
Utility of Serum Biomarkers of Myocardial Fibrosis in High-Gradient Severe Aortic Stenosis: An Explorative Cardiovascular Magnetic Resonance Imaging-Based Study
 ,
,  , and
, and
Abstract
1. Introduction
2. Methods
2.1. Study Design
2.2. CMR Image Acquisition
2.3. CMR Image Analysis
2.4. Blood Sample Collection and Storage
2.5. Enzyme-Linked Immunosorbent Assay (ELISA)
2.6. Statistical Analysis
3. Results
3.1. Study Population
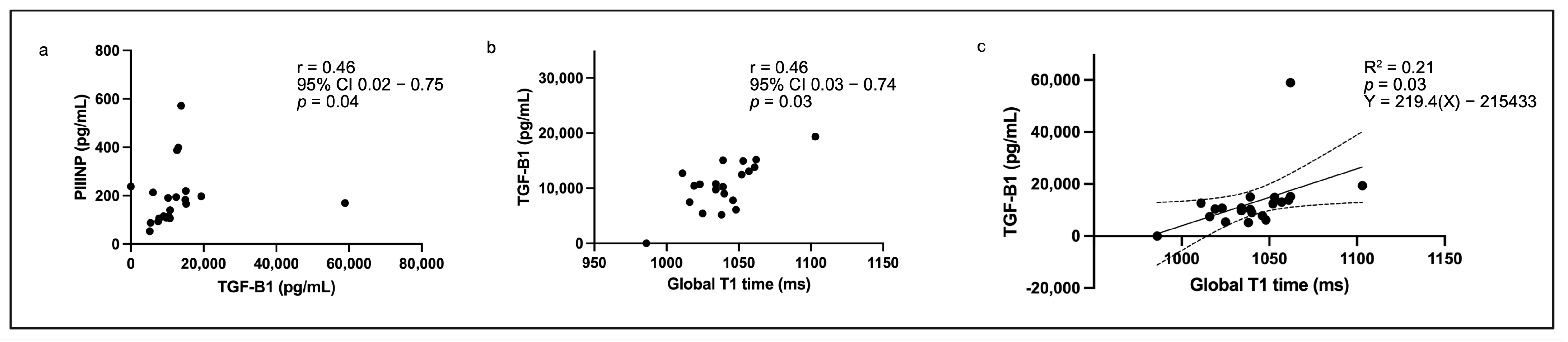
3.2. Biomarkers in the Total Cohort
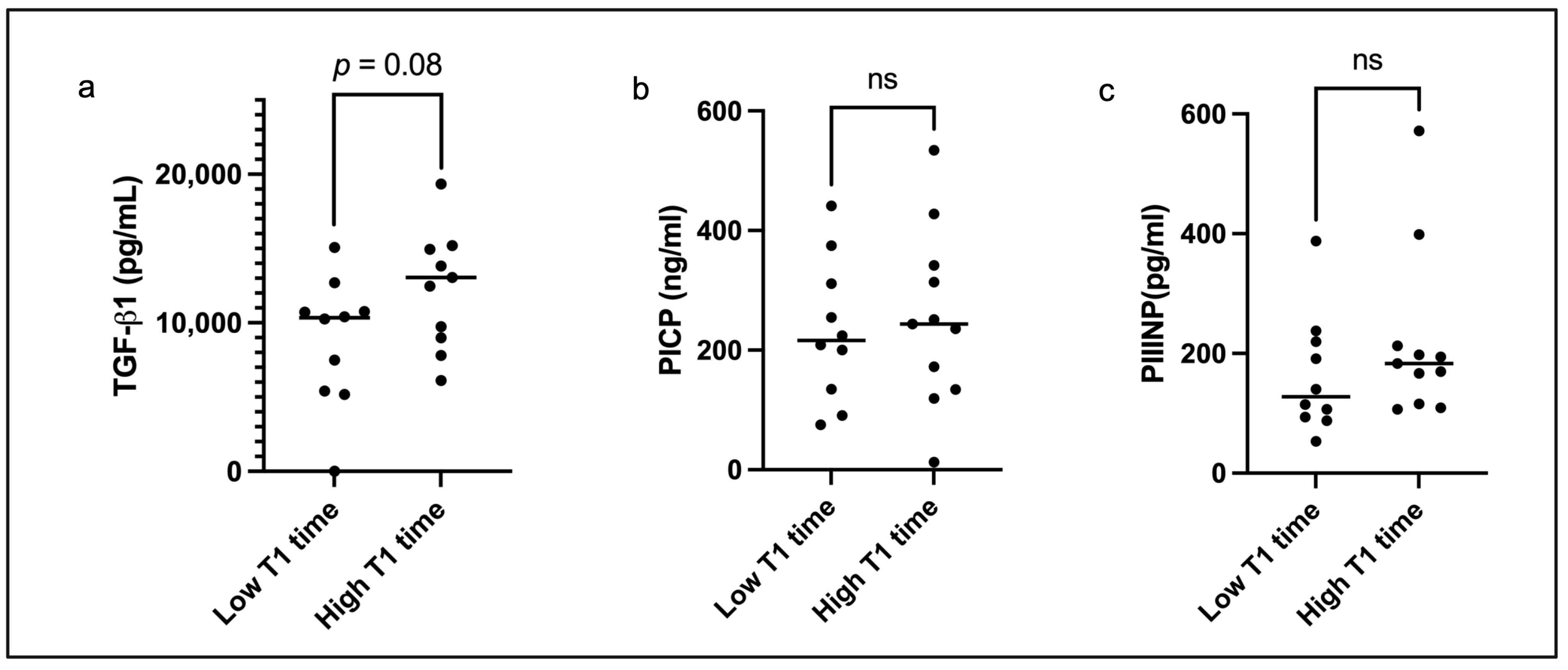
3.3. Left Ventricular Remodelling and Serum TGF-β1 in the Subgroup with High Global T1 Relaxation Time
4. Discussion
4.1. TGF-β1 Is a Potential Surrogate Marker of Diffuse Interstitial Fibrosis
4.2. No Biomarker Associations with Replacement Fibrosis
4.3. Lack of Association Between PICP/PIIINP and Myocardial Fibrosis on CMR
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| AS | aortic stenosis |
| LVEF | left ventricular ejection fraction |
| LV | left ventricle/left ventricular |
| BNP | B-type natriuretic peptide |
| NT-pro BNP | N-terminal pro-B-type natriuretic peptide (NT-pro BNP) |
| CMR | cardiovascular magnetic resonance |
| LGE | late gadolinium enhancement |
| TGF-β1 | transforming growth factor beta-1 |
| PICP | procollagen I carboxy-terminal propeptide |
| PIIINP | procollagen III amino-terminal propeptide |
| AVA | aortic valve area |
| ECV | extracellular volume |
| LVEDV | left ventricular end-diastolic volume |
| LVESV | left ventricular end-systolic volume |
| LVSV | left ventricular stroke volume |
| LVM | left ventricular mass |
| ESWS | end-systolic wall stress |
| LVGFI | left ventricular global function index |
| ELISA | enzyme-linked immunosorbent assay |
| SBP | systolic blood pressure |
| DBP | diastolic blood pressure |
| MAPSE | mitral annular plane systolic excursion |
References
- Coffey, S.; Roberts-Thomson, R.; Brown, A.; Carapetis, J.; Chen, M.; Enriquez-Sarano, M.; Zühlke, L.; Prendergast, B.D. Global epidemiology of valvular heart disease. Nat. Rev. Cardiol. 2021, 18, 853–864. [Google Scholar] [CrossRef] [PubMed]
- Vahanian, A.; Beyersdorf, F.; Praz, F.; Milojevic, M.; Baldus, S.; Bauersachs, J.; Capodanno, D.; Conradi, L.; De Bonis, M.; De Paulis, R.; et al. 2021 ESC/EACTS Guidelines for the management of valvular heart disease: Developed by the Task Force for the management of valvular heart disease of the European Society of Cardiology (ESC) and the European Association for Cardio-Thoracic Surgery (EACTS). Eur. Heart J. 2022, 43, 561–632. [Google Scholar] [CrossRef]
- Otto, C.M.; Nishimura, R.A.; Bonow, R.O.; Carabello, B.A.; Erwin, J.P.; Gentile, F.; Jneid, H.; Krieger, E.V.; Mack, M.; McLeod, C.; et al. 2020 ACC/AHA Guideline for the management of patients with valvular heart disease: A report of the American College of Cardiology/American Heart Association joint committee on clinical practice guidelines. Circulation 2021, 143, e27–e227. [Google Scholar]
