
Implementing Pharmacogenomics Testing: Single Center Experience at Arkansas Children’s Hospital


 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Adoption of PGx-Patient and Physician Interest Survey
2.2. Pharmacy Records Data Extraction
2.3. Selection and Generation of PGx Panel
2.3.1. Real-Time PCR Instrument and OpenArray® Panel Analytical Validation
2.3.2. PGx OpenArray® and CNV Assay Validation
2.4. Build of Genomic Indicators in EPIC
3. Results
3.1. Pharmacogenomics Program at ACH
3.1.1. Patient and Physician Interest Survey
3.1.2. ACH Pharmacy Records Review
3.1.3. PGx Assay Performance
3.1.4. Integrating PGx into EHR with CDS
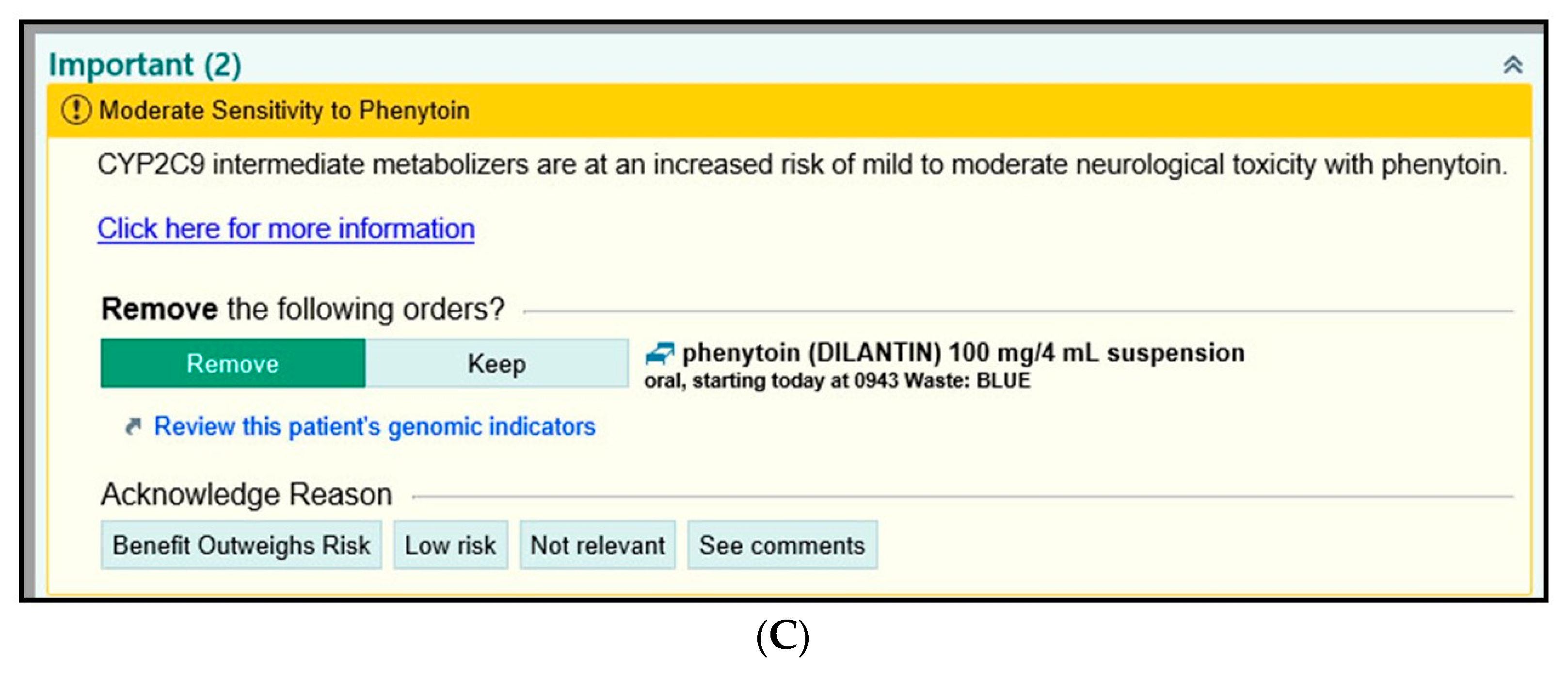
3.1.5. Examples of BPAs in EPIC
4. Discussion
4.1. Clinical Utility of Pharmacogenomics
4.2. PGx Programs at Other Pediatric Medical Centers
4.3. EHR-Based Clinical Decision Support Systems (CDSS)
4.4. Challenges and Barriers to PGx Implementation
4.4.1. Education of Future Clinicians on PGx
4.4.2. Consent/Parent Awareness
4.4.3. Cost of PGx Test
4.4.4. Test Reimbursement
4.5. Integration of PGx Test Results into EPIC
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Nebert, D.W. Pharmacogenetics and pharmacogenomics: Why is this relevant to the clinical geneticist? Clin. Genet. 1999, 56, 247–258. [Google Scholar] [CrossRef]
- Sunshine, J.E.; Meo, N.; Kassebaum, N.J.; Collison, M.L.; Mokdad, A.H.; Naghavi, M. Association of Adverse Effects of Medical Treatment with Mortality in the United States: A Secondary Analysis of the Global Burden of Diseases, Injuries, and Risk Factors Study. JAMA Netw. Open 2019, 2, e187041. [Google Scholar] [CrossRef]
- U.S. FDA. Preventable Adverse Drug Reactions: A Focus on Drug Interactions. Available online: https://www.fda.gov/drugs/drug-interactions-labeling/preventable-adverse-drug-reactions-focus-drug-interactions (accessed on 1 March 2021).
