
GENERATOR Breast DataMart—The Novel Breast Cancer Data Discovery System for Research and Monitoring: Preliminary Results and Future Perspectives

 , ,
, , 
 , , ,
, , ,  ,
, 

Abstract
1. Background
2. Materials and Methods
2.1. Domain-Specific Ontology
2.2. Multidisciplinary Team and Rapid Requirement Definition
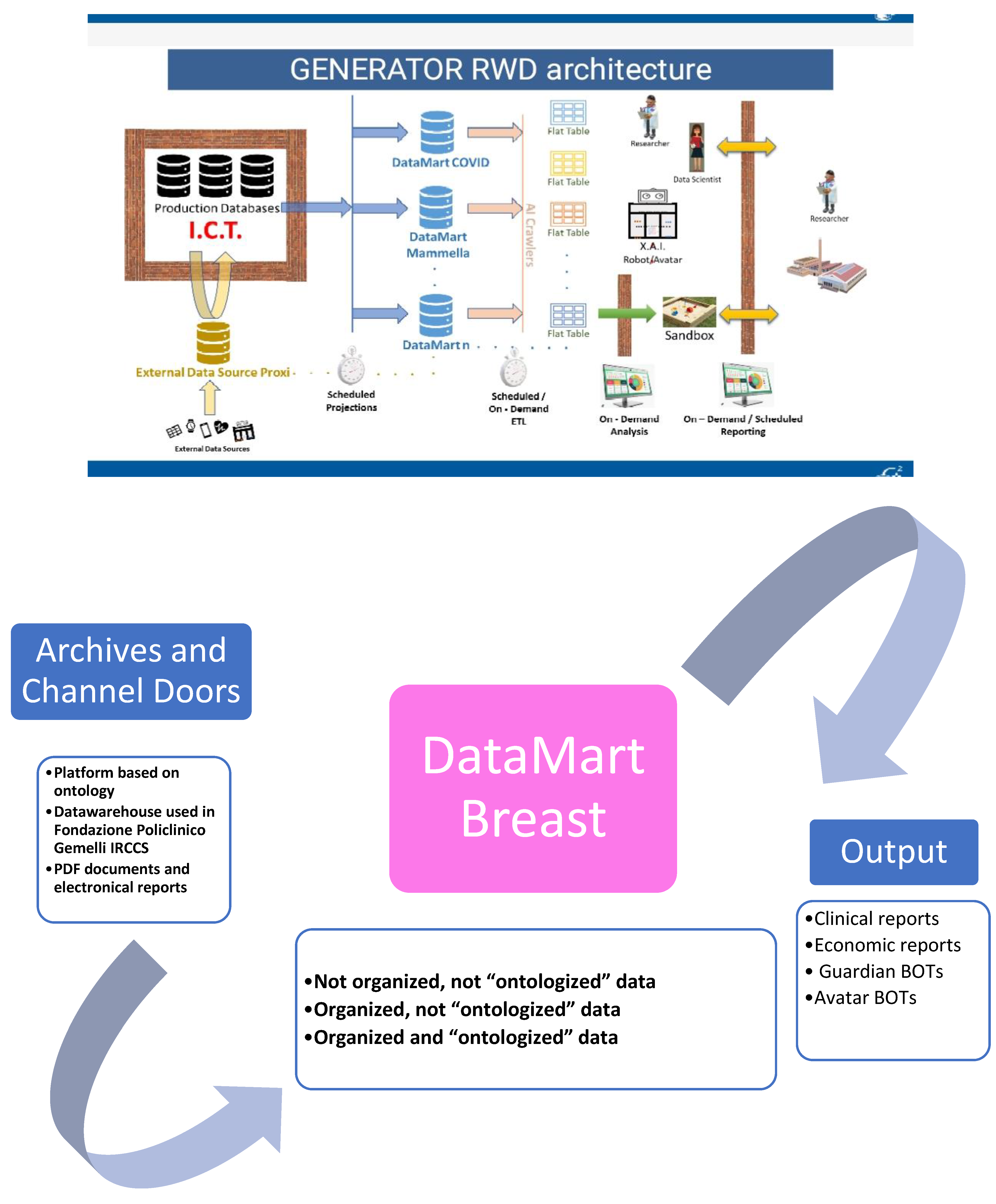
2.3. Breast Cancer DataMart Architecture
3. Results
4. Discussion
- -
- GUARDIAN ROBOT: an instrument that is able to alert the physician on determined items, capable to learn by data implementation.
