
P2Y12 Antiplatelet Choice for Patients with Chronic Kidney Disease and Acute Coronary Syndrome: A Systematic Review and Meta-Analysis

 , , ,
, , ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Data Sources and Search Strategy
2.2. Study Selection and Data Extraction
2.3. End Points
2.4. Assessment of Bias Risk and Evidence
2.5. Statistical Methods
3. Results
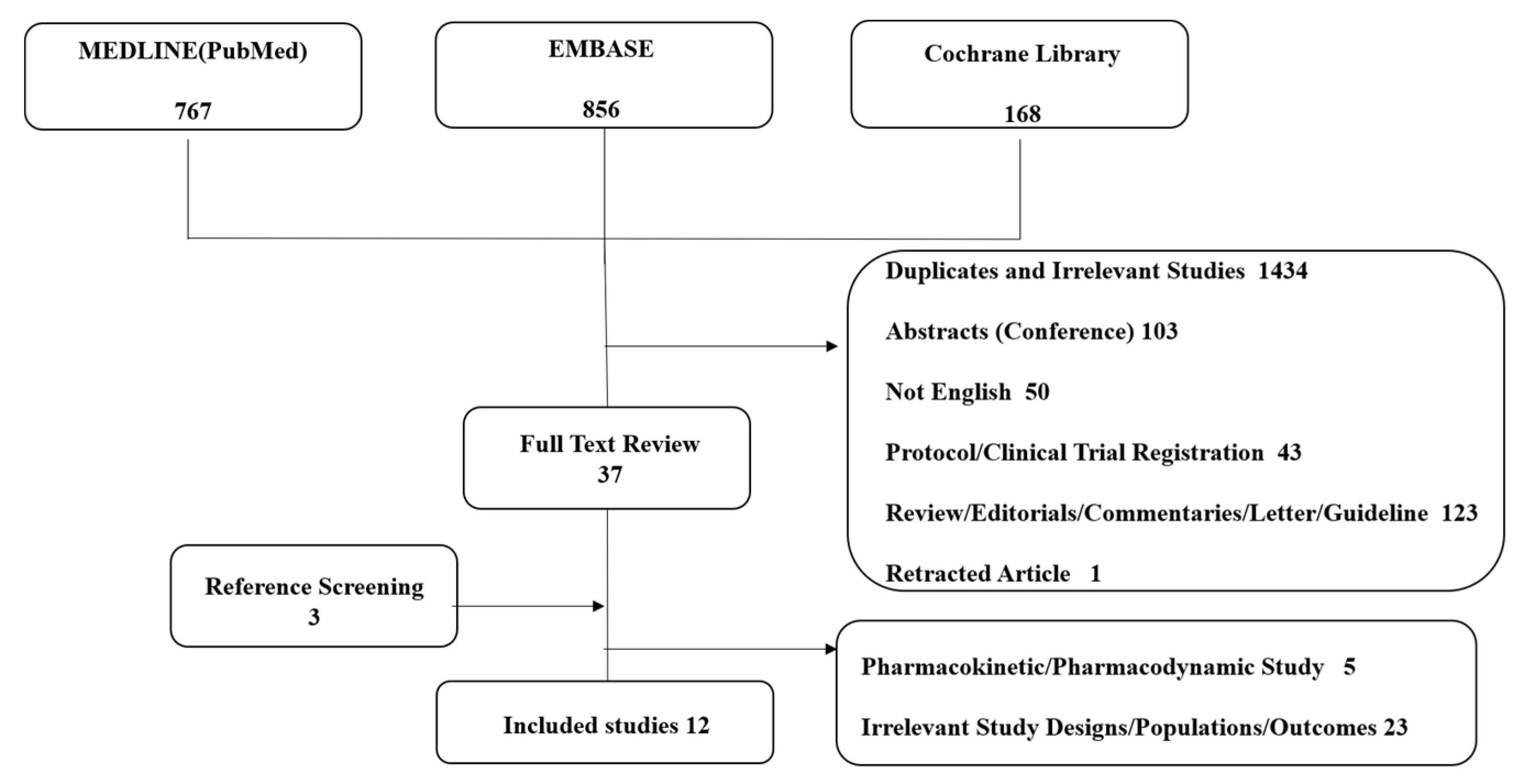
3.1. Study Search and Selection
3.2. Study Characteristics
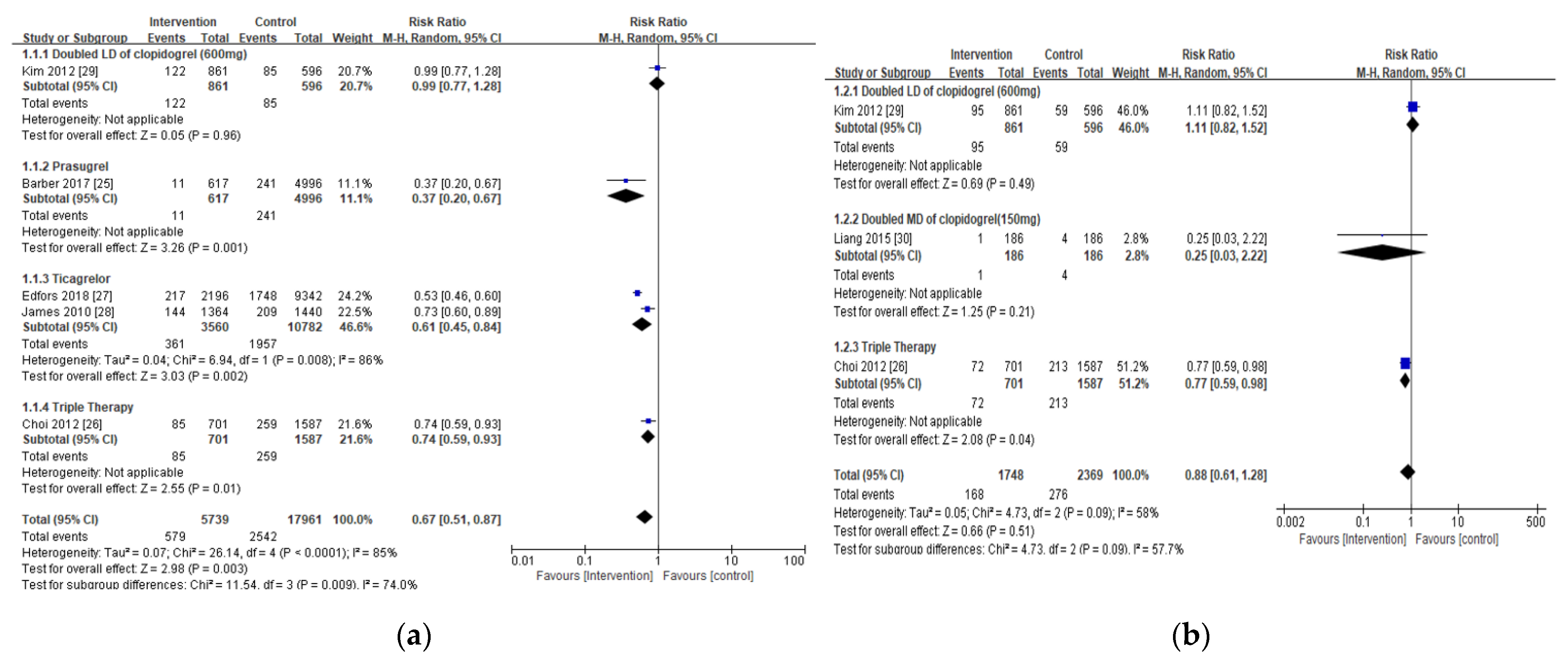
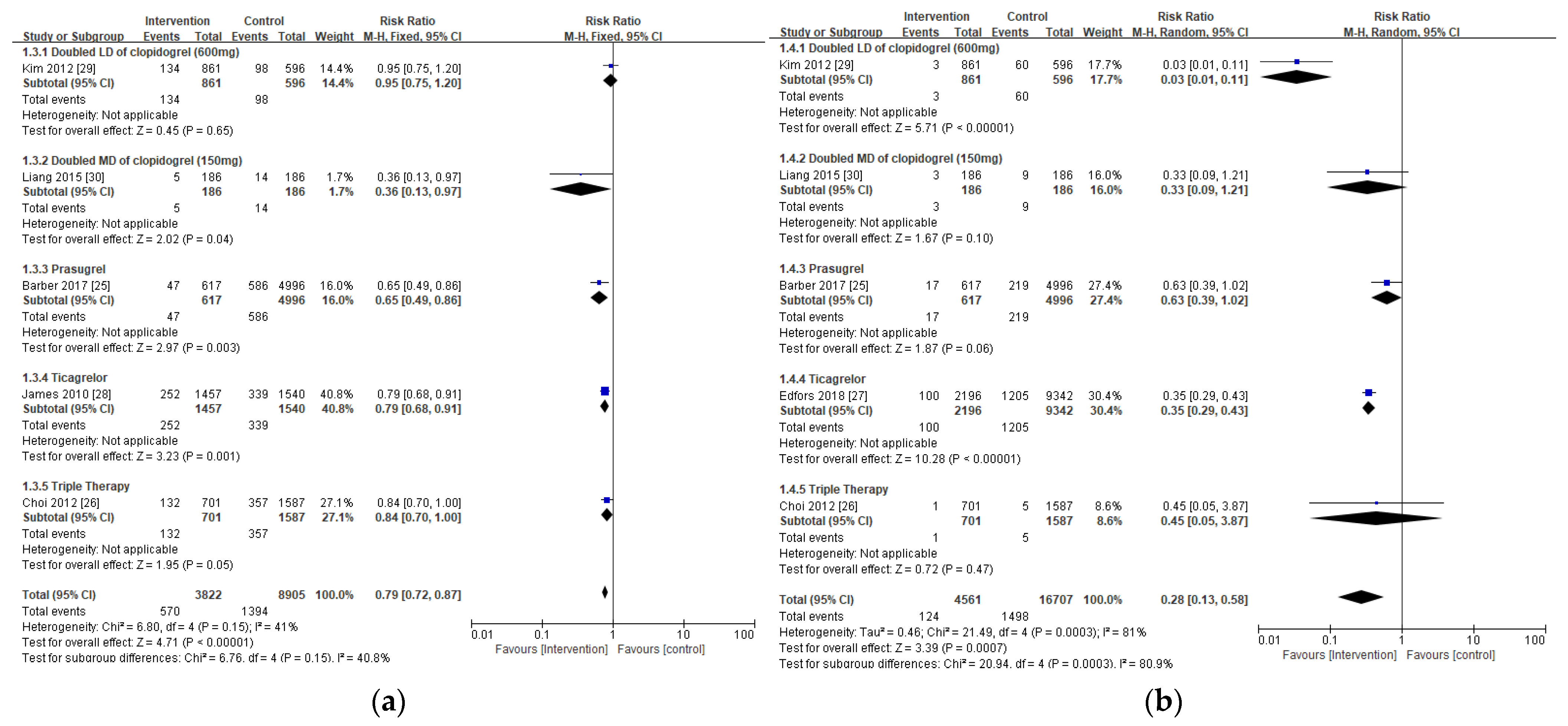
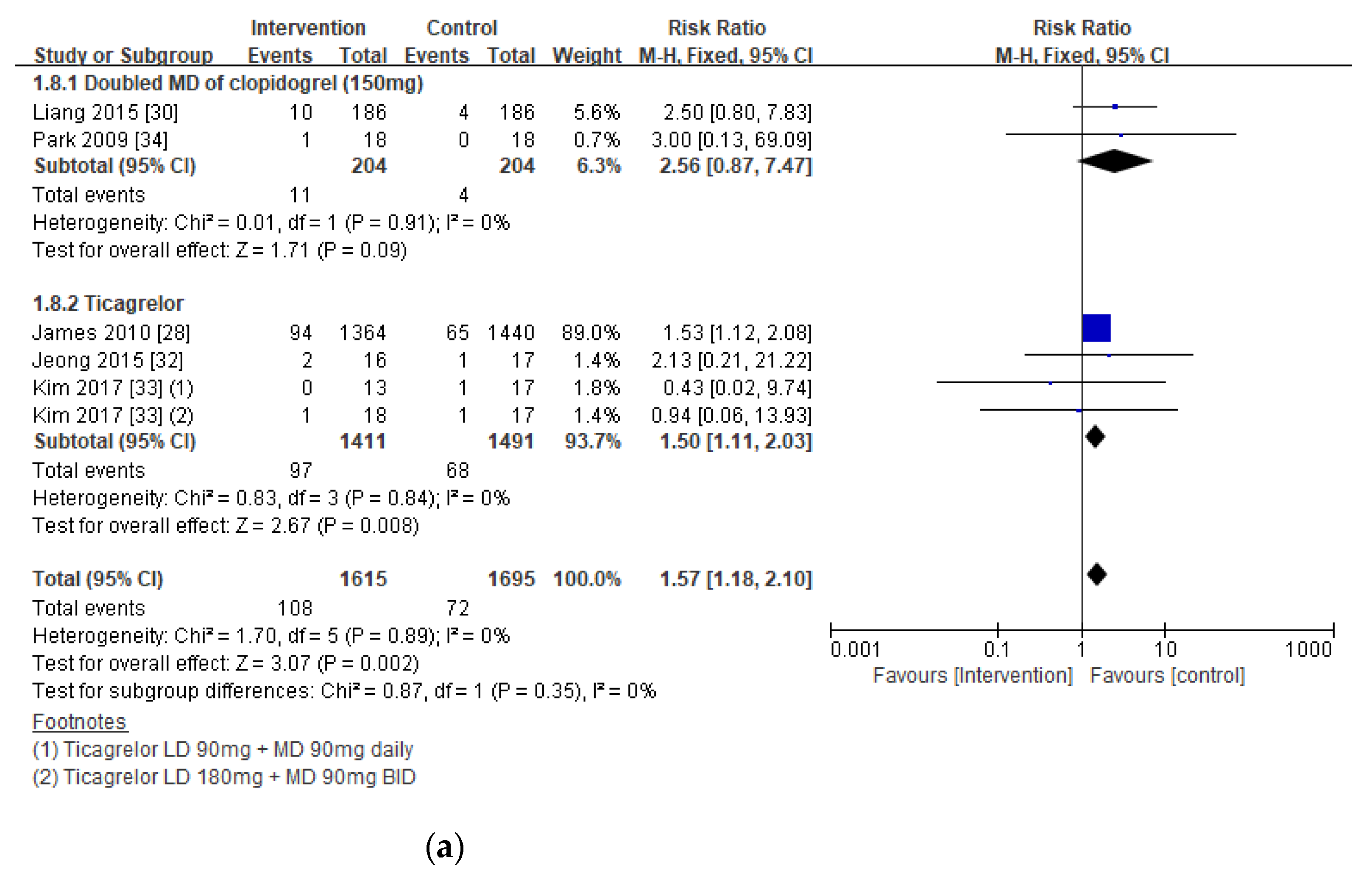
3.3. Outcomes in Patients with CKD
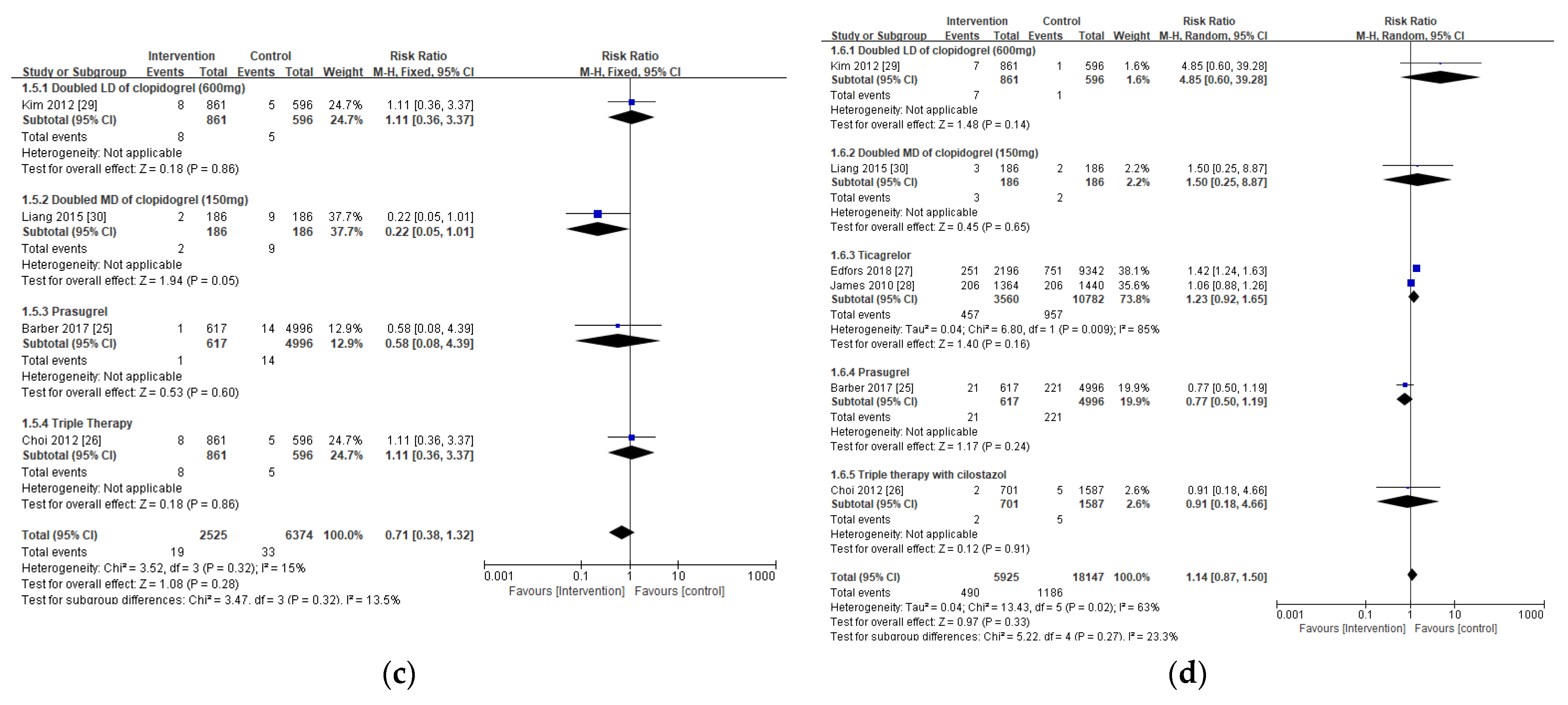
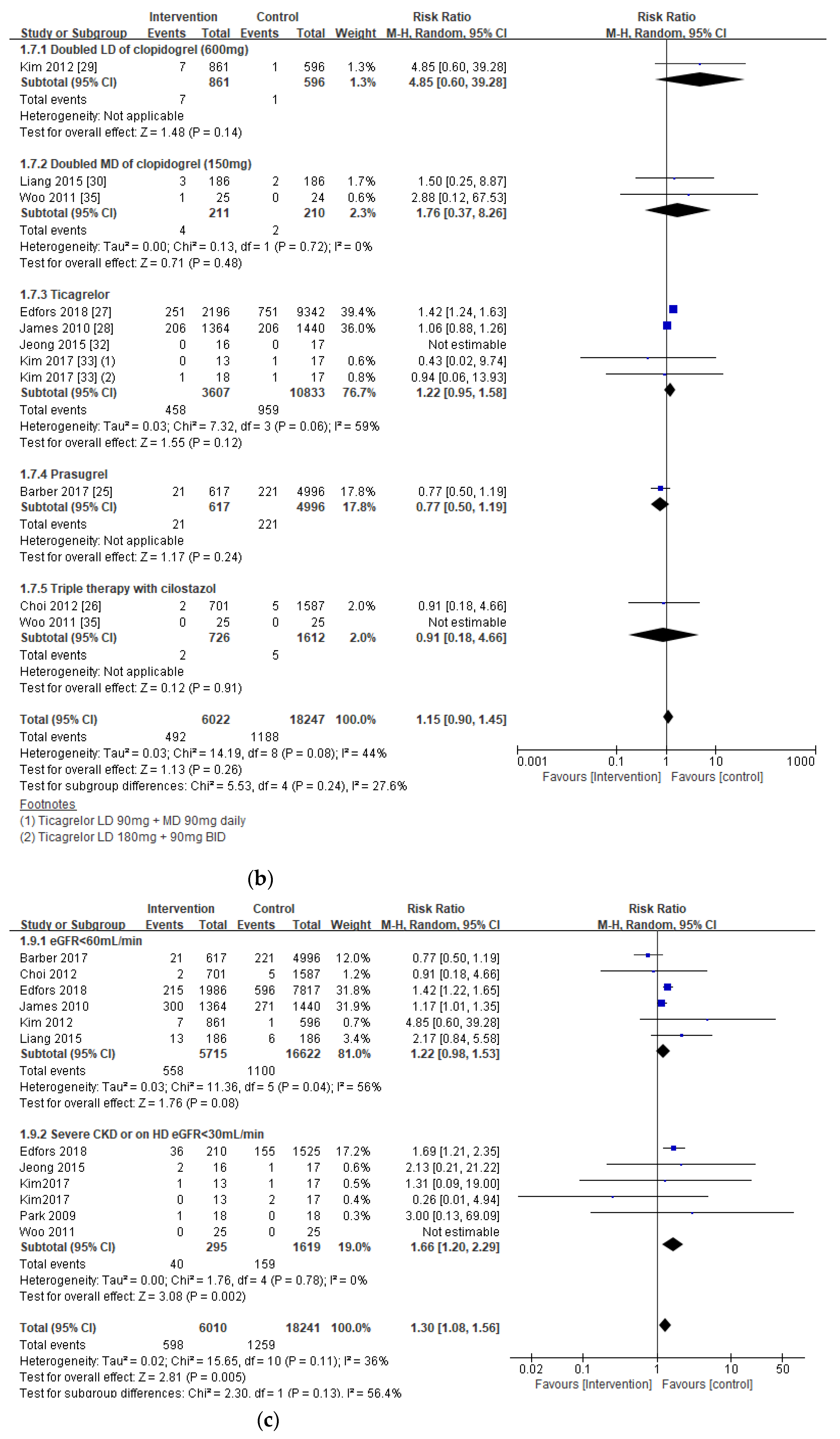
3.4. Safety Outcomes in Patients with CKD, Including Those on Hemodialysis
Subgroup Analysis in Bleeding Risks Associated with the Extent of Renal Insufficiency
3.5. Intermediate Outcomes in Patients with CKD
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Levine, G.N.; Bates, E.R.; Bittl, J.A.; Brindis, R.G.; Fihn, S.D.; Fleisher, L.A.; Granger, C.B.; Lange, R.A.; Mack, M.J.; Mauri, L.; et al. 2016 ACC/AHA Guideline Focused Update on Duration of Dual Antiplatelet Therapy in Patients With Coronary Artery Disease: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J. Am. Coll. Cardiol. 2016, 68, 1082–1115. [Google Scholar] [CrossRef] [PubMed]