- Kongkaew, C.; Noyce, P.R.; Ashcroft, D.M. Hospital admissions associated with adverse drug reactions: A systematic review of prospective observational studies. Ann. Pharmacother. 2008, 42, 1017–1025. [Google Scholar] [CrossRef]
- Giacomini, K.M.; Yee, S.W.; Ratain, M.J.; Weinshilboum, R.M.; Kamatani, N.; Nakamura, Y. Pharmacogenomics and patient care: One size does not fit all. Sci. Transl. Med. 2012, 4, 153ps18. [Google Scholar] [CrossRef] [PubMed]
- Lander, E.S.; Linton, L.M.; Birren, B.; Nusbaum, C.; Zody, M.C.; Baldwin, J.; Devon, K.; Dewar, K.; Doyle, M.; FitzHugh, W.; et al. Initial sequencing and analysis of the human genome. Nature 2001, 409, 860–921. [Google Scholar]
- International HapMap Consortium. A second generation human haplotype map of over 3.1 million SNPs. Nature 2007, 449, 851. [Google Scholar] [CrossRef]
- 1000 Genomes Project Consortium. A global reference for human genetic variation. Nature 2015, 526, 68–74. [Google Scholar] [CrossRef]
- Pirmohamed, M. Pharmacogenetics and pharmacogenomics. Br. J. Clin. Pharmacol. 2001, 52, 345–347. [Google Scholar] [CrossRef]
- Van Driest, S.L.; McGregor, T.L. Pharmacogenetics in clinical pediatrics: Challenges and strategies. Personal. Med. 2013, 10, 661–671. [Google Scholar] [CrossRef]
- Ramsey, L.B.; Prows, C.A.; Zhang, K.; Saldana, S.N.; Sorter, M.T.; Pestian, J.P.; Wenstrup, R.J.; Vinks, A.A.; Glauser, T.A. Implementation of pharmacogenetics at Cincinnati Children’s hospital medical center: Lessons learned over 14 years of personalizing medicine. Clin. Pharmacol. Ther. 2019, 105, 49–52. [Google Scholar] [CrossRef]
- NHGRI. The National Human Genome Research Institute (NHGRI) Sponsored Its 10th Genomic Medicine Meeting—Genomic Medicine X; NHGRI: Silver Spring, MD, USA, 2017. Available online: https://www.genome.gov/27568408/genomic-medicine-x-research-directions-in-pharmacogenomics-implementation (accessed on 1 March 2021).
