
Risk of Re-Rupture, Vasospasm, or Re-Stroke after Clipping or Coiling of Ruptured Intracranial Aneurysms: Long-Term Follow-Up with a Propensity Score-Matched, Population-Based Cohort Study


Abstract
:1. Introduction
2. Patients and Methods
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bederson, J.B.; Connolly, E.S., Jr.; Batjer, H.H.; Dacey, R.G.; Dion, J.E.; Diringer, M.N.; Duldner, J.E., Jr.; Harbaugh, R.E.; Patel, A.B.; Rosenwasser, R.H.; et al. Guidelines for the management of aneurysmal subarachnoid hemorrhage: A statement for healthcare professionals from a special writing group of the Stroke Council, American Heart Association. Stroke 2009, 40, 994–1025. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Connolly, E.S., Jr.; Rabinstein, A.A.; Carhuapoma, J.R.; Derdeyn, C.P.; Dion, J.; Higashida, R.T.; Hoh, B.L.; Kirkness, C.J.; Naidech, A.M.; Ogilvy, C.S.; et al. Guidelines for the management of aneurysmal subarachnoid hemorrhage: A guideline for healthcare professionals from the American Heart Association/american Stroke Association. Stroke 2012, 43, 1711–1737. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dovey, Z.; Misra, M.; Thornton, J.; Charbel, F.T.; Debrun, G.M.; Ausman, J.I. Guglielmi detachable coiling for intracranial aneurysms: The story so far. Arch. Neurol. 2001, 58, 559–564. [Google Scholar] [CrossRef]
- Francoeur, C.L.; Mayer, S.A. Management of delayed cerebral ischemia after subarachnoid hemorrhage. Crit. Care 2016, 20, 277. [Google Scholar] [CrossRef] [Green Version]
- Hillman, J.; Fridriksson, S.; Nilsson, O.; Yu, Z.; Saveland, H.; Jakobsson, K.E. Immediate administration of tranexamic acid and reduced incidence of early rebleeding after aneurysmal subarachnoid hemorrhage: A prospective randomized study. J. Neurosurg. 2002, 97, 771–778. [Google Scholar] [CrossRef] [PubMed]
- Naidech, A.M.; Janjua, N.; Kreiter, K.T.; Ostapkovich, N.D.; Fitzsimmons, B.F.; Parra, A.; Commichau, C.; Connolly, E.S.; Mayer, S.A. Predictors and impact of aneurysm rebleeding after subarachnoid hemorrhage. Arch. Neurol. 2005, 62, 410–416. [Google Scholar] [CrossRef] [Green Version]
- Ohkuma, H.; Tsurutani, H.; Suzuki, S. Incidence and significance of early aneurysmal rebleeding before neurosurgical or neurological management. Stroke 2001, 32, 1176–1180. [Google Scholar] [CrossRef] [Green Version]
- Kassell, N.F.; Torner, J.C. Aneurysmal rebleeding: A preliminary report from the Cooperative Aneurysm Study. Neurosurgery 1983, 13, 479–481. [Google Scholar] [CrossRef]
- Wilkins, R.H. Aneurysm rupture during angiography: Does acute vasospasm occur? Surg. Neurol. 1976, 5, 299–303. [Google Scholar]
- Baldwin, M.E.; Macdonald, R.L.; Huo, D.; Novakovic, R.L.; Goldenberg, F.D.; Frank, J.I.; Rosengart, A.J. Early vasospasm on admission angiography in patients with aneurysmal subarachnoid hemorrhage is a predictor for in-hospital complications and poor outcome. Stroke 2004, 35, 2506–2511. [Google Scholar] [CrossRef] [Green Version]
