
Dynamic Hip Screw versus Cannulated Cancellous Screw in Pauwels Type II or Type III Femoral Neck Fracture: A Systematic Review and Meta-Analysis


Abstract
1. Introduction
2. Materials and Methods
2.1. Literature Search
2.2. Study Selection
2.3. Data Extraction
2.4. Quality Assessment
2.5. Risk of Bias Assessment
2.6. Data Synthesis and Statistical Analysis
3. Results
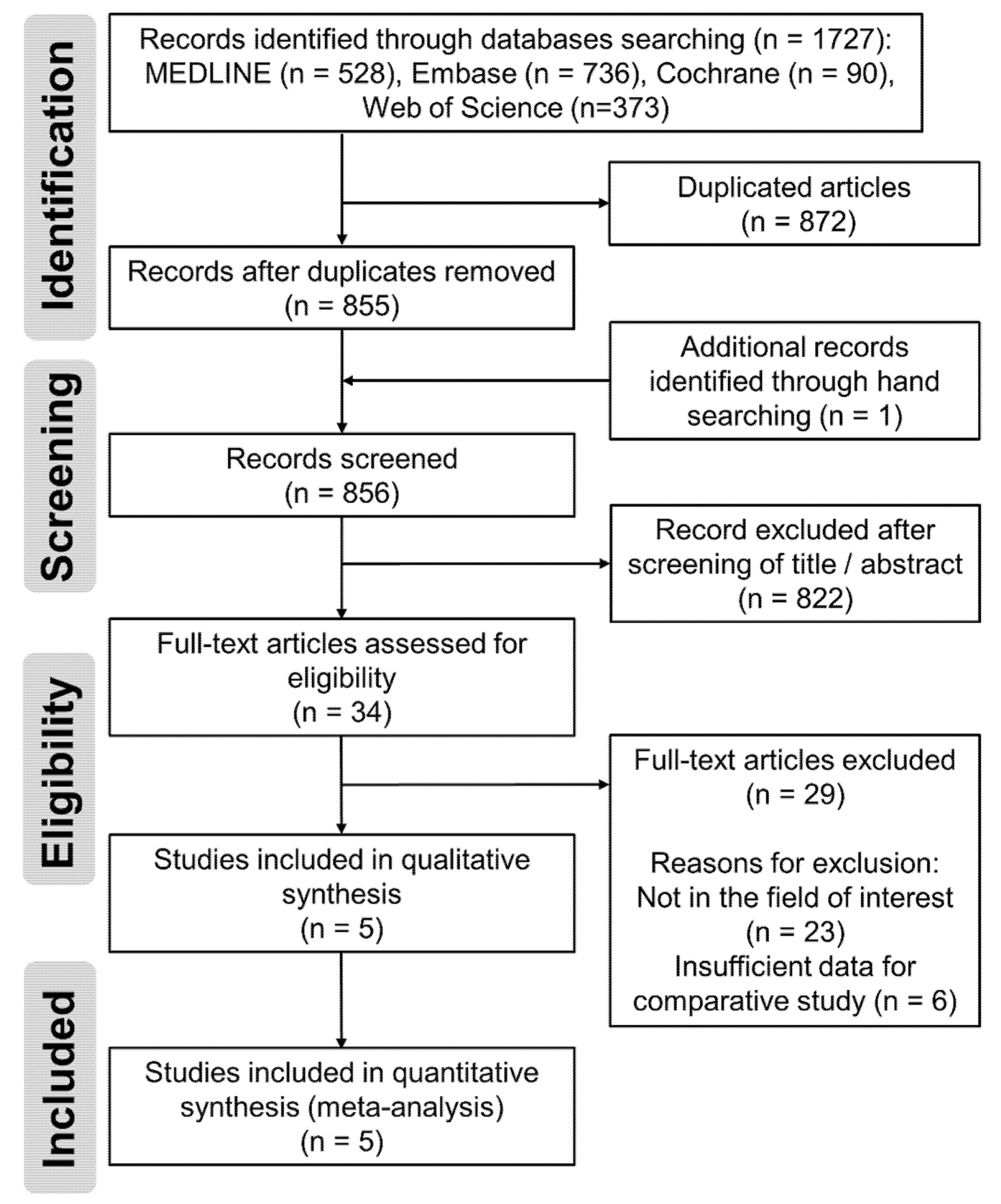
3.1. Study Identification
3.2. Study Characteristics and Qualitative Synthesis
3.3. Quality Assessment
3.4. Risk of Bias Assessment
3.5. Meta-Analysis Results
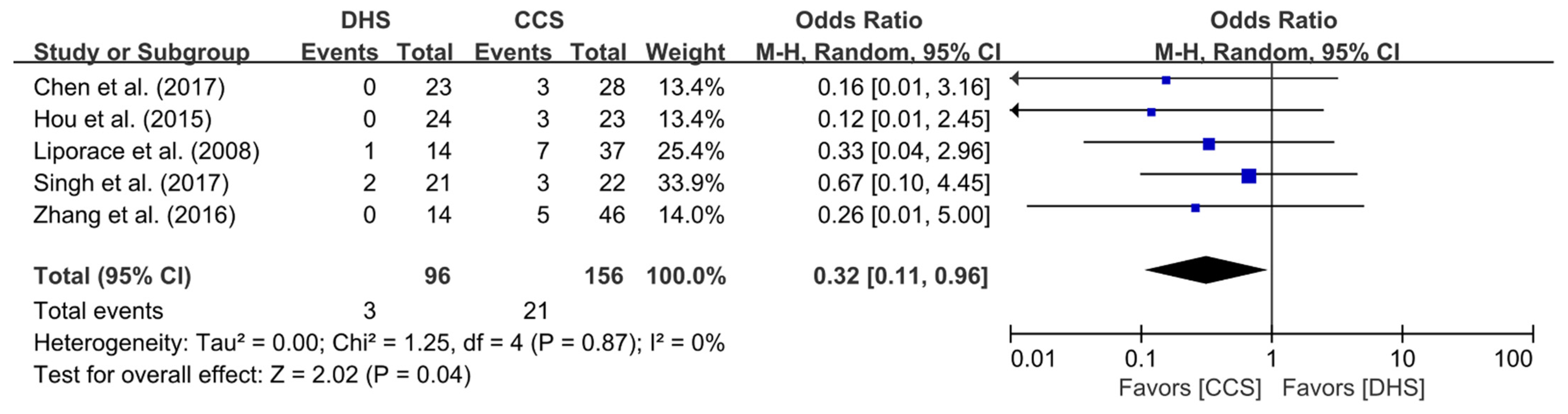
3.5.1. Nonunion Rate
3.5.2. Incidence of ONFH
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kazley, J.; Bagchi, K. Femoral Neck Fractures. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2020. [Google Scholar]
- Bartonicek, J. Pauwels’ classification of femoral neck fractures: Correct interpretation of the original. J. Orthop. Trauma 2001, 15, 358–360. [Google Scholar] [CrossRef] [PubMed]
- Meinberg, E.G.; Agel, J.; Roberts, C.S.; Karam, M.D.; Kellam, J.F. Fracture and Dislocation Classification Compendium-2018. J. Orthop. Trauma 2018, 32 (Suppl. 1), S1–S170. [Google Scholar] [CrossRef]
- Pauwels, F. Der Schenkelhalsbruch. In Gesammelte Abhandlungen zur Funktionellen Anatomie des Bewegungsapparates; Springer: Berlin/Heidelberg, Germany, 1965; pp. 1–138. [Google Scholar]
- Singh, D.M.; Sonkar, D.D.; Verma, D.R.; Shukla, D.J.; Gaur, D.S. Comparison of the functional outcome of DHS versus cannulated cancellous screws in pauwels type II and III fracture neck femur in young adults. Int. J. Orthop. Sci. 2017, 3, 745–749. [Google Scholar] [CrossRef][Green Version]
- Aminian, A.; Gao, F.; Fedoriw, W.W.; Zhang, L.Q.; Kalainov, D.M.; Merk, B.R. Vertically oriented femoral neck fractures: Mechanical analysis of four fixation techniques. J. Orthop. Trauma 2007, 21, 544–548. [Google Scholar] [CrossRef]
- Baitner, A.C.; Maurer, S.G.; Hickey, D.G.; Jazrawi, L.M.; Kummer, F.J.; Jamal, J.; Goldman, S.; Koval, K.J. Vertical shear fractures of the femoral neck. A biomechanical study. Clin. Orthop. Relat. Res. 1999, 367, 300–305. [Google Scholar] [CrossRef]
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A.; Group, P.-P. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst. Rev. 2015, 4, 1. [Google Scholar] [CrossRef] [PubMed]
