
Analyzing Insights of Super-Response in Cardiac Resynchronization Therapy with Fusion Pacing

 ,
,  ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Study Population
2.2. Inclusion Criteria
2.3. Exclusion Criteria
2.4. Device Programming in F-CRT
2.5. Criteria for Response and Study Groups
2.6. Echocardiographic Assessment
2.7. Statistical Analysis
3. Results
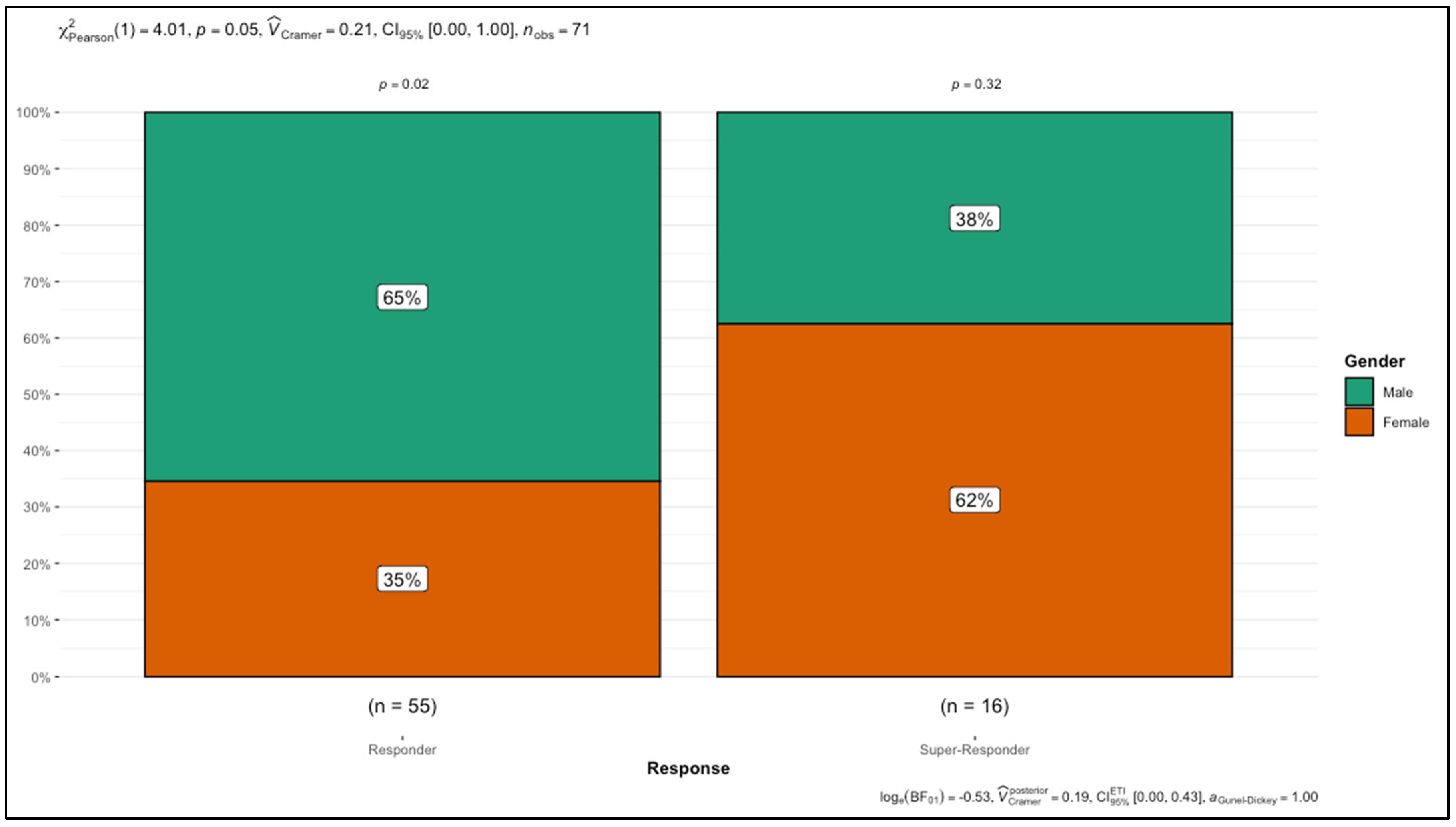
3.1. Baseline Characteristics of Fusion-CRT in Non-Super-Responders and Super-Responders
3.1.1. Baseline Clinical Characteristics, Comorbidities, and Follow-Up
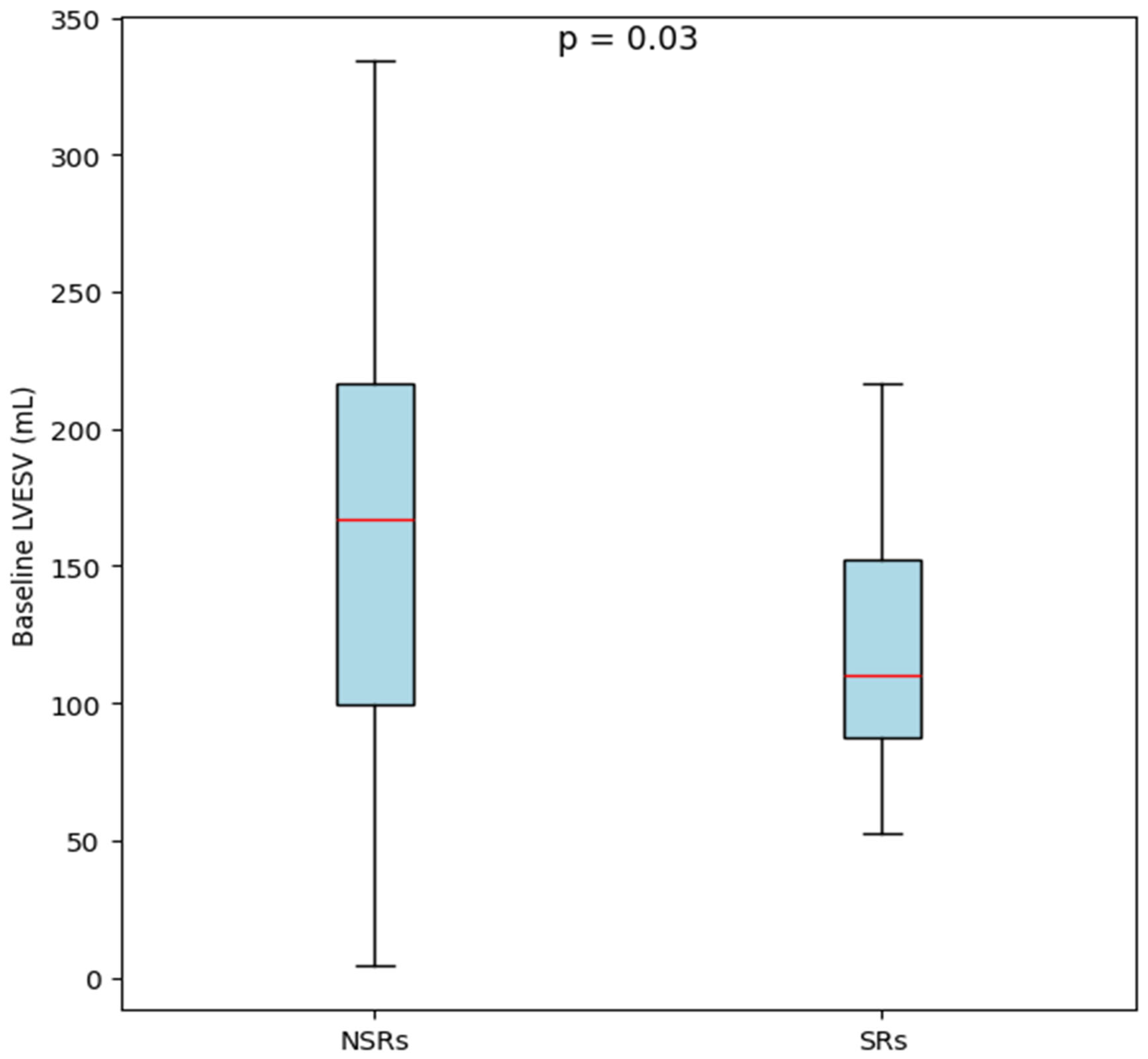
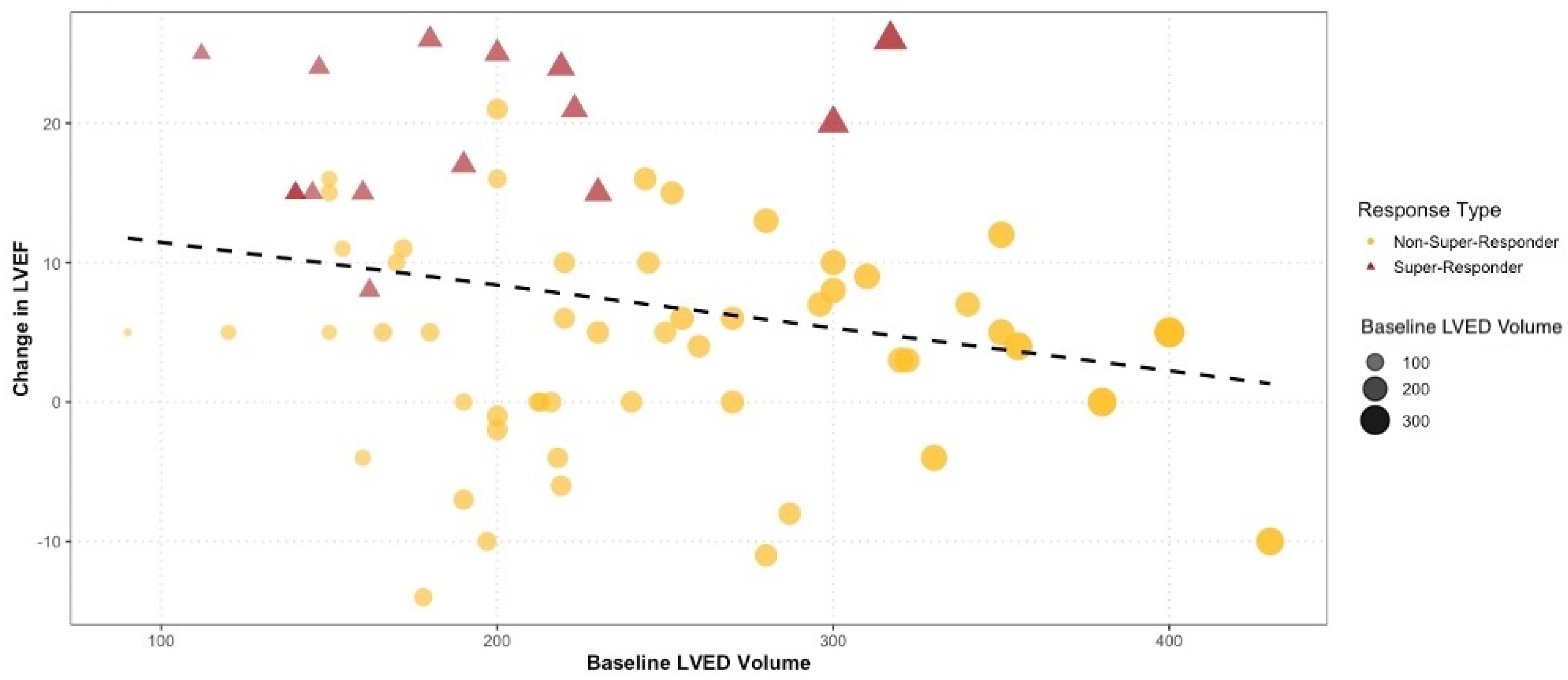
3.1.2. Baseline Echocardiographic Parameters
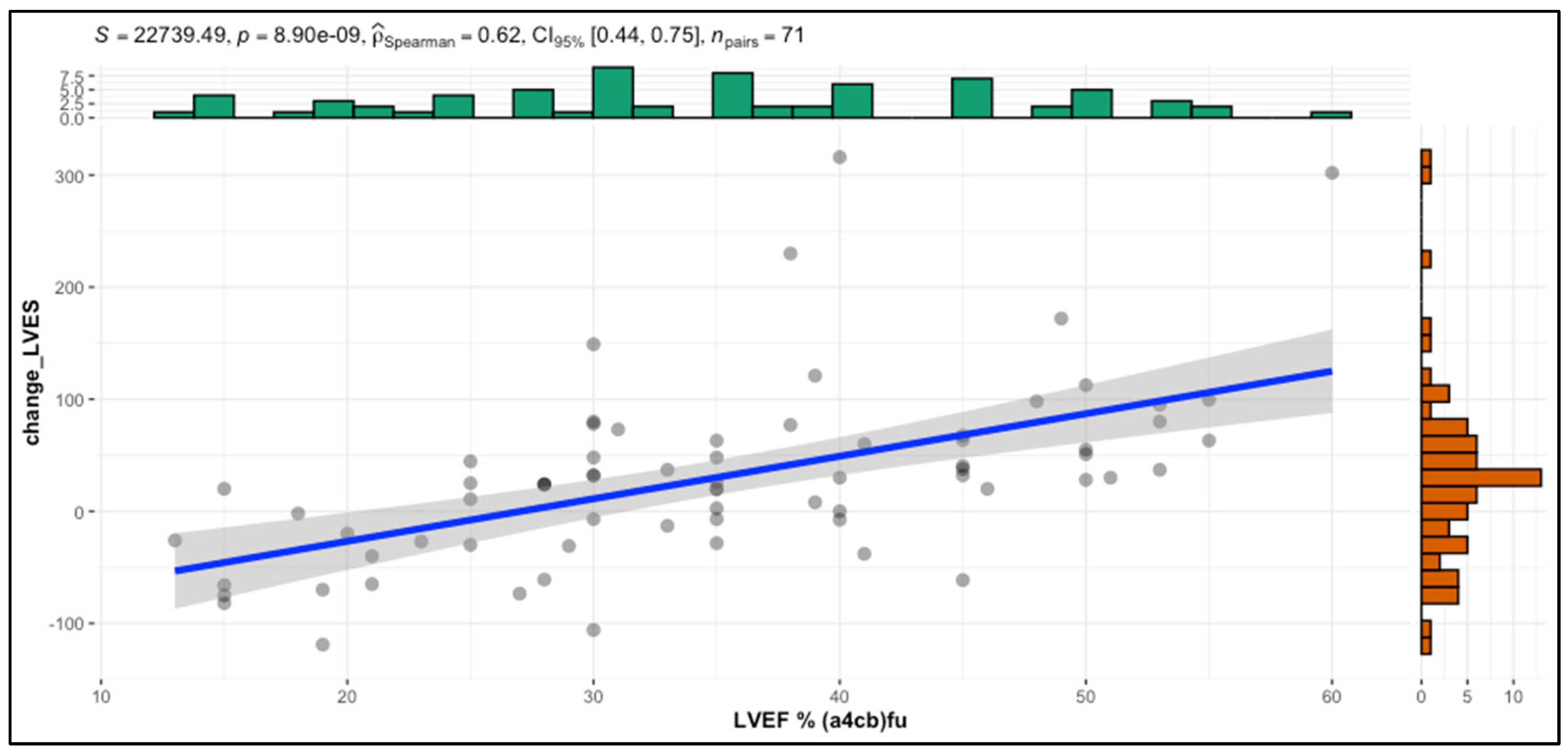
3.2. Correlation Analysis of Structural, Functional, and Electrical Parameters in f-CRT Outcomes
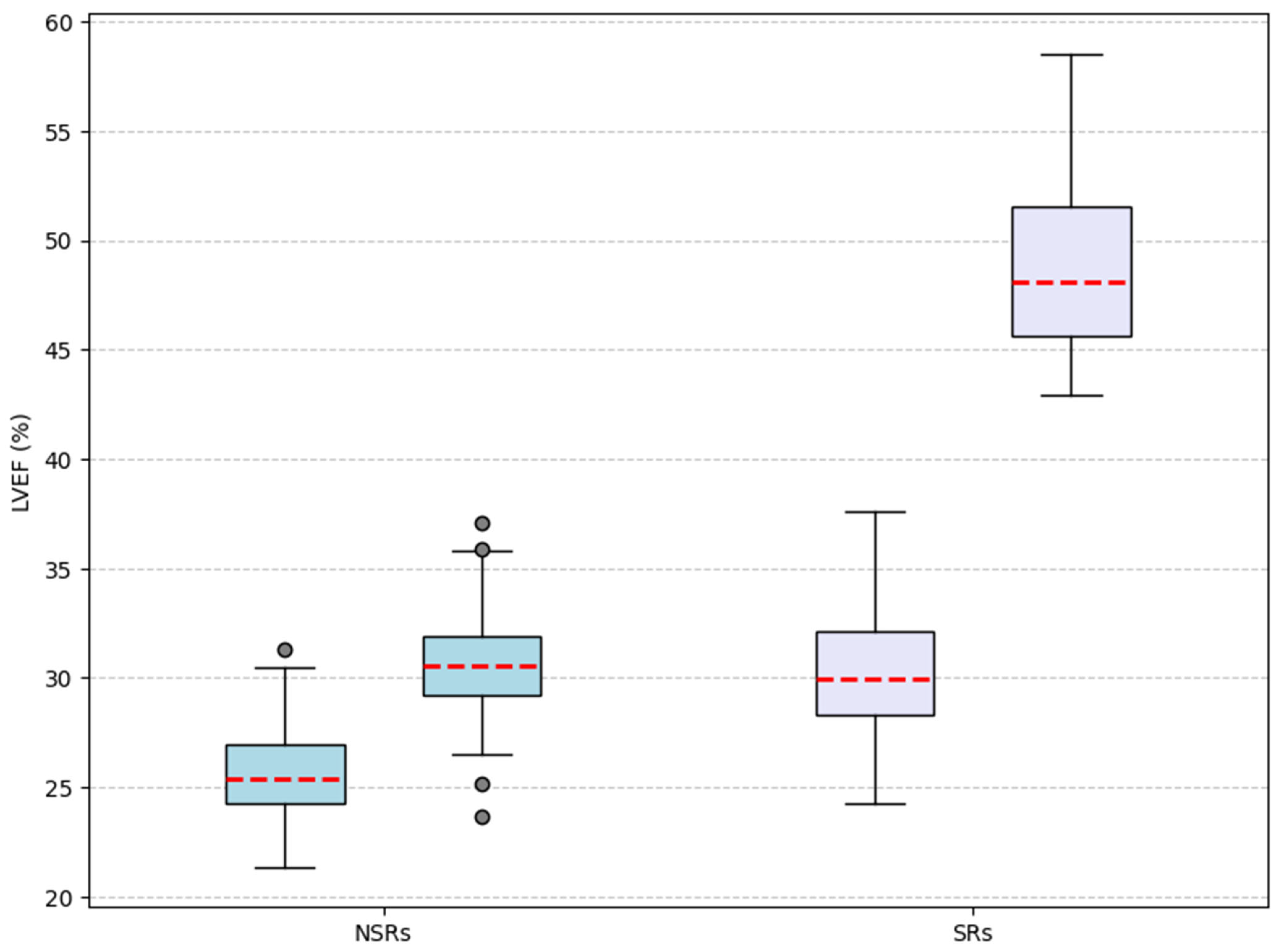
3.3. Longitudinal Analysis of Structural and Functional Changes After Fusion-CRT
3.4. Univariate Logistic Regression Analysis of Predictors for the Super-Responder Status
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A
References
- Auricchio, A.; Stellbrink, C.; Block, M.; Sack, S.; Vogt, J.; Bakker, P.; Klein, H.; Kramer, A.; Ding, J.; Salo, R.; et al. Effect of Pacing Chamber and Atrioventricular Delay on Acute Systolic Function of Paced Patients with Congestive Heart Failure. Circulation 1999, 99, 2993–3001. [Google Scholar] [CrossRef] [PubMed]
- Blanc, J.-J.; Bertault-Valls, V.; Fatemi, M.; Gilard, M.; Pennec, P.-Y.; Etienne, Y. Midterm Benefits of Left Univentricular Pacing in Patients With Congestive Heart Failure. Circulation 2004, 109, 1741–1744. [Google Scholar] [CrossRef] [PubMed]
- Vatasescu, R.; Berruezo, A.; Mont, L.; Tamborero, D.; Sitges, M.; Silva, E.; Tolosana, J.M.; Vidal, B.; Andreu, D.; Brugada, J. Midterm “super-Response” to Cardiac Resynchronization Therapy by Biventricular Pacing with Fusion: Insights from Electro-Anatomical Mapping. Europace 2009, 11, 1675–1682. [Google Scholar] [CrossRef] [PubMed]
- Van Gelder, B.M.; Bracke, F.A.; Meijer, A.; Pijls, N.H.J. The Hemodynamic Effect of Intrinsic Conduction During Left Ventricular Pacing as Compared to Biventricular Pacing. J. Am. Coll. Cardiol. 2005, 46, 2305–2310. [Google Scholar] [CrossRef]
- Lumens, J.; Ploux, S.; Strik, M.; Gorcsan, J.; Cochet, H.; Derval, N.; Strom, M.; Ramanathan, C.; Ritter, P.; Haïssaguerre, M.; et al. Comparative Electromechanical and Hemodynamic Effects of Left Ventricular and Biventricular Pacing in Dyssynchronous Heart Failure. J. Am. Coll. Cardiol. 2013, 62, 2395–2403. [Google Scholar] [CrossRef]
- Blanc, J.J.; Etienne, Y.; Gilard, M.; Mansourati, J.; Munier, S.; Boschat, J.; Benditt, D.G.; Lurie, K.G. Evaluation of Different Ventricular Pacing Sites in Patients with Severe Heart Failure: Results of an Acute Hemodynamic Study. Circulation 1997, 96, 3273–3277. [Google Scholar] [CrossRef]
- Etienne, Y.; Mansourati, J.; Gilard, M.; Valls-Bertault, V.; Boschat, J.; Benditt, D.G.; Lurie, K.G.; Blanc, J.J. Evaluation of Left Ventricular Based Pacing in Patients with Congestive Heart Failure and Atrial Fibrillation. Am. J. Cardiol. 1999, 83, 1138–1140. [Google Scholar] [CrossRef]