- Hicks, J.K.; Sangkuhl, K.J.J.; Swen, J.J.; Ellingrod, V.L.; Muller, D.J.; Shimoda, K.; Bishop, J.R.; Kharasch, E.D.; Skaar, T.C.; Gaedigk, A.; et al. Clinical pharmacogenetics implementation consortium guideline (CPIC) for CYP2D6 and CYP2C19 genotypes and dosing of tricyclic antidepressants: 2016 update. Clin. Pharmacol. Ther. 2017, 102, 37–44. [Google Scholar] [CrossRef]
- U.S. FDA. Available online: https://www.fda.gov/medical-devices/precision-medicine/table-pharmacogenetic-associations (accessed on 1 March 2021).
- CPIC. Available online: https://cpicpgx.org/guidelines/ (accessed on 1 March 2021).
- DPWG. Available online: https://upgx.eu/guidelines/ (accessed on 1 March 2021).
- PharmGKB. Available online: http://www.pharmgkb.org (accessed on 1 March 2021).
- Gatter, K. FDA oversight of laboratory-developed tests: Where are we now? Arch. Pathol. Lab. Med. 2017, 141, 746–748. [Google Scholar] [CrossRef] [PubMed]
- Genzen, J.R.; Mohlman, J.S.; Lynch, J.L.; Squires, M.E.; Weiss, R.L. Laboratory-Developed Tests: A Legislative and Regulatory Review. Clin. Chem. 2017, 63, 1575–1584. [Google Scholar] [CrossRef] [PubMed]
- CLIA’88. Available online: https://www.govinfo.gov/content/pkg/STATUTE-102/pdf/STATUTE-102-Pg2903.pdf (accessed on 1 March 2021).
- Scott, S.A.; Sangkuhl, K.C.M.; Stein, C.M.; Hulot, J.-S.; Roden, D.M.; Klein, T.E.; Sabatine, M.S.; Johnson, J.A.; Shuldiner, A.R. Clinical Pharmacogenetics Implementation Consortium guidelines for CYP2C19 genotype and clopidogrel therapy. Clin. Pharmacol. Ther. 2013, 94, 317–323. [Google Scholar] [CrossRef]
- Relling, M.V.; Schwab, M.; Whirl-Carrillo, M.; Suarez-Kurtz, G.; Pui, C.-H.; Stein, C.M.; Moyer, A.M.; Evans, W.E.; Klein, T.E.; Antillon-Klussmann, F.G.; et al. Clinical Pharmacogenetics Implementation Consortium Guideline for Thiopurine Dosing Based on TPMT and NUDT15 Genotypes: 2018 Update. Clin. Pharmacol. Ther. 2019, 105, 1095–1105. [Google Scholar] [CrossRef]
- Karnes, J.H.; Rettie, A.E.; Somogyi, A.A.; Huddart, R.; Fohner, A.E.; Formea, C.M.; Ta, M.L.M.; Llerna, A.; Whirl-Carrillo, M.; Klein, T.E.; et al. Clinical Pharmacogenetics Implementation Consortium (CPIC) Guideline for CYP2C9 and HLA-B Genotypes and Phenytoin Dosing: 2020 Update. Clin. Pharmacol. Ther. 2021, 109, 302–309. [Google Scholar] [CrossRef] [PubMed]
- O’Kane, D.J.; Weinshilboum, R.M.; Moyer, T.P. Pharmacogenomics and reducing the frequency of adverse drug events. Pharmacogenomics 2003, 4, 1–4. [Google Scholar] [CrossRef]
- Elzagallaai, A.A.; Greff, M.; Rieder, M.J. Adverse Drug Reactions in Children: The Double-Edged Sword of Therapeutics. Clin. Pharmacol. Ther. 2017, 101, 725–735. [Google Scholar] [CrossRef]
- Weinshilboum, R.M.; Wang, L. Pharmacogenomics: Precision Medicine and Drug Response. Mayo Clin. Proc. 2017, 92, 1711–1722. [Google Scholar] [CrossRef]
- U.S. FDA. Available online: https://www.fda.gov/drugs/information-consumers-and-patients-drugs/drug-research-and-children (accessed on 1 March 2021).
