
Custom Made Monoflange Acetabular Components for the Treatment of Paprosky Type III Defects

 ,
, 
Abstract
1. Introduction
2. Methods
2.1. Patient Selection
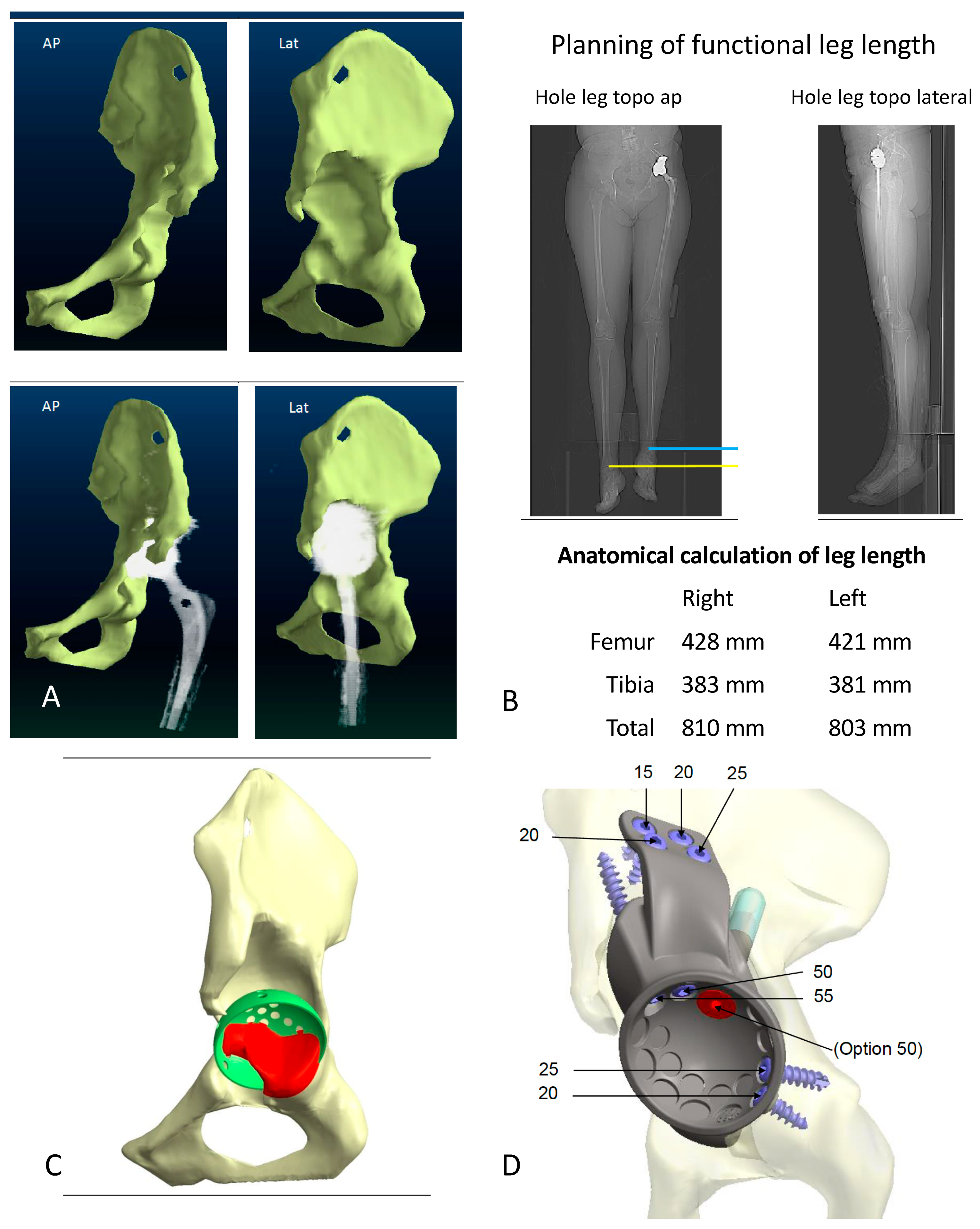
2.2. Implant
2.3. Parameters Assessed
2.4. Patients
2.5. Statistics
3. Results
3.1. Intraoperative Parameters
3.2. Perioperative Complications
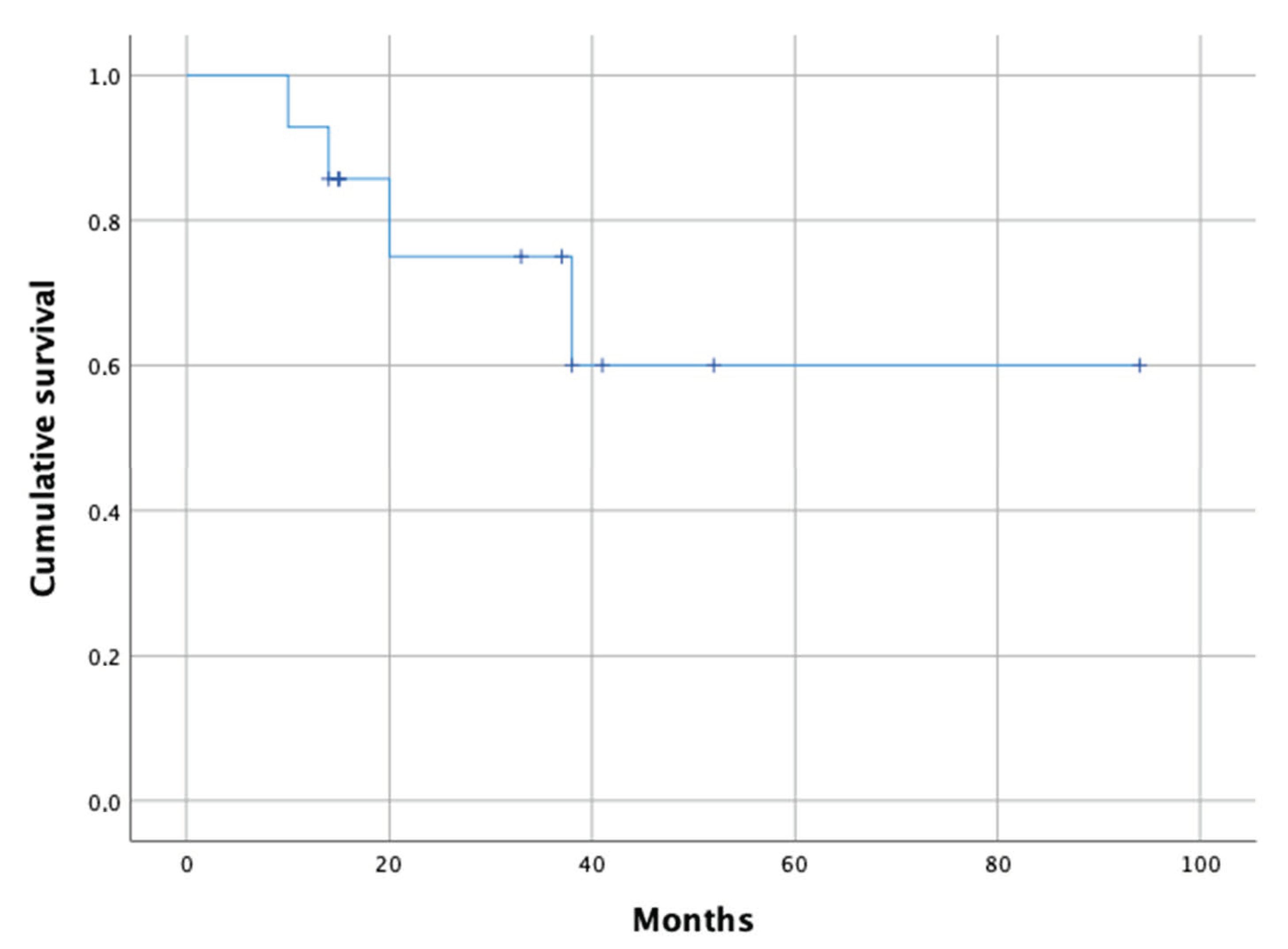
3.3. Failures
3.4. Function
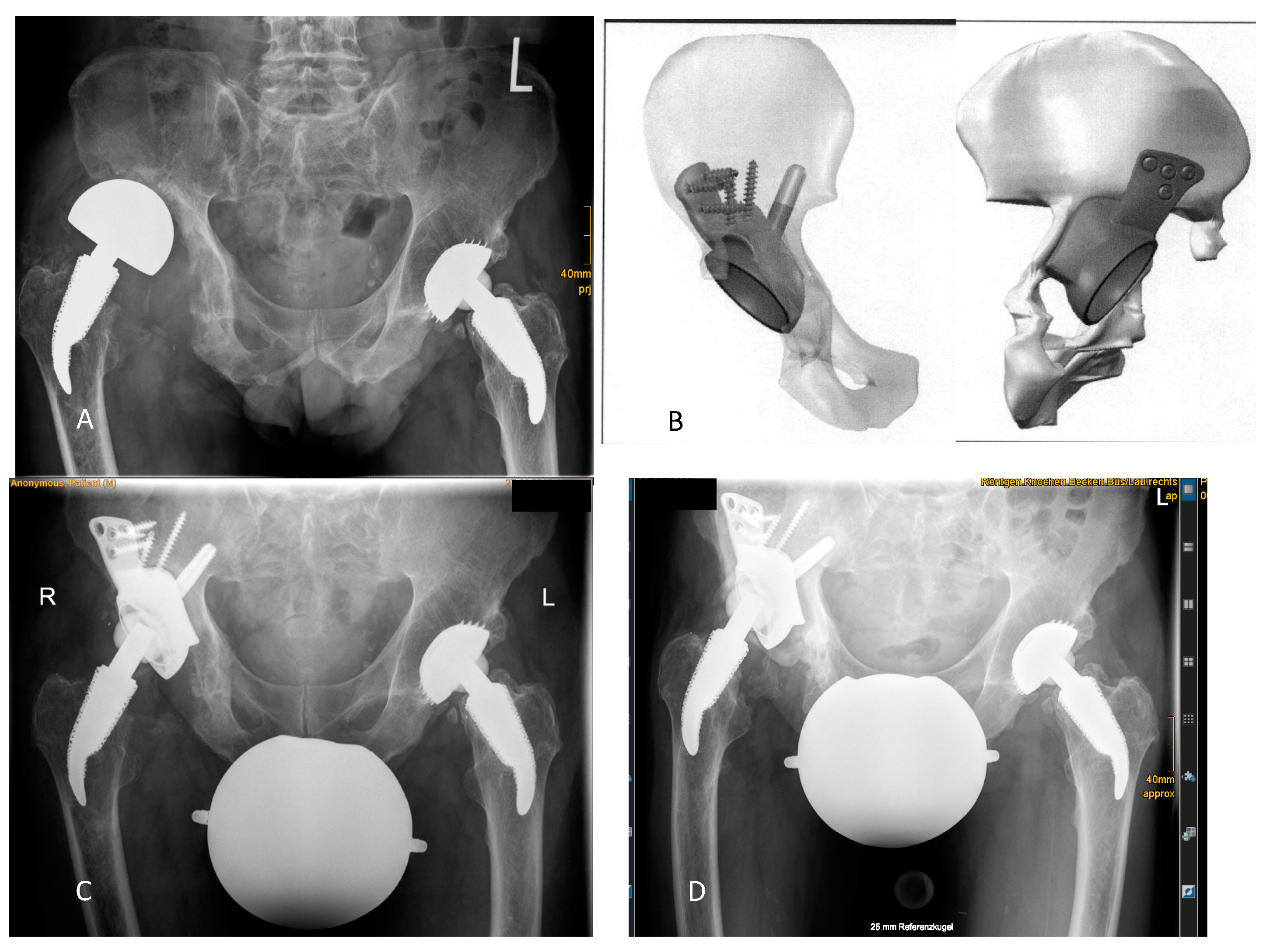
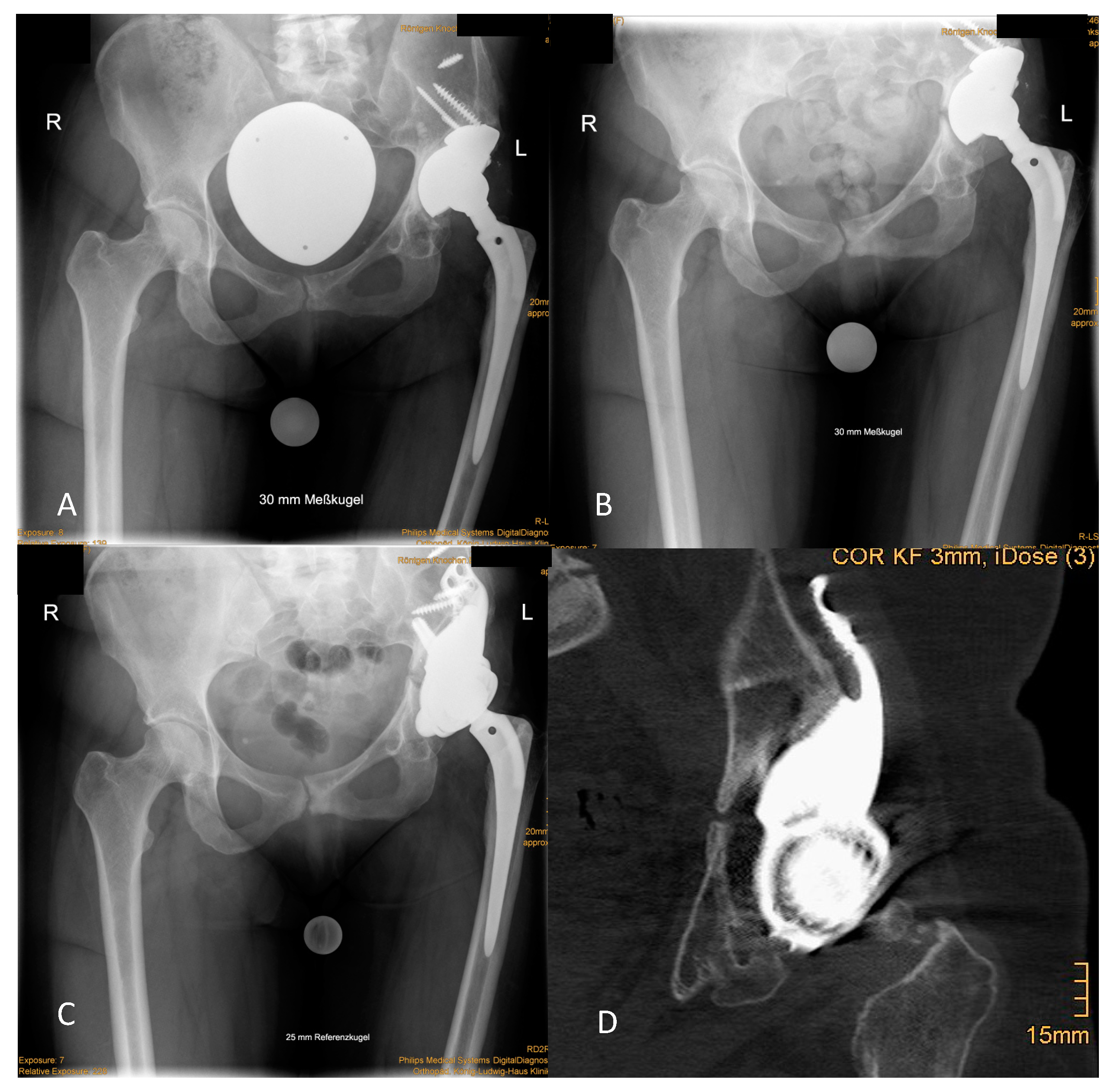
3.5. Radiographic Evaluation
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bozic, K.J.; Kamath, A.F.; Ong, K.; Lau, E.; Kurtz, S.; Chan, V.; Vail, T.P.; Rubash, H.; Berry, D.J. Comparative Epidemiology of Revision Arthroplasty: Failed THA Poses Greater Clinical and Economic Burdens Than Failed TKA. Clin. Orthop. Relat. Res. 2015, 473, 2131–2138. [Google Scholar] [CrossRef] [PubMed]
- Makita, H.; Kerboull, M.; Inaba, Y.; Tezuka, T.; Saito, T.; Kerboull, L. Revision Total Hip Arthroplasty Using the Kerboull Acetabular Reinforcement Device and Structural Allograft for Severe Defects of the Acetabulum. J. Arthroplast. 2017, 32, 3502–3509. [Google Scholar] [CrossRef]