- Thibault, B.; Ducharme, A.; Harel, F.; White, M.; O’Meara, E.; Guertin, M.-C.; Lavoie, J.; Frasure-Smith, N.; Dubuc, M.; Guerra, P.; et al. Left Ventricular Versus Simultaneous Biventricular Pacing in Patients With Heart Failure and a QRS Complex ≥120 Milliseconds. Circulation 2011, 124, 2874–2881. [Google Scholar] [CrossRef]
- Gasparini, M.; Bocchiardo, M.; Lunati, M.; Ravazzi, P.A.; Santini, M.; Zardini, M.; Signorelli, S.; Passardi, M.; Klersy, C.; BELIEVE Investigators. Comparison of 1-Year Effects of Left Ventricular and Biventricular Pacing in Patients with Heart Failure Who Have Ventricular Arrhythmias and Left Bundle-Branch Block: The Bi vs Left Ventricular Pacing: An International Pilot Evaluation on Heart Failure Patients with Ventricular Arrhythmias (BELIEVE) Multicenter Prospective Randomized Pilot Study. Am. Heart J. 2006, 152, 155.e1–155.e7. [Google Scholar] [CrossRef]
- Boriani, G.; Kranig, W.; Donal, E.; Calo, L.; Casella, M.; Delarche, N.; Lozano, I.F.; Ansalone, G.; Biffi, M.; Boulogne, E.; et al. A Randomized Double-Blind Comparison of Biventricular versus Left Ventricular Stimulation for Cardiac Resynchronization Therapy: The Biventricular versus Left Univentricular Pacing with ICD Back-up in Heart Failure Patients (B-LEFT HF) Trial. Am. Heart J. 2010, 159, 1052–1058.e1. [Google Scholar] [CrossRef]
- Leclercq, C.; Faris, O.; Tunin, R.; Johnson, J.; Kato, R.; Evans, F.; Spinelli, J.; Halperin, H.; McVeigh, E.; Kass, D.A. Systolic Improvement and Mechanical Resynchronization Does Not Require Electrical Synchrony in the Dilated Failing Heart with Left Bundle-Branch Block. Circulation 2002, 106, 1760–1763. [Google Scholar] [CrossRef] [PubMed]
- Skaf, S.; Thibault, B.; Khairy, P.; O’Meara, E.; Fortier, A.; Vakulenko, H.V.; Pitre, C.; White, M.; Ducharme, A. Impact of Left Ventricular vs Biventricular Pacing on Reverse Remodelling: Insights From the Evaluation of Resynchronization Therapy for Heart Failure (EARTH) Trial. Can. J. Cardiol. 2017, 33, 1274–1282. [Google Scholar] [CrossRef] [PubMed]
- Gianfranchi, L.; Bettiol, K.; Sassone, B.; Verlato, R.; Corbucci, G.; Alboni, P. Fusion Beat in Patients with Heart Failure Treated with Left Ventricular Pacing: May ECG Morphology Relate to Mechanical Synchrony? A Pilot Study. Cardiovasc. Ultrasound 2008, 6, 1. [Google Scholar] [CrossRef] [PubMed]
- Pestrea, C.; Rusu, M.; Enache, R.; Cicala, E.; Gavrilescu, R.; Vaduva, A.; Ortan, F.; Iorgulescu, C.; Vatasescu, R. Feasibility of Conduction System Pacing in Patients with Baseline Bundle Branch Block—A Single-Center Mid-Term Follow-Up Study. J. Clin. Med. 2024, 13, 454. [Google Scholar] [CrossRef]
- Antonio, N.; Teixeira, R.; Coelho, L.; Lourenco, C.; Monteiro, P.; Ventura, M.; Cristovao, J.; Elvas, L.; Goncalves, L.; Providencia, L.A. Identification of “super-Responders” to Cardiac Resynchronization Therapy: The Importance of Symptom Duration and Left Ventricular Geometry. Europace 2009, 11, 343–349. [Google Scholar] [CrossRef]