- Hines, R. The ontogeny of drug metabolism enzymes and implications for adverse drug events. Pharmacol. Ther. 2008, 118, 250–267. [Google Scholar] [CrossRef]
- Ramsey, L.B.; Namerow, L.B.; Bishop, J.R.; Hicks, J.K.; Bousman, C.; Croarkin, P.E.; Mathews, C.A.; Van Driest, S.L.; Strawn, J.R. Thoughtful Clinical Use of Pharmacogenetics in Child and Adolescent Psychopharmacology. J. Am. Acad. Child Adolesc. Psychiatry 2020. [Google Scholar] [CrossRef] [PubMed]
- De Wildt, S.N.; Tibboel, D.; Leeder, J.S. Drug metabolism for the paediatrician. Arch. Dis. Child. 2014, 99, 1137–1142. [Google Scholar] [CrossRef]
- Serpe, L.; Calvo, P.L.; Muntoni, E.; D’Antico, S.; Giaccone, M.; Avagnina, A.; Baldi, M.; Barbera, C.; Curti, F.; Pera, A.; et al. Thiopurine S-methyltransferase pharmacogenetics in a large-scale healthy Italian-Caucasian population: Differences in enzyme activity. Pharmacogenomics 2009, 10, 1753–1765. [Google Scholar] [CrossRef] [PubMed]
- Bielinski, S.J.; Olson, J.E.; Pathak, J.; Weinshilboum, R.M.; Wang, L.; Lyke, K.J.; Ryu, E.; Targonski, P.V.; Van Norstrand, M.D.; Hathcock, M.A.; et al. Preemptive genotyping for personalized medicine: Design of the right drug, right dose, right time-using genomic data to individualize treatment protocol. Mayo Clin. Proc. 2014, 89, 25–33. [Google Scholar] [CrossRef]
- Van Driest, S.L.; Shi, Y.; Bowton, E.A.; Schildcrout, J.S.; Peterson, J.F.; Pulley, J.; Denny, J.C.; Roden, D.M. Clinically actionable genotypes among 10,000 patients with preemptive pharmacogenomic testing. Clin. Pharmacol. Ther. 2014, 95, 423–431. [Google Scholar] [CrossRef] [PubMed]
- Ramsey, L.B.; Brown, J.T.; Vear, S.I.; Bishop, J.R.; Van Driest, S.L. Gene-Based Dose Optimization in Children. Annu. Rev. Pharmacol. Toxicol. 2020, 60, 311–331. [Google Scholar] [CrossRef] [PubMed]
- Personalized Medicine Coalition. Available online: http://www.personalizedmedicinecoalition.org/News/Press_Releases/New_Personalized_Medicine_Report_Shows_RecordSetting_Growth_to_286_in_Number_of_Personalized_Medicines_Available_Documents_Challenges_in_Regulation_Reimbursement_Clinical_Adoption (accessed on 1 March 2021).