- Lee, G.; Chikwe, J.; Milojevic, M.; Wijeysundera, H.C.; Biondi-Zoccai, G.; Flather, M.; Gaudino, M.F.L.; E Fremes, S.; Tam, D.Y. ESC/EACTS vs. ACC/AHA guidelines for the management of severe aortic stenosis. Eur. Heart J. 2023, 44, 796–812. [Google Scholar] [CrossRef] [PubMed]
- Everett, R.J.; Treibel, T.A.; Fukui, M.; Lee, H.; Rigolli, M.; Singh, A.; Bijsterveld, P.; Tastet, L.; Al Musa, T.; Dobson, L.; et al. Extracellular myocardial volume in patients with aortic stenosis. J. Am. Coll. Cardiol. 2020, 75, 304–316. [Google Scholar] [CrossRef]
- Lee, H.; Park, J.-B.; Yoon, Y.E.; Park, E.-A.; Kim, H.-K.; Lee, W.; Kim, Y.-J.; Cho, G.-Y.; Sohn, D.-W.; Greiser, A.; et al. Noncontrast myocardial T1 mapping by cardiac magnetic resonance predicts outcome in patients with aortic stenosis. JACC Cardiovasc. Imaging 2018, 11, 974–983. [Google Scholar] [CrossRef]
- Capoulade, R.; Clavel, M.-A.; Le Ven, F.; Dahou, A.; Thébault, C.; Tastet, L.; Shen, M.; Arsenault, M.; Bédard, É.; Beaudoin, J.; et al. Impact of left ventricular remodeling patterns on outcomes in patients with aortic stenosis. Eur. Heart J. Cardiovasc. Imaging 2017, 18, 1378–1387. [Google Scholar] [CrossRef]
- Barbieri, A.; Bartolacelli, Y.; Bursi, F.; Manicardi, M.; Boriani, G. Remodelling classification system considering left ventricular volume in patients with aortic stenosis: Association with adverse cardiovascular outcomes. Echocardiography 2019, 36, 639–650. [Google Scholar] [CrossRef]
- Bohbot, Y.; Ravenstein, C.d.M.d.; Chadha, G.; Rusinaru, D.; Belkhir, K.; Trouillet, C.; Pasquet, A.; Marechaux, S.; Vanoverschelde, J.-L.; Tribouilloy, C. Relationship between left ventricular ejection fraction and mortality in asymptomatic and minimally symptomatic patients with severe aortic stenosis. JACC Cardiovasc. Imaging 2019, 12, 38–48. [Google Scholar] [CrossRef]
- Jacquemyn, X.; Strom, J.B.; Strange, G.; Playford, D.; Stewart, S.; Kutty, S.; Bhatt, D.L.; Bleiziffer, S.; Grubb, K.J.; Pellikka, P.A.; et al. Moderate aortic valve stenosis is associated with increased mortality rate and lifetime loss: Systematic review and meta-analysis of reconstructed time-to-event data of 409 680 patients. J. Am. Heart Assoc. 2024, 13, e033872. [Google Scholar] [CrossRef]
- Cavalcante, P.N.; Kanhouche, G.; Rosa, V.E.E.; Campos, C.M.; Lopes, M.P.; Lopes, M.A.A.A.M.; Sampaio, R.O.; Júnior, F.S.d.B.; Tarasoutchi, F.; Abizaid, A.A.C. B-type natriuretic peptide and N-terminal Pro-B-type natriuretic peptice in severe aortic stenosis: A comprehensive literature review. Front. Cardiovasc. Med. 2023, 10, 1182530. [Google Scholar] [CrossRef] [PubMed]
