
Comparison of Risk of Metachronous Advanced Colorectal Neoplasia in Patients with Sporadic Adenomas Aged < 50 Versus ≥ 50 years: A Systematic Review and Meta-Analysis


Abstract
1. Introduction
2. Methods
2.1. Search Strategy
2.2. Inclusion/Exclusion Criteria
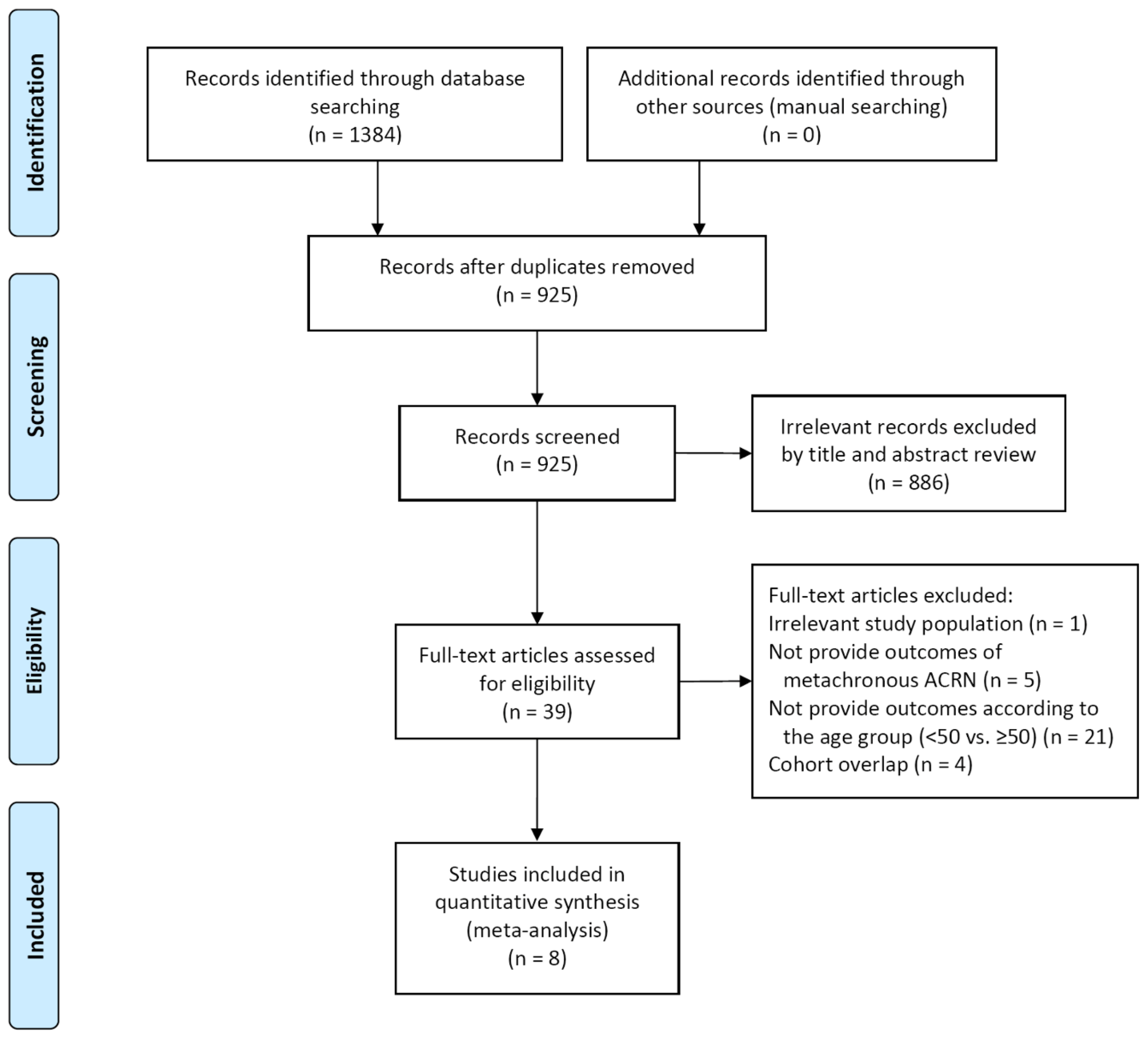
2.3. Study Selection
2.4. Assessment of Study Quality
2.5. Data Extraction
2.6. Study Endpoint
2.7. Statistical Analysis
3. Results
3.1. Study Selection and Characteristics
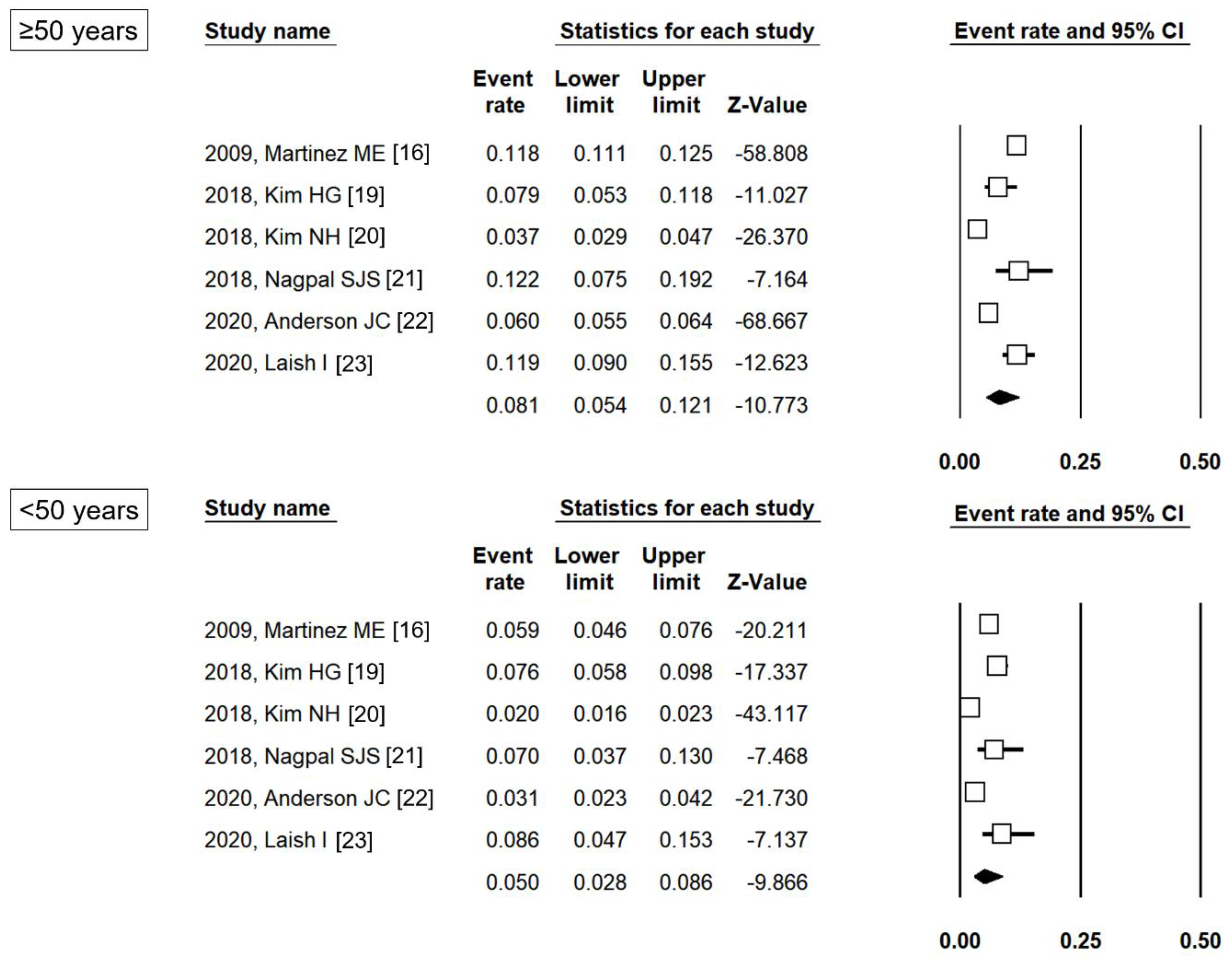
3.2. The Proportion of Patients with Metachronous ACRN According to Age Group
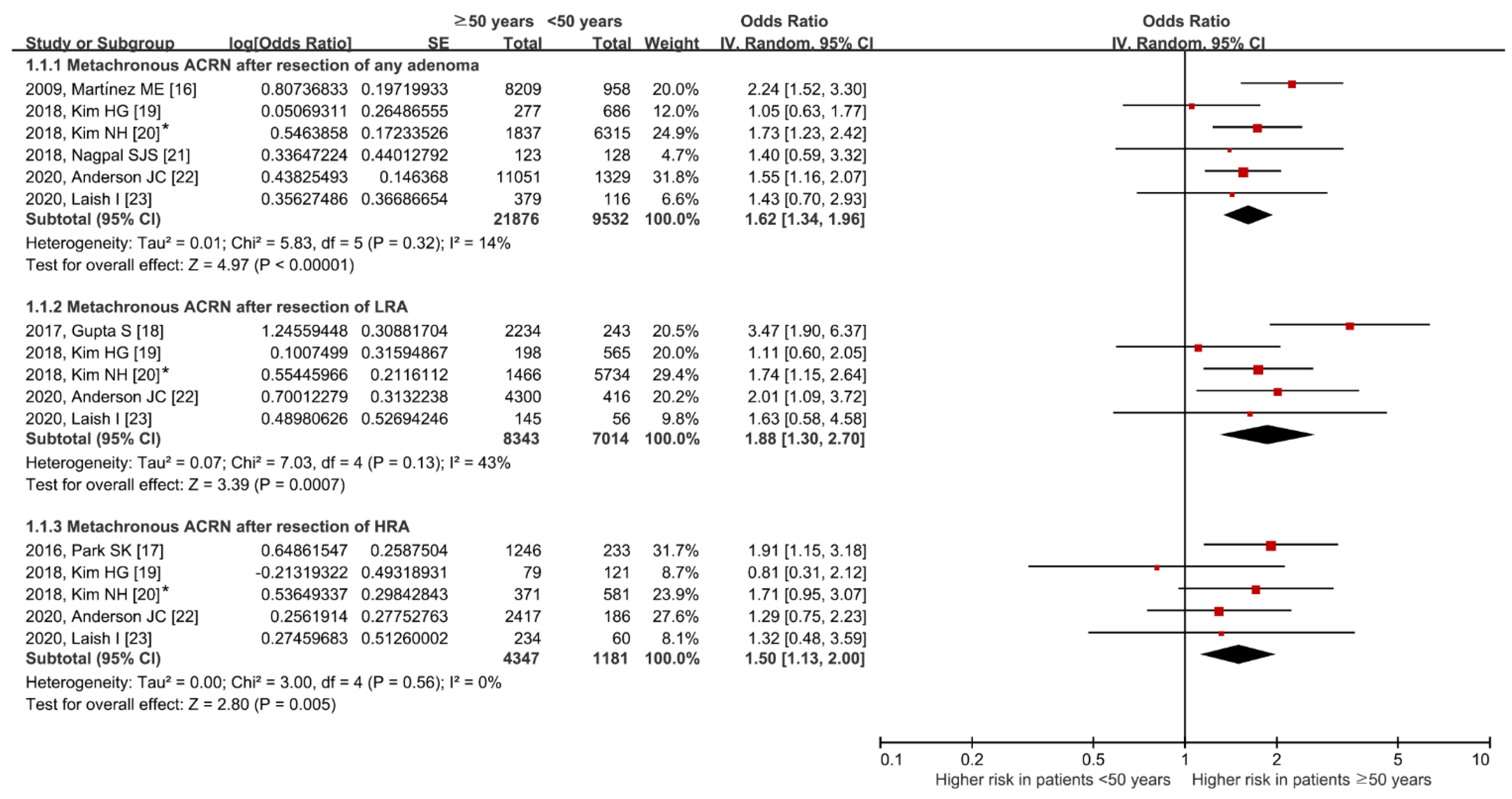
3.3. Comparative Risk of Metachronous ACRN According to Age Group
3.4. Sensitivity Analysis
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A. Detailed Search Strategy
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef]
- Bailey, C.E.; Hu, C.Y.; You, Y.N.; Bednarski, B.K.; Rodriguez-Bigas, M.A.; Skibber, J.M.; Cantor, S.B.; Chang, G.J. Increasing disparities in the age-related incidences of colon and rectal cancers in the United States, 1975–2010. JAMA Surg. 2015, 150, 17–22. [Google Scholar] [CrossRef] [PubMed]