- Suarez, J.I. Diagnosis and Management of Subarachnoid Hemorrhage. Continuum (Minneap Minn) 2015, 21, 1263–1287. [Google Scholar] [CrossRef]
- Rowland, M.J.; Hadjipavlou, G.; Kelly, M.; Westbrook, J.; Pattinson, K.T. Delayed cerebral ischaemia after subarachnoid haemorrhage: Looking beyond vasospasm. Br. J. Anaesth. 2012, 109, 315–329. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Helbok, R.; Kurtz, P.; Vibbert, M.; Schmidt, M.J.; Fernandez, L.; Lantigua, H.; Ostapkovich, N.D.; Connolly, S.E.; Lee, K.; Claassen, J.; et al. Early neurological deterioration after subarachnoid haemorrhage: Risk factors and impact on outcome. J. Neurol. Neurosurg. Psychiatry 2013, 84, 266–270. [Google Scholar] [CrossRef] [Green Version]
- Rosengart, A.J.; Schultheiss, K.E.; Tolentino, J.; Macdonald, R.L. Prognostic factors for outcome in patients with aneurysmal subarachnoid hemorrhage. Stroke 2007, 38, 2315–2321. [Google Scholar] [CrossRef] [Green Version]
- Macdonald, R.L.; Hunsche, E.; Schuler, R.; Wlodarczyk, J.; Mayer, S.A. Quality of life and healthcare resource use associated with angiographic vasospasm after aneurysmal subarachnoid hemorrhage. Stroke 2012, 43, 1082–1088. [Google Scholar] [CrossRef] [Green Version]
- Rabinstein, A.A.; Friedman, J.A.; Weigand, S.D.; McClelland, R.L.; Fulgham, J.R.; Manno, E.M.; Atkinson, J.L.; Wijdicks, E.F. Predictors of cerebral infarction in aneurysmal subarachnoid hemorrhage. Stroke 2004, 35, 1862–1866. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Luckl, J.; Lemale, C.L.; Kola, V.; Horst, V.; Khojasteh, U.; Oliveira-Ferreira, A.I.; Major, S.; Winkler, M.K.L.; Kang, E.J.; Schoknecht, K.; et al. The negative ultraslow potential, electrophysiological correlate of infarction in the human cortex. Brain 2018, 141, 1734–1752. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dreier, J.P. The role of spreading depression, spreading depolarization and spreading ischemia in neurological disease. Nat. Med. 2011, 17, 439–447. [Google Scholar] [CrossRef]
- Wen, C.P.; Tsai, S.P.; Chung, W.S. A 10-year experience with universal health insurance in Taiwan: Measuring changes in health and health disparity. Ann. Intern. Med. 2008, 148, 258–267. [Google Scholar] [CrossRef] [Green Version]
- Shao, Y.J.; Chan, T.S.; Tsai, K.; Wu, S.Y. Association between proton pump inhibitors and the risk of hepatocellular carcinoma. Aliment. Pharmacol. Ther. 2018, 48, 460–468. [Google Scholar] [CrossRef]
- Lin, W.C.; Ding, Y.F.; Hsu, H.L.; Chang, J.H.; Yuan, K.S.; Wu, A.T.H.; Chow, J.M.; Chang, C.L.; Chen, S.U.; Wu, S.Y. Value and application of trimodality therapy or definitive concurrent chemoradiotherapy in thoracic esophageal squamous cell carcinoma. Cancer 2017, 123, 3904–3915. [Google Scholar] [CrossRef] [Green Version]