- Collet, J.P.; Thiele, H.; Barbato, E.; Barthelemy, O.; Bauersachs, J.; Bhatt, D.L.; Dendale, P.; Dorobantu, M.; Edvardsen, T.; Folliguet, T.; et al. 2020 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation. Eur. Heart J. 2020, ehaa575. [Google Scholar] [CrossRef]
- Becker, R.C.; Bassand, J.P.; Budaj, A.; Wojdyla, D.M.; James, S.K.; Cornel, J.H.; French, J.; Held, C.; Horrow, J.; Husted, S.; et al. Bleeding complications with the P2Y12 receptor antagonists clopidogrel and ticagrelor in the PLATelet inhibition and patient Outcomes (PLATO) trial. Eur. Heart J. 2011, 32, 2933–2944. [Google Scholar] [CrossRef] [PubMed]
- Angiolillo, D.J. Variability in responsiveness to oral antiplatelet therapy. Am. J. Cardiol 2009, 103 (Suppl. 3), 27a–34a. [Google Scholar] [CrossRef] [PubMed]
- Melloni, C.; Cornel, J.H.; Hafley, G.; Neely, M.L.; Clemmensen, P.; Zamoryakhin, D.; Prabhakaran, D.; White, H.D.; Fox, K.A.; Ohman, E.M.; et al. Impact of chronic kidney disease on long-term ischemic and bleeding outcomes in medically managed patients with acute coronary syndromes: Insights from the TRILOGY ACS Trial. Eur. Heart J. Acute Cardiovasc. Care 2016, 5, 443–454. [Google Scholar] [CrossRef]
- Wiviott, S.; Braunwald, E.; McCabe, C.; McCabe, B.; Montalescot, G.; Ruzyllo, W.; Gottlieb, S.; Neumann, F.; Ardissino, D.; De Servi, S.; et al. Prasugrel versus clopidogrel in patients with acute coronary syndromes. N. Engl. J. Med. 2007, 357, 2001–2015. [Google Scholar] [CrossRef] [PubMed]