- Hoberg, M.; Holzapfel, B.M.; Steinert, A.F.; Kratzer, F.; Walcher, M.; Rudert, M. Treatment of acetabular bone defects in revision hip arthroplasty using the Revisio-System. Orthopade 2017, 46, 126–132. [Google Scholar] [CrossRef]
- Prodinger, P.M.; Lazic, I.; Horas, K.; Burgkart, R.; von Eisenhart-Rothe, R.; Weissenberger, M.; Rudert, M.; Holzapfel, B.M. Revision Arthroplasty Through the Direct Anterior Approach Using an Asymmetric Acetabular Component. J. Clin. Med. 2020, 9, 3031. [Google Scholar] [CrossRef] [PubMed]
- Rudert, M.; Holzapfel, B.M.; Kratzer, F.; Gradinger, R. Standardized reconstruction of acetabular bone defects using the cranial socket system. Oper. Orthop. Traumatol. 2010, 22, 241–255. [Google Scholar] [CrossRef]
- Wassilew, G.I.; Janz, V.; Perka, C.; Muller, M. Treatment of acetabular defects with the trabecular metal revision system. Orthopade 2017, 46, 148–157. [Google Scholar] [CrossRef]
- Frenzel, S.; Horas, K.; Rak, D.; Boelch, S.P.; Rudert, M.; Holzapfel, B.M. Acetabular Revision With Intramedullary and Extramedullary Iliac Fixation for Pelvic Discontinuity. J. Arthroplast. 2020. [Google Scholar] [CrossRef]
