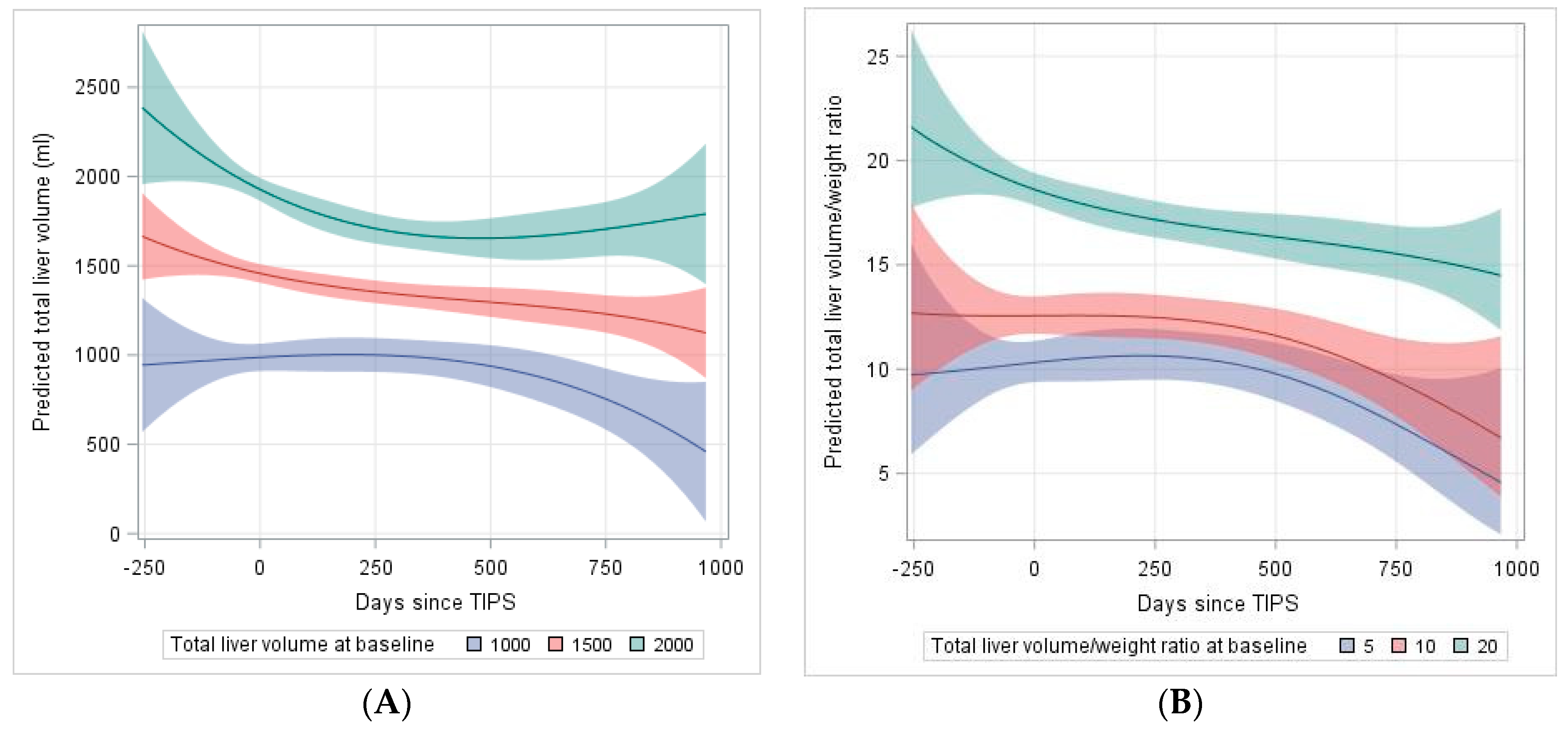
2.3. Analysis of Predictors for the Development of Liver Volume after TIPS
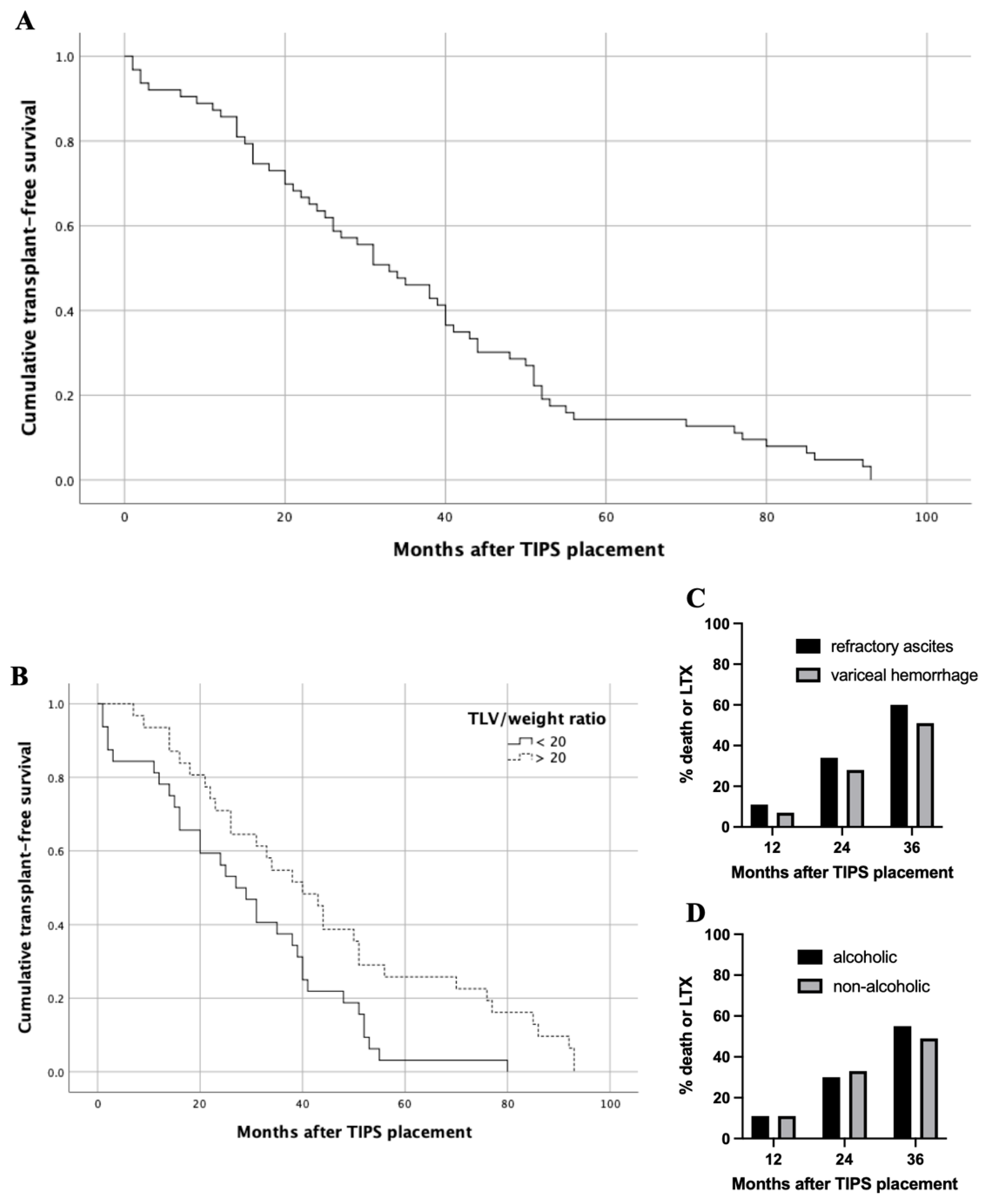
2.4. Survival Analysis Regarding Baseline Liver Volumes
3. Discussion
4. Materials and Methods
4.1. Study Design and Patient Selection
4.2. TIPS Procedure
4.3. Data Collection and Follow-Up
4.4. Imaging-Based Volumetry of the Liver
4.5. Statistics
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hung, M.L.; Lee, E.W. Role of Transjugular Intrahepatic Portosystemic Shunt in the Management of Portal Hypertension: Review and Update of the Literature. Clin. Liver Dis. 2019, 23, 737–754. [Google Scholar] [CrossRef]
- Russo, M.W.; Sood, A.; Jacobson, I.M.; Brown, R.S. Transjugular intrahepatic portosystemic shunt for refractory ascites: An analysis of the literature on efficacy, morbidity, and mortality. Am. J. Gastroenterol. 2003, 98, 2521–2527. [Google Scholar] [CrossRef]
- Perry, B.C.; Kwan, S.W. Portosystemic Shunts: Stable Utilization and Improved Outcomes, Two Decades after the Transjugular Intrahepatic Portosystemic Shunt. J. Am. Coll. Radiol. 2015, 12, 1427–1433. [Google Scholar] [CrossRef]
- Bureau, C.; Thabut, D.; Oberti, F.; Dharancy, S.; Carbonell, N.; Bouvier, A.; Mathurin, P.; Otal, P.; Cabarrou, P.; Péron, J.M.; et al. Transjugular Intrahepatic Portosystemic Shunts with Covered Stents Increase Transplant-Free Survival of Patients with Cirrhosis and Recurrent Ascites. Gastroenterology 2017, 152, 157–163. [Google Scholar] [CrossRef] [PubMed]
- Horhat, A.; Bureau, C.; Thabut, D.; Rudler, M. Transjugular intrahepatic portosystemic shunt in patients with cirrhosis: Indications and post-transjugular intrahepatic portosystemic shunt complications in 2020. United Eur. Gastroenterol. J. 2020, 9, 203–208. [Google Scholar] [CrossRef] [PubMed]
- Lopera, J.E.; Speeg, K.V.; Young, C.; Garg, D.; Michalek, J.; Chen, Y.; Kroma, G.; Suri, R.; Garza-Berlanga, A. Effect of liver volume in morbidity and mortality after elective transjugular intrahepatic portosystemic shunt. Gastrointest. Interv. 2014, 3, 93–97. [Google Scholar] [CrossRef][Green Version]