- Shea, B.J.; Grimshaw, J.M.; Wells, G.A.; Boers, M.; Andersson, N.; Hamel, C.; Porter, A.C.; Tugwell, P.; Moher, D.; Bouter, L.M. Development of AMSTAR: A measurement tool to assess the methodological quality of systematic reviews. BMC Med. Res. Methodol. 2007, 7, 10. [Google Scholar] [CrossRef]
- Downs, S.H.; Black, N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J. Epidemiol. Community Health 1998, 52, 377–384. [Google Scholar] [CrossRef] [PubMed]
- Sterne, J.A.; Hernán, M.A.; Reeves, B.C.; Savović, J.; Berkman, N.D.; Viswanathan, M.; Henry, D.; Altman, D.G.; Ansari, M.T.; Boutron, I.; et al. ROBINS-I: A tool for assessing risk of bias in non-randomised studies of interventions. BMJ Clin. Res. Ed. 2016, 355, i4919. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, F.L.; Oh, I.S.; Hayes, T.L. Fixed- versus random-effects models in meta-analysis: Model properties and an empirical comparison of differences in results. Br. J. Math. Stat. Psychol. 2009, 62, 97–128. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. Cochrane Handbook for Systematic Reviews of Interventions, 2nd ed.; John Wiley & Sons: Chichester, UK, 2019. [Google Scholar]
- Chen, Z.; Wang, G.; Lin, J.; Yang, T.; Fang, Y.; Liu, L.; Zhang, H. Efficacy comparison between dynamic hip screw combined with anti-rotation screw and cannulated screw in treating femoral neck fractures. Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi Zhongguo Xiufu Chongjian Waike Zazhi Chin. J. Reparative Reconstr. Surg. 2011, 25, 26–29. [Google Scholar]
- Hou, W.; Xu, M. Comparison among three cannulated screws and dynamic hip screw combined with antirotation screw for comminuted fractures of femoral neck. Zhongguo Gu Shang China J. Orthop. Traumatol. 2015, 28, 796–801. [Google Scholar]
- Liporace, F.; Gaines, R.; Collinge, C.; Haidukewych, G.J. Results of internal fixation of Pauwels type-3 vertical femoral neck fractures. J. Bone Jt. Surg. Ser. A 2008, 90, 1654–1659. [Google Scholar] [CrossRef]
- Zhang, Y.L.; Chen, S.; Ai, Z.S.; Gao, Y.S.; Mei, J.; Zhang, C.Q. Osteonecrosis of the femoral head, nonunion and potential risk factors in Pauwels grade-3 femoral neck fractures A retrospective cohort study. Medcine 2016, 95. [Google Scholar] [CrossRef]
- Lee, Y.S.; Chen, S.H.; Tsuang, Y.H.; Huang, H.L.; Lo, T.Y.; Huang, C.R. Internal fixation of undisplaced femoral neck fractures in the elderly: A retrospective comparison of fixation methods. J. Trauma 2008, 64, 155–162. [Google Scholar] [CrossRef]