- Vuik, F.E.; Nieuwenburg, S.A.; Bardou, M.; Lansdorp-Vogelaar, I.; Dinis-Ribeiro, M.; Bento, M.J.; Zadnik, V.; Pellisé, M.; Esteban, L.; Kaminski, M.F.; et al. Increasing incidence of colorectal cancer in young adults in Europe over the last 25 years. Gut 2019, 68, 1820–1826. [Google Scholar] [CrossRef]
- Siegel, R.L.; Fedewa, S.A.; Anderson, W.F.; Miller, K.D.; Ma, J.; Rosenberg, P.S.; Jemal, A. Colorectal Cancer Incidence Patterns in the United States, 1974–2013. J. Natl. Cancer Inst. 2017, 109. [Google Scholar] [CrossRef] [PubMed]
- Wolf, A.M.D.; Fontham, E.T.H.; Church, T.R.; Flowers, C.R.; Guerra, C.E.; LaMonte, S.J.; Etzioni, R.; McKenna, M.T.; Oeffinger, K.C.; Shih, Y.T.; et al. Colorectal cancer screening for average-risk adults: 2018 guideline update from the American Cancer Society. CA Cancer J. Clin. 2018, 68, 250–281. [Google Scholar] [CrossRef] [PubMed]
- Wong, M.C.S.; Huang, J.; Huang, J.L.W.; Pang, T.W.Y.; Choi, P.; Wang, J.; Chiang, J.I.; Jiang, J.Y. Global Prevalence of Colorectal Neoplasia: A Systematic Review and Meta-Analysis. Clin. Gastroenterol. Hepatol. 2020, 18, 553–561.e10. [Google Scholar] [CrossRef] [PubMed]
- Jung, Y.S.; Ryu, S.; Chang, Y.; Yun, K.E.; Park, J.H.; Kim, H.J.; Cho, Y.K.; Sohn, C.I.; Jeon, W.K.; Kim, B.I.; et al. Risk factors for colorectal neoplasia in persons aged 30 to 39 years and 40 to 49 years. Gastrointest. Endosc. 2015, 81, 637–645.e7. [Google Scholar] [CrossRef]
- Kim, N.H.; Jung, Y.S.; Yang, H.J.; Park, S.K.; Park, J.H.; Park, D.I.; Sohn, C.I. Prevalence of and Risk Factors for Colorectal Neoplasia in Asymptomatic Young Adults (20–39 Years Old). Clin. Gastroenterol. Hepatol. 2019, 17, 115–122. [Google Scholar] [CrossRef]
- Gupta, S.; Lieberman, D.; Anderson, J.C.; Burke, C.A.; Dominitz, J.A.; Kaltenbach, T.; Robertson, D.J.; Shaukat, A.; Syngal, S.; Rex, D.K. Recommendations for Follow-Up After Colonoscopy and Polypectomy: A Consensus Update by the US Multi-Society Task Force on Colorectal Cancer. Am. J. Gastroenterol. 2020, 115, 415–434. [Google Scholar] [CrossRef]
- Rutter, M.D.; East, J.; Rees, C.J.; Cripps, N.; Docherty, J.; Dolwani, S.; Kaye, P.V.; Monahan, K.J.; Novelli, M.R.; Plumb, A.; et al. British Society of Gastroenterology/Association of Coloproctology of Great Britain and Ireland/Public Health England post-polypectomy and post-colorectal cancer resection surveillance guidelines. Gut 2020, 69, 201–223. [Google Scholar] [CrossRef]
- Cha, J.M.; La Selva, D.; Kozarek, R.A.; Gluck, M.; Ross, A.; Lin, O.S. Young patients with sporadic colorectal adenomas: Current endoscopic surveillance practices and outcomes. Gastrointest. Endosc. 2018, 88, 818–825.e1. [Google Scholar] [CrossRef] [PubMed]
- Stang, A. Critical evaluation of the Newcastle-Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses. Eur. J. Epidemiol. 2010, 25, 603–605. [Google Scholar] [CrossRef]
- Higgins, J.P.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.; Green, S. Cochrane Handbook for Systematic Reviews of Interventions, Version 5.1.0. Available online: https://handbook-5-1.cochrane.org/ (accessed on 11 June 2020).