- Schiano, T.D.; Bodian, C.; Schwartz, M.E.; Glajchen, N.; Min, A.D. Accuracy and significance of computed tomographic scan assessment of hepatic volume in patients undergoing liver transplantation. Transplantation 2000, 69, 545–550. [Google Scholar] [CrossRef] [PubMed]
- Vizzutti, F.; Schepis, F.; Arena, U.; Fanelli, F.; Gitto, S.; Aspite, S.; Turco, L.; Dragoni, G.; Laffi, G.; Marra, F. Transjugular intrahepatic portosystemic shunt (TIPS): Current indications and strategies to improve the outcomes. Intern. Emerg. Med. 2020, 15, 37–48. [Google Scholar] [CrossRef]
- Tu, R.; Xia, L.P.; Yu, A.L.; Wu, L. Assessment of hepatic functional reserve by cirrhosis grading and liver volume measurement using CT. World J. Gastroenterol. 2007, 13, 3956–3961. [Google Scholar] [CrossRef]
- Saygili, O.B.; Tarhan, N.C.; Yildirim, T.; Serin, E.; Ozer, B.; Agildere, A.M. Value of computed tomography and magnetic resonance imaging for assessing severity of liver cirrhosis secondary to viral hepatitis. Eur. J. Radiol. 2005, 54, 400–407. [Google Scholar] [CrossRef] [PubMed]
- Kok, B.; Abraldes, J.G. Patient Selection in Transjugular Intrahepatic Portosystemic Shunt (TIPS) for Refractory Ascites and Associated Conditions. Curr. Hepatol. Rep. 2019, 18, 197–205. [Google Scholar] [CrossRef]
- Lim, M.C.; Tan, C.H.; Cai, J.; Zheng, J.; Kow, A.W.C. CT volumetry of the liver: Where does it stand in clinical practice? Clin. Radiol. 2014, 69, 887–895. [Google Scholar] [CrossRef] [PubMed]
- Kishi, Y.; Abdalla, E.K.; Chun, Y.S.; Zorzi, D.; Madoff, D.C.; Wallace, M.J.; Curley, S.A.; Vauthey, J.N. Three hundred and one consecutive extended right hepatectomies: Evaluation of outcome based on systematic liver volumetry. Ann. Surg. 2009, 250, 540–547. [Google Scholar] [CrossRef]
- Wei, L.; Zhu, Z.J.; Lü, Y.; Jiang, W.T.; Gao, W.; Zeng, Z.G.; Shen, Z.Y. Application of computer-assisted three-dimensional quantitative assessment and a surgical planning tool for living donor liver transplantation. Chin. Med. J. 2013, 126, 1288–1291. [Google Scholar] [PubMed]
