
Advancing Colorectal Cancer Diagnostics from Barium Enema to AI-Assisted Colonoscopy

 ,
,  ,
,
Abstract
1. Introduction
2. Materials and Methods
3. Results
3.1. Epidemiology
3.2. Risk Factors
3.3. Prophylactic Factors
3.4. Diagnostic Methods
3.5. Survival
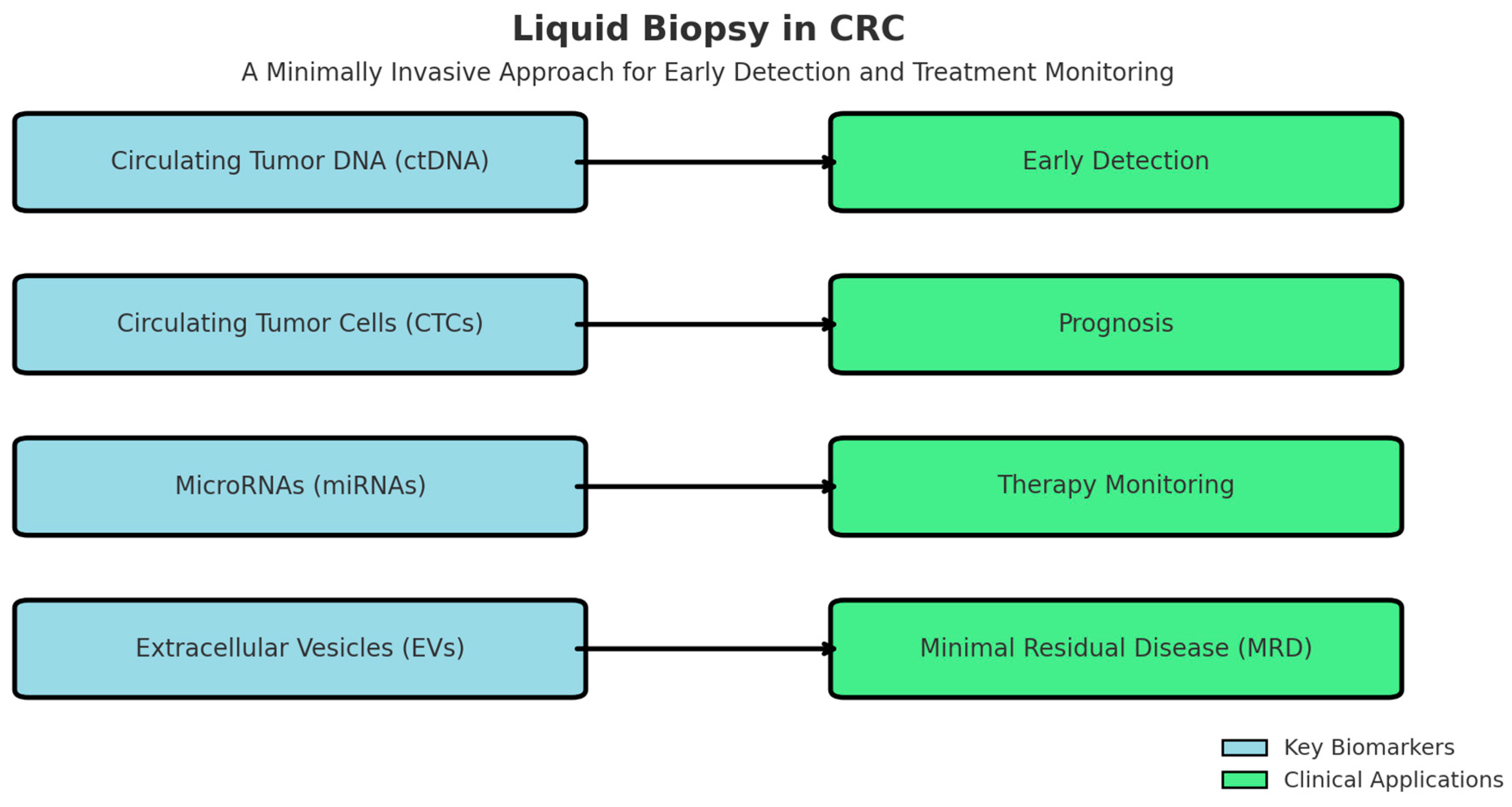
3.6. Liquid Biopsy
3.7. Ai-Assisted Imaging and Deep Learning in Colonoscopy and CRC Diagnostic
3.7.1. Uses and Benefits
3.7.2. Architecture Types
3.7.3. Public Datasets for AI in Colonoscopy
3.7.4. AI-Driven Quality Assessment Tools
4. Conclusions
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| CRC | Colorectal cancer |
| FOBT | Fecal occult blood tests |
| ADR | Adenoma detection rates |
| LD | Linear dichroism |
| EGFR | Epidermal growth factor receptor |
| FAP | Familial adenomatous polyposis |
| MMR | Mismatch repair |
| ctDNA | Circulating Tumor DNA |
| CTCs | Circulating Tumor Cells |
| miRNAs | MicroRNAs |
| EVs | Extracellular Vehicles |
| ML | Machine learning |
| DL | Deep learning |
| CADx | Computer-aided detection |
| CNNs | Convolutional neural networks |
| RNNs | Recurrent neural networks |
References
- Daley, N.E.; Rosenthal, M.B.; Ganguli, I. Safe, Then Sorry?—The Psychological Biases that Drive Care Cascades. J. Gen. Intern. Med. 2025, 2025, 1–3. [Google Scholar] [CrossRef] [PubMed]
- International Agency for Research on Cancer (IARC), Global Cancer Observatory. Colorectal Cancer Fact Sheet (GLOBOCAN 2022). Available online: https://gco.iarc.who.int/media/globocan/factsheets/populations/900-world-fact-sheet.pdf (accessed on 10 February 2025).