- Burastero, G.; Cavagnaro, L.; Chiarlone, F.; Zanirato, A.; Mosconi, L.; Felli, L.; de Lorenzo, F.D.R. Clinical study of outcomes after revision surgery using porous titanium custom-made implants for severe acetabular septic bone defects. Int. Orthop. 2020, 44, 1957–1964. [Google Scholar] [CrossRef]
- Von Lewinski, G. Custom-made acetabular implants in revision total hip arthroplasty. Orthopade 2020, 49, 417–423. [Google Scholar] [CrossRef] [PubMed]
- De Martino, I.; Strigelli, V.; Cacciola, G.; Gu, A.; Bostrom, M.P.; Sculco, P.K. Survivorship and Clinical Outcomes of Custom Triflange Acetabular Components in Revision Total Hip Arthroplasty: A Systematic Review. J. Arthroplast. 2019, 34, 2511–2518. [Google Scholar] [CrossRef]
- Horas, K.; Arnholdt, J.; Steinert, A.F.; Hoberg, M.; Rudert, M.; Holzapfel, B.M. Acetabular defect classification in times of 3D imaging and patient-specific treatment protocols. Orthopade 2017, 46, 168–178. [Google Scholar] [CrossRef]
- Schofer, M.D.; Pressel, T.; Heyse, T.J.; Schmitt, J.; Boudriot, U. Radiological determination of the anatomic hip centre from pelvic landmarks. Acta Orthop. Belg. 2010, 76, 479–485. [Google Scholar] [PubMed]