- Wallentin, L.; Becker, R.C.; Budaj, A.; Cannon, C.P.; Emanuelsson, H.; Held, C.; Horrow, J.; Husted, S.; James, S.; Katus, H.; et al. Ticagrelor versus Clopidogrel in Patients with Acute Coronary Syndromes. N. Engl. J. Med. 2009, 361, 1045–1057. [Google Scholar] [CrossRef] [PubMed]
- Marenzi, G.; Cabiati, A.; Assanelli, E. Chronic kidney disease in acute coronary syndromes. World J. Nephrol. 2012, 1, 134–145. [Google Scholar] [CrossRef]
- Konishi, A.; Shinke, T.; Otake, H.; Takaya, T.; Osue, T.; Kinutani, H.; Kuroda, M.; Takahashi, H.; Terashita, D.; Hirata, K. Impact of residual platelet reactivity under clopidogrel treatment for lesions and the clinical outcome after drug-eluting stent implantation in patients with hemodialysis. J. Cardiol. 2016, 67, 531–537. [Google Scholar] [CrossRef][Green Version]
- Ocak, G.; Rookmaaker, M.B.; Algra, A.; de Borst, G.J.; Doevendans, P.A.; Kappelle, L.J.; Verhaar, M.C.; Visseren, F.L.; Group, S.S. Chronic kidney disease and bleeding risk in patients at high cardiovascular risk: A cohort study. J. Thromb. Haemost. 2018, 16, 65–73. [Google Scholar] [CrossRef]
- Urban, P.; Mehran, R.; Colleran, R.; Angiolillo, D.J.; Byrne, R.A.; Capodanno, D.; Cuisset, T.; Cutlip, D.; Eerdmans, P.; Eikelboom, J.; et al. Defining High Bleeding Risk in Patients Undergoing Percutaneous Coronary Intervention. Circulation 2019, 140, 240–261. [Google Scholar] [CrossRef] [PubMed]