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. J. Clin. Epidemiol. 2009, 62, e1–e34. [Google Scholar] [CrossRef] [PubMed]
- Martínez, M.E.; Baron, J.A.; Lieberman, D.A.; Schatzkin, A.; Lanza, E.; Winawer, S.J.; Zauber, A.G.; Jiang, R.; Ahnen, D.J.; Bond, J.H.; et al. A pooled analysis of advanced colorectal neoplasia diagnoses after colonoscopic polypectomy. Gastroenterology 2009, 136, 832–841. [Google Scholar] [CrossRef]
- Park, S.K.; Kim, N.H.; Jung, Y.S.; Kim, W.H.; Eun, C.S.; Ko, B.M.; Seo, G.S.; Cha, J.M.; Park, J.J.; Kim, K.O.; et al. Risk of developing advanced colorectal neoplasia after removing high-risk adenoma detected at index colonoscopy in young patients: A KASID study. J. Gastroenterol. Hepatol. 2016, 31, 138–144. [Google Scholar] [CrossRef] [PubMed]
- Gupta, S.; Jacobs, E.T.; Baron, J.A.; Lieberman, D.A.; Murphy, G.; Ladabaum, U.; Cross, A.J.; Jover, R.; Liu, L.; Martinez, M.E. Risk stratification of individuals with low-risk colorectal adenomas using clinical characteristics: A pooled analysis. Gut 2017, 66, 446–453. [Google Scholar] [CrossRef]
- Kim, H.G.; Cho, Y.S.; Cha, J.M.; Shin, J.E.; Kim, K.O.; Yang, H.J.; Koo, H.S.; Joo, Y.E.; Boo, S.J. Risk of metachronous neoplasia on surveillance colonoscopy in young patients with colorectal neoplasia. Gastrointest. Endosc. 2018, 87, 666–673. [Google Scholar] [CrossRef]
- Kim, N.H.; Jung, Y.S.; Park, J.H.; Park, D.I.; Sohn, C.I. Risk of developing metachronous advanced colorectal neoplasia after colonoscopic polypectomy in patients aged 30 to 39 and 40 to 49 years. Gastrointest. Endosc. 2018, 88, 715–723. [Google Scholar] [CrossRef] [PubMed]
- Nagpal, S.J.S.; Mukhija, D.; Sanaka, M.; Lopez, R.; Burke, C.A. Metachronous colon polyps in younger versus older adults: A case-control study. Gastrointest. Endosc. 2018, 87, 657–665. [Google Scholar] [CrossRef]
- Anderson, J.C.; Robinson, C.M.; Butterly, L.F. Young adults and metachronous neoplasia: Risks for future advanced adenomas and large serrated polyps compared with older adults. Gastrointest. Endosc. 2020, 91, 669–675. [Google Scholar] [CrossRef] [PubMed]
- Laish, I.; Katz, L.; Ben-Horin, S.; Yablecovitch, D.; Naftali, T. Risk of metachronous neoplasia on surveillance colonoscopy among young and older patients after polypectomy. Dig. Liver Dis. 2020, 52, 427–433. [Google Scholar] [CrossRef] [PubMed]
- Pearlman, R.; Frankel, W.L.; Swanson, B.; Zhao, W.; Yilmaz, A.; Miller, K.; Bacher, J.; Bigley, C.; Nelsen, L.; Goodfellow, P.J.; et al. Prevalence and Spectrum of Germline Cancer Susceptibility Gene Mutations Among Patients With Early-Onset Colorectal Cancer. JAMA Oncol. 2017, 3, 464–471. [Google Scholar] [CrossRef] [PubMed]
- Mendelsohn, R.B.; Herzog, K.; Shia, J.; Rahaman, N.; Stadler, Z.K.; Shike, M. Molecular Screening for Lynch Syndrome in Young Patients With Colorectal Adenomas. Clin. Colorectal. Cancer 2017, 16, 173–177. [Google Scholar] [CrossRef]
- Velayos, F.S.; Allen, B.A.; Conrad, P.G.; Gum, J., Jr.; Kakar, S.; Chung, D.C.; Truta, B.; Sleisenger, M.H.; Kim, Y.S.; Terdiman, J.P. Low rate of microsatellite instability in young patients with adenomas: Reassessing the Bethesda guidelines. Am. J. Gastroenterol. 2005, 100, 1143–1149. [Google Scholar] [CrossRef] [PubMed]
- Kang, K.J.; Min, B.H.; Ryu, K.; Kim, K.M.; Kim, E.R.; Kim, J.Y.; Chang, D.K.; Kim, J.J.; Rhee, J.C.; Kim, Y.H. Clinical usefulness of microsatellite instability test in Korean young patients with high-risk features associated with adenoma. Clin. Res. Hepatol. Gastroenterol. 2012, 36, 378–383. [Google Scholar] [CrossRef] [PubMed]