- Cohen, B.; Tafreshi, S.; Tafreshi, R.; Cantos, A. Abstract No. 582 Liver volume as a predictor of 30-day mortality post transjugular intrahepatic portosystemic shunt (TIPS) creation. J. Vasc. Interv. Radiol. 2019, 30, S251. [Google Scholar] [CrossRef]
- García-Pagán, J.C.; Saffo, S.; Mandorfer, M.; Garcia-Tsao, G. Where does TIPS fit in the management of patients with cirrhosis? JHEP Rep. 2020, 2, 100122. [Google Scholar] [CrossRef] [PubMed]
- Ronald, J.; Wang, Q.; Choi, S.S.; Suhocki, P.V.; Hall, M.D.; Smith, T.P.; Kim, C.Y. Albumin-bilirubin grade versus MELD score for predicting survival after transjugular intrahepatic portosystemic shunt (TIPS) creation. Diagn. Interv. Imaging 2018, 99, 163–168. [Google Scholar] [CrossRef]
- Zhou, C.; Hou, C.; Cheng, D.; Tang, W.; Lv, W. Predictive accuracy comparison of meld and child-turcotte-pugh scores for survival in patients underwent TIPS placement: A systematic meta-analytic review. Int. J. Clin. Exp. Med. 2015, 8, 13464–13472. [Google Scholar] [PubMed]
- Bettinger, D.; Sturm, L.; Pfaff, L.; Hahn, F.; Kloeckner, R.; Volkwein, L.; Praktiknjo, M.; Lv, Y.; Han, G.; Huber, J.P.; et al. Refining prediction of survival after TIPS with the novel Freiburg index of post-TIPS survival. J. Hepatol. 2021, 74, 1362–1372. [Google Scholar] [CrossRef]
- Yao, X.; Zhou, H.; Huang, S.; Tang, S.H.; Qin, J.P. Effects of transjugular intrahepatic portosystemic shunt using the Viatorr stent on hepatic reserve function in patients with cirrhosis. World J. Clin. Cases 2021, 9, 1532–1542. [Google Scholar] [CrossRef]
- Vauthey, J.N.; Chaoui, A.; Do, K.A.; Bilimoria, M.M.; Fenstermacher, M.J.; Charnsangavej, C.; Hicks, M.; Alsfasser, G.; Lauwers, G.; Hawkins, I.F.; et al. Standardized measurement of the future liver remnant prior to extended liver resection: Methodology and clinical associations. Surgery 2000, 127, 512–519. [Google Scholar] [CrossRef] [PubMed]
- Zahel, T.; Wildgruber, M.; Ardon, R.; Schuster, T.; Rummeny, E.J.; Dobritz, M. Rapid assessment of liver volumetry by a novel automated segmentation algorithm. J. Comput. Assist. Tomogr. 2013, 37, 577–582. [Google Scholar] [CrossRef] [PubMed]