- Hsu, J.C.; Solomon, S.D.; Bourgoun, M.; McNitt, S.; Goldenberg, I.; Klein, H.; Moss, A.J.; Foster, E. Predictors of Super-Response to Cardiac Resynchronization Therapy and Associated Improvement in Clinical Outcome. J. Am. Coll. Cardiol. 2012, 59, 2366–2373. [Google Scholar] [CrossRef]
- Goanță, E.-V.; Luca, C.-T.; Vacarescu, C.; Crișan, S.; Petrescu, L.; Vatasescu, R.; Lazăr, M.-A.; Gurgu, A.; Turi, V.-R.; Cozma, D. Nonischemic Super-Responders in Fusion CRT Pacing with Normal Atrioventricular Conduction. Diagnostics 2022, 12, 2032. [Google Scholar] [CrossRef]
- Auricchio, A.; Stellbrink, C.; Butter, C.; Sack, S.; Vogt, J.; Misier, A.R.; Böcker, D.; Block, M.; Kirkels, J.H.; Kramer, A.; et al. Clinical Efficacy of Cardiac Resynchronization Therapy Using Left Ventricular Pacing in Heart Failure Patients Stratified by Severity of Ventricular Conduction Delay. J. Am. Coll. Cardiol. 2003, 42, 2109–2116. [Google Scholar] [CrossRef]
- Leitz, P.; Köbe, J.; Rath, B.; Reinke, F.; Frommeyer, G.; Andresen, C.; Güner, F.; Wolfes, J.; Lange, P.S.; Ellermann, C.; et al. Very Long-Term Follow-Up in Cardiac Resynchronization Therapy: Wider Paced QRS Equals Worse Prognosis. J. Pers. Med. 2021, 11, 1176. [Google Scholar] [CrossRef]
- Ypenburg, C.; Van Bommel, R.J.; Borleffs, C.J.W.; Bleeker, G.B.; Boersma, E.; Schalij, M.J.; Bax, J.J. Long-Term Prognosis After Cardiac Resynchronization Therapy Is Related to the Extent of Left Ventricular Reverse Remodeling at Midterm Follow-Up. J. Am. Coll. Cardiol. 2009, 53, 483–490. [Google Scholar] [CrossRef]
- Castellant, P.; Fatemi, M.; Bertault-Valls, V.; Etienne, Y.; Blanc, J.-J. Cardiac Resynchronization Therapy: “Nonresponders” and “Hyperresponders”. Heart Rhythm 2008, 5, 193–197. [Google Scholar] [CrossRef] [PubMed]
- Jin, H.; Gu, M.; Hua, W.; Fan, X.-H.; Niu, H.-X.; Ding, L.-G.; Wang, J.; Xue, C.; Zhang, S. Predictors of Super-Response to Cardiac Resynchronization Therapy: The Significance of Heart Failure Medication, Pre-Implant Left Ventricular Geometry and High Percentage of Biventricular Pacing. J. Geriatr. Cardiol. JGC 2017, 14, 737–742. [Google Scholar] [CrossRef]
- Patel, D.; Trulock, K.M.; Moennich, L.A.; Kiehl, E.L.; Kumar, A.; Toro, S.; Donnellan, E.; Grimaldi, A.; Baranowski, B.; Hussein, A.A.; et al. Predictors of Long-term Outcomes Greater than 10 Years after Cardiac Resynchronization Therapy Implantation. J. Cardiovasc. Electrophysiol. 2020, 31, 1182–1186. [Google Scholar] [CrossRef]
- Rickard, J.; Kumbhani, D.J.; Popovic, Z.; Verhaert, D.; Manne, M.; Sraow, D.; Baranowski, B.; Martin, D.O.; Lindsay, B.D.; Grimm, R.A.; et al. Characterization of Super-Response to Cardiac Resynchronization Therapy. Heart Rhythm 2010, 7, 885–889. [Google Scholar] [CrossRef] [PubMed]
- Galloo, X.; Khidir, M.; Stassen, J.; Hirasawa, K.; Cosyns, B.; Van Der Bijl, P.; Delgado, V.; Ajmone Marsan, N.; Bax, J.J. Risk Factors for Short-Term Versus Long-Term Mortality in Patients Who Underwent Cardiac Resynchronization Therapy. Am. J. Cardiol. 2023, 197, 34–41. [Google Scholar] [CrossRef]
- Vătășescu, R.G.; Târtea, G.C.; Iorgulescu, C.; Cojocaru, C.; Deaconu, A.; Badiul, A.; Goanță, E.-V.; Bogdan, Ștefan; Cozma, D. Predictors for Super-Responders in Cardiac Resynchronization Therapy. Am. J. Ther. 2023, 31, e13–e23. [Google Scholar] [CrossRef]