- Călin, A.; Roşca, M.; Beladan, C.C.; Enache, R.; Mateescu, A.D.; Ginghină, C.; Popescu, B.A. The left ventricle in aortic stenosis—Imaging assessment and clinical implications. Cardiovasc. Ultrasound 2015, 13, 22. [Google Scholar] [CrossRef] [PubMed]
- Calin, A.; Mateescu, A.D.; Popescu, A.C.; Bing, R.; Dweck, M.R.; Popescu, B.A. Role of advanced left ventricular imaging in adults with aortic stenosis. Heart 2020, 106, 962–969. [Google Scholar] [CrossRef]
- Bing, R.; Cavalcante, J.L.; Everett, R.J.; Clavel, M.-A.; Newby, D.E.; Dweck, M.R. Imaging and impact of myocardial fibrosis in aortic stenosis. JACC Cardiovasc. Imaging 2019, 12, 283–296. [Google Scholar] [CrossRef]
- Chin, C.W.; Everett, R.J.; Kwiecinski, J.; Vesey, A.T.; Yeung, E.; Esson, G.; Jenkins, W.; Koo, M.; Mirsadraee, S.; White, A.C.; et al. Myocardial fibrosis and cardiac decompensation in aortic stenosis. JACC Cardiovasc. Imaging 2017, 10, 1320–1333. [Google Scholar] [CrossRef]
- Castrichini, M.; Vitrella, G.; De Luca, A.; Altinier, A.; Korcova, R.; Pagura, L.; Radesich, C.; Sinagra, G. Clinical impact of myocardial fibrosis in severe aortic stenosis. Eur. Heart J. Suppl. 2021, 23 (Suppl. SE), E147–E150. [Google Scholar] [CrossRef]
- Bull, S.; White, S.K.; Piechnik, S.K.; Flett, A.S.; Ferreira, V.M.; Loudon, M.; Francis, J.M.; Karamitsos, T.D.; Prendergast, B.D.; Robson, M.D.; et al. Human non-contrast T1 values and correlation with histology in diffuse fibrosis. Heart 2013, 99, 932–937. [Google Scholar] [CrossRef] [PubMed]
- Park, S.-J.; Cho, S.W.; Kim, S.M.; Ahn, J.; Carriere, K.; Jeong, D.S.; Lee, S.-C.; Park, S.W.; Choe, Y.H.; Park, P.W.; et al. Assessment of myocardial fibrosis using multimodality imaging in severe aortic stenosis. JACC Cardiovasc. Imaging 2019, 12, 109–119. [Google Scholar] [CrossRef]
- Treibel, T.A.; Fontana, M.; Reant, P.; A Espinosa, M.; Castelletti, S.; Herrey, A.S.; Manisty, C.; Roberts, N.; Yap, J.; Moon, J. T1 mapping in severe aortic stenosis: Insights into LV remodelling. J. Cardiovasc. Magn. Reson. 2015, 17 (Suppl. S1), 089. [Google Scholar] [CrossRef]
- Lee, S.-P.; Lee, W.; Lee, J.M.; Park, E.-A.; Kim, H.-K.; Kim, Y.-J.; Sohn, D.-W. Assessment of diffuse myocardial fibrosis by using MR imaging in asymptomatic patients with aortic stenosis. Radiology 2015, 274, 359–369. [Google Scholar] [CrossRef]
- Weidemann, F.; Herrmann, S.; Störk, S.; Niemann, M.; Frantz, S.; Lange, V.; Beer, M.; Gattenlöhner, S.; Voelker, W.; Ertl, G.; et al. Impact of myocardial fibrosis in patients with symptomatic severe aortic stenosis. Circulation 2009, 120, 157–184. [Google Scholar] [CrossRef] [PubMed]
- Dweck, M.R.; Joshi, S.; Murigu, T.; Alpendurada, F.; Jabbour, A.; Melina, G.; Banya, W.; Gulati, A.; Roussin, I.; Raza, S.; et al. Midwall fibrosis is an independent predictor of mortality in patients with aortic stenosis. J. Am. Coll. Cardiol. 2011, 58, 1271–1279. [Google Scholar] [CrossRef] [PubMed]