- Chen, C.; Yu, L.; Tang, X.; Liu, M.Z.; Sun, L.Z.; Liu, C.; Zhang, Z.; Li, C.Z. Dynamic hip system blade versus cannulated compression screw for the treatment of femoral neck fractures: A retrospective study. Acta Orthop. Traumatol. Turc. 2017, 51, 381–387. [Google Scholar] [CrossRef] [PubMed]
- Shu, D.P.; Xiao, Y.P.; Bei, M.J.; Ji, T.; Peng, Y.J.; Ma, B.; Li, S.G. Dynamic compression locking system versus multiple cannulated compression screw for the treatment of femoral neck fractures: A comparative study. BMC Musculoskelet. Disord. 2020, 21, 230. [Google Scholar] [CrossRef] [PubMed]
- Li, L.; Zhao, X.; Yang, X.; Tang, X.; Liu, M. Dynamic hip screws versus cannulated screws for femoral neck fractures: A systematic review and meta-analysis. J. Orthop. Surg. Res. 2020, 15, 352. [Google Scholar] [CrossRef]
- Xia, Y.; Zhang, W.; Zhang, Z.; Wang, J.; Yan, L. Treatment of femoral neck fractures: Sliding hip screw or cannulated screws? A meta-analysis. J. Orthop. Surg. Res. 2021, 16, 54. [Google Scholar] [CrossRef] [PubMed]
- Deneka, D.A.; Simonian, P.T.; Stankewich, C.J.; Eckert, D.; Chapman, J.R.; Tencer, A.F. Biomechanical comparison of internal fixation techniques for the treatment of unstable basicervical femoral neck fractures. J. Orthop. Trauma 1997, 11, 337–343. [Google Scholar] [CrossRef] [PubMed]
- Sahin, A.; Agar, A.; Gulabi, D.; Erturk, C. Comparison of dynamic hip screw and antirotation screw with cannulated screw in the treatment of transcervical collum femoris fractures. Jt. Dis. Relat. Surg. 2020, 31, 320–327. [Google Scholar] [CrossRef]
- Haidukewych, G.J.; Rothwell, W.S.; Jacofsky, D.J.; Torchia, M.E.; Berry, D.J. Operative treatment of femoral neck fractures in patients between the ages of fifteen and fifty years. J. Bone Jt. Surg. Am. 2004, 86, 1711–1716. [Google Scholar] [CrossRef]
- Papakostidis, C.; Panagiotopoulos, A.; Piccioli, A.; Giannoudis, P.V. Timing of internal fixation of femoral neck fractures. A systematic review and meta-analysis of the final outcome. Injury 2015, 46, 459–466. [Google Scholar] [CrossRef]
- Xu, J.-L.; Liang, Z.-R.; Xiong, B.-L.; Zou, Q.-Z.; Lin, T.-Y.; Yang, P.; Chen, D.; Zhang, Q.-W. Risk factors associated with osteonecrosis of femoral head after internal fixation of femoral neck fracture:a systematic review and meta-analysis. BMC Musculoskelet. Disord. 2019, 20, 632. [Google Scholar] [CrossRef] [PubMed]
