Behavioral and Psychological Symptoms of Dementia (BPSD): Clinical Characterization and Genetic Correlates in an Italian Alzheimer’s Disease Cohort

 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Sample and Clinical Evaluation
2.2. Genetic Analysis
2.3. Statistical Analyses
2.3.1. Principal Component Analysis (PCA)
2.3.2. Classification and Regression Tree (CART) Analysis for Single BPSD Symptoms and Endophenotypes
3. Results
3.1. Clinical Characterization according to Single NPI Scores
3.2. Clinical Characterization according to Behavioral Endophenotypes
3.3. APOE, MTHFR, and COMT Genetic Correlates in Endophenotype Clusterization and in Single BPSD Symptoms
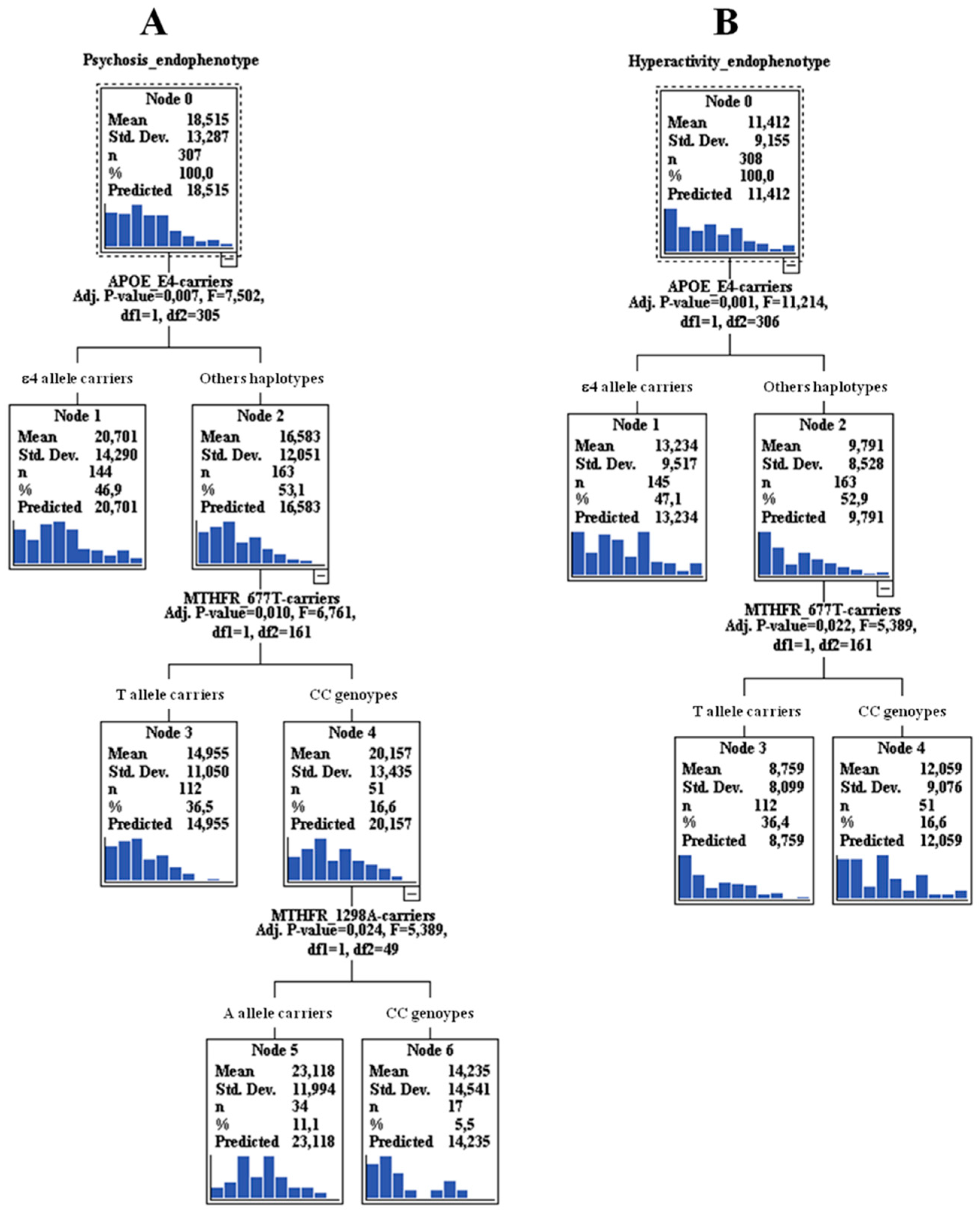
3.3.1. “Genexgene” Interactions in “Psychosis” Endophenotype and the Relative Single BPSD Symptoms
3.3.2. “Genexgene” Interactions in “Hyperactivity” Endophenotype and the Relative Single BPSD Symptoms
3.3.3. “Genexgene” Interactions in “Mood”/”Frontal” Endophenotypes and the Relative Single BPSD Symptoms
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- McKhann, G.M.; Knopman, D.S.; Chertkow, H.; Hyman, B.T.; Jack, C.R., Jr.; Kawas, C.H.; Klunk, W.E.; Koroshetz, W.J.; Manly, J.J.; Mayeux, R.; et al. The diagnosis of dementia due to Alzheimer’s disease: Recommendations from the National Institute on Aging-Alzheimer’s Association workgroups on diagnostic guidelines for Alzheimer’s disease. Alzheimers Dement. 2011, 7, 263–269. [Google Scholar] [CrossRef]
- Haupt, M.; Kurz, A.; Janner, M. A 2-year follow-up of behavioural and psychological symptoms in Alzheimer’s disease. Dement. Geriatr. Cogn. Disord. 2000, 11, 147–152. [Google Scholar] [CrossRef] [PubMed]
- Cerejeira, J.; Lagarto, L.; Mukaetova-Ladinska, E.B. Behavioral and psychological symptoms of dementia. Front. Neurol. 2012, 3, 73. [Google Scholar] [CrossRef] [PubMed]
- Cloak, N.; Al Khalili, Y. Behavioral and Psychological Symptoms in Dementia (BPSD); StatPearls Publishing LLC: Treasure Island, FL, USA, 2020. [Google Scholar]
- Angelucci, F.; Spalletta, G.; di Iulio, F.; Ciaramella, A.; Salani, F.; Colantoni, L.; Varsi, A.E.; Gianni, W.; Sancesario, G.; Caltagirone, C.; et al. Alzheimer’s disease (AD) and Mild Cognitive Impairment (MCI) patients are characterized by increased BDNF serum levels. Curr. Alzheimer Res. 2010, 7, 15–20. [Google Scholar] [CrossRef] [PubMed]
- Finkel, S.I.; Costa e Silva, J.; Cohen, G.; Miller, S.; Sartorius, N. Behavioral and psychological signs and symptoms of dementia: A consensus statement on current knowledge and implications for research and treatment. Int. Psychogeriatr. 1996, 8, 497–500. [Google Scholar] [CrossRef] [PubMed]
- Frisoni, G.B.; Rozzini, L.; Gozzetti, A.; Binetti, G.; Zanetti, O.; Bianchetti, A.; Trabucchi, M.; Cummings, J.L. Behavioral syndromes in Alzheimer’s disease: Description and correlates. Dement. Geriatr. Cogn. Disord. 1999, 10, 130–138. [Google Scholar] [CrossRef]