- Hoffman, J.M.; Haidar, C.E.; Wilkinson, M.R.; Crews, K.R.; Baker, D.K.; Kornegay, N.M.; Yang, W.; Pui, C.H.; Reiss, U.M.; Gaur, A.H.; et al. PG4KDS: A Model for the Clinical Implementation of Pre-emptive Pharmacogenetics. Am. J. Med. Genet. Part C Semin. Med. Genet. 2014, 1, 45–55. [Google Scholar] [CrossRef]
- Pulley, J.M.; Denny, J.C.; Peterson, J.F.; Bernard, G.R.; Vnencak-Jones, C.L.; Ramirez, A.H.; Delaney, J.T.; Bowton, E.; Brothers, K.; Johnson, K.; et al. Operational Implementation of Prospective Genotyping for Personalized Medicine: The Design of the Vanderbilt PREDICT Project. Clin. Pharmacol. Ther. 2012, 1, 87–95. [Google Scholar] [CrossRef]
- Gregornik, D.; Salyakina, D.; Brown, M.; Roiko, S.; Ramos, K. Pediatric pharmacogenomics: Challenges and opportunities: On behalf of the Sanford Children’s Genomic Medicine Consortium. Pharm. J. 2021, 21, 8–19. [Google Scholar] [CrossRef]
- Dunnenberger, H.M.; Biszewski, M.; Bell, G.C.; Sereika, A.; May, H.; Johnson, S.G.; Hulick, P.J.; Khandekar, J. Implementation of a multidisciplinary pharmacogenomics clinic in a community health system. Am. J. Health Syst. Pharm. 2016, 73, 1956–1966. [Google Scholar] [CrossRef]
- Haga, S.B. Pharmacogenomic Testing in Pediatrics: Navigating the Ethical, Social, And Legal Challenges. Pharmgenomics Pers. Med. 2019, 12, 273–285. [Google Scholar] [CrossRef] [PubMed]
- Giri, J.; Moyer, A.M.; Bielinski, S.J.; Caraballo, P.J. Concepts Driving Pharmacogenomics Implementation into Everyday Healthcare. Pharmgenomics Pers. Med. 2019, 12, 305–318. [Google Scholar] [CrossRef] [PubMed]
- Cicali, E.J.; Weitzel, K.W.; Elsey, A.R.; Orlando, F.A.; Vinson, M.; Mosley, S.; Smith, D.M.; Davis, R.; Drum, L.; Estores, D.; et al. Challenges and lessons learned from clinical pharmacogenetic implementation of multiple gene-drug pairs across ambulatory care settings. Genet. Med. 2019, 21, 2264–2274. [Google Scholar] [CrossRef] [PubMed]
- Basyouni, D.; Shatnawi, A. Pharmacogenomics Instruction Depth, Extent, and Perception in US Medical Curricula. J. Med. Educ. Curric. Dev. 2020, 7. [Google Scholar] [CrossRef] [PubMed]
- Guy, J.W.; Patel, I.; Oestreich, J.H. Clinical Application and Educational Training for Pharmacogenomics. Pharmacy 2020, 8, 163. [Google Scholar] [CrossRef] [PubMed]
- Coriolan, S.; Arikawe, N.; Arden Moscati, A.; Zhou, L.; Dyn, S.; Donmez, S.; Garba, A.; Falbaum, S.; Loewy, Z.; Lull, M.; et al. Pharmacy students’ attitudes and perceptions toward pharmacogenomics education. Am. J. Health Syst. Pharm. 2019, 76, 836–845. [Google Scholar] [CrossRef]
- Lose, E.J. The emerging role of primary care in genetics. Curr. Opin. Pediatr. 2008, 20, 634–638. [Google Scholar] [CrossRef]
- Green, E.D.; Guyer, M.S. Charting a course for genomic medicine from base pairs to bedside. Nature 2011, 470, 204–213. [Google Scholar] [CrossRef] [PubMed]