- Yen, Y.C.; Chang, J.H.; Lin, W.C.; Chiou, J.F.; Chang, Y.C.; Chang, C.L.; Hsu, H.L.; Chow, J.M.; Yuan, K.S.; Wu, A.T.H.; et al. Effectiveness of esophagectomy in patients with thoracic esophageal squamous cell carcinoma receiving definitive radiotherapy or concurrent chemoradiotherapy through intensity-modulated radiation therapy techniques. Cancer 2017, 123, 2043–2053. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chang, S.C.; Chen, H.M.; Wu, S.Y. There Are No Differences in Positive Surgical Margin Rates or Biochemical Failure-Free Survival among Patients Receiving Open, Laparoscopic, or Robotic Radical Prostatectomy: A Nationwide Cohort Study from the National Cancer Database. Cancers 2020, 13, 106. [Google Scholar] [CrossRef] [PubMed]
- Chang, S.C.; Hsu, C.H.; Lin, Y.C.; Wu, S.Y. Effects of 1-Year Hospital Volume on Surgical Margin and Biochemical-Failure-Free Survival in Patients Undergoing Robotic versus Nonrobotic Radical Prostatectomy: A Nationwide Cohort Study from the National Taiwan Cancer Database. Cancers 2021, 13, 488. [Google Scholar] [CrossRef]
- Wu, S.Y.; Fang, S.C.; Shih, H.J.; Wen, Y.C.; Shao, Y.J. Mortality associated with statins in men with advanced prostate cancer treated with androgen deprivation therapy. Eur. J. Cancer 2019, 112, 109–117. [Google Scholar] [CrossRef] [PubMed]
- Liu, W.C.; Liu, H.E.; Kao, Y.W.; Qin, L.; Lin, K.C.; Fang, C.Y.; Tsai, L.L.; Shia, B.C.; Wu, S.Y. Definitive intensity-modulated radiotherapy or surgery for early oral cavity squamous cell carcinoma: Propensity-score-matched, nationwide, population-based cohort study. Head Neck 2020. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.C.; Wang, T.J.; Sung, L.C.; Kao, P.F.; Yang, T.Y.; Hao, W.R.; Chen, C.C.; Hsu, Y.P.; Wu, S.Y. Influenza vaccination reduces hemorrhagic stroke risk in patients with atrial fibrillation: A population-based cohort study. Int. J. Cardiol. 2017, 232, 315–323. [Google Scholar] [CrossRef]
- Lin, K.C.; Tsai, L.L.; Ko, E.C.; Sheng-Po Yuan, K.; Wu, S.Y. Comorbidity profiles among patients with recurrent aphthous stomatitis: A case-control study. J. Formos. Med. Assoc. 2019, 118, 664–670. [Google Scholar] [CrossRef]
- Charlson, M.; Szatrowski, T.P.; Peterson, J.; Gold, J. Validation of a combined comorbidity index. J. Clin. Epidemiol. 1994, 47, 1245–1251. [Google Scholar] [CrossRef]
- Chen, J.H.; Yen, Y.C.; Yang, H.C.; Liu, S.H.; Yuan, S.P.; Wu, L.L.; Lee, F.P.; Lin, K.C.; Lai, M.T.; Wu, C.C.; et al. Curative-Intent Aggressive Treatment Improves Survival in Elderly Patients With Locally Advanced Head and Neck Squamous Cell Carcinoma and High Comorbidity Index. Medicine (Baltimore) 2016, 95, e3268. [Google Scholar] [CrossRef]
- Grambsch, P.M. Goodness-of-fit and diagnostics for proportional hazards regression models. Cancer Treat Res. 1995, 75, 95–112. [Google Scholar] [PubMed]
- D’Agostino, R.B., Jr. Propensity score methods for bias reduction in the comparison of a treatment to a non-randomized control group. Stat. Med. 1998, 17, 2265–2281. [Google Scholar] [CrossRef]
- Lau, B.; Cole, S.R.; Gange, S.J. Competing risk regression models for epidemiologic data. Am. J. Epidemiol. 2009, 170, 244–256. [Google Scholar] [CrossRef] [PubMed]