- van der Linde, R.M.; Dening, T.; Matthews, F.E.; Brayne, C. Grouping of behavioural and psychological symptoms of dementia. Int. J. Geriatr. Psychiatry 2014, 29, 562–568. [Google Scholar] [CrossRef]
- Mushtaq, R.; Pinto, C.; Tarfarosh, S.F.; Hussain, A.; Shoib, S.; Shah, T.; Shah, S.; Manzoor, M.; Bhat, M.; Arif, T. A Comparison of the Behavioral and Psychological Symptoms of Dementia (BPSD) in Early-Onset and Late-Onset Alzheimer’s Disease-A Study from South East Asia (Kashmir, India). Cureus 2016, 8, e625. [Google Scholar] [CrossRef]
- Flirski, M.; Sobow, T.; Kloszewska, I. Behavioural genetics of Alzheimer’s disease: A comprehensive review. Arch. Med. Sci. 2011, 7, 195–210. [Google Scholar] [CrossRef]
- Borroni, B.; Agosti, C.; Archetti, S.; Costanzi, C.; Bonomi, S.; Ghianda, D.; Lenzi, G.L.; Caimi, L.; Di Luca, M.; Padovani, A. Catechol-O-methyltransferase gene polymorphism is associated with risk of psychosis in Alzheimer Disease. Neurosci. Lett. 2004, 370, 127–129. [Google Scholar] [CrossRef]
- Borroni, B.; Grassi, M.; Agosti, C.; Archetti, S.; Costanzi, C.; Cornali, C.; Caltagirone, C.; Caimi, L.; Di Luca, M.; Padovani, A. Cumulative effect of COMT and 5-HTTLPR polymorphisms and their interaction with disease severity and comorbidities on the risk of psychosis in Alzheimer disease. Am. J. Geriatr. Psychiatry 2006, 14, 343–351. [Google Scholar] [CrossRef] [PubMed]
- Borroni, B.; Grassi, M.; Agosti, C.; Costanzi, C.; Archetti, S.; Franzoni, S.; Caltagirone, C.; Di Luca, M.; Caimi, L.; Padovani, A. Genetic correlates of behavioral endophenotypes in Alzheimer disease: Role of COMT, 5-HTTLPR and APOE polymorphisms. Neurobiol. Aging 2006, 27, 1595–1603. [Google Scholar] [CrossRef] [PubMed]
- Borroni, B.; Grassi, M.; Costanzi, C.; Zanetti, M.; Archetti, S.; Franzoni, S.; Caimi, L.; Padovani, A. Haplotypes in cathechol-O-methyltransferase gene confer increased risk for psychosis in Alzheimer disease. Neurobiol. Aging 2007, 28, 1231–1238. [Google Scholar] [CrossRef] [PubMed]
- Akil, M.; Kolachana, B.S.; Rothmond, D.A.; Hyde, T.M.; Weinberger, D.R.; Kleinman, J.E. Catechol-O-methyltransferase genotype and dopamine regulation in the human brain. J. Neurosci. 2003, 23, 2008–2013. [Google Scholar] [CrossRef]
- Lewandowski, C.T.; Maldonado Weng, J.; LaDu, M.J. Alzheimer’s disease pathology in APOE transgenic mouse models: The Who, What, When, Where, Why, and How. Neurobiol. Dis. 2020, 139, 104811. [Google Scholar] [CrossRef]
- Muller, T. Catechol-O-methyltransferase enzyme: Cofactor S-adenosyl-L-methionine and related mechanisms. Int. Rev. Neurobiol. 2010, 95, 49–71. [Google Scholar]
- Seshadri, S.; Beiser, A.; Selhub, J.; Jacques, P.F.; Rosenberg, I.H.; D’Agostino, R.B.; Wilson, P.W.; Wolf, P.A. Plasma homocysteine as a risk factor for dementia and Alzheimer’s disease. N. Engl. J. Med. 2002, 346, 476–483. [Google Scholar] [CrossRef]