- Mastalier, B.; Tihon, C.; Ghiţă, B.; Botezatu, C.; Deaconescu, V.; Mandisodza, P.; Drăghici, C.; Simion, S. Surgical treatment of colon cancer: Colentina surgical clinic experience. J. Med. Life 2012, 5, 348–353. [Google Scholar] [PubMed] [PubMed Central]
- Calva, A.M.; Acevedo Tirado, M.T. Revisión y actualización general en cancer colorrectal. Rev. Radiol. México 2009, 1, 99–115. [Google Scholar]
- Wu, D.; Song, Q.Y.; Dai, B.S.; Li, J.; Wang, X.X.; Liu, J.Y.; Xie, T.Y. Colorectal cancer early screening: Dilemmas and solutions. World J. Gastroenterol. 2025, 31, 98760. [Google Scholar] [CrossRef] [PubMed]
- Lew, J.; Luo, Q.; Worthington, J.; Ge, H.; He, E.; Steinberg, J.; Caruana, M.; O’Connell, D.; Feletto, E.; Canfell, K. Recalibrating an Established Microsimulation Model to Capture Trends and Projections of Colorectal Cancer Incidence and Mortality. Med. Decis. Mak. 2025, 45, 257–275. [Google Scholar] [CrossRef]
- Rustgi, S.; Soddano, J.; Ingram, M.; Hampel, H.; Hur, C.; Kastrinos, F. Cost-Effectiveness of Lynch Syndrome Identification Strategies in Individuals with Colorectal Cancer and the Impact on At-Risk Relatives. Clin. Gastroenterol. Hepatol. 2025; in press. [Google Scholar] [CrossRef]
- Fujita, Y.; Hida, K.; Nishigori, T.; Hamasu, S.; Shiota, T.; Kan, T.; Okamura, R.; Itatani, Y.; Obama, K. Perioperative changes in the quality of life and the impact of preoperative quality of life on the time to return to work after surgery among patients with colorectal cancer: A prospective, multicenter, cohort study. Surg. Today 2025, 1–8. [Google Scholar] [CrossRef]
- Yang, Z.; Wang, X.; Zhou, H.; Jiang, M.; Wang, J.; Sui, B. Molecular Complexity of Colorectal Cancer: Pathways, Biomarkers, and Therapeutic Strategies. Cancer Manag. Res. 2024, 16, 1389–1403. [Google Scholar] [CrossRef]
- Kudryavtseva, A.V.; Lipatova, A.V.; Zaretsky, A.R.; Moskalev, A.A.; Fedorova, M.S.; Rasskazova, A.S.; Shibukhova, G.; Snezhkina, A.; Kaprin, A.; Alekseev, B. Important molecular genetic markers of colorectal cancer. Oncotarget 2016, 7, 53959. [Google Scholar] [CrossRef]
- Kanthan, R.; Senger, J.L.; Kanthan, S.C. Molecular Events in Primary and Metastatic Colorectal Carcinoma: A Review. Pathol. Res. Int. 2012, 2012, 597497. [Google Scholar] [CrossRef]
- Banias, L.; Jung, I.; Chiciudean, R.; Gurzu, S. From Dukes-MAC Staging System to Molecular Classification: Evolving Concepts in Colorectal Cancer. Int. J. Mol. Sci. 2022, 23, 9455. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Wang, H.; Li, Y.; Lei, L.; Liu, C.; Chen, W.; Dai, M.; Wang, X.; Lew, J.; Shi, J.; Li, N.; et al. Estimating the economic burden of colorectal cancer in China, 2019–2030: A population-level prevalence-based analysis. Cancer Med. 2024, 13, e6787. [Google Scholar] [CrossRef] [PubMed]
- Natale, A.; Khaleghi Hashemian, D.; Polesel, J.; Giacosa, A.; Augustin, L.; Negri, E.; Toffolutti, F.; La Vecchia, C.; Rossi, M.; Bravi, F. Healthy Eating Index (HEI-2020) score and colorectal cancer risk. Cancer Epidemiol. 2025, 95, 102771. [Google Scholar] [CrossRef] [PubMed]