- Wong, M.C.; Ding, H.; Wang, J.; Chan, P.S.; Huang, J. Prevalence and risk factors of colorectal cancer in Asia. Intest. Res. 2019, 17, 317–329. [Google Scholar] [CrossRef] [PubMed]
- Kim, T.J.; Kim, E.R.; Hong, S.N.; Kim, Y.H.; Baek, S.Y.; Ahn, S.; Chang, D.K. Adenoma detection rate influences the risk of metachronous advanced colorectal neoplasia in low-risk patients. Gastrointest. Endosc. 2018, 87, 809–817.e1. [Google Scholar] [CrossRef]
- Park, S.K.; Hwang, S.W.; Kim, K.O.; Cha, J.M.; Boo, S.J.; Shin, J.E.; Joo, Y.E.; Jung, Y.; Lee, J.; Yang, H.J.; et al. Risk of advanced colorectal neoplasm in patients with more than 10 adenomas on index colonoscopy: A Korean Association for the Study of Intestinal Diseases (KASID) study. J. Gastroenterol. Hepatol. 2017, 32, 803–808. [Google Scholar] [CrossRef]
- Lee, J.L.; Cha, J.M.; Lee, H.M.; Jeon, J.W.; Kwak, M.S.; Yoon, J.Y.; Shin, H.P.; Joo, K.R.; Lee, J.I.; Park, D.I. Determining the optimal surveillance interval after a colonoscopic polypectomy for the Korean population? Intest. Res. 2017, 15, 109–117. [Google Scholar] [CrossRef]
- Baik, S.J.; Park, H.; Park, J.J.; Lee, H.J.; Jo, S.Y.; Park, Y.M.; Lee, H.S. Advanced Colonic Neoplasia at Follow-up Colonoscopy According to Risk Components and Adenoma Location at Index Colonoscopy: A Retrospective Study of 1,974 Asymptomatic Koreans. Gut Liver 2017, 11, 667–673. [Google Scholar] [CrossRef] [PubMed]
- Van Heijningen, E.M.; Lansdorp-Vogelaar, I.; van Hees, F.; Kuipers, E.J.; Biermann, K.; de Koning, H.J.; van Ballegooijen, M.; Steyerberg, E.W. Developing a score chart to improve risk stratification of patients with colorectal adenoma. Endoscopy 2016, 48, 563–570. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Publication Year, FIRST Author | Study Design | Study Period | Country | Exclusion Criteria | Number of Patients | Male, % | Follow-Up Duration, Years | Quality Assessment (Newcastle–Ottawa Scale: Selection/Comparability/Outcome) | Metachronous ACRN | |
|---|---|---|---|---|---|---|---|---|---|---|
| Definition of Metachronous ACRN | Event and Number of Patients | |||||||||
| 2009, Martínez ME [16] | Pooled analysis using patient-level data from 7 randomized controlled trials and 1 cohort study | 1980–1999 (enrollment period) | USA | Most individual studies excluded the high-risk population for CRC such as hereditary CRC syndrome * | 9167 | 71.2 | Median 47.2 (IQR 6.1–91.4) | All individual studies were assessed as having a high quality * | High-grade dysplasia, villous adenoma, or adenoma ≥ 10 mm | <50 years: 57/958 ≥50 years: 967/8209 |
| 2016, Park SK [17] | Retrospective, multicenter cohort | 2004–2006 (enrollment period) | Korea | Polyposis syndrome, a history of CRC, surgical resection of the intestine, IBD, incomplete procedures | 1479 | 73.8 | <50 years: mean 4.1 (SD 1.4) 50–70 years: mean 4.0 (SD 1.4) ≥70 years: mean 4.0 (SD 1.5) | 4/1/3 | High-grade dysplasia, villous adenoma, adenoma ≥ 10 mm, or cancer | <50 years: 18/233 ≥50 years: 172/1246 |
| 2017, Gupta S [18] | Pooled analysis using patient-level data from six randomized controlled trials and one cohort study | 1984–1999 (enrollment period) | USA | Most individual studies excluded the high-risk population for CRC, such as hereditary CRC syndrome * | 2477 | 73.7 | N/A | All individual studies were assessed as having a high quality * | High-grade dysplasia, villous adenoma, or adenoma ≥ 10 mm | <50 years: 7/243 ≥50 years: 181/2234 |