- Musa, T.A.; Treibel, T.A.; Vassiliou, V.S.; Captur, G.; Singh, A.; Chin, C.; Dobson, L.E.; Pica, S.; Loudon, M.; Malley, T.; et al. Myocardial scar and mortality in svere aortic stenosis. Circulation 2018, 138, 1935–1947. [Google Scholar] [CrossRef] [PubMed]
- Rajesh, G.N.; Thottian, J.J.; Subramaniam, G.; Desabandhu, V.; Sajeev, C.G.; Krishnan, M.N. Prevalence and prognostic significance of left ventricular myocardial late gadolinium enhancement in severe aortic stenosis. Indian Heart J. 2017, 69, 742–750. [Google Scholar] [CrossRef]
- Azevedo, C.F.; Nigri, M.; Higuchi, M.L.; Pomerantzeff, P.M.; Spina, G.S.; Sampaio, R.O.; Tarasoutchi, F.; Grinberg, M.; Rochitte, C.E. Prognostic significance of myocardial fibrosis quantification by histopathology and magnetic resonance imaging in patients with severe aortic valve disease. J. Am. Coll. Cardiol. 2010, 56, 278–287. [Google Scholar] [CrossRef]
- Lakshmanan, S.; Mbanze, I. A comparison of cardiovascular imaging practices in Africa, North America, and Europe: Two faces of the same coin. Eur. Heart J. Imaging Methods Pract. 2023, 1, qyad005. [Google Scholar] [CrossRef]
- López, B.; González, A.; Ravassa, S.; Beaumont, J.; Moreno, M.U.; José, G.S.; Querejeta, R.; Díez, J. Circulating biomarkers of myocardial fibrosis. The need for a reappraisal. J. Am. Coll. Cardiol. 2015, 65, 2449–2456. [Google Scholar] [CrossRef]
- Wittig, C.; Szulcek, R. Extracellular matrix protein ratios in the human heart and vessels: How to distinguish pathological from physiological changes? Front. Physiol. 2021, 12, 708656. [Google Scholar] [CrossRef]
- López, B.; González, A.; Querejeta, R.; Zubillaga, E.; Larman, M.; Díez, J. Galectin-3 and histological, molecular and biochemical aspects of myocardial fibrosis in heart failure of hypertensive origin. Eur. J. Heart Fail. 2015, 17, 385–392. [Google Scholar] [CrossRef]
- Villar, A.V.; Cobo, M.; Llano, M.; Montalvo, C.; González-Vílchez, F.; Martín-Durán, R.; Hurlé, M.A.; Nistal, J.F. Plasma levels of transforming growth factor-β1 reflect left ventricular remodeling in aortic stenosis. PLoS ONE 2009, 4, e8476. [Google Scholar] [CrossRef]
- Polyakova, V.; Richter, M.; Ganceva, N.; Lautze, H.-J.; Kamata, S.; Pöling, J.; Beiras-Fernandez, A.; Hein, S.; Szalay, Z.; Braun, T.; et al. Distinct structural and molecular features of the myocardial extracellular matrix remodeling in compensated and decompensated cardiac hypertrophy due to aortic stenosis. Int. J. Cardiol. Heart Vessel. 2014, 4, 145–160. [Google Scholar] [CrossRef]
- Kieć-Wilk, B.; Stolarz-Skrzypek, K.; Sliwa, A.; Zdzienicka, A.; Kawecka-Jaszcz, K. Peripheral blood concentrations of TGFβ1, IGF-1 and bFGF and remodelling of the left ventricle and blood vessels in hypertensive patients. Kardiol. Pol. 2010, 68, 996–1002. [Google Scholar] [PubMed]