- Austin, P.C. Balance diagnostics for comparing the distribution of baseline covariates between treatment groups in propensity-score matched samples. Stat. Med. 2009, 28, 3083–3107. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nguyen, T.L.; Collins, G.S.; Spence, J.; Daures, J.P.; Devereaux, P.J.; Landais, P.; Le Manach, Y. Double-adjustment in propensity score matching analysis: Choosing a threshold for considering residual imbalance. BMC Med. Res. Methodol. 2017, 17, 78. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Z.; Kim, H.J.; Lonjon, G.; Zhu, Y.; written on behalf of AME Big-Data Clinical Trial Collaborative Group. Balance diagnostics after propensity score matching. Ann. Transl. Med. 2019, 7, 16. [Google Scholar] [CrossRef]
- Schaafsma, J.D.; Sprengers, M.E.; van Rooij, W.J.; Sluzewski, M.; Majoie, C.B.; Wermer, M.J.; Rinkel, G.J. Long-term recurrent subarachnoid hemorrhage after adequate coiling versus clipping of ruptured intracranial aneurysms. Stroke 2009, 40, 1758–1763. [Google Scholar] [CrossRef] [Green Version]
- Abulhasan, Y.B.; Alabdulraheem, N.; Simoneau, G.; Angle, M.R.; Teitelbaum, J. Mortality after Spontaneous Subarachnoid Hemorrhage: Causality and Validation of a Prediction Model. World Neurosurg. 2018, 112, e799–e811. [Google Scholar] [CrossRef]
- Vergouwen, M.D.; Jong-Tjien-Fa, A.V.; Algra, A.; Rinkel, G.J. Time trends in causes of death after aneurysmal subarachnoid hemorrhage: A hospital-based study. Neurology 2016, 86, 59–63. [Google Scholar] [CrossRef]
- Roos, Y.B.; de Haan, R.J.; Beenen, L.F.; Groen, R.J.; Albrecht, K.W.; Vermeulen, M. Complications and outcome in patients with aneurysmal subarachnoid haemorrhage: A prospective hospital based cohort study in the Netherlands. J. Neurol. Neurosurg. Psychiatry 2000, 68, 337–341. [Google Scholar] [CrossRef] [Green Version]
- Bederson, J.B.; Levy, A.L.; Ding, W.H.; Kahn, R.; DiPerna, C.A.; Jenkins, A.L., III; Vallabhajosyula, P. Acute vasoconstriction after subarachnoid hemorrhage. Neurosurgery 1998, 42, 352–360, discussion 360–352. [Google Scholar] [CrossRef] [PubMed]
- Qureshi, A.I.; Sung, G.Y.; Suri, M.A.; Straw, R.N.; Guterman, L.R.; Hopkins, L.N. Prognostic value and determinants of ultraearly angiographic vasospasm after aneurysmal subarachnoid hemorrhage. Neurosurgery 1999, 44, 967–973, discussion 973–964. [Google Scholar] [CrossRef] [PubMed]
- Etminan, N.; Vergouwen, M.D.; Ilodigwe, D.; Macdonald, R.L. Effect of pharmaceutical treatment on vasospasm, delayed cerebral ischemia, and clinical outcome in patients with aneurysmal subarachnoid hemorrhage: A systematic review and meta-analysis. J. Cereb. Blood Flow Metab. 2011, 31, 1443–1451. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Winkler, M.K.; Dengler, N.; Hecht, N.; Hartings, J.A.; Kang, E.J.; Major, S.; Martus, P.; Vajkoczy, P.; Woitzik, J.; Dreier, J.P. Oxygen availability and spreading depolarizations provide complementary prognostic information in neuromonitoring of aneurysmal subarachnoid hemorrhage patients. J. Cereb. Blood Flow Metab. 2017, 37, 1841–1856. [Google Scholar] [CrossRef]