- Sharma, R.; Abbasi-Kangevari, M.; Abd-Rabu, R.; Abidi, H.; Abu-Gharbieh, E.; Acuna, J.; Adhikari, S.; Advani, S.M.; Afzal, M.S.; Meybodi, M.A.; et al. Global, regional, and national burden of colorectal cancer and its risk factors, 1990–2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet Gastroenterol. Hepatol. 2022, 7, 627–647. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Zhang, X.; Li, R.; Lin, M.; Ou, T.; Zhou, H.; Chen, Z.; Zhen, L. Global, regional, and national analyses of the burden of colorectal cancer attributable to diet low in milk from 1990 to 2019: Longitudinal observational study. Front. Nutr. 2024, 11, 1431962. [Google Scholar] [CrossRef]
- Xu, Q.; Zhou, M.; Yin, P.; Jin, D. Projections of cancer mortality by 2025 in central China: A modeling study of global burden of disease 2019. Heliyon 2023, 9, e13432. [Google Scholar] [CrossRef]
- Juárez-Vázquez, C.; Rosales-Reynoso, M. Cancer colorrectal (CCR): Alteraciones genéticas y moleculares. Gac. Médica México 2014, 150, 154–164. [Google Scholar]
- Russo, A.; Rizzo, S.; Bronte, G.; Silvestris, N.; Colucci, G.; Gebbia, N.; Bazan, V.; Fulfaro, F. The long and winding road to useful predictive factors for anti-EGFR therapy in metastatic colorectal carcinoma: The KRAS/BRAF pathway. Oncology 2009, 77, 57–68. [Google Scholar] [CrossRef]
- Smeu, A.; Marcovici, I.; Dehelean, C.A.; Dumitrel, S.I.; Borza, C.; Lighezan, R. Flavonoids and Flavonoid-Based Nanopharmaceuticals as Promising Therapeutic Strategies for Colorectal Cancer—An Updated Literature Review. Pharmaceuticals 2025, 18, 231. [Google Scholar] [CrossRef]
- Guarini, C.; Grassi, T.; Pezzicoli, G.; Porta, C. Beyond RAS and BRAF: HER2, a New Actionable Oncotarget in Advanced Colorectal Cancer. Int. J. Mol. Sci. 2021, 22, 6813. [Google Scholar] [CrossRef]
- Yang, Y.H.; Lim, S.B.; Kim, M.J.; Chung, H.J.; Yoo, H.W.; Byeon, J.S.; Myung, S.J.; Lee, W.; Chun, S.; Min, W.K. Three novel mutations of the APC gene in Korean patients with familial adenomatous polyposis. Cancer Genet. Cytogenet. 2010, 200, 34–39. [Google Scholar]
- García-Mico, B.; Gimeno-Valiente, F.; Martin-Arana, J.; Martínez-Castedo, B.; Camblor, D.G.; García-Bartolomé, M.; Palomar, B.; Ciarpaglini, C.M.; Segura, M.C.; Gambardella, V.; et al. 583P COMPReS study: Multiomic profiling reveals organ-specific differences in metastases and identifies novel predictive biomarkers in relapsed localized colon cancer. Ann. Oncol. 2024, 35, S472. [Google Scholar] [CrossRef]
- Lasota, J.; Kaczorowski, M.; Chłopek, M.; Miłek-Krupa, J.; Szczepaniak, M.; Ylaya, K.; Chodyna, M.; Iżycka-Świeszewska, E.; Scherping, A.; Czapiewski, P. An immunohistochemical and molecular genetic study of 60 colorectal carcinoma brain metastases in pursuit of predictive biomarkers for cancer therapy. Hum. Pathol. 2025, 155, 105717. [Google Scholar] [CrossRef] [PubMed]