- Austin, P.C. Optimal caliper widths for propensity-score matching when estimating differences in means and differences in proportions in observational studies. Pharm. Stat. 2011, 10, 150–161. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| No. (%), Median (Range) or Mean (SD) | |
|---|---|
| Total | 72 (100) |
| Sex | |
| male | 40 (55.6) |
| female | 32 (44.4) |
| median age (range), y | 60 (21–81) |
| etiology of liver disease | |
| alcoholic | 36 (50.0) |
| viral | 9 (12.5) |
| NAFLD | 8 (11.1) |
| other | 19 (26.4) |
| Child’s grade | |
| A | 14 (19.4) |
| B | 47 (65.3) |
| C | 11 (15.3) |
| Mean MELD-score pre-TIPS (SD) | 11.7 (6.0) |
| indication for TIPS | |
| refractory ascites | 54 (75.0) |
| variceal hemorrhage | 14 (19.4) |
| other | 4 (5.6) |
| Baseline n = 72 | FU 1 | FU 2 | FU 3 | FU 4 | FU 5 | p-Value * | |
|---|---|---|---|---|---|---|---|
| 90–180 d n = 32 | 180–365 d n = 36 | 365–545 d n = 26 | 545–730 d n = 10 | >730 d n = 19 | |||
| MELD-score | 12.08 (6.01) | 12.44 (7.79) | 12.31 (3.89) | 13.89 (6.33) | 15.22 (6.16) | 9.52 (3.28) | 0.0224 |
| Albumin, g/dL | 3.55 (3.99) | 2.81 (0.68) | 3.2 (0.39) | 3.13 (0.72) | 3.39 (0.71) | 3.53 (0.61) | 0.8792 |
| Bilirubin, mg/dL | 1.72 (1.01) | 2.63 (2.91) | 2.58 (2.23) | 4.03 (4.2) | 3.6 (4.24) | 1.67 (1.02) | 0.0008 |
| Creatinine, mg/dL | 1.27 (0.96) | 1.09 (0.89) | 1.06 (0.59) | 1.09 (0.65) | 1.28 (0.44) | 0.96 (0.21) | 0.0801 |
| AST, U/L | 41.71 (18.01) | 73.48 (119.23) | 63.09 (65.57) | 73.58 (103.5) | 46 (26.14) | 54.68 (51.09) | 0.3755 |
| ALT, U/L | 27.45 (16.35) | 40.9 (39.86) | 39.56 (38.93) | 41.46 (47.24) | 30 (9.74) | 55.53 (124.29) | 0.3760 |
| INR | 1.38 (0.28) | 1.53 (0.69) | 1.4 (0.27) | 1.5 (0.45) | 1.49 (0.43) | 1.25 (0.21) | 0.0125 |
| LDH, U/L | 163.15 (63.53) | 256.65 (162.44) | 271.58 (172.76) | 210.57 (62.79) | 313.86 (132.32) | 226.92 (54.02) | 0.0004 |
| PTT, s | 42.54 (11.44) | 46.97 (18.99) | 45.86 (16.58) | 46.69 (15.09) | 46 (16.25) | 43.11 (23.18) | 0.3581 |
| Quick, % | 62.83 (15.6) | 58.81 (17.1) | 60.61 (12.96) | 59 (16.4) | 61.5 (21.46) | 73.74 (14.94) | 0.0057 |
| Sodium, mmol/L | 136.7 (4.88) | 138.84 (4.27) | 139.34 (2.99) | 137.92 (4.87) | 140.56 (3.71) | 140.39 (2.33) | 0.0003 |