- Abrahams, J.M.; Kim, Y.S.; Callary, S.A.; De Ieso, C.; Costi, K.; Howie, D.W.; Solomon, L.B. The diagnostic performance of radiographic criteria to detect aseptic acetabular component loosening after revision total hip arthroplasty. Bone Jt. J. 2017, 99, 458–464. [Google Scholar] [CrossRef] [PubMed]
- Martin, J.R.; Barrett, I.; Sierra, R.J.; Lewallen, D.G.; Berry, D.J. Construct Rigidity: Keystone for Treating Pelvic Discontinuity. J. Bone Jt. Surg. Am. 2017, 99, e43. [Google Scholar] [CrossRef] [PubMed]
- Chiarlone, F.; Zanirato, A.; Cavagnaro, L.; Alessio-Mazzola, M.; Felli, L.; Burastero, G. Acetabular custom-made implants for severe acetabular bone defect in revision total hip arthroplasty: A systematic review of the literature. Arch. Orthop. Trauma Surg. 2020, 140, 415–424. [Google Scholar] [CrossRef] [PubMed]
- Walter, S.G.; Randau, T.M.; Gravius, N.; Gravius, S.; Froschen, F.S. Monoflanged Custom-Made Acetabular Components Promote Biomechanical Restoration of Severe Acetabular Bone Defects by Metallic Defect Reconstruction. J. Arthroplast. 2020, 35, 831–835. [Google Scholar] [CrossRef] [PubMed]