- Ferreiro, J.L.; Angiolillo, D.J. Clopidogrel response variability: Current status and future directions. Thromb. Haemost. 2009, 102, 7–148. [Google Scholar] [CrossRef]
- Park, K.W.; Kim, H. Options to overcome clopidogrel response variability. Circ. J. 2012, 76, 287–292. [Google Scholar] [CrossRef]
- Muller, C.; Caillard, S.; Jesel, L.; Ghannudi, S.E.; Ohlmann, P.; Sauleau, E.; Hannedouche, T.; Gachet, C.; Moulin, B.; Morel, O. Association of estimated GFR with platelet inhibition in patients treated with clopidogrel. Am. J. Kidney Dis. 2012, 59, 777–785. [Google Scholar] [CrossRef] [PubMed]
- Bonello, L.; Laine, M.; Lemesle, G.; Puymirat, E.; Darby, T.; Thuny, F.; Paganelli, F.; Aradi, D.; Frere, C.; Burtey, S.; et al. Meta-analysis of potent P2Y12-ADP receptor antagonist therapy compared to clopidogrel therapy in acute coronary syndrome patients with chronic kidney disease. Thromb. Haemost. 2018, 118, 1839–1846. [Google Scholar] [CrossRef]
- Rymer, J.A.; Kaltenbach, L.A.; Doll, J.A.; Messenger, J.C.; Peterson, E.D.; Wang, T.Y. Safety of Dual-Antiplatelet Therapy After Myocardial Infarction Among Patients With Chronic Kidney Disease. J. Am. Heart Assoc. 2019, 8, e012236. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. BMJ 2009, 339, b2535. [Google Scholar] [CrossRef]