| Urea, mg/dL | 21.79 (15.17) | 20.8 (15.74) | 17.36 (7.76) | 16.94 (9.1) | 26.75 (22.41) | 15.62 (4.27) | 0.1490 |
| PPG, mmHg | 8.64 (3.34) | 8.56 (3.25) | 8.89 (3.21) | 8.04 (3.59) | 7.6 (3.03) | 9.95 (3.34) | 0.4051+ |
| Baseline | FU 1 | FU 2 | FU 3 | FU 4 | FU 5 | p-Value * | |
|---|---|---|---|---|---|---|---|
| 90–180 d | 180–365 d | 365–545 d | 545–730 d | >730 d | |||
| TLV | 1603.66 (561.4) | 1446.52 (500.03) | 1427.53 (544.12) | 1432.83 (510.6) | 1149.18 (364.63) | 1373.71 (702.68) | <0.0001 |
| LLV | 613.31 (283.67) | 571.31 (353.7) | 526.64 (286.17) | 606.11 (304.59) | 460.19 (181.63) | 488.87 (331.78) | 0.0102 |
| RLV | 904.17 (382.13) | 781.14 (323.07) | 818.57 (290.14) | 766.77 (298.45) | 647.5 (245.71) | 810.49 (342.41) | <0.0001 |
| TLV/weight | 20.6 (7.76) | 18.43 (7) | 17.79 (7.12) | 17.25 (5.66) | 18.19 (8.79) | 16.93 (8.55) | <0.0001 |
| Correlation *\p-Value | TLV | TLV/Weight | MELD | Albumin | Bilirubin | Creatinine | AST | ALT | INR | LDH | PTT | Quick | Sodium | Urea |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| TLV | ./. | 0.00065 | 0.1973 | 0.74895 | 0.03839 | 0.44190 | 0.48834 | 0.64177 | 0.51723 | 0.67516 | 0.81028 | 0.46601 | 0.58287 | 0.88812 |
| TLV/weight | 0.69624 | ./. | 0.0649 | 0.45499 | 0.04249 | 0.85433 | 0.61763 | 0.58616 | 0.26867 | 0.60208 | 0.78863 | 0.24511 | 0.80954 | 0.88729 |
| MELD | −0.28579 | −0.42046 | ./. | 0.2530 | <0.0001 | 0.0063 | 0.1803 | 0.7223 | <0.0001 | 0.6677 | 0.0100 | <0.0001 | 0.9844 | 0.0006 |
| Albumin | 0.10934 | 0.26748 | −0.31485 | ./. | 0.74289 | 0.01812 | 0.72696 | 0.51659 | 0.36531 | 0.57033 | 0.59542 | 0.51607 | 0.14692 | 0.28611 |
| Bilirubin | −0.44413 | −0.45760 | 0.75902 | 0.09254 | ./. | 0.82206 | 0.00303 | 0.01641 | 0.00016 | 0.94956 | 0.00107 | 0.00005 | 0.99360 | 0.01020 |
| Creatinine | 0.17280 | 0.04386 | 0.4742 | −0.59971 | −0.04139 | ./. | 0.48094 | 0.19296 | 0.66223 | 0.22505 | 0.41006 | 0.76493 | 0.65456 | 0.01296 |
| AST | −0.15593 | −0.11889 | 0.24702 | 0.09848 | 0.51506 | −0.13144 | ./. | 0.00012 | 0.09792 | 0.40718 | 0.09001 | 0.10339 | 0.27817 | 0.25259 |