- -
- PREDICTIVE ROBOT: an instrument capable to predict trend of outcomes capable to learn by data implementation.
- -
- DESCRIPTIVE ROBOT: an instrument capable to describe determined trends that can be used for cost/effectiveness purposes.
- -
- AUTHOMATED ROBOT: an instrument that is linked to some diagnostic and therapeutic procedure, to reduce time of elaboration and lead physicians to more precise results.
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Harbeck, N.; Penault-Llorca, F.; Cortes, J.; Gnant, M.; Houssami, N.; Poortmans, P.; Ruddy, K.; Tsang, J.; Cardoso, F. Breast cancer. Nat. Rev. Dis. Primers 2019, 5, 66. [Google Scholar] [CrossRef] [PubMed]
- Tagliaferri, L.; Budrukkar, A.; Lenkowicz, J.; Cambeiro, M.; Bussu, F.; Guinot, J.L.; Hildebrandt, G.; Johansson, B.; Meyer, J.E.; Niehoff, P.; et al. ENT COBRA ONTOLOGY: The covariates classification system proposed by the Head & Neck and Skin GEC-ESTRO Working Group for interdisciplinary standardized data collection in head and neck patient cohorts treated with interventional radiotherapy (brachytherapy). J. Contemp. Brachytherapy 2018, 10, 260–266. [Google Scholar] [CrossRef]
- Tagliaferri, L.; Gobitti, C.; Colloca, G.F.; Boldrini, L.; Farina, E.; Furlan, C.; Paiar, F.; Vianello, F.; Basso, M.; Cerizza, L.; et al. A new standardized data collection system for interdisciplinary thyroid cancer management: Thyroid COBRA. Eur. J. Intern. Med. 2018, 53, 73–78. [Google Scholar] [CrossRef] [PubMed]
- Meldolesi, E.; van Soest, J.; Alitto, A.R.; Autorino, R.; Dinapoli, N.; Dekker, A.; Gambacorta, M.A.; Gatta, R.; Tagliaferri, L.; Damiani, A.; et al. VATE: VAlidation of high TEchnology based on large database analysis by learning machine. Colorectal Cancer 2014, 3, 435–450. [Google Scholar] [CrossRef]
- Lambin, P.; Roelofs, E.; Reymen, B.; Velazquez, E.R.; Buijsen, J.; Zegers, C.M.; Carvalho, S.; Leijenaar, R.T.; Nalbantov, G.; Oberije, C.; et al. Rapid Learning health care in oncology’—An approach towards decision support systems enabling customised radiotherapy. Radiother. Oncol. 2013, 109, 159–164. [Google Scholar] [CrossRef]
- Weidlich, V.; Weidlich, G.A. Artificial Intelligence in Medicine and Radiation Oncology. Cureus 2018, 10. [Google Scholar] [CrossRef]
- Wolberg, W.H.; Street, W.N.; Mangasarian, O.L. Machine learning techniques to diagnose breast cancer from image-processed nuclear features of fine needle aspirates. Cancer Lett. 1994, 77, 163–171. [Google Scholar] [CrossRef]
- Yang, M.; Jaaks, P.; Dry, J.; Garnett, M.; Menden, M.P.; Saez-Rodriguez, J. Stratification and prediction of drug synergy based on target functional similarity. NPJ Syst. Biol. Appl. 2020, 6. [Google Scholar] [CrossRef]
- Holzinger, A.; Haibe-Kains, B.; Jurisica, I. Why imaging data alone is not enough: AI-based integration of imaging, omics, and clinical data. Eur. J. Nucl. Med. Mol. Imaging 2019, 46, 2722–2730. [Google Scholar] [CrossRef]
- Valentini, V.; Maurizi, F.; Tagliaferri, L.; Balducci, M.; Cellini, F.; Gambacorta, M.A.; Lanzotti, V.; Manfrida, S.; Mantini, G.; Mattiucci, G.C.; et al. Spider: Managing clinical data of cancer patients treated through a multidisciplinary approach by a palm based system. Public Health 2008, 5, 11. [Google Scholar]