- Podolec, J.; Baran, J.; Siedlinski, M.; Urbanczyk, M.; Krupinski, M.; Bartus, K.; Niewiara, L.; Podolec, M.; Guzik, T.; Tomkiewicz-Pajak, L.; et al. Serum rantes, transforming growth factor-β1 and interleukin-6 levels correlate with cardiac muscle fibrosis in patients with aortic valve stenosis. J. Physiol. Pharmacol. 2018, 69, 615–623. [Google Scholar]
- Kramer, C.M.; Barkhausen, J.; Flamm, S.D.; Kim, R.J.; Nagel, E. Standardized cardiovascular magnetic resonance (CMR) protocols 2013. J. Cardiovasc. Magn. Reson. 2013, 15, 91. [Google Scholar] [CrossRef] [PubMed]
- Schulz-Menger, J.; Bluemke, D.A.; Bremerich, J.; Flamm, S.D.; Fogel, M.A.; Friedrich, M.G.; Kim, R.J.; von Knobelsdorff-Brenkenhoff, F.; Kramer, C.M.; Pennell, D.J.; et al. Standardized image interpretation and post-processing in cardiovascular magnetic resonance—2020 update. J. Cardiovasc. Magn. Reson. 2020, 20, 19–22. [Google Scholar] [CrossRef]
- Reichek, N.; Wilson, J.; Sutton, M.S.J.; A Plappert, T.; Goldberg, S.; Hirshfeld, J.W. Noninvasive Determination of Left Ventricular End-systolic Stress: Validation of the Method and Initial Application. Circulation 1982, 65, 99–108. [Google Scholar] [CrossRef]
- Mewton, N.; Opdahl, A.; Choi, E.-Y.; Almeida, A.L.; Kawel, N.; Wu, C.O.; Burke, G.L.; Liu, S.; Liu, K.; Bluemke, D.A.; et al. Left ventricular global function index by magnetic resonance imaging—A novel marker for assessment of cardiac performance for the prediction of cardiovascular events. Hypertension 2013, 61, 770–778. [Google Scholar] [CrossRef]
- Dweck, M.R.; Joshi, S.; Murigu, T.; Gulati, A.; Alpendurada, F.; Jabbour, A.; Maceira, A.; Roussin, I.; Northridge, D.B.; Kilner, P.J.; et al. Left ventricular remodeling and hypertrophy in patients with aortic stenosis: Insights from cardiovascular magnetic resonance. J. Cardiovasc. Magn. Reson. 2012, 14, 50. [Google Scholar] [CrossRef]
- Flett, A.S.; Hayward, M.P.; Ashworth, M.T.; Hansen, M.S.; Taylor, A.M.; Elliot, P.M.; McGregor, C.; Moon, J.C. Equilibrium contrast cardiovascular magnetic resonance for the measurement of diffuse myocardial fibrosis: Preliminary validation in humans. Circulation 2010, 122, 138–144. [Google Scholar] [CrossRef]
- Haaf, P.; Garg, P.; Messroghli, D.R.; Broadbent, D.A.; Greenwood, J.P.; Plein, S. Cardiac T1 mapping and extracellular volume (ECV) in clinical practice: A comprehensive review. J. Cardiovasc. Magn. Reson. 2016, 18, 89. [Google Scholar] [CrossRef]
- Frangogiannis, N.G. Transforming growth factor-β in myocardial disease. Nat. Rev. Cardiol. 2022, 19, 435–455. [Google Scholar] [CrossRef] [PubMed]
- Yousefi, F.; Shabaninejad, Z.; Vakili, S.; Derakhshan, M.; Movahedpour, A.; Dabiri, H.; Ghasemi, Y.; Mahjoubin-Tehran, M.; Nikoozadeh, A.; Savardashtaki, A.; et al. TGF-β and WNT signaling pathways in cardiac fibrosis: Non-coding RNAs come into focus. Cell Commun. Signal. 2020, 18, 87. [Google Scholar] [CrossRef]