| ALT | −0.10783 | 0.13339 | 0.06768 | 0.18943 | 0.43458 | −0.24445 | 0.65256 | ./. | 0.16737 | 0.03503 | 0.31801 | 0.29051 | 0.35454 | 0.91387 |
| INR | −0.14585 | −0.25979 | −0.67927 | −0.25179 | 0.61828 | −0.08029 | 0.30267 | 0.16737 | ./. | 0.55882 | <0.0001 | <0.0001 | 0.80411 | 0.15309 |
| LDH | 0.11807 | 0.15978 | 0.10233 | −0.18246 | −0.01512 | 0.28394 | 0.19616 | 0.03503 | 0.13904 | ./. | 0.16707 | 0.53069 | 0.82577 | 0.43791 |
| PTT | 0.05431 | −0.06401 | 0.44845 | −0.14928 | 0.55158 | −0.15079 | 0.30968 | 0.31801 | 0.81249 | 0.32138 | ./. | <0.0001 | 0.44752 | 0.07011 |
| Quick | 0.16393 | 0.27249 | −0.67927 | 0.18206 | −0.65460 | 0.05501 | −0.29807 | −0.19951 | −0.98577 | −0.14900 | −0.79421 | ./. | 0.88089 | 0.10789 |
| Sodium | 0.12387 | −0.05756 | 0.00359 | 0.39334 | −0.00148 | −0.08223 | −0.20104 | −0.17516 | −0.04564 | −0.05257 | −0.13915 | 0.02758 | ./. | 0.95956 |
| Urea | 0.03826 | −0.04176 | 0.70034 | −0.40000 | 0.56021 | 0.54497 | 0.26838 | −0.02746 | 0.33170 | 0.22567 | 0.41327 | −0.37043 | 0.01212 | ./. |
| Effect | Estimate | Standard Error | Pr > |t| | Lower | Upper |
|---|---|---|---|---|---|
| Intercept | 47.1441 | 82.8292 | 0.5711 | −118.05 | 212.34 |
| Time (days since TIPS) | 1.5689 | 0.9389 | 0.1015 | −0.3210 | 3.4588 |
| Volume before TIPS | 0.9403 | 0.04938 | <0.0001 | 0.8418 | 1.0387 |
| Time × volume before TIPS | −0.00143 | 0.000617 | 0.0251 | −0.00267 | −0.00019 |
| Time2 × volume | 2.031 × 10−6 | 2.346 × 10−6 | 0.3910 | −2.69 × 10−6 | 6.75 × 10−6 |
| Time2 | −0.00226 | 0.003483 | 0.5195 | −0.00927 | 0.00475 |
| Time3 × volume | −14 × 10−11 | 0 | <0.0001 | . | . |
| Time3 | −3.58 × 10−7 | 2.968 × 10−6 | 0.9045 | −6.33 × 10−6 | 5.615 × 10−6 |
| Effect | Estimate | Standard Error | Pr > |t| | Lower | Upper |
|---|---|---|---|---|---|
| Intercept | 2.1375 | 0.06172 | <0.0001 | 2.0143 | 2.2607 |
| Time (days since TIPS) | 0.000454 | 0.000630 | 0.4749 | −0.00082 | 0.000172 |
| TLV/weight before TIPS | 0.03932 | 0.002835 | <0.0001 | 0.03366 | 0.04498 |
| Time x TLV/weight before TIPS | −0.00004 | 0.000032 | 0.1792 | −0.00011 | 0.00002 |
| Time2 × TLV/weight | 4.858 × 10−8 | 0 | <0.0001 | . | . |
| Time2 | −4.64 × 10−7 | 2.45 × 10−6 | 0.8506 | −5.4 × 10−6 | 4.473 × 10−6 |