- Molyneux, A.J.; Kerr, R.S.; Birks, J.; Ramzi, N.; Yarnold, J.; Sneade, M.; Rischmiller, J.; Collaborators, I. Risk of recurrent subarachnoid haemorrhage, death, or dependence and standardised mortality ratios after clipping or coiling of an intracranial aneurysm in the International Subarachnoid Aneurysm Trial (ISAT): Long-term follow-up. Lancet Neurol. 2009, 8, 427–433. [Google Scholar] [CrossRef] [Green Version]
- Investigators, C. Rates of delayed rebleeding from intracranial aneurysms are low after surgical and endovascular treatment. Stroke 2006, 37, 1437–1442. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Johnston, S.C.; Dowd, C.F.; Higashida, R.T.; Lawton, M.T.; Duckwiler, G.R.; Gress, D.R.; Investigators, C. Predictors of rehemorrhage after treatment of ruptured intracranial aneurysms: The Cerebral Aneurysm Rerupture After Treatment (CARAT) study. Stroke 2008, 39, 120–125. [Google Scholar] [CrossRef]
- Charpentier, C.; Audibert, G.; Guillemin, F.; Civit, T.; Ducrocq, X.; Bracard, S.; Hepner, H.; Picard, L.; Laxenaire, M.C. Multivariate analysis of predictors of cerebral vasospasm occurrence after aneurysmal subarachnoid hemorrhage. Stroke 1999, 30, 1402–1408. [Google Scholar] [CrossRef] [Green Version]
- Badjatia, N.; Topcuoglu, M.A.; Buonanno, F.S.; Smith, E.E.; Nogueira, R.G.; Rordorf, G.A.; Carter, B.S.; Ogilvy, C.S.; Singhal, A.B. Relationship between hyperglycemia and symptomatic vasospasm after subarachnoid hemorrhage. Crit. Care Med. 2005, 33, 1603–1609, quiz 1623. [Google Scholar] [CrossRef]
- Gross, B.A.; Rosalind Lai, P.M.; Frerichs, K.U.; Du, R. Treatment modality and vasospasm after aneurysmal subarachnoid hemorrhage. World Neurosurg. 2014, 82, e725–e730. [Google Scholar] [CrossRef]
- Dumont, A.S.; Crowley, R.W.; Monteith, S.J.; Ilodigwe, D.; Kassell, N.F.; Mayer, S.; Ruefenacht, D.; Weidauer, S.; Pasqualin, A.; Macdonald, R.L. Endovascular treatment or neurosurgical clipping of ruptured intracranial aneurysms: Effect on angiographic vasospasm, delayed ischemic neurological deficit, cerebral infarction, and clinical outcome. Stroke 2010, 41, 2519–2524. [Google Scholar] [CrossRef] [Green Version]
- Taha, M.M.; Nakahara, I.; Higashi, T.; Iwamuro, Y.; Iwaasa, M.; Watanabe, Y.; Tsunetoshi, K.; Munemitsu, T. Endovascular embolization vs surgical clipping in treatment of cerebral aneurysms: Morbidity and mortality with short-term outcome. Surg. Neurol. 2006, 66, 277–284, discussion 284. [Google Scholar] [CrossRef] [PubMed]
- De Oliveira, J.G.; Beck, J.; Ulrich, C.; Rathert, J.; Raabe, A.; Seifert, V. Comparison between clipping and coiling on the incidence of cerebral vasospasm after aneurysmal subarachnoid hemorrhage: A systematic review and meta-analysis. Neurosurg. Rev. 2007, 30, 22–30, discussion 30–21. [Google Scholar] [CrossRef] [PubMed]