- Schrijver, I.; Aziz, N.; Farkas, D.H.; Furtado, M.; Gonzalez, A.F.; Greiner, T.C.; Grody, W.W.; Hambuch, T.; Kalman, L.; Kant, J.A.; et al. Opportunities and challenges associated with clinical diagnostic genome sequencing: A report of the Association for Molecular Pathology. J. Mol. Diagn. 2012, 14, 525–540. [Google Scholar] [CrossRef]
- Liko, I.; Lee, Y.M.; Stutzman, D.L.; Blackmer, A.B.; Deininger, K.M.; Reynolds, A.M.; Aquilante, C.L. Providers’ perspectives on the clinical utility of pharmacogenomic testing in pediatric patients. Pharmacogenomics 2021, 22, 263–274. [Google Scholar] [CrossRef]
- Porter-Gill, P.A.; Gill, P.; Schaefer, G.B.; Allen, J.; Boyanton, B.L.; Yu, F. Arkansas Physicians’ Interests and learning opportunities with Pharmacogenomics. J. Ark. Med. Soc. 2021, in press. [Google Scholar]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Drug Name | Gene/s | Total | Drug Name | Gene/s | Total |
|---|---|---|---|---|---|
| Amikacin | MT-RNR1 | 6 | Hydrocodone | CYP2D6 | 303 |
| Amitriptyline | CYP2C19, CYP2D6 | 1382 | Imipramine | CYP2C19, CYP2D6 | 190 |
| Aripiprazole | CYP2D6 | 24 | Mercaptopurine | TPMT, NUDT15 | 809 |
| Atazanavir | UGT1A1 | 3 | Neomycin | MT-RNR1 | 33 |
| Atomoxetine | CYP2D6 | 59 | Nortriptyline | CYP2D6 | 147 |
| Azathioprine | TPMT, NUDT15 | 116 | Ondansetron | CYP2D6 | 21,147 |
| Celecoxib | CYP2C9 | 55 | Oxybutynin | NA | 795 |
| Cisplatin | ACYP2 | 59 | Oxycodone | CYP2D6 | 12,978 |
| Citalopram | CYP2C19 | 21 | Paroxetine | CYP2D6 | 5 |
| Clomipramine | CYP2C19, CYP2D6 | 1 | Phenytoin | CYP2C9 | 31 |
| Clopidogrel | CYP2C19 | 16 | Pimozide | CYP2D6 | 9 |
| Doxepin | CYP2C19, CYP2D6 | 11 | Salmeterol | ADRB2 | 224 |
| Eltrombopag | F5 | 7 | Sertraline | CYP2C19 | 271 |
| Escitalopram | CYP2C19 | 46 | Simvastatin | CYP3A4, SLCO1B1 | 24 |
| Fluorouracil | DDYD | 9 | Tacrolimus | CYP3A5 | 463 |
| Fluoxetine | CYP2D6 | 197 | Thioguanine | TPMT, NUDT15 | 36 |
| Fluvoxamine | CYP2D6 | 11 | Tobramycin | MT-RNR1 | 61 |
| Formoterol | ADRB2 | 995 | Tramadol | CYP2D6 | 90 |
| Fosphenytoin | CYP2C9 | 113 | Vincristine | CEP72 | 1528 |
| Gentamicin | MT-RNR1 | 258 | Voriconazole | CYP2C19 | 31 |
| Warfarin | CYP2C9, VKORC1, CYP2C, DYP4F2 | 313 |
| PGx 174 SNP Panel | ||
|---|---|---|
| Gene | No. of SNPs | SNP rs# |
| ACYP2 | 1 | rs1872328 |
| CACNA1S | 2 | rs772226819, rs1800559 |
| CEP72 | 1 | rs924607 |
| CYP2C | 1 | rs12777823 |
| CYP2C19 | 12 | rs12769205, rs12248560, rs17884712, rs72552267, rs4986893, rs56337013, rs72558186, rs6413438, rs58973490, rs41291556, rs28399504, rs4244285 |
| CYP2C9 | 13 | rs72558193, rs72558189, rs2256871, rs7900194, rs1799853, rs1057910, rs28371686, rs9332239, rs56165452, rs28371685, rs9332131, rs72558187, rs72558190 |
