
Discrimination of Exudative Pleural Effusions Based on Pleural Adenosine Deaminase (ADA)-C-Reactive Protein (CRP) Levels, and Their Combination: An Observational Prospective Study




Abstract
1. Introduction
2. Materials and Methods
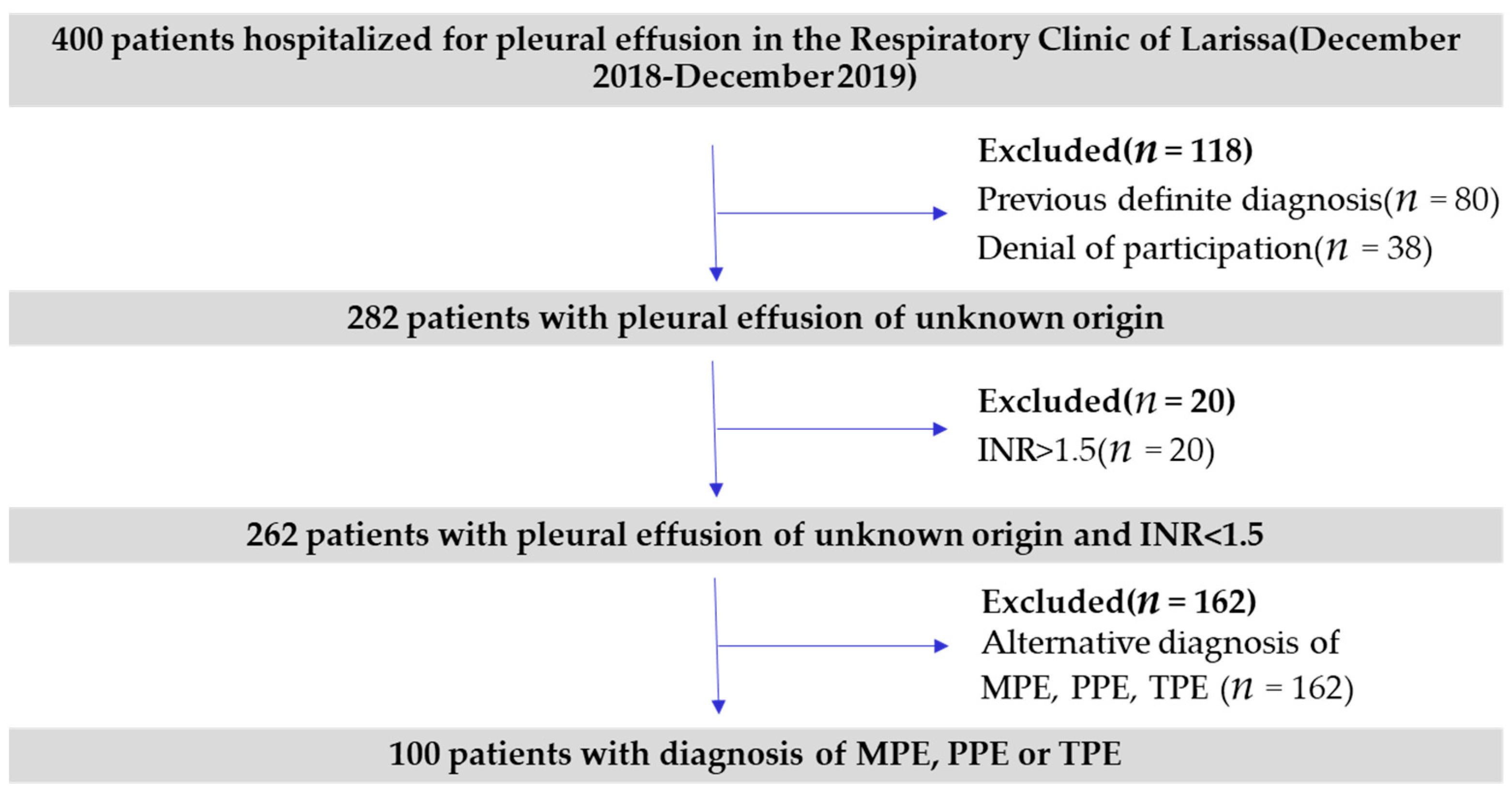
2.1. Study Population
2.2. Laboratory Tests
2.3. Statistical Analysis
3. Results
3.1. Patients Characteristics
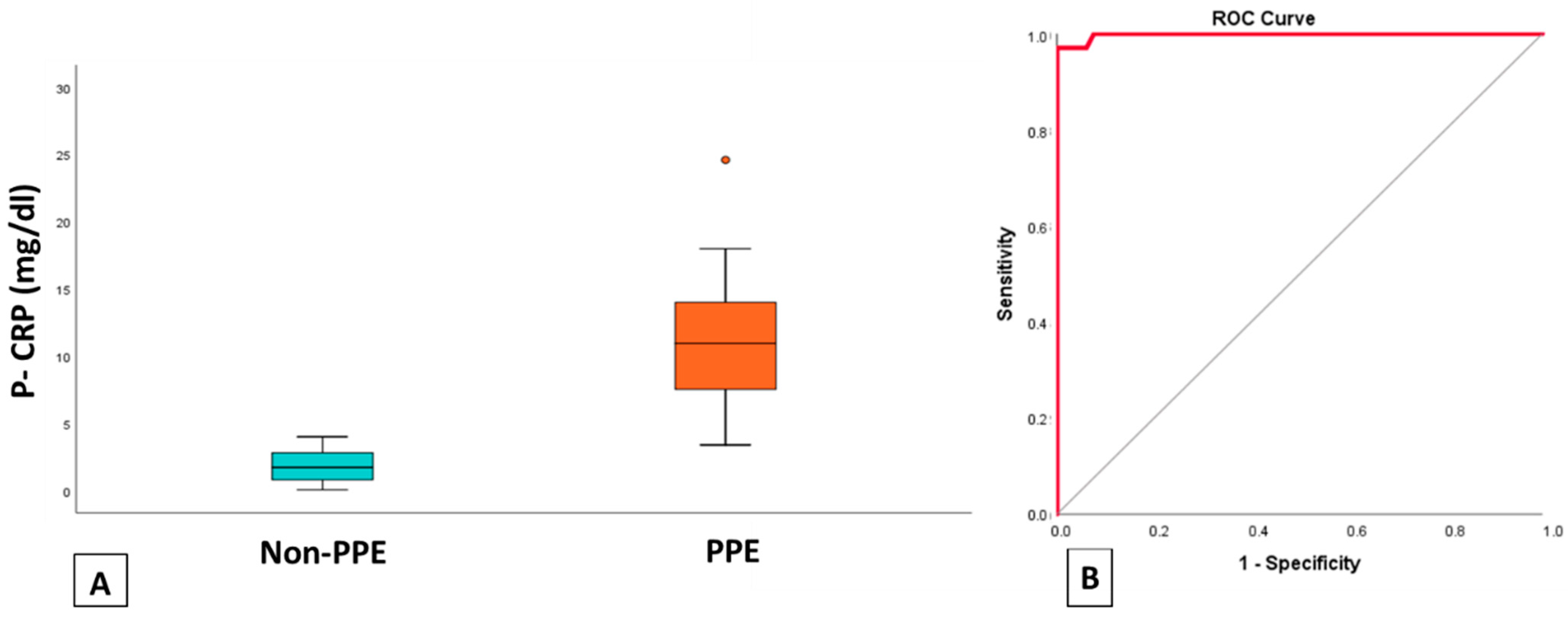
3.2. Discriminating PPE Based on p-CRP Levels
3.3. ADA Levels among MPE and Non-MPE
3.4. ADA and CRP Levels as Differentiators between PPE. MPE, TPE
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Feller-Kopman, D.; Light, R. Pleural Disease. N. Engl. J. Med. 2018, 378, 740–751. [Google Scholar] [CrossRef]
- Ashbaugh, D.G. Empyema thoracis: Factors influencing morbidity and mortality. Chest 1991, 99, 1162–1165. [Google Scholar] [CrossRef] [PubMed]
- Porcel, J.M. Pleural Fluid Biomarkers: Beyond the Light Criteria. Clin. Chest Med. 2013, 34, 27–37. [Google Scholar] [CrossRef] [PubMed]
- Izhakian, S.; Wasser, W.G.; Fox, B.D.; Vainshelboim, B.; Kramer, M.R. The diagnostic value of the pleural fluid C-reactive protein in parapneumonic effusions. Dis. Markers 2016, 2016, 7539780. [Google Scholar] [CrossRef]
- Li, D.; Shen, Y.; Qin, J.; Wan, C.; Zeng, N.; Chen, L.; Dong, Y. Diagnostic performance of C-reactive protein for parapneumonic pleural effusion: A meta-analysis. Ann. Transl. Med. 2019, 7, 1. [Google Scholar] [CrossRef] [PubMed]
- Turay, Ü.Y.; Yildirim, Z.; Türköz, Y.; Biber, Ç.; Erdogan, Y.; Keyf, A.I.; Ugurman, F.; Ayaz, A.; Ergün, P.; Harputluoglu, Y. Use of pleural fluid C-reactive protein in diagnosis of pleural effusions. Respir. Med. 2000, 94, 432–435. [Google Scholar] [CrossRef] [PubMed]
- Porcel, J.M.; Bielsa, S.; Esquerda, A.; Ruiz-González, A.; Falguera, M. Pleural fluid C-reactive protein contributes to the diagnosis and assessment of severity of parapneumonic effusions. Eur. J. Intern. Med. 2012, 23, 447–450. [Google Scholar] [CrossRef] [PubMed]