- Makki, D.; Mohamed, A.M.; Gadiyar, R.; Patterson, M. Addition of an anti-rotation screw to the dynamic hip screw for femoral neck fractures. Orthopedics 2013, 36, e865–e868. [Google Scholar] [CrossRef] [PubMed]
- Stoffel, K.; Zderic, I.; Gras, F.; Sommer, C.; Eberli, U.; Mueller, D.; Oswald, M.; Gueorguiev, B. Biomechanical Evaluation of the Femoral Neck System in Unstable Pauwels III Femoral Neck Fractures: A Comparison with the Dynamic Hip Screw and Cannulated Screws. J. Orthop. Trauma 2017, 31, 131–137. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Author (Year) | Study Design | Number of Patients | Mean Age, Years | Male Sex, % | Pauwels Type | Mean Follow-Up Period, Months | NU | ONFH | |||
|---|---|---|---|---|---|---|---|---|---|---|---|
| DHS | CCS | DHS | CCS | DHS | CCS | ||||||
| Chen et al. (2011) [14] | RCS | 23 | 28 | 41.8 | 49.0 | II, III (41.2%:58.8%) | ≥12 | 0 (0%) | 3 (11%) | 0 (0%) | 1 (4%) |
| Hou et al. (2015) [15] | RCS | 24 | 23 | 43.4 | 55.3 | III | 30.0 | 0 (0%) | 3 (13%) | NA | NA |
| Liporace et al. (2008) [16] | RCS | 14 | 37 | 42 | NA | III | 24 | 1 (7%) | 7 (19%) | 1 (7%) | 5 (14%) |
| Singh et al. (2017) [5] | RCT | 21 | 22 | 28.8 | 79.1 | II, III (53.5%:46.5%) | 10.5 | 2 (10%) | 3 (14%) | 1 (5%) | 3 (14%) |
| Zhang et al. (2016) [17] | RCS | 14 | 46 | 47.7 | 73.1 | III | 21.6 | 0 (0%) | 5 (11%) | 7 (50%) | 8 (17%) |
| Mode of Injury | Initial Displacement | Timing of Surgery from Injury | Operation Time (min) | Postoperative Infection | |||||
|---|---|---|---|---|---|---|---|---|---|
| DHS | CCS | DHS | CCS | DHS | CCS | DHS | CCS | ||
| Chen et al. (2011) [14] | Low energy 1 (4%) High energy 22 (96%) | Low energy 1 (4%) High energy 27 (96%) | NA | 9.2 (2–18) h | 9.0 (2–16) h | 48.3 ± 5.3 | 44.0 ± 3.6 | NA | NA |
| Hou et al. (2015) [15] | Low energy 2 (7%) High energy 28 (93%) | Low energy 5 (15%) High energy 29 (85%) | Displaced 47 (100%) | 32.0 (2–72) h | 33.0 (3–67) h | 51.0 ± 8.7 | 49.0 ± 8.3 | 0 (0%) | 0 (0%) |
| Liporace et al. (2008) [16] | NA | NA | Displaced 58 (91%) Nondisplaced 4 (9%) | <24 h | NA | NA | 1 (7%) | 0 (0%) | |
| Singh et al. (2017) [5] | NA | NA | NA | 6.2 days | NA | NA | 1 (5%) | 0 (0%) | |
| Zhang et al. (2016) [17] | NA | NA | Displaced 57 (85%) Nondisplaced 10 (15%) | 2.3 ± 0.8 days | NA | NA | NA | NA | |