- Zheng, Z.; Wang, J.; Yi, L.; Yu, H.; Kong, L.; Cui, W.; Chen, H.; Wang, C. Correlation between behavioural and psychological symptoms of Alzheimer type dementia and plasma homocysteine concentration. BioMed Res. Int. 2014, 2014, 383494. [Google Scholar] [CrossRef]
- Reif, A.; Pfuhlmann, B.; Lesch, K.P. Homocysteinemia as well as methylenetetrahydrofolate reductase polymorphism are associated with affective psychoses. Prog. Neuro-psychopharmacol. Biol. Psychiatry 2005, 29, 1162–1168. [Google Scholar] [CrossRef]
- Monji, A.; Yanagimoto, K.; Maekawa, T.; Sumida, Y.; Yamazaki, K.; Kojima, K. Plasma folate and homocysteine levels may be related to interictal "schizophrenia-like" psychosis in patients with epilepsy. J. Clin. Psychopharmacol. 2005, 25, 3–5. [Google Scholar] [CrossRef]
- Vogel, T.; Dali-Youcef, N.; Kaltenbach, G.; Andres, E. Homocysteine, vitamin B12, folate and cognitive functions: A systematic and critical review of the literature. Int. J. Clin. Pract. 2009, 63, 1061–1067. [Google Scholar] [CrossRef] [PubMed]
- Frosst, P.; Blom, H.J.; Milos, R.; Goyette, P.; Sheppard, C.A.; Matthews, R.G.; Boers, G.J.; den Heijer, M.; Kluijtmans, L.A.; van den Heuvel, L.P. A candidate genetic risk factor for vascular disease: A common mutation in methylenetetrahydrofolate reductase. Nat. Genet. 1995, 10, 111–113. [Google Scholar] [CrossRef] [PubMed]
- Rozen, R. Genetic predisposition to hyperhomocysteinemia: Deficiency of methylenetetrahydrofolate reductase (MTHFR). Thromb. Haemost. 1997, 78, 523–526. [Google Scholar] [CrossRef] [PubMed]
- Rai, V. Methylenetetrahydrofolate Reductase (MTHFR) C677T Polymorphism and Alzheimer Disease Risk: A Meta-Analysis. Mol. Neurobiol. 2017, 54, 1173–1186. [Google Scholar] [CrossRef]
- Stoccoro, A.; Tannorella, P.; Salluzzo, M.G.; Ferri, R.; Romano, C.; Nacmias, B.; Siciliano, G.; Migliore, L.; Coppede, F. The Methylenetetrahydrofolate Reductase C677T Polymorphism and Risk for Late-Onset Alzheimer’s disease: Further Evidence in an Italian Multicenter Study. J. Alzheimers Dis. 2017, 56, 1451–1457. [Google Scholar] [CrossRef]
- Hu, Q.; Teng, W.; Li, J.; Hao, F.; Wang, N. Homocysteine and Alzheimer’s Disease: Evidence for a Causal Link from Mendelian Randomization. J. Alzheimers Dis. 2016, 52, 747–756. [Google Scholar] [CrossRef]
- Roussotte, F.F.; Hua, X.; Narr, K.L.; Small, G.W.; Thompson, P.M. Alzheimer’s Disease Neuroimaging Initiative The C677T variant in MTHFR modulates associations between brain integrity, mood, and cognitive functioning in old age. Biol. Psychiatry Cogn. Neurosci. Neuroimaging 2017, 2, 280–288. [Google Scholar]
- van der Put, N.M.; Gabreels, F.; Stevens, E.M.; Smeitink, J.A.; Trijbels, F.J.; Eskes, T.K.; van den Heuvel, L.P.; Blom, H.J. A second common mutation in the methylenetetrahydrofolate reductase gene: An additional risk factor for neural-tube defects? Am. J. Hum. Genet. 1998, 62, 1044–1051. [Google Scholar] [CrossRef]