- Methley, A.M.; Campbell, S.; Chew-Graham, C.; McNally, R.; Cheraghi-Sohi, S. PICO, PICOS and SPIDER: A comparison study of specificity and sensitivity in three search tools for qualitative systematic reviews. BMC Health Serv. Res. 2014, 14, 579. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savovic, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef] [PubMed]
- Sterne, J.A.C.; Higgins, J.P.T.; Elbers RG Reeves BC and the development group for ROBINSI. Risk of Bias in Non-randomized Studies of Interventions (ROBINS-I): Detailed guidance, updated 12 October 2016. Available online: http://www.riskofbias.info (accessed on 1 November 2020).
- Sterne, J.A.; Hernán, M.A.; Reeves, B.C.; Savović, J.; Berkman, N.D.; Viswanathan, M.; Henry, D.; Altman, D.G.; Ansari, M.T.; Boutron, I.; et al. ROBINS-I: A tool for assessing risk of bias in non-randomised studies of interventions. BMJ 2016, 355, i4919. [Google Scholar] [CrossRef]
- Cochran, W.G. The combination of estimates from different experiments. Biometrics 1954, 10, 101–129. [Google Scholar] [CrossRef]
- Higgins, J.P.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [PubMed]
- Review Manager (RevMan) [Computer Program]. Version 5.4. The Nordic Cochrane Centre, The Cochrane Collaboration: Copenhagen, Denmark. Available online: https://training.cochrane.org/ (accessed on 22 January 2021).