| Downs and Black Total Score | Crude Agreement | Cohen’s Kappa Coefficient | ||
|---|---|---|---|---|
| Reviewer 1 | Reviewer 2 | |||
| Chen et al. (2011) [14] | 13 | 14 | 95.8% | 0.92 |
| Hou et al. (2015) [15] | 16 | 16 | 91.7% | 0.81 |
| Liporace et al. (2008) [16] | 16 | 15 | 95.8% | 0.91 |
| Singh et al. (2017) [5] | 13 | 16 | 87.5% | 0.74 |
| Zhang et al. (2016) [17] | 12 | 13 | 95.8% | 0.92 |
| Study | Confounding | Selection | Intervention Classification | Deviation from Intervention | Missing Data | Measurement of Outcome | Selection of Reported Result | Overall |
|---|---|---|---|---|---|---|---|---|
| Chen et al. (2011) [14] | Low | Low | Moderate | Low | NI | Low | Low | Moderate |
| Hou et al. (2015) [15] | Low | Moderate | Moderate | Low | NI | Low | Low | Moderate |
| Liporace et al. (2008) [16] | Moderate | Low | Moderate | Low | Low | Low | Low | Moderate |
| Singh et al. (2017) [5] | Moderate | Serious | Low | Moderate | Low | Low | Low | Serious |
| Zhang et al. (2016) [17] | Low | Serious | Moderate | Moderate | Low | Low | Low | Serious |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lim, E.J.; Shon, H.-C.; Cho, J.-W.; Oh, J.-K.; Kim, J.; Kim, C.-H. Dynamic Hip Screw versus Cannulated Cancellous Screw in Pauwels Type II or Type III Femoral Neck Fracture: A Systematic Review and Meta-Analysis. J. Pers. Med. 2021, 11, 1017. https://doi.org/10.3390/jpm11101017
Lim EJ, Shon H-C, Cho J-W, Oh J-K, Kim J, Kim C-H. Dynamic Hip Screw versus Cannulated Cancellous Screw in Pauwels Type II or Type III Femoral Neck Fracture: A Systematic Review and Meta-Analysis. Journal of Personalized Medicine. 2021; 11(10):1017. https://doi.org/10.3390/jpm11101017
Chicago/Turabian StyleLim, Eic Ju, Hyun-Chul Shon, Jae-Woo Cho, Jong-Keon Oh, Junhyun Kim, and Chul-Ho Kim. 2021. "Dynamic Hip Screw versus Cannulated Cancellous Screw in Pauwels Type II or Type III Femoral Neck Fracture: A Systematic Review and Meta-Analysis" Journal of Personalized Medicine 11, no. 10: 1017. https://doi.org/10.3390/jpm11101017
APA StyleLim, E. J., Shon, H.-C., Cho, J.-W., Oh, J.-K., Kim, J., & Kim, C.-H. (2021). Dynamic Hip Screw versus Cannulated Cancellous Screw in Pauwels Type II or Type III Femoral Neck Fracture: A Systematic Review and Meta-Analysis. Journal of Personalized Medicine, 11(10), 1017. https://doi.org/10.3390/jpm11101017