
Documenting Pharmacogenomic Test Results in Electronic Health Records: Practical Considerations for Primary Care Teams


Abstract
:1. The Problem
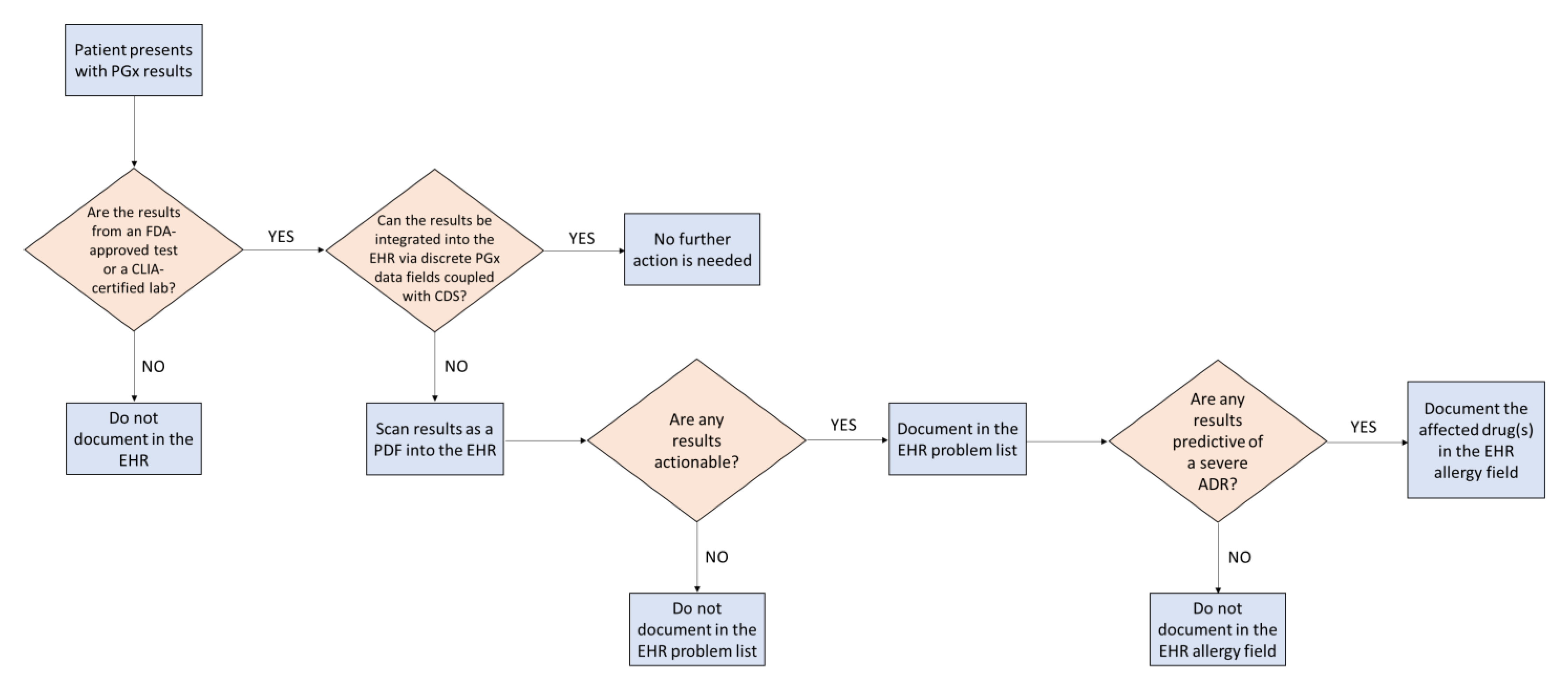
2. Proposed Solutions
Funding
Conflicts of Interest
References
- Hull, L.E.; Lehmann, L.S.; Lynch, J.A. Gene-Based Prescribing Is Here. Are Providers Ready? Am. J. Med. 2019, 132, 1009–1010. [Google Scholar] [CrossRef] [PubMed]
- Empey, P.E.; Pratt, V.M.; Hoffman, J.M.; Caudle, K.E.; Klein, T.E. Expanding evidence leads to new pharmacogenomics payer coverage. Genet. Med. 2021, 23, 830–832. [Google Scholar] [CrossRef] [PubMed]
- FDA. Authorizes First Direct-to-Consumer Test for Detecting Genetic Variants that May Be Associated with Medication Metabolism. Available online: https://www.fda.gov/news-events/press-announcements/fda-authorizes-first-direct-consumer-test-detecting-genetic-variants-may-be-associated-medication (accessed on 24 November 2020).