- Arshad, A.; Moss, A.J.; Foster, E.; Padeletti, L.; Barsheshet, A.; Goldenberg, I.; Greenberg, H.; Hall, W.J.; McNitt, S.; Zareba, W.; et al. Cardiac Resynchronization Therapy Is More Effective in Women Than in Men. J. Am. Coll. Cardiol. 2011, 57, 813–820. [Google Scholar] [CrossRef] [PubMed]
- Varma, N.; Mittal, S.; Prillinger, J.B.; Snell, J.; Dalal, N.; Piccini, J.P. Survival in Women Versus Men Following Implantation of Pacemakers, Defibrillators, and Cardiac Resynchronization Therapy Devices in a Large, Nationwide Cohort. J. Am. Heart Assoc. 2017, 6, e005031. [Google Scholar] [CrossRef]
- Pujol-López, M.; Tolosana, J.M.; Guasch, E.; Trucco, E.; Jiménez-Arjona, R.; Borràs, R.; Garre, P.; San Antonio, R.; Doltra, A.; Roca-Luque, I.; et al. Cardiac Resynchronization Therapy Response Is Equalized in Men and Women by Electrical Optimization. JACC Clin. Electrophysiol. 2021, 7, 1400–1409. [Google Scholar] [CrossRef]
- Arbelo, E.; Tolosana, J.M.; Trucco, E.; Penela, D.; Borràs, R.; Doltra, A.; Andreu, D.; Aceña, M.; Berruezo, A.; Sitges, M.; et al. Fusion-Optimized Intervals (FOI): A New Method to Achieve the Narrowest QRS for Optimization of the AV and VV Intervals in Patients Undergoing Cardiac Resynchronization Therapy. J. Cardiovasc. Electrophysiol. 2014, 25, 283–292. [Google Scholar] [CrossRef]
- Trucco, E.; Tolosana, J.M.; Arbelo, E.; Doltra, A.; Castel, M.Á.; Benito, E.; Borràs, R.; Guasch, E.; Vidorreta, S.; Vidal, B.; et al. Improvement of Reverse Remodeling Using Electrocardiogram Fusion-Optimized Intervals in Cardiac Resynchronization Therapy. JACC Clin. Electrophysiol. 2018, 4, 181–189. [Google Scholar] [CrossRef] [PubMed]
- Moss, A.J.; Hall, W.J.; Cannom, D.S.; Klein, H.; Brown, M.W.; Daubert, J.P.; Estes, N.A.M.; Foster, E.; Greenberg, H.; Higgins, S.L.; et al. Cardiac-Resynchronization Therapy for the Prevention of Heart-Failure Events. N. Engl. J. Med. 2009, 361, 1329–1338. [Google Scholar] [CrossRef] [PubMed]
- Giamouzis, G.; Kalogeropoulos, A.P.; Butler, J.; Karayannis, G.; Georgiopoulou, V.V.; Skoularigis, J.; Triposkiadis, F. Epidemiology and Importance of Renal Dysfunction in Heart Failure Patients. Curr. Heart Fail. Rep. 2013, 10, 411–420. [Google Scholar] [CrossRef]
- Dries, D.L.; Exner, D.V.; Domanski, M.J.; Greenberg, B.; Stevenson, L.W. The Prognostic Implications of Renal Insufficiency in Asymptomatic and Symptomatic Patients with Left Ventricular Systolic Dysfunction. J. Am. Coll. Cardiol. 2000, 35, 681–689. [Google Scholar] [CrossRef] [PubMed]
- Boerrigter, G.; Costello-Boerrigter, L.C.; Abraham, W.T.; St. John Sutton, M.G.; Heublein, D.M.; Kruger, K.M.; Hill, M.R.S.; McCullough, P.A.; Burnett, J.C. Cardiac Resynchronization Therapy Improves Renal Function in Human Heart Failure With Reduced Glomerular Filtration Rate. J. Card. Fail. 2008, 14, 539–546. [Google Scholar] [CrossRef]
- Van Bommel, R.J.; Mollema, S.A.; Borleffs, C.J.W.; Bertini, M.; Ypenburg, C.; Marsan, N.A.; Delgado, V.; Van Der Wall, E.E.; Schalij, M.J.; Bax, J.J. Impaired Renal Function Is Associated With Echocardiographic Nonresponse and Poor Prognosis After Cardiac Resynchronization Therapy. J. Am. Coll. Cardiol. 2011, 57, 549–555. [Google Scholar] [CrossRef]