- Weisberg, I.; Tran, P.; Christensen, B.; Sibani, S.; Rozen, R. A second genetic polymorphism in methylenetetrahydrofolate reductase (MTHFR) associated with decreased enzyme activity. Mol. Genet. Metab. 1998, 64, 169–172. [Google Scholar] [CrossRef]
- McKhann, G.; Drachman, D.; Folstein, M.; Katzman, R.; Price, D.; Stadlan, E.M. Clinical diagnosis of Alzheimer’s disease: Report of the NINCDS-ADRDA Work Group under the auspices of Department of Health and Human Services Task Force on Alzheimer’s Disease. Neurology 1984, 34, 939–944. [Google Scholar] [CrossRef]
- Folstein, M.F.; Folstein, S.E.; McHugh, P.R. “Mini-mental state”. A practical method for grading the cognitive state of patients for the clinician. J. Psychiatr. Res. 1975, 12, 189–198. [Google Scholar] [CrossRef]
- Miller, M.D.; Paradis, C.F.; Houck, P.R.; Mazumdar, S.; Stack, J.A.; Rifai, A.H.; Mulsant, B.; Reynolds, C.F., 3rd. Rating chronic medical illness burden in geropsychiatric practice and research: Application of the Cumulative Illness Rating Scale. Psychiatry Res. 1992, 41, 237–248. [Google Scholar] [CrossRef]
- Katz, S.; Downs, T.D.; Cash, H.R.; Grotz, R.C. Progress in development of the index of ADL. Gerontologist 1970, 10, 20–30. [Google Scholar] [CrossRef] [PubMed]
- Lawton, M.P.; Brody, E.M. Assessment of older people: Self-maintaining and instrumental activities of daily living. Gerontologist 1969, 9, 179–186. [Google Scholar] [CrossRef] [PubMed]
- Cummings, J.L.; Mega, M.; Gray, K.; Rosenberg-Thompson, S.; Carusi, D.A.; Gornbein, J. The Neuropsychiatric Inventory: Comprehensive assessment of psychopathology in dementia. Neurology 1994, 44, 2308–2314. [Google Scholar] [CrossRef] [PubMed]
- Desjardins, P.; Conklin, D. NanoDrop microvolume quantitation of nucleic acids. J. Vis. Exp. 2010, 45, 2565. [Google Scholar] [CrossRef]
- Ingelsson, M.; Shin, Y.; Irizarry, M.C.; Hyman, B.T.; Lilius, L.; Forsell, C.; Graff, C. Genotyping of apolipoprotein E: Comparative evaluation of different protocols. Curr. Protoc. Hum. Genet. 2003, 38, 9–14. [Google Scholar] [CrossRef]
- Gorsuch, R. Factor Analysis; Erlbaum: Hillsdale, NJ, USA, 1983. [Google Scholar]
- Breiman, L.; Friedman, J.; Stone, C.J.; Olshen, R.A. Classification and Regression Trees; CRC Press: Boca Raton, FL, USA, 1984. [Google Scholar]
- Zhang, H.; Bonney, G. Use of classification trees for association studies. Genet. Epidemiol. 2000, 19, 323–332. [Google Scholar] [CrossRef]
- Biggs, D.; De Ville, B.; Suen, E. A method of choosing multiway partitions for classification and decision trees. J. Appl. Stat. 1991, 18, 49–62. [Google Scholar] [CrossRef]
- Deardorff, W.J.; Grossberg, G.T. Behavioral and psychological symptoms in Alzheimer’s dementia and vascular dementia. Handb. Clin. Neurol. 2019, 165, 5–32. [Google Scholar]