- Nakayama, M.; Saito, H.; Murakami, K.; Oshima, H.; Oshima, M. Missense Mutant p53 Transactivates Wnt/β-Catenin Signaling in Neighboring p53-Destabilized Cells through the COX-2/PGE2 Pathway. Cancer Res. Commun. 2025, 5, 13–23. [Google Scholar] [CrossRef] [PubMed]
- Levy, L.; Hill, C.S. Alterations in components of the TGF-beta, superfamily signaling pathways in human cancer. Cytokine Growth Factor. Rev. 2006, 17, 41–58. [Google Scholar] [CrossRef]
- Stolfi, C.; Marafini, I.; De Simone, V.; Pallone, F.; Monteleone, G. The Dual Role of Smad7 in the Control of Cancer Growth and Metastasis. Int. J. Mol. Sci. 2013, 14, 23774–23790. [Google Scholar] [CrossRef]
- Chen, S.Q.; Chen, Z.H.; Lin, S.Y.; Dai, Q.B.; Fu, L.X.; Chen, R.Q. KISS1 methylation and expression as predictors of disease progression in colorectal cancer patients. World J. Gastroenterol. 2014, 20, 10071–10081. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Zhang, T.Q.; Cai, J.D.; Li, C.; Xu, Y.; Xu, Y. De novo familial adenomatous polyposis with germline double heterozygosity of APC/BRCA2: A case report and literature review. Hered. Cancer Clin. Pract. 2025, 23, 6. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Gala, M.; Chung, D.C. Hereditary colon cancer syndromes. Semin. Oncol. 2011, 38, 490–499. [Google Scholar] [CrossRef]
- Sahoo, D.K.; Heilmann, R.M.; Patel, A. Understanding molecular mechanisms to facilitate the development of biomarkers for therapeutic intervention in gastrointestinal diseases and sepsis. Front. Genet. 2025, 16, 1581299. [Google Scholar] [CrossRef]
- Zhang, K.; Civan, J.; Mukherjee, S.; Patel, F.; Yang, H. Genetic variations in colorectal cancer risk and clinical outcome. World J. Gastroenterol. 2014, 20, 4167–4177. [Google Scholar] [CrossRef]
- Li, H.; Zhu, F.; Boardman, L.A.; Wang, L.; Oi, N.; Lui, K.; Li, X.; Fu, Y.; Limburg, P.J.; Bode, A.M.; et al. Aspirin Prevents Colorectal Cancer by Normalizing EGFR Expression. EBioMedicine 2005, 2, 447–455. [Google Scholar] [CrossRef] [PubMed]
- Gowhar, R.; Ashraf, K.N.; Deena, E.; Andleeb, R.; Tanzeelah; Haleema, A.; Humaira, M.; Amaan, R.; Salik, U.M.; Ma, B.A.; et al. Non-steroidal anti-inflammatory drugs and biomarkers: A new paradigm in colorectal cancer. Front. Med. 2023, 10, 1130710. [Google Scholar]
- Wang, X.; Chan, A.T.; Slattery, M.L.; Chang-Claude, J.; Potter, J.D.; Gallinger, S.; Caan, B.; Lampe, J.W.; Newcomb, P.A.; Zubair, N.; et al. Influence of smoking, body mass index, and other factors on the preventive effect of nonsteroidal anti-inflammatory drugs on colorectal cancer risk. Cancer Res. 2018, 78, 4790–4799. [Google Scholar] [CrossRef]
- National Comprehensive Cancer Network Guidelines (NCCN Guidelines). Colorectal Cancer Screening. NCCN Guidelines; Version 1.2024; National Comprehensive Cancer Network Guidelines (NCCN Guidelines): Plymouth Meeting, PA, USA, 2024.