- Filippatos, G.; Farmakis, D.; Parissis, J. Renal Dysfunction and Heart Failure: Things Are Seldom What They Seem. Eur. Heart J. 2014, 35, 416–418. [Google Scholar] [CrossRef]
- Moreira, R.I.; Cunha, P.S.; Rio, P.; Da Silva, M.N.; Branco, L.M.; Galrinho, A.; Feliciano, J.; Soares, R.; Ferreira, R.C.; Oliveira, M.M. Response and Outcomes of Cardiac Resynchronization Therapy in Patients with Renal Dysfunction. J. Interv. Card. Electrophysiol. 2018, 51, 237–244. [Google Scholar] [CrossRef]
- Kutyifa, V.; Kloppe, A.; Zareba, W.; Solomon, S.D.; McNitt, S.; Polonsky, S.; Barsheshet, A.; Merkely, B.; Lemke, B.; Nagy, V.K.; et al. The Influence of Left Ventricular Ejection Fraction on the Effectiveness of Cardiac Resynchronization Therapy. J. Am. Coll. Cardiol. 2013, 61, 936–944. [Google Scholar] [CrossRef]
- Bytyçi, I.; Bajraktari, G.; Henein, M. Left Atrial Volume Index Predicts Response to Cardiac Resynchronisation Therapy: A Systematic Review and Meta-Analysis. Arch. Med. Sci. 2020, 18, 930. [Google Scholar] [CrossRef]
- Stassen, J.; Galloo, X.; Chimed, S.; Hirasawa, K.; Marsan, N.A.; Delgado, V.; Van Der Bijl, P.; Bax, J.J. Clinical Implications of Left Atrial Reverse Remodelling after Cardiac Resynchronization Therapy. Eur. Heart J.-Cardiovasc. Imaging 2022, 23, 730–740. [Google Scholar] [CrossRef] [PubMed]
- Valzania, C.; Gadler, F.; Boriani, G.; Rapezzi, C.; Eriksson, M.J. Effect of Cardiac Resynchronization Therapy on Left Atrial Size and Function as Expressed by Speckle Tracking 2-Dimensional Strain. Am. J. Cardiol. 2016, 118, 237–243. [Google Scholar] [CrossRef] [PubMed]
- Donal, E.; Tan, K.; Leclercq, C.; Ollivier, R.; Derumeaux, G.; Bernard, M.; De Place, C.; Mabo, P.; Daubert, J.-C. Left Atrial Reverse Remodeling and Cardiac Resynchronization Therapy for Chronic Heart Failure Patients in Sinus Rhythm. J. Am. Soc. Echocardiogr. 2009, 22, 1152–1158. [Google Scholar] [CrossRef]
- Stassen, J.; Galloo, X.; Hirasawa, K.; Van Der Bijl, P.; Leon, M.B.; Marsan, N.A.; Bax, J.J. Interaction between Secondary Mitral Regurgitation and Left Atrial Function and Their Prognostic Implications after Cardiac Resynchronization Therapy. Eur. Heart J.-Cardiovasc. Imaging 2023, 24, 532–541. [Google Scholar] [CrossRef]
- Dokuni, K.; Matsumoto, K.; Tatsumi, K.; Suto, M.; Tanaka, H.; Fukuzawa, K.; Hirata, K.-I. Cardiac Resynchronization Therapy Improves Left Atrial Reservoir Function through Resynchronization of the Left Atrium in Patients with Heart Failure with Reduced Ejection Fraction. Int. J. Cardiovasc. Imaging 2020, 36, 1203–1212. [Google Scholar] [CrossRef] [PubMed]
- Stassen, J.; Galloo, X.; Hirasawa, K.; Marsan, N.A.; Van Der Bijl, P.; Delgado, V.; Bax, J.J. Tricuspid Regurgitation after Cardiac Resynchronization Therapy: Evolution and Prognostic Significance. EP Eur. 2022, 24, 1291–1299. [Google Scholar] [CrossRef]
- Sharma, A.; Lavie, C.J.; Vallakati, A.; Garg, A.; Goel, S.; Lazar, J.; Fonarow, G.C. Changes in Parameters of Right Ventricular Function with Cardiac Resynchronization Therapy. Clin. Cardiol. 2017, 40, 1033–1043. [Google Scholar] [CrossRef]