- Saadat, S.; Noureddini, M.; Mahjoubin-Tehran, M.; Nazemi, S.; Shojaie, L.; Aschner, M.; Maleki, B.; Abbasi-Kolli, M.; Moghadam, H.R.; Alani, B.; et al. Pivotal role of TGF-β/Smad signaling in cardiac fibrosis: Non-coding RNAs as effectual players. Front. Cardiovasc. Med. 2021, 7, 588347. [Google Scholar] [CrossRef] [PubMed]
- Robbertse, P.S.; Doubell, A.F.; Esterhuizen, T.M.; Herbst, P.G. Antiretroviral therapy and HIV-associated cardiovascular disease: A prospective cardiac biomarker and CMR tissue characterization study. ESC Heart Fail. 2024, 11, 748–758. [Google Scholar] [CrossRef] [PubMed]
- Stassen, J.; Ewe, S.H.; Hirasawa, K.; Butcher, S.C.; Singh, G.K.; Amanullah, M.R.; Sin, K.Y.K.; Ding, Z.P.; Pio, S.M.; Chew, N.W.S.; et al. Left ventricular remodelling patterns in patients with moderate aortic stenosis. Eur. Heart J. Cardiovasc. Imaging 2022, 23, 1326–1335. [Google Scholar] [CrossRef]
- Debry, N.; Maréchaux, S.; Rusinaru, D.; Peltier, M.; Messika-Zeitoun, D.; Menet, A.; Tribouilloy, C. Prognostic significance of left ventricular concentric remodelling in patients with aortic stenosis. Arch. Cardiovasc. Dis. 2017, 110, 26–34. [Google Scholar] [CrossRef]
- Rajah, M.R.; Doubell, A.F.; Herbst, P.G. Quantification of replacement fibrosis in aortic stenosis: A narrative review on the utility of cardiovascular magnetic resonance imaging. Diagnostics 2024, 14, 2435. [Google Scholar] [CrossRef]
- Treibel, T.A.; López, B.; González, A.; Menacho, K.; Schofield, R.S.; Ravassa, S.; Fontana, M.; White, S.K.; DiSalvo, C.; Roberts, N.; et al. Reappraising myocardial fibrosis in severe aortic stenosis: An invasive and non-invasive study in 133 patients. Eur. Heart J. 2018, 39, 699–709. [Google Scholar] [CrossRef]
- de Meester de Ravenstein, C.; Bouzin, C.; Lazam, S.; Boulif, J.; Amzulescu, M.; Melchior, J.; Pasquet, A.; Vancraeynest, D.; Pouleur, A.-C.; Vanoverschelde, J.-L.J.; et al. Histological validation of measurement of diffuse interstitial myocardial fibrosis by myocardial extravascular volume fraction from Modified Look-Locker imaging (MOLLI) T1 mapping at 3T. J. Cardiovasc. Magn. Reson. 2015, 17, 48. [Google Scholar] [CrossRef]
- Maltes, S.; Abecasis, J.; Pinto, D.G.; Santos, R.R.; Oliveira, L.; Mendes, G.S.; Guerreiro, S.; Lima, T.; Freitas, P.; Ferreira, A.; et al. Histology-verified myocardial fibrosis and quantification in severe As patient: Correlation with non-invasive LV myocardial tissue assessment. Eur. Heart J. 2022, 43 (Suppl. S2), ehac544.2996. [Google Scholar] [CrossRef]
- Nathan, M.; Ying, L.C.; Pierre, C.; David, B.; João, L. Assessment of myocardial fibrosis with cardiac magnetic resonance. J. Am. Coll. Cardiol. 2011, 57, 891–903. [Google Scholar]