- Jiang, X.; Lv, G.; Yuan, J.; Lu, K. Colorectal cancer burden, trends, and risk factors in China: Rising incidence and disparities in the last 3 decades. Lancet Reg. Health—West. Pac. 2025, 55, 101427. [Google Scholar] [CrossRef]
- Wang, X.P.; Li, Z.J.; Magnusson, J.; Brunicardi, F.C. Tissue MicroArray analyses of pancreatic duodenal homeobox-1 in human cancers. World J. Surg. 2005, 29, 334–338. [Google Scholar] [CrossRef]
- Ballian, N.; Liu, S.H.; Brunicardi, F.C. Transcription factor PDX-1 in human colorectal adenocarcinoma: A potential tumor marker? World J. Gastroenterol. 2008, 14, 5823–5826. [Google Scholar] [CrossRef]
- Jack, S. Screening for colorrectal cancer. Gastroenterol. Clin. N. Am. 2008, 37, 97–115. [Google Scholar]
- Xia, K.; Hu, W.; Wang, Y.; Chen, J.; Hu, Z.; An, C.; Xu, P.; Teng, L.; Wu, J.; Liu, L.; et al. Extracellular matrix stiffness modulates the mechanophenotypes and focal adhesions of colon cancer cells leading to their invasions via YAP1. Mechanobiol. Med. 2024, 2, 100062. [Google Scholar] [CrossRef]
- Dong, X. The Biological and Therapeutic Role of DRIM (Down Regulated in Metastasis) in Cancer and Metastatic Cancers. Ph.D. Thesis, Cardiff University, Cardiff, UK, 2024. [Google Scholar]
- Andersen, G.T.; Ianevski, A.; Resell, M.; Pojskic, N.; Rabben, H.L.; Geithus, S.; Kodama, Y.; Hiroyuki, T.; Kainov, D.; Grønbech, J.E.; et al. Multi-bioinformatics revealed potential biomarkers and repurposed drugs for gastric adenocarcinoma-related gastric intestinal metaplasia. npj Syst. Biol. Appl. 2024, 10, 127. [Google Scholar] [CrossRef]
- An, S.; Shim, H.; Kim, K.; Kim, B.; Bang, H.J.; Do, H.; Lee, H.R.; Kim, Y. Pretreatment inflammatory markers predicting treatment outcomes in colorectal cancer. Ann. Coloproctol. 2022, 38, 97–108. [Google Scholar] [CrossRef]
- Sohda, M.; Sakai, M.; Yamaguchi, A.; Watanabe, T.; Nakazawa, N.; Ubukata, Y.; Kuriyam, K.; Sano, A.; Yokobori, T.; Ogawa, H.; et al. Pre-treatment CRP and Albumin Determines Prognosis for Unresectable Advanced Oesophageal Cancer. In Vivo 2022, 36, 1930–1936. [Google Scholar] [CrossRef] [PubMed]
- Kos, F.T.; Cecen Kaynak, S.; Aktürk Esen, S.; Arslan, H.; Uncu, D. Comparison of Different Machine Learning Models for Predicting Long-Term Overall Survival in Non-metastatic Colorectal Cancers. Cureus 2024, 16, e75713. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Mihanfar, A.; Asghari, F.; Majidinia, M. WEE1 Inhibition by AZD1775 Augments Colorectal Cancer Cells Susceptibility to VE-822-induced DNA Damage and Apoptosis. Drug Res. 2025, 75, 66–75. [Google Scholar] [CrossRef] [PubMed]
- Mowat, A.N.; Al-Abady, Z.N. Study the Effect of Caspase-3, Lactate Dehydrogenase, and Oxidative Stress Levels as Promising Biomarkers to Mediate Colon Cancer Therapy. J. Biomed. Biochem. 2024, 3, 23–30. [Google Scholar] [CrossRef]
- Chao, M.W.; Wang, L.T.; Lai, C.Y.; Yang, X.M.; Cheng, Y.W.; Lee, K.H.; Pan, S.L.; Teng, C.M. eIF4E binding protein 1 expression is associated with clinical survival outcomes in colorectal cancer. Oncotarget 2015, 6, 24092–24104. [Google Scholar] [CrossRef]
- Gattuso, G.; Longo, F.; Spoto, G.; Ricci, D.; Lavoro, A.; Candido, S.; Di Cataldo, A.; Broggi, G.; Salvatorelli, L.; Magro, G.; et al. Diagnostic and Prognostic Significance of a Four-miRNA Signature in Colorectal Cancer. Int. J. Mol. Sci. 2025, 26, 1219. [Google Scholar] [CrossRef]
- Kim, L.A.; Han, J.; Kim, T.I.; Park, J.J.; Lee, J.M.; Kim, J.K.; Park, S.; Lee, H. Circulating RNA Markers Associated with Adenoma–Carcinoma Sequence in Colorectal Cancer. Int. J. Mol. Sci. 2025, 26, 1518. [Google Scholar] [CrossRef]