- Xia, Z.W.; Liu, X.M.; Wang, J.Y.; Cao, H.; Chen, F.H.; Huang, J.; Li, Q.Z.; Fan, S.S.; Jiang, B.; Chen, Z.G.; et al. Coiling Is Not Superior to Clipping in Patients with High-Grade Aneurysmal Subarachnoid Hemorrhage: Systematic Review and Meta-Analysis. World Neurosurg. 2017, 98, 411–420. [Google Scholar] [CrossRef]
- Jones, J.; Sayre, J.; Chang, R.; Tian, J.; Szeder, V.; Gonzalez, N.; Jahan, R.; Vinuela, F.; Duckwiler, G.; Tateshima, S. Cerebral vasospasm patterns following aneurysmal subarachnoid hemorrhage: An angiographic study comparing coils with clips. J. Neurointerv. Surg. 2015, 7, 803–807. [Google Scholar] [CrossRef] [PubMed]
- Vergouwen, M.D.; Vermeulen, M.; van Gijn, J.; Rinkel, G.J.; Wijdicks, E.F.; Muizelaar, J.P.; Mendelow, A.D.; Juvela, S.; Yonas, H.; Terbrugge, K.G.; et al. Definition of delayed cerebral ischemia after aneurysmal subarachnoid hemorrhage as an outcome event in clinical trials and observational studies: Proposal of a multidisciplinary research group. Stroke 2010, 41, 2391–2395. [Google Scholar] [CrossRef] [Green Version]

{kind=link}
{kind=link}
{kind=link}
| Univariate | Multivariate | |||||
|---|---|---|---|---|---|---|
| HR | (95% CI) | p Value | AHR * | (95% CI) | p Value | |
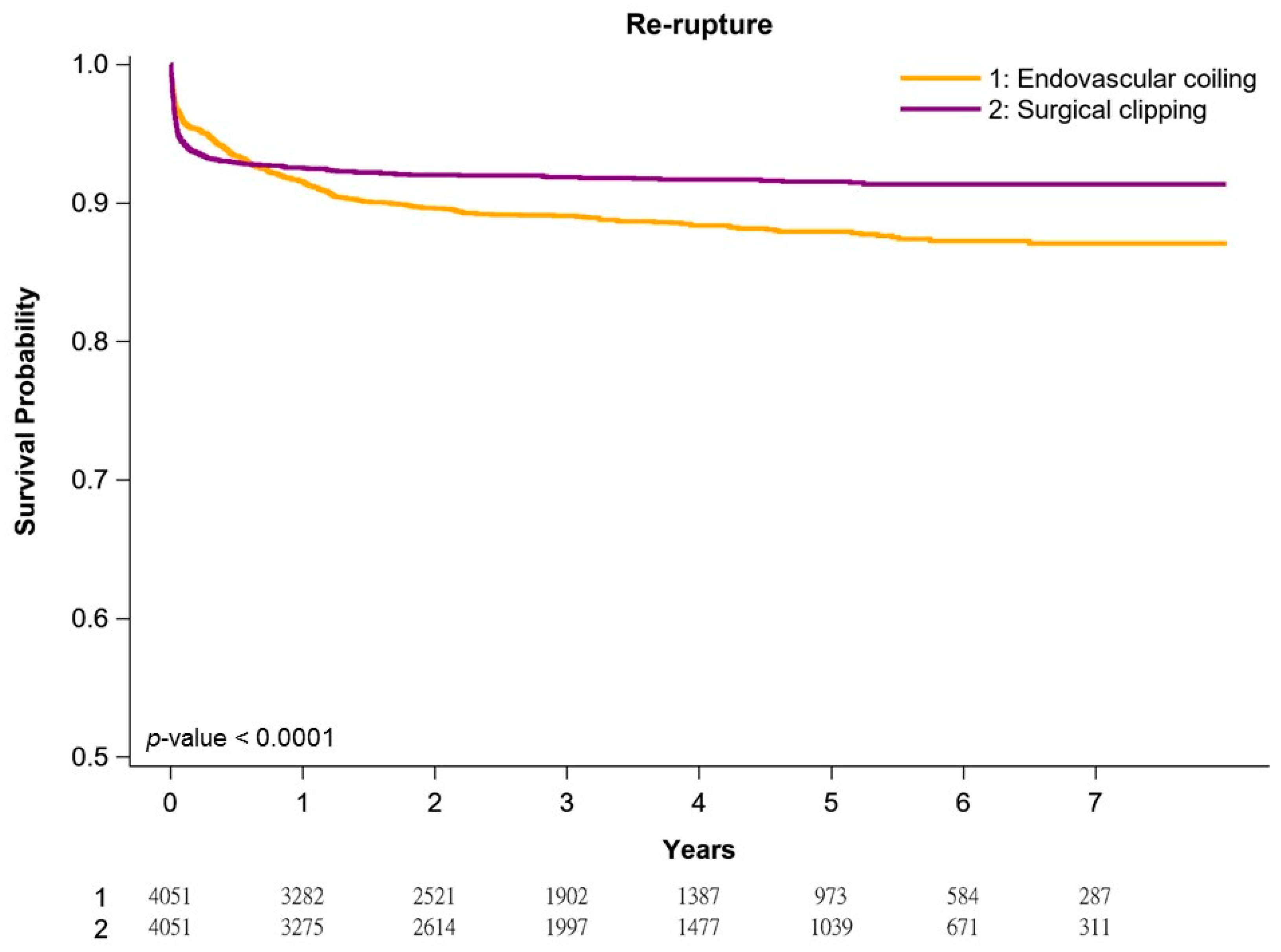
| Aneurysm repair modalities | ||||||
| Surgical clipping | 1 | <0.0001 | 1 | <0.0001 | ||
| Endovascular coil embolization | 1.34 | (1.16–1.55) | 1.36 | (1.17–1.57) | ||
| Age | ||||||
| 20–64 | 1 | 0.2320 | 1 | 0.5407 | ||
| 65–74 | 0.86 | (0.71–1.04) | 0.86 | (0.71–1.05) | ||
| 75–84 | 1.07 | (0.43–1.77) | 1.04 | (0.40–1.17) | ||
| 85+ | 1.03 | (0.55–1.93) | 1.02 | (0.44–1.58) | ||
| Sex | ||||||
| Female | 1 | 0.5664 | 1 | 0.9608 | ||
| Male | 1.04 | (0.90–1.21) | 1.00 | (0.86–1.17) | ||
| Treatment year | ||||||
| 2011–2013 | 1 | 0.0913 | 1 | 0.1560 | ||
| 2014–2015 | 1.05 | (0.88–1.25) | 1.07 | (0.90–1.27) | ||
| 2016–2017 | 0.86 | (0.72–1.03) | 0.89 | (0.74–1.07) | ||
| Diabetes | 0.79 | (0.63–0.99) | 0.0451 | 0.85 | (0.67–1.07) | 0.1679 |
| Congestive heart failure | 0.79 | (0.46–1.37) | 0.3994 | 0.86 | (0.49–1.51) | 0.5984 |
| Hypertension | 0.91 | (0.79–1.06) | 0.2222 | 1.08 | (0.93–1.26) | 0.3318 |
| Renal diseases | ||||||
| No renal diseases | 1 | 0.2274 | 1 | 0.5193 | ||
| Chronic kidney disease | 0.90 | (0.58–1.41) | 1.01 | (0.65–1.59) | ||
| End-stage renal disease | 1.74 | (0.90–3.36) | 1.49 | (0.75–2.97) | ||
| Stroke or TIA | 0.83 | (0.71–0.97) | 0.0175 | 0.91 | (0.77–1.07) | 0.2479 |
| CCI Scores | ||||||
| 0 | 1 | <0.4801 | 1 | 0.8913 | ||
| 1 | 1.04 | (0.54–1.27) | 1.01 | (0.58–1.16) | ||
| 2+ | 1.13 | (0.51–1.28) | 1.01 | (0.56–1.19) | ||
| Hospital level | ||||||
| Academic centers | 1 | 0.1815 | 1 | 0.1847 | ||
| Nonacademic centers | 0.88 | (0.73–1.06) | 0.88 | (0.73–1.06) | ||
| Hospital area | ||||||
| North | 1 | <0.5562 | 1 | 0.6544 | ||
| Central | 1.08 | (0.56–1.54) | 1.07 | (0.56–1.44) | ||
| South/East | 1.05 | (0.54–1.58) | 1.04 | (0.55–1.41) | ||