- Mahmod, M.; Francis, J.M.; Pal, N.; Lewis, A.; Dass, S.; De Silva, R.; Petrou, M.; Sayeed, R.; Westaby, S.; Robson, M.D.; et al. Myocardial perfusion and oxygenation are impaired during stress in severe aortic stenosis and correlate with impaired energetics and subclinical left ventricular dysfunction. J. Cardiovasc. Magn. Reson. 2014, 16, 29. [Google Scholar] [CrossRef] [PubMed]
- Steadman, C.D.; Jerosch-Herold, M.; Grundy, B.; Rafelt, S.; Ng, L.L.; Squire, I.B.; Samani, N.J.; McCann, G.P. Determinants and Functional Significance of Myocardial Perfusion Reserve in Severe Aortic Stenosis. JACC Cardiovasc. Imaging 2012, 5, 182–189. [Google Scholar] [CrossRef] [PubMed]
- Podlesnikar, T.; Delgado, V.; Bax, J.J. Cardiovascular magnetic resonance imaging to assess myocardial fibrosis in valvular heart disease. Int. J. Cardiovasc. Imaging 2018, 34, 97–112. [Google Scholar] [CrossRef] [PubMed]
- Grainger, D.J.; Mosedale, D.E.; Metcalfe, J.C. TGF-β in blood: A complex problem. Cytokine Growth Factor Rev. 2000, 11, 133–145. [Google Scholar] [CrossRef]
- Ding, Y.; Wang, Y.; Zhang, W.; Jia, Q.; Wang, X.; Li, Y.; Lv, S.; Zhang, J. Roles of biomarkers in myocardial fibrosis. Aging Dis. 2020, 11, 1157–1174. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Parameter | Total Cohort (n = 21) | Low T1 (n = 10) | High T1 (n = 11) | p Value |
|---|---|---|---|---|
| Age (years) | 60 ± 11 | 63 ± 12 | 57 ± 10 | p = 0.21 |
| Sex | ||||
| Female n (%) | 13 (62) | 8 (80) | 5 (45) | p = 0.10 |
| Male n (%) | 8 (38) | 2 (20) | 6 (55) | p = 0.10 |
| Chest pain n (%) | 11 (52) | 5 (50) | 6 (55) | p > 0.99 |
| Dyspnoea n (%) | 20 (95) | 9 (90) | 11 (100) | p = 0.28 |
| Orthopnoea n (%) | 9 (43) | 4 (40) | 5 (45) | p = 0.80 |
| Pre-syncope n (%) | 7 (33) | 4 (40) | 3 (27) | p = 0.54 |
| Syncope n (%) | 6 (29) | 3 (30) | 3 (27) | p = 0.89 |
| Fatigue n (%) | 14 (67) | 8 (80) | 6 (55) | p = 0.22 |
| Hypertension n (%) | 13 (62) | 8 (80) | 5 (45) | p = 0.10 |
| Diabetes mellitus n (%) | 6 (29) | 2 (20) | 4 (36) | p = 0.41 |
| Dyslipidaemia n (%) | 9 (43) | 4 (40) | 5 (45) | p = 0.80 |
| Smoking status | ||||
| Current use n (%) | 4 (19) | 2 (20) | 2 (18) | p = 0.92 |
| Past user n (%) | 2 (10) | 2 (20) | 0 (0) | p = 0.14 |
| Heart failure n (%) | 9 (43) | 3 (30) | 6 (55) | p = 0.26 |
| Heart rate (beats per minute) | 75 ± 15 | 72 ± 15 | 77 ± 15 | p = 0.49 |
| Resting SBP (mmHg) | 128 ± 20 | 128 ± 16 | 128 ± 23 | p = 0.99 |
| Resting DBP (mmHg) | 75 ± 13 | 75 ± 15 | 75 ± 11 | p = 0.90 |
| Body mass index (kg/m2) | 29.07 ± 6.08 | 29.38 ± 6.56 | 28.79 ± 5.91 | p = 0.83 |
| Mean AVA (cm2) | 0.65 ± 0.21 | 0.58 ± 0.13 | 0.72 ± 0.26 | p = 0.15 |
| Mean gradient (mmHg) | 50 (41–56) | 53 (46–57) | 45 (40–53) | p = 0.13 |
| Peak gradient (mmHg) | 75 (66–90) | 83 (72–92) | 72 (59–96) | p = 0.40 |
| Parameter | Total Cohort (n = 21) | Low T1 (n = 10) | High T1 (n = 11) | p Value |
|---|---|---|---|---|
| Global native T1 time (ms) | 1040 ± 24 | 1023 ± 16 | 1056 ± 18 | p < 0.01 |
| LVEDV (mL) | 173.8 (138.5–229.2) | 156.8 ± 40.9 | 228.0 ± 79.4 | p = 0.02 |