- Dawood, M.; Elsharkawy, E.; Nawar, M.; Sanhoury, M. Right Ventricular Response to Cardiac Resynchronization Therapy: A Three-Dimensional and Speckle Tracking Echocardiographic Study. Am. J. Cardiol. 2023, 205, 150–161. [Google Scholar] [CrossRef]
- Galloo, X.; Stassen, J.; Hirasawa, K.; Mertens, B.J.A.; Cosyns, B.; Van Der Bijl, P.; Delgado, V.; Ajmone Marsan, N.; Bax, J.J. Prognostic Implications of Right Ventricular Size and Function in Patients Undergoing Cardiac Resynchronization Therapy. Circ. Arrhythm. Electrophysiol. 2023, 16, e011676. [Google Scholar] [CrossRef]
- Papageorgiou, N.; Providência, R.; Lambiase, P.D.; Tousoulis, D.; Lloyd, G.; Bhattacharyya, S. Does Presence of Left Ventricular Contractile Reserve Improve Response to Cardiac Resynchronization Therapy? An Updated Meta-Analysis. Int. J. Cardiol. 2018, 252, 224–228. [Google Scholar] [CrossRef]
- St John Sutton, M.G.; Plappert, T.; Abraham, W.T.; Smith, A.L.; DeLurgio, D.B.; Leon, A.R.; Loh, E.; Kocovic, D.Z.; Fisher, W.G.; Ellestad, M.; et al. Effect of Cardiac Resynchronization Therapy on Left Ventricular Size and Function in Chronic Heart Failure. Circulation 2003, 107, 1985–1990. [Google Scholar] [CrossRef] [PubMed]
- Farhangee, A.; Davies, M.J.; Mesina, M.; Morgan, D.R.; Sieniewicz, B.J.; Meyrick, R.; Gaughan, K.; Mîndrilă, I. Comparative Analysis of Response to Cardiac Resynchronisation Therapy Upgrades in Patients with Implantable Cardioverter-Defibrillators and Pacemakers. J. Clin. Med. 2024, 13, 2755. [Google Scholar] [CrossRef] [PubMed]
- Galloo, X.; Stassen, J.; Hirasawa, K.; Chimed, S.; Cosyns, B.; Ajmone Marsan, N.; Delgado, V.; Van Der Bijl, P.; Bax, J.J. Impact of Baseline Left Ventricular Volume on Left Ventricular Reverse Remodeling after Cardiac Resynchronization Therapy. Heart Rhythm 2022, 19, 927–936. [Google Scholar] [CrossRef] [PubMed]
- Hua, J.; Chen, Y.; Yu, J.; Xiong, Q.; Xia, Z.; Xia, Z.; Huang, Q.; Kong, Q.; Chen, H.; Zhang, Y.; et al. Long-Term Outcomes of Left Bundle Branch Area Pacing versus Biventricular Pacing in Patients with Heart Failure and Complete Left Bundle Branch Block. Heart Vessel. 2022, 37, 1162–1174. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Non-Super-Responder | Super-Responder | p-Value | |
|---|---|---|---|
| Variable | N = 55 | N = 16 | |
| Baseline clinical characteristics | |||
| Age [years] | 70.0 (62.0–74.5) | 67.5 (65.0–71.5) | 0.75 |
| Sex | |||
| Male | 36 (65.45%) | 6 (37.5%) | 0.05 * |
| Female | 19 (34.55%) | 10 (62.5%) | |
| Body mass index [kg/m2] | 28.30 (25.85–32.60) | 27.90 (26.73–31.40) | 0.94 |
| Body surface area [m2] | 1.90 (1.80–2.00) | 1.80 (1.78–2.00) | 0.45 |
| QRS duration [ms] | 160.0 (150.0–168.0) | 160.0 (146.0–160.0) | 0.31 |
| Comorbidities | |||
| Arterial hypertension [yes] | 34 (61.82%) | 11 (68.75%) | 0.61 |
| Chronic kidney disease | |||
| G1 | 9 (16.36%) | 5 (31.25%) | 0.21 |
| G2 | 15 (27.27%) | 7 (43.75%) | |
| G3a | 13 (23.64%) | 3 (18.75%) | |
| G3b | 17 (30.91%) | 1 (6.25%) | |
| G4 | 1 (1.82%) | 0 (0%) | |
| Heart failure etiology | |||
| Ischemic | 6 (10.91%) | 1 (6.25%) | 0.85 |
| Non-ischemic | 9 (16.36%) | 3 (18.75%) | |