| CYP2D6 | 42 | rs730882170, rs28371710, rs1135822, rs267608319, rs28371696, rs267608279, rs16947, rs35742686, rs72549352, rs61736512adjC, rs61736512, rs148769737, rs148769737, rs267608297, rs267608313, rs28371706, rs1065852, rs1135840, rs3892097, rs769258, rs5030862, rs201377835, rs5030867, hCV32407220, rs72549349, rs5030656, rs72549351, rs72549353, rs28371717, rs72549356, rs5030655, rs774671100, rs1080985, rs59421388, rs72549348, rs28371725, rs72549346, rs72549347, rs1135823, rs5030865, rs5030865, rs730882251 |
| CYP3A4 | 5 | rs4986910, rs4987161, rs12721629, rs55785340, rs35599367 |
| CYP3A5 | 3 | rs776746, rs10264272, rs41303343 |
| CYP4F2 | 1 | rs2108622 |
| DPYD | 22 | rs75017182, rs3918289, rs3918289, rs1801159, rs1801158, rs1801268, rs1801267, rs1801266, rs1801265, rs1801160, rs55886062, rs2297595, rs17376848, rs56038477, rs67376798, rs6670886, rs3918290, rs72549309, rs72549306, rs72549310, rs80081766, rs115232898 |
| F2 | 1 | rs1799963 |
| F5 | 1 | rs6025 |
| G6PD | 11 | rs137852328, rs72554665, rs72554665, rs137852328, rs78478128, rs1050828, rs1050829, rs5030868, rs137852339, rs76723693, rs5030869 |
| NUDT15 | 3 | rs766023281, rs116855232, s186364861 |
| RARG | 1 | rs2229774 |
| RYR1 | 41 | rs118192163, rs28933396, rs118192176, rs193922770, rs144336148, rs118192162, rs118192116, rs121918592, rs1801086, rs118192161, rs28933397, rs63749869, rs121918594, rs118192170, rs193922802, rs118192167, rs121918595, rs118192168, rs121918593, rs118192124, rs118192122, rs118192175, rs118192172, rs111888148, rs112563513, rs118192178, rs121918596, rs193922747, rs193922748, rs193922753, rs193922764, rs193922768, rs193922772, rs193922803, rs193922807, rs193922816, rs193922818, rs193922832, rs193922843, rs193922876, rs193922878 |
| SLC28A3 | 1 | rs7853758 |
| SLCO1B1 | 1 | rs4149056 |
| TPMT | 5 | rs1142345, rs56161402, rs1800584, rs1800462, rs1800460 |
| UGT1A1 | 3 | rs4148323, rs35350960, rs887829 |
| UGT1A6 | 1 | rs17863783 |
| VKORC1 | 1 | rs9923231 |
| ID | Title | Indicators | Ordinal Value | Meaning | Logic |
|---|---|---|---|---|---|
| 882001281 | Decreased Amitriptyline Exposure | 87005959 | 1 | Amitryptyline Prescribed | 1 AND ((2 AND 3) OR (3 AND 4)) |
| 873000170 | 2 | CYP2C19 Poor Metabolizer | |||
| 873000181 | 3 | CYP2D6 Rapid Metabolizer | |||
| 873001569 | 4 | CYP2C19 Poor Metabolizer |
| Condition | Drug | Gene/s |
|---|---|---|
| Anesthesia | Desflurane | RYR1/CACNA1S |
| Enflurane | RYR1/CACNA1S | |
| Halothane | RYR1/CACNA1S | |
| Isoflurane | RYR1/CACNA1S | |
| Sevoflurane | RYR1/CACNA1S | |
| Succinycholine | RYR1/CACNA1S | |
| Cancer | Azathioprine | TPMT/NUDT15 |
| Capecitabine | DPYD | |
| Cisplatin | ACYP2 | |
| Daunorubicin | RARG/UGT1A6/SLC28A3 | |
| Doxorubicin | RARG/UGT1A6/SLC28A3 | |
| Fluorouracil | DPYD | |
| Mercaptopurine | TPMT/NUDT15 | |
| Rasburicase | G6PD | |
| Thioguanine | TPMT/NUDT15 | |
| Vincristine | CEP72 | |
| Cardiovascular | Clopidogrel | CYP2C19 |
| Propranolol | CYP2D6 | |
| Simvastatin | CYP3A4/SLCO1B1 | |
| Warfarin | CYP2C9/VKORC1/CYP2C/CYP4F2 | |
| Gastrointestinal (GI) | Dexlanosoprazole | CYP2C19 |