- Telleria, J.J.; Gee, A.O. Classifications in brief: Paprosky classification of acetabular bone loss. Clin. Orthop. Relat. Res. 2013, 471, 3725–3730. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Paprosky Classification with and without PD | N | Iliac Stem N | Failure N (Mode) |
|---|---|---|---|
| IIIa | 2 | 0 | 1 (infection) |
| IIIa with PD | 5 | 5 | 1 (aseptic) |
| IIIB | 5 | 5 | 0 |
| IIIB with PD | 2 | 2 | 2 (one each) |
| total | 14 | 12 | 4 |
| Preoperative (N) | 1 Year Postoperative (N) | p * | |
|---|---|---|---|
| pain | 51.00 (10–92) (10) | 21.27 (10–70) (11) | 0.038 |
| stiffness | 53.50 (10–100) (10) | 28.18 (10–60) (11) | 0.068 |
| physical function | 72.30 (30–94) (10) | 32.36 (1–85) (10) | 0.007 |
| all | 63.89 (27–82) (10) | 29.45 (11–78) (11) | 0.015 |
| Mean (Min to Max) | |
|---|---|
| Leg Length Discrepancy in mm | +3 (−8 to 20) |
| Lateralization of COR in mm | +8 (−8 to 35) |
| Proximalization of COR in mm | +6 (−13 to 26) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