| 2018, Kim HG [19] | Retrospective, multicenter cohort | 2006–2015 | Korea | A strong family history of CRC, genetic syndromes, multiple (>16) adenomas at index colonoscopy, IBD, CRC, any malignancy, incomplete procedures, previous colorectal surgery | 2709 | 59.2 | N/A | 4/1/3 | High-grade dysplasia, villous adenoma, adenoma ≥ 10 mm, or cancer | 20–49 years: 52/686 50–54 years: 22/277 |
| 2018, Kim NH [20] | Retrospective cohort | 2010–2017 | Korea | A history of CRC or colorectal surgery, IBD, poor bowel preparation | 10014 | 82.9 | Mean 3.4 (SD 1.4) | 4/2/3 | High-grade dysplasia, villous adenoma, adenoma ≥ 10 mm, or cancer | 30-49 years: 124/6315 ≥50 years: 68/1837 |
| 2018, Nagpal SJS [21] | Case-control | 1984–2012 | USA | A personal or family history of hereditary CRC syndromes, Incomplete colonoscopy, previous colon surgery, history of CRC, IBD | 251 | 47.4 | <50 years: median 2.8 (IQR 1.3–3.9) ≥50 years: median 4.1 (IQR 2.9–5.2) | 4/2/3 | SSP with dysplasia, TSA, high-grade dysplasia, villous adenoma, adenoma ≥ 10 mm, or cancer | <50 years: 9/128 ≥50 years: 15/123 |
| 2020, Anderson JC [22] | Retrospective cohort | N/A | USA | Familial syndromes, IBD, incomplete colonoscopy, poor bowel preparation | 12380 | 54.8 | <40 years: mean 4.0 (SD 2.4) 40–49 years: mean 4.6 (SD 2.3) 50–59 years: mean 4.8 (SD 2.2) ≥60 years: mean 4.3 (SD 1.9) | 4/2/3 | High-grade dysplasia, villous adenoma, adenoma ≥ 10 mm, or cancer | <50 years: 41/1329 ≥50 years: 660/11051 |
| 2020, Laish I [23] | Retrospective cohort | 2005–2015 | Israel | A strong family history of CRC, hereditary syndrome, multiple (≥10) adenomas at index colonoscopy, previous colonoscopies with removal of polyps, IBD, history of CRC, previous bowel resection, incomplete procedures, ≥3 non-advanced adenomas at index colonoscopy | 496 | 49.4 | Low risk adenoma group: median 5.0 Advanced adenoma group: median 3.0 | 4/1/3 | High-grade dysplasia, villous adenoma, adenoma ≥ 10 mm, SSP ≥ 10 mm, SSP with dysplasia, or cancer | <50 years: 10/116 ≥50 years: 45/379 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jung, Y.S.; Park, J.H.; Park, C.H. Comparison of Risk of Metachronous Advanced Colorectal Neoplasia in Patients with Sporadic Adenomas Aged < 50 Versus ≥ 50 years: A Systematic Review and Meta-Analysis. J. Pers. Med. 2021, 11, 120. https://doi.org/10.3390/jpm11020120
Jung YS, Park JH, Park CH. Comparison of Risk of Metachronous Advanced Colorectal Neoplasia in Patients with Sporadic Adenomas Aged < 50 Versus ≥ 50 years: A Systematic Review and Meta-Analysis. Journal of Personalized Medicine. 2021; 11(2):120. https://doi.org/10.3390/jpm11020120
Chicago/Turabian StyleJung, Yoon Suk, Jung Ho Park, and Chan Hyuk Park. 2021. "Comparison of Risk of Metachronous Advanced Colorectal Neoplasia in Patients with Sporadic Adenomas Aged < 50 Versus ≥ 50 years: A Systematic Review and Meta-Analysis" Journal of Personalized Medicine 11, no. 2: 120. https://doi.org/10.3390/jpm11020120
APA StyleJung, Y. S., Park, J. H., & Park, C. H. (2021). Comparison of Risk of Metachronous Advanced Colorectal Neoplasia in Patients with Sporadic Adenomas Aged < 50 Versus ≥ 50 years: A Systematic Review and Meta-Analysis. Journal of Personalized Medicine, 11(2), 120. https://doi.org/10.3390/jpm11020120