- Gopi, A.; Madhavan, S.M.; Sharma, S.K.; Sahn, S.A. Diagnosis and treatment of tuberculous pleural effusion in 2006. Chest 2007, 131, 880–889. [Google Scholar] [CrossRef]
- Kotsiou, O.S.; Tzortzi, P.; Beta, R.A.A.; Kyritsis, A.; Gourgoulianis, K.I. Repeatability of pleural adenosine deaminase measurements in diagnostic evaluation of pleural effusions. J. Clin. Lab. Anal. 2018, 32, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Light, R.W. Update on tuberculous pleural effusion. Respirology 2010, 15, 451–458. [Google Scholar] [CrossRef]
- Jiménez Castro, D.; Díaz Nuevo, G.; Pérez-Rodríguez, E.; Light, R.W. Diagnostic value of adenosine deaminase in nontuberculous lymphocytic pleural effusions. Eur. Respir. J. 2003, 21, 220–224. [Google Scholar] [CrossRef]
- Barua, R.; Hossain, M. Adenosine Deaminase in Diagnosis of Tuberculosis: A Review. Anwer Khan Mod. Med. Coll. J. 2014, 5, 43–48. [Google Scholar] [CrossRef]
- Sproston, N.R.; Ashworth, J.J. Role of C-reactive protein at sites of inflammation and infection. Front. Immunol. 2018, 9, 754. [Google Scholar] [CrossRef] [PubMed]
- Daniil, Z.D.; Zintzaras, E.; Kiropoulos, T.; Papaioannou, A.I.; Koutsokera, A.; Kastanis, A.; Gourgoulianis, K.I. Discrimination of exudative pleural effusions based on multiple biological parameters. Eur. Respir. J. 2007, 30, 957–964. [Google Scholar] [CrossRef]
- Havelock, T.; Teoh, R.; Laws, D.; Gleeson, F. Pleural procedures and thoracic ultrasound: British Thoracic Society pleural disease guideline 2010. Thorax 2010, 65 (Suppl. 2), i61–i76. [Google Scholar] [CrossRef] [PubMed]
- Suárez, P.R.; Gilart, J.F.; Pérez, J.M.H.; Serhal, M.H.; Artalejo, A.L. Treatment of complicated parapneumonic pleural effusion and pleural parapneumonic empyema. Med. Sci. Monit. 2012, 18, CR443–CR449. [Google Scholar] [CrossRef]