- Shah, C.; DeMichele-Sweet, M.A.; Sweet, R.A. Genetics of psychosis of Alzheimer disease. Am. J. Med. Genet. B Neuropsychiatr. Genet. 2017, 174, 27–35. [Google Scholar] [CrossRef] [PubMed]
- DeMichele-Sweet, M.A.A.; Weamer, E.A.; Klei, L.; Vrana, D.T.; Hollingshead, D.J.; Seltman, H.J.; Sims, R.; Foroud, T.; Hernandez, I.; Moreno-Grau, S.; et al. Genetic risk for schizophrenia and psychosis in Alzheimer disease. Mol. Psychiatry 2018, 23, 963–972. [Google Scholar] [CrossRef] [PubMed]
- Panza, F.; Frisardi, V.; Seripa, D.; D’Onofrio, G.; Santamato, A.; Masullo, C.; Logroscino, G.; Solfrizzi, V.; Pilotto, A. Apolipoprotein E genotypes and neuropsychiatric symptoms and syndromes in late-onset Alzheimer’s disease. Ageing Res. Rev. 2012, 11, 87–103. [Google Scholar] [CrossRef] [PubMed]
- Ruthirakuhan, M.; Lanctot, K.L.; Di Scipio, M.; Ahmed, M.; Herrmann, N. Biomarkers of agitation and aggression in Alzheimer’s disease: A systematic review. Alzheimers Dement. 2018, 14, 1344–1376. [Google Scholar] [CrossRef]
- Rosenberg, P.B.; Nowrangi, M.A.; Lyketsos, C.G. Neuropsychiatric symptoms in Alzheimer’s disease: What might be associated brain circuits? Mol. Asp. Med. 2015, 43–44, 25–37. [Google Scholar] [CrossRef]
- Banning, L.C.P.; Janssen, E.P.C.J.; Hamel, R.E.G.; de Vugt, M.; Kohler, S.; Wolfs, C.A.G.; Oosterveld, S.M.; Melis, R.J.F.; Olde Rikkert, M.G.M.; Kessels, R.P.C.; et al. Determinants of Cross-Sectional and Longitudinal Health-Related Quality of Life in Memory Clinic Patients Without Dementia. J. Geriatr. Psychiatry Neurol. 2019, 33, 256–264. [Google Scholar] [CrossRef]
- Garcia-Segura, M.E.; Fischer, C.E.; Schweizer, T.A.; Munoz, D.G. APOE varepsilon4/varepsilon4 Is Associated with Aberrant Motor Behavior Through Both Lewy Body and Cerebral Amyloid Angiopathy Pathology in High Alzheimer’s Disease Pathological Load. J. Alzheimers Dis. 2019, 72, 1077–1087. [Google Scholar] [CrossRef]
- Oliveira, F.F.; Chen, E.S.; Smith, M.C.; Bertolucci, P.H. Associations of cerebrovascular metabolism genotypes with neuropsychiatric symptoms and age at onset of Alzheimer’s disease dementia. Braz. J. Psychiatry. 2017, 39, 95–103. [Google Scholar] [CrossRef]
- Steinberg, M.; Corcoran, C.; Tschanz, J.T.; Huber, C.; Welsh-Bohmer, K.; Norton, M.C.; Zandi, P.; Breitner, J.C.; Steffens, D.C.; Lyketsos, C.G. Risk factors for neuropsychiatric symptoms in dementia: The Cache County Study. Int. J. Geriatr. Psychiatry 2006, 21, 824–830. [Google Scholar] [CrossRef]
- Polito, L.; Poloni, T.E.; Vaccaro, R.; Abbondanza, S.; Mangieri, M.; Davin, A.; Villani, S.; Guaita, A. High homocysteine and epistasis between MTHFR and APOE: Association with cognitive performance in the elderly. Exp. Gerontol. 2016, 76, 9–16. [Google Scholar] [CrossRef]