- Srivastava, S.; Anand, A.; Kandhula, A.G.; Jaiswal, P.; Kumar, S.; Gulati, M.; Sachdeva, M.; Behl, T. Precision Medicine in Colorectal Cancer: Targeted Therapies and Biomarker Insights. Curr. Cancer Drug Targets 2025, 25, 1–18. [Google Scholar] [CrossRef]
- Morris, V.K.; Quintanilha, J.; Elvin, J.A.; Graf, R.P.; Kopetz, S. Clinical relevance of tumor fraction assessment from circulating tumor DNA in metastatic colorectal cancer. J. Clin. Oncol. 2025, 43, 237. [Google Scholar] [CrossRef]
- Jacobsen, C.M.; Matos do Canto, L.; Kahns, S.; Hansen, T.F.; Andersen, R.F. What the clinician needs to know about laboratory analyses of circulating tumor DNA. Clin. Color. Cancer, 2025; in press. [Google Scholar] [CrossRef]
- Gottschalk, Z.; Cohen, S.A. The Potential Role of Circulating Tumor DNA as a Tool in the Management of Gastrointestinal Malignancies. Adv. Oncol. 2025; in press. [Google Scholar] [CrossRef]
- Miyashita, Y.; Bando, H.; Watanabe, J.; Suwa, Y.; Kagawa, Y.; Kato, T.; Hasegawa, H.; Komatsu, Y.; Yuki, S.; Asayama, M. Clinical validation of plasma circulating-tumor DNA assay using highly sensitive Safe-SeqS technology for detecting RAS and BRAF V600E in metastatic colorectal cancer. J. Clin. Oncol. 2025, 43 (Suppl. S4), 50. [Google Scholar] [CrossRef]
- Stintzing, S.; Klein-Scory, S.; Fischer von Weikersthal, L.; Fuchs, M.; Kaiser, F.; Heinrich, K.; Modest, D.P.; Hofheinz, R.D.; Decker, T.; Gerger, A.; et al. Baseline Liquid Biopsy in Relation to Tissue-Based Parameters in Metastatic Colorectal Cancer: Results From the Randomized FIRE-4 (AIO-KRK-0114) Study. J. Clin. Oncol. 2025, JCO-24. [Google Scholar] [CrossRef] [PubMed]
- Terán-Brage, E.; Lopez-Mateos, Y.; Abad Hernández, M.M.; Sayagues-Manzano, J.M.; Rodrigues Francoso, A.; Díaz-Sánchez, P.; Fonseca-Sánchez, E., Sr.; Vidal-Tocino, R. Role of RAS/BRAF and PIK3CA mutations in tissue and plasma for prognostic assessment in metastatic colorectal cancer (mCRC). J. Clin. Oncol. 2025, 43 (Suppl. S4), 281. [Google Scholar] [CrossRef]
- LaPelusa, M.B.; Qiao, W.; Iorgulescu, B.; San Lucas, F.A.; Patel, K.; Bhamidipati, D.; Thomas, J.V.; You, Y.N.; Foo, W.C.; Maru, D.M.; et al. Prognostic value of circulating tumor DNA for progression-free survival in patients with locally advanced dMMR/MSI-H colorectal cancer managed without surgery. J. Clin. Oncol. 2025, 43 (Suppl. S4), 256. [Google Scholar] [CrossRef]
- Misawa, M.; Kudo, S.-e. Current Status of Artificial Intelligence Use in Colonoscopy. Digestion 2025, 106, 138–145. [Google Scholar] [CrossRef]
- Chen, J.; Wang, G.; Zhou, J.; Zhang, Z.; Ding, Y.; Xia, K.; Xu, X. AI support for colonoscopy quality control using CNN and transformer architectures. BMC Gastroenterol. 2024, 24, 257. [Google Scholar] [CrossRef]
- Bangolo, A.; Wadhwani, N.; Nagesh, V.K.; Dey, S.; Tran, H.H.V.; Aguilar, I.K.; Auda, A.; Sidiqui, A.; Menon, A.; Daoud, D.; et al. Impact of artificial intelligence in the management of esophageal, gastric and colorectal malignancies. Artif. Intell. Gastrointest. Endosc. 2024, 5, 90704. [Google Scholar] [CrossRef]
- Wei, G.X.; Zhou, Y.W.; Li, Z.P.; Qiu, M. Application of artificial intelligence in the diagnosis, treatment, and recurrence prediction of peritoneal carcinomatosis. Heliyon 2024, 10, e29249. [Google Scholar] [CrossRef]
- Ioanovici, A.-C.; Mărușteri, M.-Ș.; Feier, A.M.; Ioanovici, I.; Dobru, D.-E. Using Synthetic and Pseudosynthetic Data to Enhance Polyp Detection in Future AI-Assisted Endoscopy Frameworks. Is it the Right Time? Preprints 2025. [Google Scholar] [CrossRef]
- Bai, S.; Singh, B.; Ethakota, J.; Ogedegbe, O.; Ntukidem, O.; Chitkara, A.; Rani, S.; Kumar, D.; Hirth, J.o.A.; Malik, D. The role of artificial intelligence in colorectal cancer and polyp detection: A systematic review. J. Clin. Oncol. 2025, 43 (Suppl. S4), 47. [Google Scholar] [CrossRef]