- Sperandeo, M.; Filabozzi, P.; Varriale, A.; Carnevale, V.; Piattelli, M.L.; Sperandeo, G.; Brunetti, E.; Decuzzi, M. Role of thoracic ultrasound in the assessment of pleural and pulmonary diseases. J. Ultrasound 2008, 11, 39–46. [Google Scholar] [CrossRef]
- Mironov, O.; Ishill, N.M.; Mironov, S.; Vargas, H.A.; Zheng, J.; Moskowitz, C.S.; Sonoda, Y.; Papas, R.S.; Chi, D.S.; Hricak, H. Pleural effusion detected at CT prior to primary cytoreduction for stage III or IV ovarian carcinoma: Effect on survival. Radiology 2011, 258, 776–784. [Google Scholar] [CrossRef]
- Na, M.J. Diagnostic tools of pleural effusion. Tuberc. Respir. Dis. 2014, 76, 199–210. [Google Scholar] [CrossRef]
- Sobhey, K.E.; Naglaa, B.A. Diagnostic significance of pleural fluid pH and pCO2. Egypt. J. Chest Dis. Tuberc. 2015, 64, 877–885. [Google Scholar] [CrossRef]
- Lee, J.; Lee, Y.H.; Seo, H.; Lee, H.; Kim, Y.K.; Yoo, S.S.; Lee, S.Y.; Cha, S.I.; Park, J.Y.; Kim, C.H. Laboratory Discrimination Between Neutrophilic Malignant and Parapneumonic Pleural Effusions. Am. J. Med. Sci. 2019, 358, 115–120. [Google Scholar] [CrossRef]
- Porcel, J.M.; Light, R.W. Diagnostic approach to pleural effusion in adults. Am. Fam. Phys. 2006, 73, 1211–1220. [Google Scholar]
- Wu, K.A.; Wu, C.C.; Liu, Y.C.; Hsueh, P.C.; Chin, C.Y.; Wang, C.L.; Chu, C.M.; Shih, L.J.; Yang, C.Y. Combined serum biomarkers in the noninvasive diagnosis of complicated parapneumonic effusions and empyema. BMC Pulm. Med. 2019, 19, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Kiropoulos, T.S.; Kostikas, K.; Oikonomidi, S.; Tsilioni, I.; Nikoulis, D.; Germenis, A.; Gourgoulianis, K.I. Acute phase markers for the differentiation of infectious and malignant pleural effusions. Respir. Med. 2007, 101, 910–918. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Yao, C.W.; Wu, B.R.; Huang, K.Y.; Chen, H.J. Adenosine deaminase activity in pleural effusions of lymphoma patients. Qjm 2014, 107, 887–893. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total Number | Percentage (%) | ||
|---|---|---|---|