| Income | ||||||
| <NTD 18,000 | 1 | 0.4338 | 1 | 0.5663 | ||
| NTD 18,000–22,500 | 1.09 | (0.88–1.35) | 1.12 | (0.90–1.40) | ||
| NTD 22,500–30,000 | 0.93 | (0.74–1.16) | 0.96 | (0.77–1.20) | ||
| NTD 30,000+ | 1.08 | (0.89–1.31) | 1.02 | (0.84–1.25) | ||
| Univariate | Multivariate | |||||
|---|---|---|---|---|---|---|
| HR | (95% CI) | p Value | AHR * | (95% CI) | p Value | |
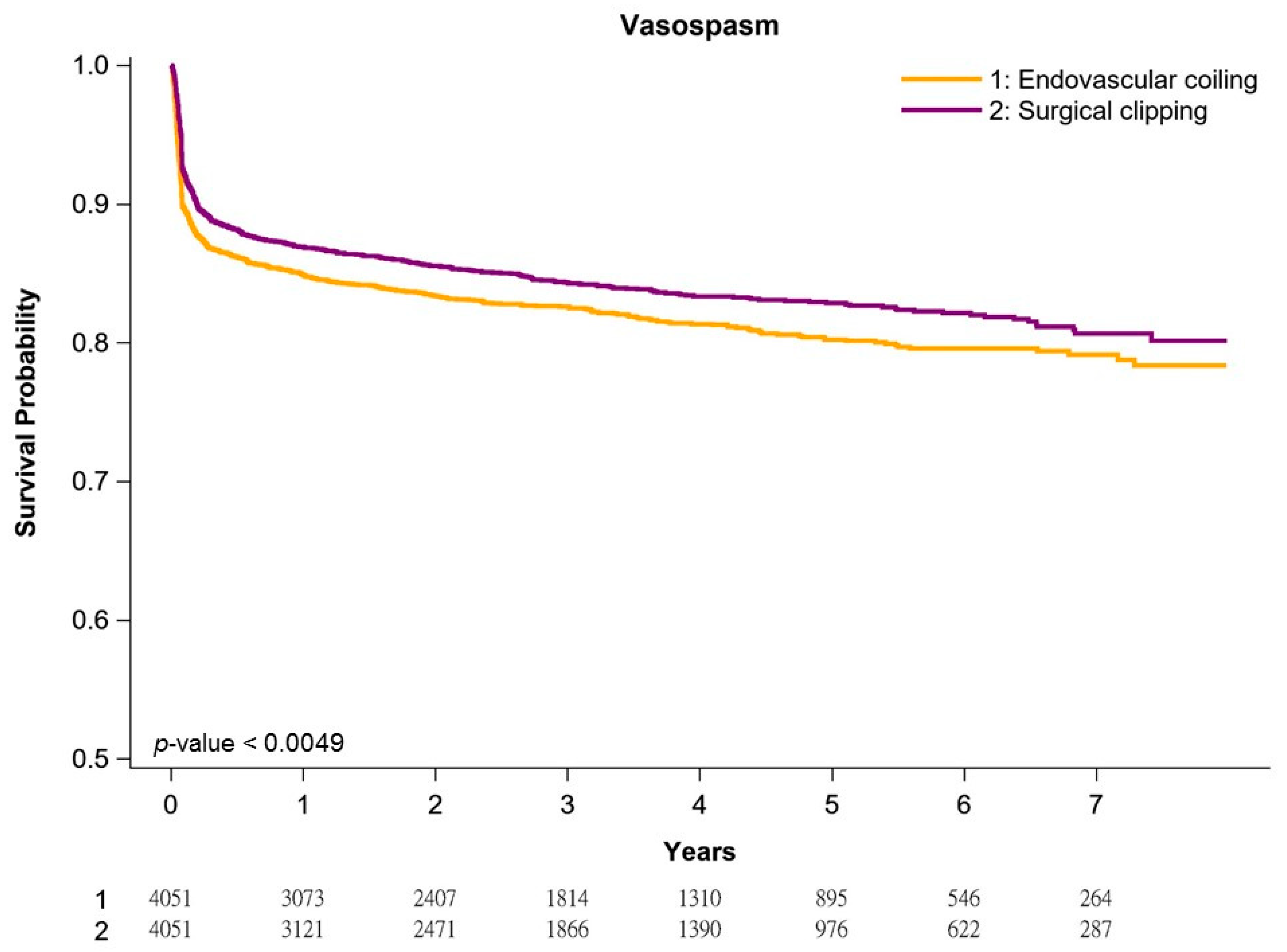
| Aneurysm repair modalities | ||||||
| Surgical clipping | 1 | 0.0050 | 1 | 0.0214 | ||
| Endovascular coil embolization | 1.17 | (1.05–1.30) | 1.14 | (1.02–1.27) | ||
| Age | ||||||
| 20–64 | 1 | <0.0001 | 1 | <0.0001 | ||
| 65–74 | 1.45 | (1.27–1.66) | 1.27 | (1.11–1.46) | ||
| 75–84 | 1.78 | (1.52–2.08) | 1.40 | (1.19–1.66) | ||
| 85+ | 1.38 | (1.08–2.18) | 1.07 | (1.01–1.53) | ||
| Sex | ||||||
| Female | 1 | 0.0020 | 1 | 0.0004 | ||
| Male | 1.19 | (1.07–1.33) | 1.22 | (1.10–1.37) | ||
| Treatment year | ||||||
| 2011–2013 | 1 | 0.3838 | 1 | 0.1567 | ||
| 2014–2015 | 0.96 | (0.84–1.10) | 0.94 | (0.82–1.07) | ||
| 2016–2017 | 0.91 | (0.80–1.04) | 0.87 | (0.75–1.00) | ||
| Diabetes | 1.47 | (1.28–1.68) | <0.0001 | 1.20 | (1.04–1.39) | 0.0141 |
| Congestive heart failure | 1.69 | (1.16–2.27) | 0.0005 | 1.30 | (1.06–1.76) | 0.0297 |
| Hypertension | 1.35 | (1.21–1.51) | <0.0001 | 1.17 | (1.04–1.32) | 0.0089 |
| Renal diseases | ||||||
| No renal diseases | 1 | 0.0364 | 1 | 0.2182 | ||
| Chronic kidney disease | 1.43 | (1.09–1.89) | 1.09 | (0.82–1.44) | ||
| End-stage renal disease | 1.09 | (0.58–2.02) | 0.60 | (0.32–1.11) | ||
| Stroke or TIA | 1.31 | (1.18–1.46) | <0.0001 | 1.27 | (1.14–1.43) | <0.0001 |
| CCI Scores | ||||||
| 0 | 1 | 0.3241 | 1 | 0.6873 | ||
| 1 | 0.91 | (0.78–1.07) | 1.01 | (0.68–1.05) | ||
| 2+ | 1.30 | (0.90–1.54) | 1.02 | (0.85–1.22) | ||
| Hospital level | ||||||
| Academic centers | 1 | 0.7209 | 1 | 0.1738 | ||
| Nonacademic centers | 0.98 | (0.85–1.12) | 0.91 | (0.79–1.04) | ||
| Hospital area | ||||||
| North | 1 | 0.4004 | 1 | 0.0570 | ||
| Central | 0.90 | (0.78–1.05) | 0.84 | (0.72–1.07) | ||
| South/East | 0.96 | (0.85–1.10) | 0.96 | (0.84–1.10) | ||
| Income | ||||||
| <NTD 18,000 | 1 | 0.0006 | 1 | 0.1133 | ||
| NTD 18,000–22,500 | 1.00 | (0.86–1.17) | 1.05 | (0.90–1.23) | ||
| NTD 22,500–30,000 | 0.97 | (0.82–1.13) | 1.04 | (0.88–1.22) | ||
| NTD 30,000+ | 0.77 | (0.66–0.89) | 1.04 | (0.73–1.08) | ||
| Univariate | Multivariate | |||||
|---|---|---|---|---|---|---|
| HR | (95% CI) | p Value | AHR * | (95% CI) | p Value | |
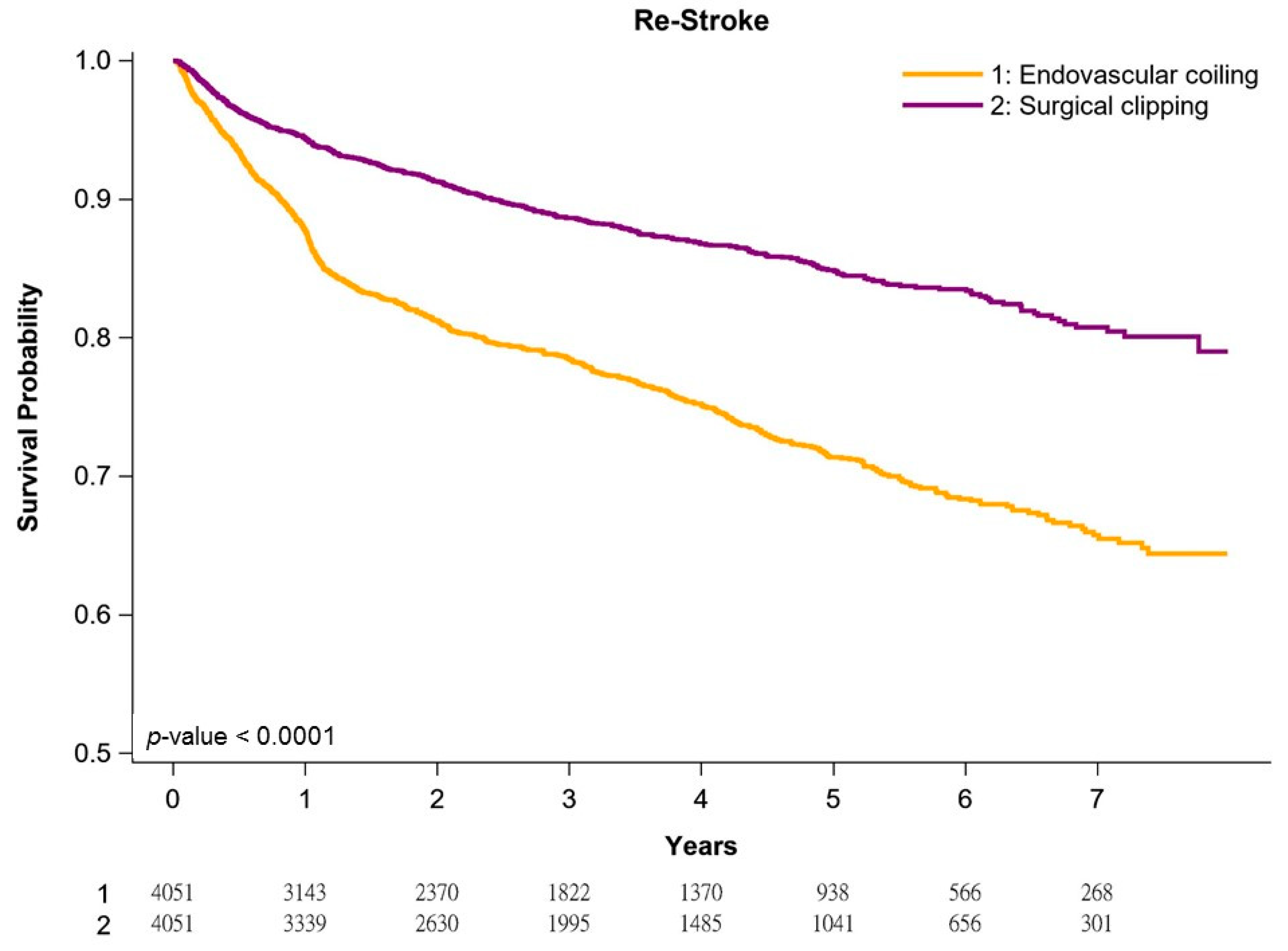
| Aneurysm repair modalities | ||||||
| Surgical clipping | 1 | <0.0001 | 1 | <0.0001 | ||
| Endovascular coil embolization | 2.08 | (1.86–2.32) | 2.04 | (1.83–2.29) | ||
| Age | ||||||
| 20–64 | 1 | <0.0001 | 1 | 0.0135 | ||
| 65–74 | 1.30 | (1.14–1.48) | 1.10 | (1.06–1.26) | ||
| 75–84 | 1.50 | (1.27–1.77) | 1.21 | (1.04–1.20) | ||
| 85+ | 1.22 | (1.12–2.06) | 1.22 | (1.15–1.52) | ||