- Tan, Y.; Liu, R.; Xue, J.W.; Feng, Z. Construction and validation of artificial intelligence pathomics models for predicting pathological staging in colorectal cancer: Using multimodal data and clinical variables. Cancer Med. 2024, 13, e6947. [Google Scholar] [CrossRef]
- Grosu, S.; Fabritius, M.; Winkelmann, M.; Puhr-Westerheide, D.; Ingenerf, M.; Maurus, S.; Graser, A.; Schulz, C.; Knösel, T.; Cyran, C.; et al. Effect of artificial intelligence-aided differentiation of adenomatous and non-adenomatous colorectal polyps at CT colonography on radiologists’ therapy management. Eur. Radiol. 2025, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Pal, P.; Pooja, K.; Nabi, Z.; Gupta, R.; Tandan, M.; Rao, G.V.; Reddy, N. Artificial intelligence in endoscopy related to inflammatory bowel disease: A systematic review. Indian. J. Gastroenterol. 2024, 43, 172–187. [Google Scholar] [CrossRef] [PubMed]
- Bernal, J.; Sánchez, F.J.; Fernández-Esparrach, G.; Gil, D.; Rodríguez, C.; Vilariño, F. WM-DOVA maps for accurate polyp highlighting in colonoscopy: Validation vs. saliency maps from physicians. Comput. Med. Imaging Graph. 2015, 43, 99–111. [Google Scholar] [CrossRef] [PubMed]
- Ali, S.; Zhou, F.; Daul, C.; Braden, B.; Bailey, A.; East, J.; Realdon, S.; Georges, W.; Loshchenov, M.; Blondel, W.; et al. Endoscopy Artefact Detection (EAD) Dataset, Version 1; Mendeley: London, UK, 2019. [CrossRef]
- Silva, J.; Histace, A.; Romain, O.; Dray, X.; Granado, B. Toward embedded detection of polyps in WCE images for early diagnosis of colorectal cancer. Int. J. Comput. Assist. Radiol. Surg. 2014, 9, 283–293. [Google Scholar] [CrossRef]
- Koulaouzidis, A.; Iakovidis, D.K.; Yung, D.E.; Rondonotti, E.; Kopylov, U.; Plevris, J.N.; Toth, E.; Eliakim, A.; Wurm Johansson, G.; Marlicz, W.; et al. KID Project: An internet-based digital video atlas of capsule endoscopy for research purposes. Endosc. Int. Open 2017, 5, E477–E483. [Google Scholar] [CrossRef]
- The Gastrolab Image Gallery. Available online: https://www.gastrolab.net/index.htm (accessed on 16 March 2025).
- The Gastrointestinal Atlas-gastrointestinalatlas.com. Available online: https://www.gastrointestinalatlas.com/english/english.html (accessed on 16 March 2025).
- Pogorelov, K.; Randel, K.; Griwodz, C.; de Lange, T.; Eskeland, S.; Johansen, D.; Spampinato, C.; Dang Nguyen, D.T.; Lux, M.; Schmidt, P.; et al. Kvasir: A multi-class image dataset for computer aided gastrointestinal disease detection. In Proceedings of the 8th ACM Multimedia Systems Conference, MMSys 2017, Taipei, Taiwan, 20–23 June 2017; Volume 6, pp. 164–169. [Google Scholar] [CrossRef]
- Jha, D.; Smedsrud, P.; Riegler, M.; Halvorsen, P.; de Lange, T.; Johansen, D.; Dagenborg, H. Kvasir-SEG: A Segmented Polyp Dataset. In Proceedings of the International Conference on Multimedia Modeling, Daejeon, Republic of Korea, 5 January 2020; Lecture Notes in Computer Science (Including Subseries Lecture Notes in Artificial Intelligence and Lecture Notes in Bioinformatics). Volume 11962, pp. 451–462. [Google Scholar] [CrossRef]
- Pogorelov, K.; Randel, K.; de Lange, T.; Eskeland, S.; Johansen, D.; Griwodz, C.; Spampinato, C.; Taschwer, M.; Lux, M.; Schmidt, P.; et al. Nerthus: A bowel preparation quality video dataset. In Proceedings of the 8th ACM Multimedia Systems Conference, MMSys 2017, Taipei, Taiwan, 20–23 June 2017; Volume 5, pp. 170–174. [Google Scholar] [CrossRef]
- Borgli, H.; Thambawita, V.; Smedsrud, P.; Hicks, S.; Jha, D.; Eskeland, S.; Randel, K.; Pogorelov, K.; Lux, M.; Dang, N.; et al. HyperKvasir, a comprehensive multi-class image and video dataset for gastrointestinal endoscopy. Sci. Data 2020, 7, 1–14. [Google Scholar] [CrossRef]