| Gender | Female | 28 | 28.0 |
| Male | 72 | 72.0 | |
| Diagnosis | PPE | 34 | 34.0 |
| TPE | 7 | 7.0 | |
| MPE | 59 | 59.0 | |
| Pleural effusion size (Chest CT, portion of visualized hemithorax) | <1/3 | 23 | 23.0 |
| 1/3–2/3 | 33 | 33.0 | |
| >2/3 | 44 | 44.0 | |
| Ultrasound Image | Anechoic | 47 | 47.0 |
| Complex non-septate | 21 | 21.0 | |
| Complex septate | 26 | 26.0 | |
| Homogeneously Hyperechogenic | 6 | 6.0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Perlepe, G.; Varsamas, C.; Petinaki, E.; Antonopoulos, D.; Daniil, Z.; Gourgoulianis, K.I. Discrimination of Exudative Pleural Effusions Based on Pleural Adenosine Deaminase (ADA)-C-Reactive Protein (CRP) Levels, and Their Combination: An Observational Prospective Study. J. Pers. Med. 2021, 11, 864. https://doi.org/10.3390/jpm11090864
Perlepe G, Varsamas C, Petinaki E, Antonopoulos D, Daniil Z, Gourgoulianis KI. Discrimination of Exudative Pleural Effusions Based on Pleural Adenosine Deaminase (ADA)-C-Reactive Protein (CRP) Levels, and Their Combination: An Observational Prospective Study. Journal of Personalized Medicine. 2021; 11(9):864. https://doi.org/10.3390/jpm11090864
Chicago/Turabian StylePerlepe, Garifallia, Charalampos Varsamas, Efthymia Petinaki, Dionysios Antonopoulos, Zoe Daniil, and Konstantinos I. Gourgoulianis. 2021. "Discrimination of Exudative Pleural Effusions Based on Pleural Adenosine Deaminase (ADA)-C-Reactive Protein (CRP) Levels, and Their Combination: An Observational Prospective Study" Journal of Personalized Medicine 11, no. 9: 864. https://doi.org/10.3390/jpm11090864
APA StylePerlepe, G., Varsamas, C., Petinaki, E., Antonopoulos, D., Daniil, Z., & Gourgoulianis, K. I. (2021). Discrimination of Exudative Pleural Effusions Based on Pleural Adenosine Deaminase (ADA)-C-Reactive Protein (CRP) Levels, and Their Combination: An Observational Prospective Study. Journal of Personalized Medicine, 11(9), 864. https://doi.org/10.3390/jpm11090864