- Dunnenberger, H.M.; Biszewski, M.; Bell, G.C.; Sereika, A.; May, H.; Johnson, S.G.; Hulick, P.J.; Khandekar, J. Implementation of a multidisciplinary pharmacogenomics clinic in a community health system. Am. J. Health Syst. Pharm. 2016, 73, 1956–1966. [Google Scholar] [CrossRef]
- Arwood, M.J.; Dietrich, E.A.; Duong, B.Q.; Smith, D.M.; Cook, K.; Elchynski, A.; Rosenberg, E.I.; Huber, K.N.; Nagoshi, Y.L.; Wright, A.; et al. Design and Early Implementation Successes and Challenges of a Pharmacogenetics Consult Clinic. J. Clin. Med. 2020, 9, 2274. [Google Scholar] [CrossRef]
- All of Us Research Program Investigators; Denny, J.C.; Rutter, J.L.; Goldstein, D.B.; Philippakis, A.; Smoller, J.W.; Jenkins, G.; Dishman, E. The “All of Us” Research Program. N. Engl. J. Med. 2019, 381, 668–676. [Google Scholar]
- Dong, O.M.; Bates, J.; Chanfreau-Coffinier, C.; Naglich, M.; Kelley, M.J.; Meyer, L.J.; Icardi, M.; Vassy, J.L.; Sriram, P.; Heise, C.W.; et al. Veterans Affairs Pharmacogenomic Testing for Veterans (PHASER) clinical program. Pharmacogenomics 2021, 22, 137–144. [Google Scholar] [CrossRef] [PubMed]
- Dunnenberger, H.M.; Crews, K.R.; Hoffman, J.M.; Caudle, K.E.; Broeckel, U.; Howard, S.C.; Hunkler, R.J.; Klein, T.E.; Evans, W.E.; Relling, M.V. Preemptive clinical pharmacogenetics implementation: Current programs in five US medical centers. Annu. Rev. Pharmacol. Toxicol. 2015, 55, 89–106. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, D.; Olson, K.L.; Manzi, S.F.; Mandl, K.D. Patients dispensed medications with actionable pharmacogenomic biomarkers: Rates and characteristics. Genet. Med. 2021, 23, 782–786. [Google Scholar] [CrossRef] [PubMed]
- Kimpton, J.E.; Carey, I.M.; Threapleton, C.J.D.; Robinson, A.; Harris, T.; Cook, D.G.; DeWilde, S.; Baker, E.H. Longitudinal exposure of English primary care patients to pharmacogenomic drugs: An analysis to inform design of pre-emptive pharmacogenomic testing. Br. J. Clin. Pharmacol. 2019, 85, 2734–2746. [Google Scholar] [CrossRef] [PubMed]
- Chanfreau-Coffinier, C.; Hull, L.E.; Lynch, J.A.; Duvall, S.L.; Damrauer, S.M.; Cunningham, F.E.; Voight, B.F.; Matheny, M.; Oslin, D.W.; Icardi, M.S.; et al. Projected Prevalence of Actionable Pharmacogenetic Variants and Level A Drugs Prescribed Among US Veterans Health Administration Pharmacy Users. JAMA Netw. Open 2019, 2, e195345. [Google Scholar] [CrossRef] [PubMed]
- Table of Pharmacogenomic Biomarkers in Drug Labeling. Available online: https://www.fda.gov/drugs/science-and-research-drugs/table-pharmacogenomic-biomarkers-drug-labeling (accessed on 24 November 2020).