| Idiopathic | 40 (72.73%) | 12 (75%) | |
| Follow-up | |||
| Mean follow-up [months] | 43.3 | 42.9 | 0.49 |
| Non-Super-Responder | Super-Responder | p-Value | ||
|---|---|---|---|---|
| Variable | N = 55 | N = 16 | ||
| Echocardiographic data at baseline | ||||
| Interventricular septum wall diameter [cm] | 1.10 (1.00–1.25) | 1.05 (1.00–1.22) | 0.43 | |
| Left ventricle posterior wall diameter [cm] | 1.10 (1.00–1.20) | 1.15 (1.00–1.20) | 0.39 | |
| Left ventricle end-diastolic diameter [cm] | 6.80 (6.20–7.30) | 6.30 (5.30–6.73) | 0.02 * | |
| Left ventricle end-diastolic volume [mL] | 240.00 (193.50–300.00) | 185.00 (146.50–224.75) | 0.03 * | |
| Left ventricle end-systolic volume [mL] | 175.00 (130.00–231.00) | 132.50 (99.50–162.00) | 0.03 * | |
| Left ventricle ejection fraction [%] | 26 ± 6.9 | 29.4 ± 4.5 | 0.03 * | |
| Left atrium area [cm2] | 26.91 (26.45–27.00) | 25.50 (20.48–26.91) | 0.02 * | |
| Left atrium volume [mL] | 99.72 (80.50–129.00) | 78.50 (49.75–102.50) | 0.02 * | |
| Left atrium volume index [mL/m2] | 53.08 (43.90–64.85) | 44.70 (28.68–53.08) | 0.03 * | |
| E/A ratio | 1.50 (0.72–2.00) | 1.15 (0.57–1.63) | 0.4 | |
| Systolic pulmonary arterial pressure [mmHg] | 46.29 (41.50–49.00) | 46.29 (46.29–50.00) | 0.72 | |
| Mitral valve regurgitation | 0.49 | |||
| Mild | 11 (20%) | 5 (31.3%) | ||
| Moderate | 33 (60%) | 8 (50%) | ||
| Severe | 11 (20%) | 3 (18.8%) | ||
| Tricuspid valve regurgitation | 0.78 | |||
| Mild | 23 (41.8%) | 7 (43.8%) | ||
| Moderate | 30 (54.5%) | 9 (56.3%) | ||
| Severe | 2 (3.6%) | 0 | ||
| Correlation | Variable 1 | Variable 2 | ρ (rho) | p-Value |
|---|---|---|---|---|
| Correlations between baseline variables and follow-up variables | LVEF (b) | LVEF (fu) | 0.443 | <0.001 ** |
| Left ventricle end-systolic volume (b) | Left ventricle end-systolic volume (fu) | 0.603 | <0.001 ** | |
| Left atrium volume (b) | Left atrium volume (fu) | 0.640 | <0.001 ** | |
| Correlations using left ventricle ejection fraction | LVEF (fu) | Change left ventricle end-systolic volume | 0.557 | <0.001 ** |
| LVEF (fu) | Change NYHA | 0.184 | 0.125 | |
| LVEF (fu) | Left ventricle end-systolic volume (b) | −0.426 | <0.001 ** | |
| LVEF (fu) | Left ventricle end-diastolic volume (b) | −0.394 | <0.001 ** | |
| LVEF (fu) | Left atrium volume (b) | −0.374 | 0.001 ** | |
| Correlations between baseline QRS duration and left ventricle reverse-remodeling parameters | QRS duration (b) | Left ventricle end-systolic volume (fu) | −0.169 | 0.159 |
| QRS duration (b) | LEF (fu) | 0.201 | 0.093 |
| All Patients (N = 71) | p-Value | Non-Super-Responders (N = 55) | p-Value | Super-Responders (N = 16) | p-Value | ||||
|---|---|---|---|---|---|---|---|---|---|
| Variable | Baseline | Follow-Up | Baseline | Follow-Up | Baseline | Follow-Up | |||
| New York Heart Association Class | <0.001 ** | <0.001 ** | 0.007 ** | ||||||
| I | 0% | 8.5% | 0% | 7.3% | 0% | 12.5% | |||
| II | 50.7% | 59.1% | 49.1% | 54.5% | 56.3% | 75% | |||
| III | 45.1% | 23.9% | 45.5% | 27.3% | 43.8% | 12.5% | |||
| IV | 4.2% | 8.5% | 5.5% | 10.9% | 0% | 0% | |||
| Mitral valve regurgitation | 0.99 | 0.13 | 0.02 * | ||||||