- Baber, U.; Chandrasekhar, J.; Sartori, S.; Aquino, M.; Kini, A.S.; Kapadia, S.; Weintraub, W.; Muhlestein, J.B.; Vogel, B.; Faggioni, M.; et al. Associations Between Chronic Kidney Disease and Outcomes With Use of Prasugrel Versus Clopidogrel in Patients With Acute Coronary Syndrome Undergoing Percutaneous Coronary Intervention: A Report From the PROMETHEUS Study. JACC Cardiovasc. Interv. 2017, 10, 2017–2025. [Google Scholar] [CrossRef]
- Choi, Y.H.; Suh, S.H.; Choi, J.S.; Kim, C.S.; Sim, D.S.; Bae, E.H.; Lim, S.Y.; Ma, S.K.; Jeong, M.H.; Kim, S.W.; et al. Triple vs. dual antiplatelet therapy in patients with acute myocardial infarction and renal dysfunction. Circ. J. 2012, 76, 2405–2411. [Google Scholar] [CrossRef] [PubMed]
- Edfors, R.; Sahlen, A.; Szummer, K.; Renlund, H.; Evans, M.; Carrero, J.J.; Spaak, J.; James, S.K.; Lagerqvist, B.; Varenhorst, C.; et al. Outcomes in patients treated with ticagrelor versus clopidogrel after acute myocardial infarction stratified by renal function. Heart 2018, 104, 1575–1582. [Google Scholar] [CrossRef] [PubMed]
- James, S.; Budaj, A.; Aylward, P.; Buck, K.K.; Cannon, C.P.; Cornel, J.H.; Harrington, R.A.; Horrow, J.; Katus, H.; Keltai, M.; et al. Ticagrelor versus clopidogrel in acute coronary syndromes in relation to renal function: Results from the Platelet Inhibition and Patient Outcomes (PLATO) trial. Circulation 2010, 122, 1056–1067. [Google Scholar] [CrossRef]
- Kim, J.Y.; Jeong, M.H.; Moon, J.H.; Ahn, Y.K.; Chae, S.C.; Hur, S.H.; Hong, T.J.; Kim, Y.J.; Seong, I.W.; Chae, I.H.; et al. Impact of Clopidogrel loading dose in patients with chronic kidney disease undergoing primary percutaneous coronary intervention for ST-segment elevation myocardial infarction. Am. J. Cardiol. 2012, 110, 1598–1606. [Google Scholar] [CrossRef]
- Liang, J.; Wang, Z.; Shi, D.; Liu, Y.; Zhao, Y.; Han, H.; Li, Y.; Liu, W.; Zhang, L.; Yang, L.; et al. High clopidogrel dose in patients with chronic kidney disease having clopidogrel resistance after percutaneous coronary intervention. Angiology 2015, 66, 319–325. [Google Scholar] [CrossRef] [PubMed]
- Nishi, T.; Ariyoshi, N.; Nakayama, T.; Fujimoto, Y.; Sugimoto, K.; Wakabayashi, S.; Hanaoka, H.; Kobayashi, Y. Impact of chronic kidney disease on platelet inhibition of clopidogrel and prasugrel in Japanese patients. J. Cardiol. 2017, 69, 752–755. [Google Scholar] [CrossRef]
- Jeong, K.H.; Cho, J.H.; Woo, J.S.; Kim, J.B.; Kim, W.S.; Lee, T.W.; Kim, K.S.; Ihm, C.G.; Kim, W. Platelet reactivity after receiving clopidogrel compared with ticagrelor in patients with kidney failure treated with hemodialysis: A randomized crossover study. Am. J. Kidney Dis. 2015, 65, 916–924. [Google Scholar] [CrossRef]
- Kim, J.S.; Woo, J.S.; Kim, J.B.; Kim, W.S.; Lee, T.W.; Kim, K.S.; Ihm, C.G.; Kim, W.; Jeong, K.H. The pharmacodynamics of low and standard doses of ticagrelor in patients with end stage renal disease on hemodialysis. Int. J. Cardiol. 2017, 238, 110–116. [Google Scholar] [CrossRef] [PubMed]
- Park, S.H.; Kim, W.; Park, C.S.; Kang, W.Y.; Hwang, S.H.; Kim, W. A comparison of clopidogrel responsiveness in patients with versus without chronic renal failure. Am. J. Cardiol. 2009, 104, 1292–1295. [Google Scholar] [CrossRef]
- Woo, J.S.; Kim, W.; Lee, S.R.; Jung, K.H.; Kim, W.S.; Lew, J.H.; Lee, T.W.; Lim, C.K. Platelet reactivity in patients with chronic kidney disease receiving adjunctive cilostazol compared with a high-maintenance dose of clopidogrel: Results of the effect of platelet inhibition according to clopidogrel dose in patients with chronic kidney disease (PIANO-2 CKD) randomized study. Am. Heart J. 2011, 162, 1018–1025. [Google Scholar] [PubMed]
- Shuldiner, A.R.; O’Connell, J.R.; Bliden, K.P.; Gandhi, A.; Ryan, K.; Horenstein, R.B.; Damcott, C.M.; Pakyz, R.; Tantry, U.S.; Gibson, Q.; et al. Association of cytochrome P450 2C19 genotype with the antiplatelet effect and clinical efficacy of clopidogrel therapy. JAMA 2009, 302, 849–857. [Google Scholar] [CrossRef] [PubMed]
- Ma, T.K.; Lam, Y.Y.; Tan, V.P.; Yan, B.P. Variability in response to clopidogrel: How important are pharmacogenetics and drug interactions? Br. J. Clin. Pharmacol. 2011, 72, 697–706. [Google Scholar] [CrossRef] [PubMed]
- Hochholzer, W.; Trenk, D.; Fromm, M.F.; Valina, C.M.; Stratz, C.; Bestehorn, H.P.; Büttner, H.J.; Neumann, F.J. Impact of cytochrome P450 2C19 loss-of-function polymorphism and of major demographic characteristics on residual platelet function after loading and maintenance treatment with clopidogrel in patients undergoing elective coronary stent placement. J. Am. Coll. Cardiol. 2010, 55, 2427–2434. [Google Scholar] [CrossRef] [PubMed]
- Gragano, F.; Moscarella, E.; Calabro, P.; Arturo, C.; Pafundi, P.C.; Lelasi, A.; Patti, G.; Cavallari, I.; Antonucci, E.; Cirillo, P.; et al. Clopidogrel versus ticagrelor in high-bleeding risk patients presenting with acute coronary syndromes:insights from the multicenter STAR-ANTIPLATELET registry. Intern. Emerg. Med. 2020, 16, 379–387. [Google Scholar] [CrossRef]