- Altini, M.; Balzi, W.; Maltoni, R.; Falcini, F.; Foca, F.; Ioli, G.M.; Ricotti, A.; Bertetto, O.; Mistrangelo, M.; Amunni, G.; et al. Key performance indicators for monitoring the integrated care pathway in breast cancer: The E.Pic.A. project. AboutOpen 2019, 6, 31–38. [Google Scholar] [CrossRef]
- Carter, S.M.; Rogers, W.; Win, K.T.; Frazer, H.; Richards, B.; Houssami, N. The ethical, legal and social implications of using artificial intelligence systems in breast cancer care. Breast 2020, 49, 25–32. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Z.; Pi, Y.; Jiang, L.; Xiang, Y.; Wei, J.; Yang, P.; Zhang, W.; Zhong, X.; Zhou, K.; Li, Y.; et al. Deep neural network based artificial intelligence assisted diagnosis of bone scintigraphy for cancer bone metastasis. Sci. Rep. 2020, 10, 17046. [Google Scholar] [CrossRef]
- Xing, L.; Goetsch, S.; Cai, J. Artificial Intelligence should be part of medical physics graduate program curriculum. Med. Phys. 2020. [Google Scholar] [CrossRef] [PubMed]
- Schaffter, T.; Buist, D.S.; Lee, C.I.; Nikulin, Y.; Ribli, D.; Guan, Y.; Lotter, W.; Jie, Z.; Du, H.; Wang, S.; et al. Evaluation of Combined Artificial Intelligence and Radiologist Assessment to Interpret Screening Mammograms. JAMA Netw. Open 2020, 3, e200265. [Google Scholar] [CrossRef]
- Pantanowitz, L.; Hartman, D.; Qi, Y.; Cho, E.Y.; Suh, B.; Paeng, K.; Dhir, R.; Michelow, P.; Hazelhurst, S.; Song, S.Y.; et al. Accuracy and efficiency of an artificial intelligence tool when counting breast mitoses. Diagn. Pathol. 2020, 15, 80. [Google Scholar] [CrossRef]
- Raphael, M.J.; Saskin, R.; Singh, S. Association between waiting time for radiotherapy after surgery for early-stage breast cancer and survival outcomes in Ontario: A population-based outcomes study. Curr. Oncol. 2019, 27. [Google Scholar] [CrossRef]
- Fisher, B.; Bauer, M.; Margolese, R.; Poisson, R.; Pilch, Y.; Redmond, C.; Fisher, E.; Wolmark, N.; Deutsch, M.; Montague, E.; et al. Five-year results of a randomized clinical trial comparing total mastectomy and segmental mastectomy with or without radiation in the treatment of breast cancer. N. Engl. J. Med. 1985, 312, 665–673. [Google Scholar] [CrossRef]
- Recht, A.; Come, S.E.; Henderson, I.C.; Gelman, R.S.; Silver, B.; Hayes, D.F.; Shulman, L.N.; Harris, J.R. The Sequencing of Chemotherapy and Radiation Therapy after Conservative Surgery for Early-Stage Breast Cancer. N. Engl. J. Med. 1996, 334, 1356–1361. [Google Scholar] [CrossRef]
- Clark, R.M.; Whelan, T.; Levine, M.; Roberts, R.; Willan, A.; McCulloch, P.; Lipa, M.; Wilkinson, R.H.; Mahoney, L.J. Randomized Clinical Trial of Breast Irradiation Following Lumpectomy and Axillary Dissection for Node-Negative Breast Cancer: An Update. J. Natl. Cancer Inst. 1996, 88, 1659–1664. [Google Scholar] [CrossRef]
- Schnapper, G.; Marotti, L.; Casella, D.; Mano, M.P.; Mansel, R.E.; Ponti, A.; EUSOMABreast Centers Network Data Managers; Baldini, V.; Bassani, L.G.; Bissolotti, E.; et al. Data managers: A survey of the European Society of Breast Cancer Specialists in certified multi-disciplinary breast centers. Breast J. 2018, 24, 811–815. [Google Scholar] [CrossRef] [PubMed]
- Biganzoli, L.; Marotti, L.; Hart, C.D.; Cataliotti, L.; Cutuli, B.; Kühn, T.; Mansel, R.E.; Ponti, A.; Poortmans, P.; Regitnig, P.; et al. Quality indicators in breast cancer care: An update from the EUSOMA working group. Eur. J. Cancer 2017, 86, 59–81. [Google Scholar] [CrossRef] [PubMed]