- Relling, M.V.; Klein, T.E.; Gammal, R.S.; Whirl-Carrillo, M.; Hoffman, J.M.; Caudle, K.E. The Clinical Pharmacogenetics Implementation Consortium: 10 Years Later. Clin. Pharmacol. Ther. 2020, 107, 171–175. [Google Scholar] [CrossRef] [PubMed]
- CPIC Guidelines. Available online: https://cpicpgx.org/guidelines/ (accessed on 8 September 2021).
- Rollinson, V.; Turner, R.; Pirmohamed, M. Pharmacogenomics for Primary Care: An Overview. Genes 2020, 11, 1337. [Google Scholar] [CrossRef] [PubMed]
- Hicks, J.K.; Dunnenberger, H.M.; Gumpper, K.F.; Haidar, C.E.; Hoffman, J.M. Integrating pharmacogenomics into electronic health records with clinical decision support. Am. J. Health Syst. Pharm. 2016, 73, 1967–1976. [Google Scholar] [CrossRef] [PubMed]
- Liu, M.; Vnencak-Jones, C.L.; Roland, B.P.; Gatto, C.L.; Mathe, J.L.; Just, S.L.; Peterson, J.F.; Van Driest, S.L.; Weitkamp, A.O. A Tutorial for Pharmacogenomics Implementation Through End-to-End Clinical Decision Support Based on Ten Years of Experience from PREDICT. Clin. Pharmacol. Ther. 2020, 109, 101–115. [Google Scholar] [CrossRef] [PubMed]
- Danahey, K.; Borden, B.A.; Furner, B.; Yukman, P.; Hussain, S.; Saner, D.; Volchenboum, S.L.; Ratain, M.J.; O’Donnell, P.H. Simplifying the use of pharmacogenomics in clinical practice: Building the genomic prescribing system. J. Biomed Inform. 2017, 75, 110–121. [Google Scholar] [CrossRef] [PubMed]
- Hoffman, J.M.; Haidar, C.E.; Wilkinson, M.R.; Crews, K.R.; Baker, D.K.; Kornegay, N.M.; Yang, W.; Pui, C.; Reiss, U.M.; Gaur, A.H.; et al. PG4KDS: A model for the clinical implementation of pre-emptive pharmacogenetics. Am. J. Med. Genet. Part C Semin. Med. Genet. 2014, 166C, 45–55. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gammal, R.S.; Mayes, J.; Caudle, K.E. Ready or not, here it comes: Direct-to-consumer pharmacogenomic testing and its implications for community pharmacists. J. Am. Pharm. Assoc. 2019, 59, 646–650. [Google Scholar] [CrossRef] [PubMed]
- FDA Grants 23andMe Clearance to Offer Interpretive Drug Information for Two Medications. Available online: https://blog.23andme.com/news/pharmacogenetics-report/ (accessed on 23 November 2021).
- Caudle, K.E.; Dunnenberger, H.M.; Freimuth, R.; Peterson, J.F.; Burlison, J.D.; Whirl-Carrillo, M.; Scott, S.A.; Rehm, H.L.; Williams, M.S.; Klein, T.E.; et al. Standardizing terms for clinical pharmacogenetic test results: Consensus terms from the Clinical Pharmacogenetics Implementation Consortium (CPIC). Genet. Med. 2017, 19, 215–223. [Google Scholar] [CrossRef] [PubMed]
- Congress., H.R. 34-21st Century Cures Act. Published 2016. Available online: https://www.congress.gov/bill/114th-congress/house-bill/34/text (accessed on 31 August 2021).