- Cesaro, A.; Talialatela, V.; Gragnano, F.; Moscarella, E.; Fimiani, F.; Conte, M.; Barletta, V.; Monda, E.; Limongelli, G.; Severino, S.; et al. Low-dose ticagrelor in patients with high ichemic risk and previous myocaridal infarction: A multicenter prospective real-world observational study. J. Cardiovasc. Pharmacol. 2020, 76, 173–180. [Google Scholar]
- Alexopoulos, D.; Panagiotou, A.; Xanthopoulou, I.; Komninakis, D.; Kassimis, G.; Davlouros, P.; Fourtounas, C.; Goumenos, D. Antiplatelet effects of prasugrel vs. double clopidogrel in patients on hemodialysis and with high on-treatment platelet reactivity. J. Thromb. Haemost. 2011, 9, 2379–2385. [Google Scholar] [CrossRef]
- Bonaca, M.P.; Bhatt, D.L.; Cohen, M.; Steg, P.G.; Storey, R.F.; Jensen, E.C.; Magnani, G.; Bansilal, S.; Fish, M.P.; Im, K.; et al. PEGASUS-TIMI 54 Steering Committee and Investigators. Long-term use of ticagrelor in patients with prior myocardial infaction. N. Engl. J. Med. 2015, 372, 1791–1800. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Component | Definition |
|---|---|
| P (patients) | Patients in ACS with CKD, including HD |
| I (intervention) | DAPT regimen with enhanced antiplatelet activity (or reduced platelet reactivity) to overcome response variability of clopidogrel and is composed with [13]:
|
| C (comparator) | Standard dose of clopidogrel-based DAPT |
| O (outcomes) | Efficacy outcomes: all-cause or cardiac-related mortality, MACE, MI, stent thrombosis; safety outcomes: major or minor bleeding; intermediate outcomes: IPA and PRU |
| S (study design) | RCTs, observational studies, and prospective studies |
| Author Name | Study Region | Study Design | Patient Population | Intervention | Comparator (Control) | Duration | Efficacy | Safety |
|---|---|---|---|---|---|---|---|---|
| CKD Populations (eGFR < 60 mL/min) | ||||||||
| Barber et al. (2017) [25] | U.S. | Multicenter, observational study | ACS patients with CKD undergoing PCI (n = 5613) | Prasugrel + ASA (n = 617) | Clopidogrel +ASA (n = 4996) | 1 year | No significant difference in MACE, death, and MI | No significant difference in bleeding |
| Choi et al. (2012) [26] | Korea | Prospective, multicenter, online registry of Korea (KAMIR) | AMI patients with renal dysfunction (n = 2288) | Triple therapy (ASA+clopidogrel+cilostazol) (n = 701) | Clopidogrel +ASA (n = 1587) | Not available | Significantly lower rates of in-hospital death (6.7% vs. 11.3%, p = 0.001) and 1-month MACE (11.1% vs. 16.3% p = 0.002) in triple therapy group but no difference in 12-month MACE | No significant difference in bleeding, in-hospital major bleeding (p = 0.870) |
| Edfors et al. (2018) [27] | Sweden | Swedish Web-System for Enhancement and Development of Evidence-Based Care in Heart Disease Evaluated According to Recommended Therapies (SWEDEHEART) registry study | NSTEMI and STE15MI patients discharged with DAPT and eGFR less than 60 mL/min (n = 11,538) | Ticagrelor 180 mg LD followed by 90 mg BID +ASA (n = 2196) | Clopidogrel + ASA (n = 9342) | 12 months | Ticagrelor as compared with clopidogrel was associated with a lower 1-year risk of the composite outcome (eGFR 30–60: 0.82 (0.70 to 0.97), eGFR < 30: 0.95 (0.69 to 1.29), p = 0.55)across the eGFR strata. | Ticagrelor as compared with clopidogrel was associated with a higher risk of bleeding (eGFR 30–60: 1.13 (0.84 to 1.51), eGFR < 30: 1.79 (1.00 to 3.21), p for interaction = 0.30) across the eGFR strata. |
| James et al. (2010) [28] | Multinational | Post hoc analysis of a multicenter, randomized, double-blind trial | ACS patients with chronic kidney disease (n = 3237) | Ticagrelor 180 mg LD followed by 90 mg BID+ Aspirin (75–100 mg) | Clopidogrel 300 mg LD followed by 75 mg daily + Aspirin (75–100 mg) | 12 months | Significantly reduced primary end points (CV death, MI, stroke) of HR 0.77 [0.65–0.9], p = 0.03 and mortality of HR 0.72 [0.58–0.89], p = 0.02 in ticagrelor | No significant difference in major bleeding rates (HR: 1.07 [0.88–1.30]), fatal bleedings (HR: 0.48 [0.15–1.54]), and non-CABG-related major bleedings (HR:1.29 [0.97–1.68]) |
| Kim et al. (2012) [29] | Korea | Prospective, open, observational, multicenter on-line registry of Korea (KAMIR) | STEMI patients undergoing PCI with CKD within 24 h of onset (n = 1457) | Clopidogrel 600 mg LD+75 mg MD + ASA 100mg | Clopidogrel 300mg LD+ 75mg MD + ASA 100mg | Not available | No difference in MACE at 1 month (15.6 vs. 16.4%, p = 0.700) and 12 months (19.0% vs. 21.3%, p = 0.32) | In-hospital major bleeding rate was similar (0.8% vs. 0.2%, p = 0.09). |