- Durmaz, A.; Kumral, E.; Durmaz, B.; Onay, H.; Aslan, G.I.; Ozkinay, F.; Pehlivan, S.; Orman, M.; Cogulu, O. Genetic factors associated with the predisposition to late onset Alzheimer’s disease. Gene 2019, 707, 212–215. [Google Scholar] [CrossRef] [PubMed]
- Yi, J.; Xiao, L.; Zhou, S.Q.; Zhang, W.J.; Liu, B.Y. The C677T Polymorphism of the Methylenetetrahydrofolate Reductase Gene and Susceptibility to Late-onset Alzheimer’s Disease. Open Med. 2019, 14, 32–40. [Google Scholar] [CrossRef] [PubMed]
- Chen, Z.; Schwahn, B.C.; Wu, Q.; He, X.; Rozen, R. Postnatal cerebellar defects in mice deficient in methylenetetrahydrofolate reductase. Int. J. Dev. Neurosci. 2005, 23, 465–474. [Google Scholar] [CrossRef] [PubMed]
- Fatemi, S.H.; Earle, J.A.; McMenomy, T. Reduction in Reelin immunoreactivity in hippocampus of subjects with schizophrenia, bipolar disorder and major depression. Mol. Psychiatry 2000, 5, 654–663. [Google Scholar] [CrossRef] [PubMed]
- Soni, R.M.; Tiwari, S.C.; Mahdi, A.A.; Kohli, N. Serum Homocysteine and Behavioral and Psychological Symptoms of Dementia: Is There Any Correlation in Alzheimer’s Disease? Ann. Neurosci. 2019, 25, 152–159. [Google Scholar] [CrossRef]


{kind=link}
| Gender (F/M) | 241/121 | Female | Male |
|---|---|---|---|
| Age (years) | 80.5 ± 7.0 | 80.9 ± 7.1 | 79.7 ± 6.7 |
| Schooling (years) | 6.0 ± 3.6 | 5.4 ± 2.9 | 7.4 ± 4.4 |
| MMSE, total score | 11.7 ± 7.3 | 12.0 ± 6.9 | 10.9 ± 8.1 |
| Onset (years) | 76.1 ± 7.9 | 76.5 ± 8.1 | 75.4 ± 7.6 |
| Illness Duration (years) | 4.5 ± 2.9 | 4.4 ± 2.6 | 4.5 ± 3.5 |
| BMI | 22.3 ± 4.1 | 22.2 ± 4.2 | 22.5 ± 3.8 |
| IADL | 7.2 ± 1.5 | 7.4 ± 1.2 | 6.8 ± 1.9 |
| BADL | 3.7 ± 1.9 | 3.6 ± 1.9 | 3.8 ± 1.8 |
| Tinetti | 19.8 ± 5.4 | 19.8 ± 5.2 | 19.6 ± 5.9 |
| CIRS | 12.7 ± 9.7 | 12.2 ± 9.5 | 13.8 ± 10.0 |
| Hypertension | 27.9% | 29.5% | 24.8% |
| Cardiopathy | 28.7% | 26.1% | 33.9% |
| Hypercholesterolemia | 4.7% | 5.8% | 2.5% |
| Diabetes | 6.6% | 5.4% | 9.1% |
| Psychiatric diseases | 26.0% | 27.4% | 23.1% |
| AChEIs | 20.2% | 21.6% | 17.4% |
| Neuroleptics | 45.5% | 41.1% | 51.2% |
| Antidepressants | 45.6% | 46.9% | 43.0% |
| Benzodiazepines/hypnotics | 41.4% | 46.1% | 32.2% |
| APOE Haplotypes (rs429358 and rs7412) | MTHFR (rs1801133: C677T) | MTHFR (rs1801131: A1298C) | COMT (rs4680: V158M) | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| HWE | χ2 = 0.91 | p = 0.92 | HWE | χ2 = 1.70 | p = 0.19 | HWE | χ2 = 0.53 | p = 0.47 | HWE | χ2 = 1.22 | p = 0.27 |
| Alleles | N | freq | Alleles | N | freq | Alleles | N | freq | Alleles | N | freq |
| ɛ2 | 20 | 0.03 | T | 314 | 0.43 | A | 499 | 0.69 | A | 330 | 0.46 |
| ɛ3 | 510 | 0.70 | C | 410 | 0.57 | C | 225 | 0.31 | G | 394 | 0.54 |
| ɛ4 | 194 | 0.27 | |||||||||
| total | 724 | 1.00 | total | 724 | 1.00 | total | 724 | 1.00 | total | 724 | 1.00 |
| Genotypes | N | freq | Genotypes | N | freq | Genotypes | N | freq | Genotypes | N | freq |