| Sex | ||||||
| Female | 1 | 0.1537 | 1 | 0.0416 | ||
| Male | 1.08 | (0.97–1.21) | 1.06 | (1.01–1.19) | ||
| Treatment year | ||||||
| 2011–2013 | 1 | <0.7911 | 1 | <0.8801 | ||
| 2014–2015 | 0.91 | (0.97–2.66) | 0.95 | (0.70–2.23) | ||
| 2016–2017 | 0.78 | (0.84–4.41) | 0.91 | (0.84–3.34) | ||
| Diabetes | 1.45 | (1.26–1.66) | <0.0001 | 1.21 | (1.05–1.40) | 0.0099 |
| Congestive heart failure | 1.75 | (1.29–2.36) | 0.0003 | 1.26 | (1.11–1.73) | 0.0151 |
| Hypertension | 1.23 | (1.11–1.37) | <0.0001 | 1.14 | (1.02–1.28) | 0.0239 |
| Renal diseases | ||||||
| No renal diseases | 1 | 0.0053 | 1 | 0.7824 | ||
| Chronic kidney disease | 1.35 | (1.01–1.80) | 0.94 | (0.70–1.28) | ||
| End-stage renal disease | 2.00 | (1.18–3.38) | 0.84 | (0.49–1.46) | ||
| Stroke or TIA | 1.26 | (1.13–1.40) | <0.0001 | 1.27 | (1.13–1.42) | <0.0001 |
| CCI Scores | ||||||
| 0 | 1 | 0.5607 | 1 | 0.3244 | ||
| 1 | 0.78 | (0.67–1.90) | 0.84 | (0.72–1.48) | ||
| 2+ | 0.91 | (0.78–1.07) | 0.79 | (0.67–1.44) | ||
| Hospital level | ||||||
| Medical center | 1 | 0.2219 | 1 | 0.6973 | ||
| others | 1.08 | (0.95–1.23) | 0.97 | (0.85–1.11) | ||
| Hospital area | ||||||
| North | 1 | 0.5405 | 1 | <0.6611 | ||
| Central | 1.06 | (0.66–1.88) | 1.03 | (0.58–1.78) | ||
| South/East | 1.08 | (0.60–1.78) | 1.04 | (0.56–1.73) | ||
| Income | ||||||
| <NTD 18,000 | 1 | <0.0001 | 1 | 0.2340 | ||
| NTD 18,000–22,500 | 0.80 | (0.68–0.94) | 1.05 | (0.89–1.25) | ||
| NTD 22,500–30,000 | 1.35 | (1.16–1.57) | 1.17 | (1.00–1.37) | ||
| NTD 30,000+ | 0.97 | (0.84–1.13) | 1.04 | (0.89–1.20) | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhang, J.; Lo, Y.-L.; Li, M.-C.; Yu, Y.-H.; Wu, S.-Y. Risk of Re-Rupture, Vasospasm, or Re-Stroke after Clipping or Coiling of Ruptured Intracranial Aneurysms: Long-Term Follow-Up with a Propensity Score-Matched, Population-Based Cohort Study. J. Pers. Med. 2021, 11, 1209. https://doi.org/10.3390/jpm11111209
Zhang J, Lo Y-L, Li M-C, Yu Y-H, Wu S-Y. Risk of Re-Rupture, Vasospasm, or Re-Stroke after Clipping or Coiling of Ruptured Intracranial Aneurysms: Long-Term Follow-Up with a Propensity Score-Matched, Population-Based Cohort Study. Journal of Personalized Medicine. 2021; 11(11):1209. https://doi.org/10.3390/jpm11111209
Chicago/Turabian StyleZhang, Jiaqiang, Yang-Lan Lo, Ming-Chang Li, Ying-Hui Yu, and Szu-Yuan Wu. 2021. "Risk of Re-Rupture, Vasospasm, or Re-Stroke after Clipping or Coiling of Ruptured Intracranial Aneurysms: Long-Term Follow-Up with a Propensity Score-Matched, Population-Based Cohort Study" Journal of Personalized Medicine 11, no. 11: 1209. https://doi.org/10.3390/jpm11111209
APA StyleZhang, J., Lo, Y.-L., Li, M.-C., Yu, Y.-H., & Wu, S.-Y. (2021). Risk of Re-Rupture, Vasospasm, or Re-Stroke after Clipping or Coiling of Ruptured Intracranial Aneurysms: Long-Term Follow-Up with a Propensity Score-Matched, Population-Based Cohort Study. Journal of Personalized Medicine, 11(11), 1209. https://doi.org/10.3390/jpm11111209