| Liang et al. (2015) [30] | China | Prospective, randomized, open-label, parallel-group, single-center study | CAD patients with CKD undergoing PCI with DES (n = 370) | Clopidogrel 300 mg LD followed by 150 mg daily + ASA 100 mg daily (n = 186) | Clopidogrel 300 mg LD followed by 75 mg daily + ASA 100mg daily (n = 184) | 30 days | Significantly lower rates of stent thrombosis (1.1% vs. 4.9%, p = 0.03) and MACE (2.7% vs. 7.6%, p = 0.03) in patients who received 150 mg | No significant difference in major(1.6% vs. 1.1%, p = 1.00) or minor (5.4% vs. 2.2%, p = 0.11) bleeding |
| Melloni et al. (2015) [5] | Multinational | Phase 3, randomized, double-blinded, double-dummy, active-control study | ACS patients enrolled in TRIOLOGY-ACS study (n = 8953) | Prasugrel 30 mg LD followed by 10 mg daily (5 mg daily for patients older than 75 years or if < 60 kg +ASA | Clopidogrel 300 mg LD followed by 75 mg daily+ ASA | 30 months | Substantially reduced PRU in prasugrel in all three CKD stages, Difference in PRU between (prasugrel-clopidogrel): severe CKD: −81.8 [−130.6, −33.1] moderate CKD: −70.8 [−84.8, −56.8) normal/mild CKD −101.4 [−110.1, −92.7] | Not available |
| Nishi et al. (2017) [31] | Japan | Post hoc analysis of a single-center, prospective, crossover study | Japanese patients undergoing PCI (n = 53 total, n = 15 for CKD and n = 38 for non-CKD) | Prasugrel 3.75 mg daily + ASA 100 mg | Clopidogrel 300 mg LD followed by 75 mg daily+ ASA 100 mg | 28 days (crossover at day 14) | Significantly lower PRU in prasugrel treated patients (165.3 ± 61.8 vs. 224.3 ± 57.0, p = 0.002) | Not available |
| Patients on HD | ||||||||
| Jeong et al. (2015) [32] | Korea | Single-center, prospective, randomized, crossover study | Patients with kidney failure with HTPR on HD (n = 25) | Ticagrelor 180 mg LD followed by 90 mg BID +ASA 100 mg | Clopidogrel 300 mg LD followed by 75 mg daily + ASA 100 mg | 10 weeks | More rapid and greater platelet inhibition in ticagrelor treated group (p < 0.05) | Two clinically relevant cases of minor bleeding in ticagrelor-treated group (1 arteriovenousfistula bleeding and 1 oral bleeding) |
| Kim et al. (2017) [33] | Korea | Prospective, randomized, single-center study | ESRD patients on regular HD (n = 52) | (1) Ticagrelor 90 mg LD followed by 90 mg daily +ASA (n = 13) OR (2) Ticagrelor 180 mg LD followed by 90 mg BID+ ASA(n = 21)/ | Clopidogrel 300 mg LD followed by 75 mg daily +ASA(n = 18) | 14 days | Significant difference in IPA in low ticagrelor group compared to clopidogrel treated group. Standard ticagrelor group showed the highest IPA (ANCOVA < 0.001) | No bleeding events in low-dose ticagrelor BARC Type I (gum bleeding) events: clopidogrel (5.9%) standard ticagrelor (5.6%) BARC Type 2 events (arteriovenous fistula bleeding) standard ticagrelor (5.6%) |
| Park et al. (2009) [34] | Korea | Prospective, randomized, open-label single-center study | Patients with CRF (75% patients on HD) (n = 36) | Clopidogrel 600 mg LD followed by 150 mg daily +ASA 100 mg | Clopidogrel 300 mg LD followed by 75 mg daily + ASA 100 mg | 4 weeks/30 days | No significant difference in PRU (302 ± 81 vs. 308 ± 70, p = 0.824) and mean percentage of inhibition (23.4 ± 14.4 vs. 21.3 ± 16.0, p = 0.808) | Gastrointestinal ulcer bleeding in 1 patient who received clopidogrel at 150 mg |
| Woo et al. (2011) [35] | Korea | Prospective, open, randomized platelet function study | CKD patients undergoing HD who received PCI (n = 74) | (1) Clopidogrel 150 mg/day +ASA 100 mg (n = 25) (2) Triple therapy (clopidogrel 75 mg + cilostazol+ ASA 100 mg) (n = 25) | Clopidogrel 75 mg + ASA 100 mg (n = 24) | 14 days | The rate of high on-treatment platelet activity was significantly lower in triple therapy (10% vs. 43% vs. 32% p < 0.05) | Gastrointestinal ulcer bleeding in 1 patient who received clopidogrel at 150 mg |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Park, S.; Choi, Y.J.; Kang, J.E.; Kim, M.G.; Jung Geum, M.; Kim, S.D.; Rhie, S.J. P2Y12 Antiplatelet Choice for Patients with Chronic Kidney Disease and Acute Coronary Syndrome: A Systematic Review and Meta-Analysis. J. Pers. Med. 2021, 11, 222. https://doi.org/10.3390/jpm11030222
Park S, Choi YJ, Kang JE, Kim MG, Jung Geum M, Kim SD, Rhie SJ. P2Y12 Antiplatelet Choice for Patients with Chronic Kidney Disease and Acute Coronary Syndrome: A Systematic Review and Meta-Analysis. Journal of Personalized Medicine. 2021; 11(3):222. https://doi.org/10.3390/jpm11030222
Chicago/Turabian StylePark, Sohyun, Yeo Jin Choi, Ji Eun Kang, Myeong Gyu Kim, Min Jung Geum, So Dam Kim, and Sandy Jeong Rhie. 2021. "P2Y12 Antiplatelet Choice for Patients with Chronic Kidney Disease and Acute Coronary Syndrome: A Systematic Review and Meta-Analysis" Journal of Personalized Medicine 11, no. 3: 222. https://doi.org/10.3390/jpm11030222
APA StylePark, S., Choi, Y. J., Kang, J. E., Kim, M. G., Jung Geum, M., Kim, S. D., & Rhie, S. J. (2021). P2Y12 Antiplatelet Choice for Patients with Chronic Kidney Disease and Acute Coronary Syndrome: A Systematic Review and Meta-Analysis. Journal of Personalized Medicine, 11(3), 222. https://doi.org/10.3390/jpm11030222