- Everson, J.; Patel, V.; Adler-Milstein, J. Information blocking remains prevalent at the start of 21st Century Cures Act: Results from a survey of health information exchange organizations. J. Am. Med. Inform. Assoc. 2021, 28, 727–732. [Google Scholar] [CrossRef] [PubMed]
- Empey, P.E.; Stevenson, J.M.; Tuteja, S.; Weitzel, K.W.; Angiolillo, D.J.; Beitelshees, A.L.; Coons, J.C.; Duarte, J.D.; Franchi, F.; Jeng, L.J.B.; et al. Multisite Investigation of Strategies for the Implementation of CYP2C19 Genotype-Guided Antiplatelet Therapy. Clin. Pharmacol. Ther. 2018, 104, 664–674. [Google Scholar] [CrossRef] [PubMed] [Green Version]

{kind=link}
| Medications | Genes |
|---|---|
| Cardiology | |
| Clopidogrel | CYP2C19 |
| Simvastatin | SLCO1B1 |
| Warfarin | CYP2C9, CYP4F2, VKORC1 |
| Gastroenterology | |
| Dexlansoprazole | CYP2C19 |
| Lansoprazole | CYP2C19 |
| Metoclopramide | CYP2D6 |
| Omeprazole | CYP2C19 |
| Ondansetron | CYP2D6 |
| Pantoprazole | CYP2C19 |
| Immunosuppressants | |
| Azathioprine | NUDT15, TPMT |
| Mercaptopurine | NUDT15, TPMT |
| Tacrolimus | CYP3A5 |
| Infectious Disease | |
| Abacavir | HLA-B |
| Atazanavir | UGT1A1 |
| Efavirenz | CYP2B6 |
| Voriconazole | CYP2C19 |
| Neurology | |
| Carbamazepine | HLA-A, HLA-B |
| Oxcarbazepine | HLA-B |
| Phenytoin | CYP2C9, HLA-B |
| Pain Management | |
| Celecoxib | CYP2C9 |
| Codeine | CYP2D6 |
| Flurbiprofen | CYP2C9 |
| Hydrocodone | CYP2D6 |
| Ibuprofen | CYP2C9 |
| Meloxicam | CYP2C9 |
| Piroxicam | CYP2C9 |
| Tramadol | CYP2D6 |
| Psychiatry | |
| Amitriptyline | CYP2D6, CYP2C19 |
| Aripiprazole | CYP2D6 |
| Atomoxetine | CYP2D6 |
| Brexpiprazole | CYP2D6 |
| Citalopram | CYP2C19 |
| Clobazam | CYP2C19 |
| Clomipramine | CYP2D6, CYP2C19 |
| Desipramine | CYP2D6 |
| Doxepin | CYP2D6, CYP2C19 |
| Escitalopram | CYP2C19 |
| Fluvoxamine | CYP2D6 |
| Imipramine | CYP2D6, CYP2C19 |
| Nortriptyline | CYP2D6 |
| Paroxetine | CYP2D6 |
| Pimozide | CYP2D6 |
| Sertraline | CYP2C19 |
| Trimipramine | CYP2D6, CYP2C19 |
| Vortioxetine | CYP2D6 |
| Urate-Lowering Therapy | |
| Allopurinol | HLA-B |
| Rasburicase | G6PD |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gammal, R.S.; Berenbrok, L.A.; Empey, P.E.; Massart, M.B. Documenting Pharmacogenomic Test Results in Electronic Health Records: Practical Considerations for Primary Care Teams. J. Pers. Med. 2021, 11, 1296. https://doi.org/10.3390/jpm11121296
Gammal RS, Berenbrok LA, Empey PE, Massart MB. Documenting Pharmacogenomic Test Results in Electronic Health Records: Practical Considerations for Primary Care Teams. Journal of Personalized Medicine. 2021; 11(12):1296. https://doi.org/10.3390/jpm11121296
Chicago/Turabian StyleGammal, Roseann S., Lucas A. Berenbrok, Philip E. Empey, and Mylynda B. Massart. 2021. "Documenting Pharmacogenomic Test Results in Electronic Health Records: Practical Considerations for Primary Care Teams" Journal of Personalized Medicine 11, no. 12: 1296. https://doi.org/10.3390/jpm11121296
APA StyleGammal, R. S., Berenbrok, L. A., Empey, P. E., & Massart, M. B. (2021). Documenting Pharmacogenomic Test Results in Electronic Health Records: Practical Considerations for Primary Care Teams. Journal of Personalized Medicine, 11(12), 1296. https://doi.org/10.3390/jpm11121296