| Time3 × TLV/weight | 3.86 × 10−11 | 0 | <0.0001 | . | . |
| Time3 | −1.11 × 10−9 | 0 | <0.0001 | . | . |
| Effect | Estimate | Standard Error | Pr > |t| | Lower | Upper |
|---|---|---|---|---|---|
| Intercept | 408.08 | 124.74 | 0.0017 | 159.10 | 657.06 |
| Time (days since TIPS) | −0.7438 | 0.1730 | <0.0001 | −1.0900 | −0.3976 |
| INR before TIPS | −220.14 | 90.5786 | 0.0178 | −400.94 | −39.3451 |
| Time × INR | 0.3992 | 0.1203 | 0.0015 | 0.1586 | 0.6399 |
| TLV before TIPS (ml) | 0.8909 | 0.04062 | <0.0001 | 0.8098 | 0.9720 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schindler, P.; Riegel, A.; Görlich, D.; Köppe, J.; Seifert, L.L.; Masthoff, M.; Maschmeier, M.; Wilms, C.; Seidensticker, M.; Köhler, M.; et al. Lower Ratio of Liver Volume and Body Weight Is a Negative Predictor of Survival after Transjugular Intrahepatic Portosystemic Shunt. J. Pers. Med. 2021, 11, 903. https://doi.org/10.3390/jpm11090903
Schindler P, Riegel A, Görlich D, Köppe J, Seifert LL, Masthoff M, Maschmeier M, Wilms C, Seidensticker M, Köhler M, et al. Lower Ratio of Liver Volume and Body Weight Is a Negative Predictor of Survival after Transjugular Intrahepatic Portosystemic Shunt. Journal of Personalized Medicine. 2021; 11(9):903. https://doi.org/10.3390/jpm11090903
Chicago/Turabian StyleSchindler, Philipp, Arne Riegel, Dennis Görlich, Jeanette Köppe, Leon Louis Seifert, Max Masthoff, Miriam Maschmeier, Christian Wilms, Max Seidensticker, Michael Köhler, and et al. 2021. "Lower Ratio of Liver Volume and Body Weight Is a Negative Predictor of Survival after Transjugular Intrahepatic Portosystemic Shunt" Journal of Personalized Medicine 11, no. 9: 903. https://doi.org/10.3390/jpm11090903
APA StyleSchindler, P., Riegel, A., Görlich, D., Köppe, J., Seifert, L. L., Masthoff, M., Maschmeier, M., Wilms, C., Seidensticker, M., Köhler, M., Trebicka, J., Heinzow, H., & Wildgruber, M. (2021). Lower Ratio of Liver Volume and Body Weight Is a Negative Predictor of Survival after Transjugular Intrahepatic Portosystemic Shunt. Journal of Personalized Medicine, 11(9), 903. https://doi.org/10.3390/jpm11090903