| LVEDVi (mL/m2) | 95.6 (69.1–121.7) | 83.2 ± 29.6 | 116.8 ± 39.5 | p = 0.04 |
| LVESV (mL) | 80.0 (61.3–159.1) | 75.7 ± 35.1 | 151.0 ± 83.5 | p = 0.02 |
| LVESVi (mL/m2) | 44.0 (28.7–93.1) | 36.9 (26.1–46.6) | 73.6 (33.2–124.8) | p = 0.05 |
| LVSV (mL) | 78.9 ± 26.3 | 81.1 ± 29.6 | 77.0 ± 24.1 | p = 0.73 |
| LVSVi (mL/m2) | 40.5 ± 12.9 | 41.0 (30.8–51.6) | 33.8 (28.5–54.4) | p = 0.70 |
| LVM (g) | 154.5 ± 48.6 | 128.8 ± 32.8 | 177.9 ± 50.0 | p = 0.02 |
| LVMi (g/m2) | 79.4 ± 23.1 | 67.0 ± 16.9 | 91.0 ± 22.8 | p = 0.01 |
| M/V | 0.8 ± 0.2 | 0.8 ± 0.2 | 0.8 ± 0.2 | p = 0.99 |
| LVEF (%) | 41 (30–60) | 55 (38–69) | 30 (21–56) | p = 0.04 |
| MAPSE | 7 ± 4 | 9 ± 4 | 6 ± 3 | p = 0.14 |
| ESWS (×103 dynes/cm2) | 210.4 ± 105.7 | 196.5 ± 94.8 | 223.1 ± 117.9 | p = 0.57 |
| LVGFI | 28.4 ± 11.1 | 33.9 ± 9.0 | 23.4 ± 10.7 | p = 0.02 |
| LV phenotype * | ||||
| Normal | 12 (57) | 9 (90) | 3 (27) | p = 0.004 |
| Concentric hypertrophy | 1 (5) | 0 (0) | 1 (9) | p = 0.33 |
| Decompensation | 8 (38) | 1 (10) | 7 (64) | p = 0.01 |
| Global T2 time (ms) | 48 ± 2 | 49 ± 2 | 48 ± 2 | p = 0.30 |
| ECV (%) | 25 ± 3 | 24 ± 3 | 26 ± 3 | p = 0.07 |
| LGE mass (g) (visual) | 3.2 (0.1–5.2) | 3.0 (0.1–5.1) | 3.2 (0.1–5.9) | p = 0.99 |
| LGE % (visual) | 3.5 (0.1–6.3) | 3.9 (0.1–7.9) | 3.5 (0.1–5.1) | p = 0.56 |
| LGE mass (g) (3SD) | 10.7 (5.2–14.2) | 11.5 (5.9–13.1) | 7.2 (4.7–20.7) | p = 0.76 |
| LGE % (3SD) | 11.0 (6.6–19.2) | 13.2 (9.9–21.6) | 7.7 (4.9–18.9) | p = 0.17 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rajah, M.R.; Marais, E.; Maarman, G.J.; Doubell, E.; Doubell, A.F.; Herbst, P.G. Utility of Serum Biomarkers of Myocardial Fibrosis in High-Gradient Severe Aortic Stenosis: An Explorative Cardiovascular Magnetic Resonance Imaging-Based Study. Diagnostics 2025, 15, 1143. https://doi.org/10.3390/diagnostics15091143
Rajah MR, Marais E, Maarman GJ, Doubell E, Doubell AF, Herbst PG. Utility of Serum Biomarkers of Myocardial Fibrosis in High-Gradient Severe Aortic Stenosis: An Explorative Cardiovascular Magnetic Resonance Imaging-Based Study. Diagnostics. 2025; 15(9):1143. https://doi.org/10.3390/diagnostics15091143
Chicago/Turabian StyleRajah, Megan R., Erna Marais, Gerald J. Maarman, Emma Doubell, Anton F. Doubell, and Philip G. Herbst. 2025. "Utility of Serum Biomarkers of Myocardial Fibrosis in High-Gradient Severe Aortic Stenosis: An Explorative Cardiovascular Magnetic Resonance Imaging-Based Study" Diagnostics 15, no. 9: 1143. https://doi.org/10.3390/diagnostics15091143
APA StyleRajah, M. R., Marais, E., Maarman, G. J., Doubell, E., Doubell, A. F., & Herbst, P. G. (2025). Utility of Serum Biomarkers of Myocardial Fibrosis in High-Gradient Severe Aortic Stenosis: An Explorative Cardiovascular Magnetic Resonance Imaging-Based Study. Diagnostics, 15(9), 1143. https://doi.org/10.3390/diagnostics15091143