| ɛ2 ɛ3 | 16 | 0.04 | TT | 62 | 0.17 | AA | 169 | 0.47 | AA | 70 | 0.19 |
| ɛ2 ɛ4 | 4 | 0.01 | TC | 190 | 0.52 | AC | 161 | 0.44 | AG | 190 | 0.52 |
| ɛ3 ɛ3 | 178 | 0.49 | CC | 110 | 0.30 | CC | 32 | 0.09 | GG | 102 | 0.28 |
| ɛ3 ɛ4 | 138 | 0.38 | |||||||||
| ɛ4 ɛ4 | 26 | 0.07 | |||||||||
| total | 362 | 1.00 | total | 362 | 1.00 | total | 362 | 1.00 | total | 362 | 1.00 |
| ɛ2 carriers | 20 | 0.06 | T carriers | 252 | 0.70 | A carriers | 330 | 0.91 | A carriers | 260 | 0.72 |
| ɛ3 carriers | 332 | 0.92 | C carriers | 300 | 0.83 | C carriers | 193 | 0.53 | G carriers | 292 | 0.81 |
| ɛ4 carriers | 168 | 0.46 | |||||||||
| “Severity*Frequencies” Groups N Subjects (%) & | ||||
|---|---|---|---|---|
| Symptoms (“Severity*Frequencies” = 0–12) | Mean ± SD § | Free | Low | High |
| (NPI 0) | (NPI 1–4) | (NPI 6–12) | ||
| Agitation | 4.96 ± 4.32 | 102 (33.0) | 47 (15.2) | 160 (51.8) |
| Irritability | 4.57 ± 4.25 | 109 (35.4) | 52 (16.9) | 147 (47.7) |
| Night-time behavior disturbances | 4.22 ± 4.55 | 136 (44.0) | 44 (14.2) | 129 (41.7) |
| Aberrant motor behavior | 4.12 ± 4.72 | 148 (48.2) | 39 (12.7) | 120 (39.1) |
| Apathy | 3.03 ± 4.19 | 178 (58.0) | 42 (13.7) | 87 (28.3) |
| Delusions | 3.00 ± 4.00 | 166 (54.1) | 52 (16.9) | 89 (29.0) |
| Anxiety | 2.53 ± 4.10 | 200 (65.4) | 30 (9.8) | 76 (24.8) |
| Depression | 2.50 ± 3.90 | 185 (60.3) | 53 (17.3) | 69 (22.5) |
| Hallucination | 2.30 ± 3.55 | 187 (60.9) | 55 (17.9) | 65 (21.2) |
| Appetite and eating disturbances | 1.94 ± 3.59 | 223 (72.2) | 28 (9.1) | 58 (18.8) |
| Disinhibition | 0.93 ± 2.44 | 253 (82.4) | 28 (9.1) | 26 (8.5) |
| Euphoria | 0.12 ± 0.86 | 299 (97.4) | 6 (2.0) | 2 (0.7) |
| NPI, total score (0–144) | 34.1 ± 22.6 | |||
| NPI, n symptoms | 4.9 ± 2.4 | |||
| Symptoms | Endophenotype Components | |||
|---|---|---|---|---|
| Factor 1 | Factor 2 | Factor 3 | Factor 4 | |
| Mood | Hyperactivity | Psychosis | Frontal | |
| Delusions | 0.276 | 0.372 | 0.463 | 0.144 |
| Hallucination | 0.022 | 0.011 | 0.690 | 0.248 |
| Agitation | 0.058 | 0.654 | 0.468 | 0.068 |
| Depression | 0.855 | 0.058 | 0.166 | 0.089 |
| Anxiety | 0.820 | 0.062 | 0.156 | 0.075 |
| Euphoria | −0.040 | −0.109 | 0.186 | 0.766 |
| Apathy | 0.579 | 0.292 | −0.212 | −0.184 |
| Disinhibition | 0.131 | 0.376 | −0.166 | 0.687 |
| Irritability | 0.028 | 0.645 | 0.367 | 0.119 |
| Aberrant motor behavior | 0.104 | 0.373 | 0.402 | −0.157 |
| Night-time behavior disturbances | 0.029 | 0.056 | 0.621 | −0.087 |
| Appetite and eating disturbances | 0.191 | 0.671 | −0.157 | 0.014 |
| Mean of N Subjects ± SD £ (% Mean of N Subjects ± SD) $ | ||||
|---|---|---|---|---|
| Endophenotypes (Components; “Severity*Frequencies” Range) | Mean ± SD § | Free | Low | High |
| Psychosis (Delusions, Hallucination, Agitation, Aberrant motor behavior, Night-time behavior disturbances; 0–60) | 18.5 ± 13.3 | 148 ± 32 (48.0 ± 10.5) | 47 ± 6 (15.4 ± 2.1) | 113 ± 37 (36.6 ± 11.8) |