von Hertzberg-Boelch, S.P.; Wagenbrenner, M.; Arnholdt, J.; Frenzel, S.; Holzapfel, B.M.; Rudert, M. Custom Made Monoflange Acetabular Components for the Treatment of Paprosky Type III Defects. J. Pers. Med. 2021, 11, 283. https://doi.org/10.3390/jpm11040283
von Hertzberg-Boelch SP, Wagenbrenner M, Arnholdt J, Frenzel S, Holzapfel BM, Rudert M. Custom Made Monoflange Acetabular Components for the Treatment of Paprosky Type III Defects. Journal of Personalized Medicine. 2021; 11(4):283. https://doi.org/10.3390/jpm11040283
Chicago/Turabian Stylevon Hertzberg-Boelch, Sebastian Philipp, Mike Wagenbrenner, Jörg Arnholdt, Stephan Frenzel, Boris Michael Holzapfel, and Maximilian Rudert. 2021. "Custom Made Monoflange Acetabular Components for the Treatment of Paprosky Type III Defects" Journal of Personalized Medicine 11, no. 4: 283. https://doi.org/10.3390/jpm11040283
APA Stylevon Hertzberg-Boelch, S. P., Wagenbrenner, M., Arnholdt, J., Frenzel, S., Holzapfel, B. M., & Rudert, M. (2021). Custom Made Monoflange Acetabular Components for the Treatment of Paprosky Type III Defects. Journal of Personalized Medicine, 11(4), 283. https://doi.org/10.3390/jpm11040283