- Tagliaferri, L.; Kovács, G.; Autorino, R.; Budrukkar, A.; Guinot, J.L.; Hildebrand, G.; Johansson, B.; Monge, R.M.; Meyer, J.E.; Niehoff, P.; et al. ENT COBRA (Consortium for Brachytherapy Data Analysis): Interdisciplinary standardized data collection system for head and neck patients treated with interventional radiotherapy (brachytherapy). J. Contemp. Brachytherapy 2016, 4, 336–343. [Google Scholar] [CrossRef] [PubMed]
- Tagliaferri, L.; Pagliara, M.M.; Masciocchi, C.; Scupola, A.; Azario, L.; Grimaldi, G.; Autorino, R.; Gambacorta, M.A.; Laricchiuta, A.; Boldrini, L.; et al. Nomogram for predicting radiation maculopathy in patients treated with Ruthenium-106 plaque brachytherapy for uveal melanoma. J. Contemp. Brachytherapy 2017, 9, 540–547. [Google Scholar] [CrossRef]
- Damiani, A.; Masciocchi, C.; Boldrini, L.; Gatta, R.; Dinapoli, N.; Lenkowicz, J.; Chiloiro, G.; Gambacorta, M.; Tagliaferri, L.; Autorino, R.; et al. Preliminary data analysis in healthcare multicentric data mining: A privacy-preserving distributed approach. J. E-Learn. Knowl. Soc. 2018, 14, 71–81. [Google Scholar]
- Damiani, A.; Onder, G.; Valentini, V. Large databases (Big Data) and evidence-based medicine. Eur. J. Intern. Med. 2018, 53. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Data Definition and Classification | ||
|---|---|---|
| Definition | Description | Example |
| Not organized, not “ontologized” data | Data to be constructed from other records and not captured by a pre-existing ontology system | For example, “Therapeutic indications from a Tumor Board” |
| Organized, not “ontologized” data | Records constructed but not captured by a pre-existing ontology system from begin | For example, “Data of radiotherapy beginning” or ICD9 code for diagnosis |
| Organized and “ontologized” data | Data captured by a pre-existing ontology system that can be directly recovered or is deposited in another software system | For example, data collected by data manager and data entry on dedicated web or hub systems |
| Archives and Channels Doors Definitions | |||
|---|---|---|---|
| Definition | Description | Type of Data Extraction | AI Technologies and Automatisms Performed |
| Platform based on ontology | Platform in use in our hospital for standardized data collection (BLADE, RedCAP, etc.). In this platform it is integrated a shared ontology that codifies data in unique, non-ambiguous way. | Organized and “ontologized” data | NEURAL NETWORKS |
| Datawarehouse used in Fondazione Policlinico Gemelli IRCCS | Data warehouses in use in our hospital for clinical assistance (SI, Aria, Speed (advanced evolution of Spider [10], Armonia, TrackCare, etc.). In these systems, data are codified based on clinical practice (e.g., Hb value, date of surgery, etc.), and are data validated by conventional clinical use | Organized, not “ontologized” data | NEURAL NETWORKS |
| Text mining extraction from PDF documents or electronic reports | All the electronic documents present in previous archives in which a procedure of text-mining extraction was applied to recover non-structured data. This is a very relevant part of data extraction, because we can recover a big quantity of granular information and translate it into structured data for usage in clinical practice and research. | Not organized, not “ontologized” data | TEXT MINING AUTOLEARN NEURAL NETWORKS |