| Hyperactivity (Agitation, Irritability, Appetite and eating disturbances; 0–36) | 11.4 ± 9.2 | 145 ± 68 (46.9 ± 22.0) | 42 ± 13 (13.7 ± 4.1) | 122 ± 56 (39.4 ± 18.0) |
| Mood (Depression, Anxiety, Apathy; 0–36) | 8.1 ± 9.4 | 188 ± 11 (61.2 ± 3.8) | 42 ± 12 (13.6 ± 3.7) | 77 ± 9 (25.0 ± 3.0) |
| Frontal (Euphoria, Disinhibition; 0–24) | 1.0 ± 2.7 | 276 ± 33 (89.9 ± 10.6) | 17 ± 16 (5.5 ± 5.1) | 14 ± 17 (4.6 ± 5.5) |
| Gene | Free + Low & | High & | ||
|---|---|---|---|---|
| N (Freq.) | N (Freq.) | |||
| Agitation | APOE | χ2 = 7.435, padjusted = 0.006 OR = 1.87; 95% CI: 1.19–2.95 | ||
| Ɛ4-carriers | 58 (0.39) | 86 (0.54) | ||
| Ɛ4-non-carriers | 91 (0.61) | 72(0.46) | ||
| total | 149 (1.00) | 158 (1.00) | ||
| Aberrant motor behavior | APOE | χ2 = 7.553, padjusted = 0.006 OR = 1.91; 95% CI: 1.20–3.04 | ||
| 4-carriers | 76 (0.41) | 68 (0.57) | ||
| Ɛ4-non-carriers | 111 (0.59) | 52 (0.43) | ||
| total | 187 (1.00) | 120 (1.00) | ||
| Delusions | MTHFR | χ2 = 4.363, padjusted = 0.037 OR = 1.75; 95% CI: 1.04–2.94 | ||
| CC | 59 (0.27) | 35 (0.39) | ||
| Genotypes_C677T | 159 (0.73) | 54 (0.61) | ||
| T-carriers_C677T | 218 (1.00) | 89 (1.00) | ||
| Appetite/eating abnormalities | APOE | χ2 = 5.922, padjusted = 0.015 OR = 2.06; 95% CI: 1.14–3.71 | ||
| Ɛ4-carriers | 109 (0.44) | 35 (0.60) | ||
| Ɛ4-non-carriers | 141 (0.56) | 22 (0.40) | ||
| total | 250 (1.00) | 57 (1.00) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Scassellati, C.; Ciani, M.; Maj, C.; Geroldi, C.; Zanetti, O.; Gennarelli, M.; Bonvicini, C. Behavioral and Psychological Symptoms of Dementia (BPSD): Clinical Characterization and Genetic Correlates in an Italian Alzheimer’s Disease Cohort. J. Pers. Med. 2020, 10, 90. https://doi.org/10.3390/jpm10030090
Scassellati C, Ciani M, Maj C, Geroldi C, Zanetti O, Gennarelli M, Bonvicini C. Behavioral and Psychological Symptoms of Dementia (BPSD): Clinical Characterization and Genetic Correlates in an Italian Alzheimer’s Disease Cohort. Journal of Personalized Medicine. 2020; 10(3):90. https://doi.org/10.3390/jpm10030090
Chicago/Turabian StyleScassellati, Catia, Miriam Ciani, Carlo Maj, Cristina Geroldi, Orazio Zanetti, Massimo Gennarelli, and Cristian Bonvicini. 2020. "Behavioral and Psychological Symptoms of Dementia (BPSD): Clinical Characterization and Genetic Correlates in an Italian Alzheimer’s Disease Cohort" Journal of Personalized Medicine 10, no. 3: 90. https://doi.org/10.3390/jpm10030090
APA StyleScassellati, C., Ciani, M., Maj, C., Geroldi, C., Zanetti, O., Gennarelli, M., & Bonvicini, C. (2020). Behavioral and Psychological Symptoms of Dementia (BPSD): Clinical Characterization and Genetic Correlates in an Italian Alzheimer’s Disease Cohort. Journal of Personalized Medicine, 10(3), 90. https://doi.org/10.3390/jpm10030090