| Esomeprazole | CYP2C19 | |
| Lansoprazole | CYP2C19 | |
| Omeprazole | CYP2C19 | |
| Ondansetron | CYP2D6 | |
| Pantoprazole | CYP2C19 | |
| Rabeprazole | CYP2C19 | |
| Gaucher Disease | Eliglustat | CYP2D6 |
| Hematology | Eltrombopag | F5 |
| Infectious Disease | Atazanavir | UGT1A1 |
| Chloroquine | G6PD | |
| Dapsone | G6PD | |
| Nitrofurantoin | G6PD | |
| Primaquine | G6PD | |
| Proguanil | CYP2c19 | |
| Quinine | G6PD | |
| Sulfamethoxazole | G6PD | |
| Tafenoquine | G6PD | |
| Voriconazole | CYP2C19 | |
| Neurology | Fosphenytoin | CYP2C9 |
| Phenytoin | CYP2C9 | |
| Pain | Celecoxib | CYP2C9 |
| Codeine | CYP2D6 | |
| Hydrocodone | CYP2D6 | |
| Ibuprofen | CYP2C9 | |
| Meloxicam | CYP2C9 | |
| Oxycodone | CYP2D6 | |
| Tramadol | CYP2D6 | |
| Psychiatry and Addiction Medicine | Amitriptyline | CYP2C19/CYP2D6 |
| Aripiprazole | CYP2D6 | |
| Atomoxetine | CYP2D6 | |
| Citalopram | CYP2C19 | |
| Clomipramine | CYP2C19/CYP2D6 | |
| Desipramine | CYP2D6 | |
| Doxepin | CYP2C19/CYP2D6 | |
| Escitalopram | CYP2C19 | |
| Fluoxetine | CYP2D6 | |
| Fluvoxamine | CYP2D6 | |
| Iloperidone | CYP2D6 | |
| Imipramine | CYP2C19/CYP2D6 | |
| Nortriptyline | CYP2D6 | |
| Paroxetine | CYP2D6 | |
| Pimozide | CYP2D6 | |
| Sertraline | CYP2C19 | |
| Trimipramine | CYP2C19/CYP2D6 | |
| Transplantation | Tacrolimus | CYP3A5 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gill, P.S.; Yu, F.B.; Porter-Gill, P.A.; Boyanton, B.L.; Allen, J.C.; Farrar, J.E.; Veerapandiyan, A.; Prodhan, P.; Bielamowicz, K.J.; Sellars, E.; et al. Implementing Pharmacogenomics Testing: Single Center Experience at Arkansas Children’s Hospital. J. Pers. Med. 2021, 11, 394. https://doi.org/10.3390/jpm11050394
Gill PS, Yu FB, Porter-Gill PA, Boyanton BL, Allen JC, Farrar JE, Veerapandiyan A, Prodhan P, Bielamowicz KJ, Sellars E, et al. Implementing Pharmacogenomics Testing: Single Center Experience at Arkansas Children’s Hospital. Journal of Personalized Medicine. 2021; 11(5):394. https://doi.org/10.3390/jpm11050394
Chicago/Turabian StyleGill, Pritmohinder S., Feliciano B. Yu, Patricia A. Porter-Gill, Bobby L. Boyanton, Judy C. Allen, Jason E. Farrar, Aravindhan Veerapandiyan, Parthak Prodhan, Kevin J. Bielamowicz, Elizabeth Sellars, and et al. 2021. "Implementing Pharmacogenomics Testing: Single Center Experience at Arkansas Children’s Hospital" Journal of Personalized Medicine 11, no. 5: 394. https://doi.org/10.3390/jpm11050394
APA StyleGill, P. S., Yu, F. B., Porter-Gill, P. A., Boyanton, B. L., Allen, J. C., Farrar, J. E., Veerapandiyan, A., Prodhan, P., Bielamowicz, K. J., Sellars, E., Burrow, A., Kennedy, J. L., Clothier, J. L., Becton, D. L., Rule, D., & Schaefer, G. B. (2021). Implementing Pharmacogenomics Testing: Single Center Experience at Arkansas Children’s Hospital. Journal of Personalized Medicine, 11(5), 394. https://doi.org/10.3390/jpm11050394