| KPI Name | KPI Description |
|---|---|
| KPI pre-surgery | percentage of stage I and II breast cancer patients who underwent at least one radiological exam in the 60 days prior to the breast surgery |
| KPI post-surgery | percentage of stage I and II breast cancer patients who underwent at least one radiological exam within the 60 days after the surgery |
| KPI follow-up | percentage of stage I and II breast cancer patients who underwent at least one radiological exam from 60 days after the index breast surgery and up to 365 days after this surgery |
| KPI Subsequent Breast Reconstruction/Axillary dissection | percentage of patients with BC who underwent subsequent surgery |
| KPI subsequent breast surgery | percentage of patients with BC who underwent subsequent surgery following a partial resection |
| KPI chemotherapy timing | percentage of patients with BC who, as candidates for chemotherapy, initiated adjuvant treatment within 60 days of the index breast surgery |
| KPI radiotherapy timing | Percentage of patients who initiated radiotherapy within 180 days of the last surgery |
| KPI time of recovery | Percentage of patients who presented a recovery time in less than 7 days |
| KPI pathology exam | Percentage of patients who received a pathology exam in less than 15 days |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Marazzi, F.; Tagliaferri, L.; Masiello, V.; Moschella, F.; Colloca, G.F.; Corvari, B.; Sanchez, A.M.; Capocchiano, N.D.; Pastorino, R.; Iacomini, C.; et al. GENERATOR Breast DataMart—The Novel Breast Cancer Data Discovery System for Research and Monitoring: Preliminary Results and Future Perspectives. J. Pers. Med. 2021, 11, 65. https://doi.org/10.3390/jpm11020065
Marazzi F, Tagliaferri L, Masiello V, Moschella F, Colloca GF, Corvari B, Sanchez AM, Capocchiano ND, Pastorino R, Iacomini C, et al. GENERATOR Breast DataMart—The Novel Breast Cancer Data Discovery System for Research and Monitoring: Preliminary Results and Future Perspectives. Journal of Personalized Medicine. 2021; 11(2):65. https://doi.org/10.3390/jpm11020065
Chicago/Turabian StyleMarazzi, Fabio, Luca Tagliaferri, Valeria Masiello, Francesca Moschella, Giuseppe Ferdinando Colloca, Barbara Corvari, Alejandro Martin Sanchez, Nikola Dino Capocchiano, Roberta Pastorino, Chiara Iacomini, and et al. 2021. "GENERATOR Breast DataMart—The Novel Breast Cancer Data Discovery System for Research and Monitoring: Preliminary Results and Future Perspectives" Journal of Personalized Medicine 11, no. 2: 65. https://doi.org/10.3390/jpm11020065
APA StyleMarazzi, F., Tagliaferri, L., Masiello, V., Moschella, F., Colloca, G. F., Corvari, B., Sanchez, A. M., Capocchiano, N. D., Pastorino, R., Iacomini, C., Lenkowicz, J., Masciocchi, C., Patarnello, S., Franceschini, G., Gambacorta, M. A., Masetti, R., & Valentini, V. (2021). GENERATOR Breast DataMart—The Novel Breast Cancer Data Discovery System for Research and Monitoring: Preliminary Results and Future Perspectives. Journal of Personalized Medicine, 11(2), 65. https://doi.org/10.3390/jpm11020065