| Mild | 22.5% | 29.6% | 20% | 20% | 31.3% | 62.5% | |||
| Moderate | 57.7% | 43.7% | 60% | 45.5% | 50% | 37.5% | |||
| Severe | 19.7% | 26.8% | 20% | 34.5% | 18.8% | 0% | |||
| Tricuspid valve regurgitation | 0.2 | 0.03 * | 0.15 | ||||||
| Mild | 42.3% | 42.3% | 41.8% | 34.5% | 43.8% | 68.8% | |||
| Moderate | 54.9% | 43.7% | 54.5% | 47.3% | 56.3% | 31.3% | |||
| Severe | 2.8% | 14.1% | 3.6% | 18.2% | 0% | 6.3% | |||
| All Patients (N = 71) | p-Value | Non-Super-Responders (N = 55) | p-Value | Super-Responders (N = 16) | p-Value | ||||
|---|---|---|---|---|---|---|---|---|---|
| Variable | Baseline | Follow-Up | Baseline | Follow-Up | Baseline | Follow-Up | |||
| Left Ventricle End-Diastolic Volume [mL] | 220 | 195 | 0.03 * | 240 | 219.7 | 0.8 | 185 | 117.5 | <0.001 ** |
| Left Ventricle End-Systolic Volume [mL] | 160 | 130 | 0.002 * | 175 | 162 | 0.3 | 132.5 | 65.2 | <0.001 ** |
| Left Ventricle Ejection Fraction [%] | 26.7 | 35 | <0.001 ** | 26 | 30.7 | <0.001 ** | 29.4 | 50.1 | <0.001 ** |
| Left Atrium Volume [mL] | 96 | 93 | 0.76 | 99.7 | 102 | 0.2 | 78.5 | 66.5 | 0.06 |
| Left Atrium Volume Index [mL/m2] | 52.9 | 54.7 | 0.66 | 53.1 | 54.7 | 0.3 | 44.7 | 38.4 | 0.2 |
| E/A Ratio | 1.5 | 0.8 | 0.06 | 1.5 | 1.3 | 0.2 | 1.2 | 0.7 | 0.02 * |
| Systolic Pulmonary Arterial Pressure [mmHg] | 46.3 | 39.8 | <0.001 ** | 46.3 | 39.8 | 0.005 * | 46.3 | 37.4 | 0.02 * |
| Predictors | Odds Ratios | Confidence Interval | p-Value | R2 Nagelkerke |
|---|---|---|---|---|
| Left ventricle end-diastolic diameter (b) [cm] | 0.47 | 0.23–0.86 | 0.023 * | 0.126 |
| Left atrium volume (b) [mL] | 0.97 | 0.95–0.99 | 0.015 * | 0.158 |
| Left atrium volume index(b) [mL/m2] | 0.96 | 0.92–0.99 | 0.035 * | 0.115 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lazăr-Höcher, A.-I.; Crișan, S.; Văcărescu, C.; Nistor, S.; Faur-Grigori, A.A.; Cozgarea, A.; Baneu, P.; Cirin, L.; Brăescu, L.; Dăniluc, L.; et al. Analyzing Insights of Super-Response in Cardiac Resynchronization Therapy with Fusion Pacing. Diagnostics 2025, 15, 1118. https://doi.org/10.3390/diagnostics15091118
Lazăr-Höcher A-I, Crișan S, Văcărescu C, Nistor S, Faur-Grigori AA, Cozgarea A, Baneu P, Cirin L, Brăescu L, Dăniluc L, et al. Analyzing Insights of Super-Response in Cardiac Resynchronization Therapy with Fusion Pacing. Diagnostics. 2025; 15(9):1118. https://doi.org/10.3390/diagnostics15091118
Chicago/Turabian StyleLazăr-Höcher, Alexandra-Iulia, Simina Crișan, Cristina Văcărescu, Samuel Nistor, Adelina Andreea Faur-Grigori, Andreea Cozgarea, Petru Baneu, Liviu Cirin, Laurențiu Brăescu, Larissa Dăniluc, and et al. 2025. "Analyzing Insights of Super-Response in Cardiac Resynchronization Therapy with Fusion Pacing" Diagnostics 15, no. 9: 1118. https://doi.org/10.3390/diagnostics15091118
APA StyleLazăr-Höcher, A.-I., Crișan, S., Văcărescu, C., Nistor, S., Faur-Grigori, A. A., Cozgarea, A., Baneu, P., Cirin, L., Brăescu, L., Dăniluc, L., Gaiță, D., Luca, C.-T., & Cozma, D. C. (2025). Analyzing Insights of Super-Response in Cardiac Resynchronization Therapy with Fusion Pacing. Diagnostics, 15(9), 1118. https://doi.org/10.3390/diagnostics15091118