- Rochmawati, N.; Fatichah, C.; Amaliah, B.; Raharjo, A.; Dumont, F.; Thibaudeau, E.; Dumas, C. Deep Learning-Based Lesion Detection in Endoscopy: A Systematic Literature Review. IEEE Access 2025, 13, 43532–43556. [Google Scholar] [CrossRef]
- Handa, P.; Sachdeva, R.A.; Goel, N. CNN Architecture-Based Image Retrieval of Colonoscopy Polyp Frames. In Proceedings of the International Conference on Data Analytics and Computing. ICDAC 2022, Wenzhou, China, 28–29 May 2022; Lecture Notes on Data Engineering and Communications Technologies. Volume 175, pp. 15–23. [Google Scholar] [CrossRef]
- Chang, Y.; Li, P.; Chang, R.; Chang, Y.; Huang, S.; Chen, Y.; Chang, W.; Yen, H. Development and validation of a deep learning-based algorithm for colonoscopy quality assessment. Surg. Endosc. 2022, 36, 6446–6455. [Google Scholar] [CrossRef]
- Gadi, S.R.V.; Muralidharan, S.S.; Brown, J.R.G. Colonoscopy Quality, Innovation, and the Assessment of New Technology. Tech. Innov. Gastrointest. Endosc. 2024, 26, 177–192. [Google Scholar] [CrossRef]
- Taghiakbari, M.; Mori, Y.; von Renteln, D. Artificial intelligence-assisted colonoscopy: A review of current state of practice and research. World J. Gastroenterol. 2021, 27, 8103. [Google Scholar] [CrossRef]
- Finocchiaro, M.; Banfi, T.; Donaire, S.; Arezzo, A.; Guarner-Argente, C.; Menciassi, A.; Casals, A.; Ciuti, G.; Hernansanz, A. A Framework for the Evaluation of Human Machine Interfaces of Robot-Assisted Colonoscopy. IEEE Trans. Biomed. Eng. 2024, 71, 410–422. [Google Scholar] [CrossRef] [PubMed]
- Paderno, A. Scaling Artificial Intelligence in Endoscopy: From Model Development to Machine Learning Operations Frameworks. 2024. Available online: https://iris.unibs.it/handle/11379/596678 (accessed on 16 March 2025).
- Van Berkel, N.; Ahmad, O.F.; Stoyanov, D.; Lovat, L.; Blandford, A. Designing Visual Markers for Continuous Artificial Intelligence Support. ACM Trans. Comput. Healthc. 2020, 2, 1–24. [Google Scholar] [CrossRef]
- Wang, A.T. Real-Time Computer-Aided Polyp Detection and Localization for Clinical Applications. 2020. Available online: https://dspace.mit.edu/handle/1721.1/127535 (accessed on 16 March 2025).
- Hamilton, I.; Phillips, D. Improving the Localization and Coverage of Colonoscopy with Motion Tracking and Surface Mapping. November 2023. Available online: https://macsphere.mcmaster.ca/handle/11375/29113 (accessed on 16 March 2025).
- Ciuti, G.; Skonieczna-Żydecka, K.; Marlicz, W.; Iacovacci, V.; Liu, H.; Stoyanov, D.; Arezzo, A.; Chiurazzi, M.; Toth, E.; Thorlacius, H.; et al. Frontiers of Robotic Colonoscopy: A Comprehensive Review of Robotic Colonoscopes and Technologies. J. Clin. Med. 2020, 9, 1648. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Gene | Purpose | Mutation & Role in Cancer | Associated Cancers |
|---|---|---|---|
| APC | Encodes a tumor suppressor protein involved in signaling, migration, and cell adhesion. | Mutations disrupt cell adhesion and proliferation control. | CRC |
| DCC | Produces netrin-1 protein, functions as a tumor suppressor. | Loss of function can lead to tumor development. | CRC, Esophageal Cancer |
| TP53 | Tumor suppressor gene regulating cell-cycle arrest and apoptosis. | Mutations impair apoptosis, leading to uncontrolled growth. | CRC |
| BRAF | Regulates MAP kinase signaling, impacting cell differentiation and division. | Mutations can lead to hyperactive cell signaling. | CRC, Non-Hodgkin Lymphoma, Malignant Melanoma, Thyroid Cancer, Non-Small Cell Lung Cancer |
| PIK3CA | Encodes p110 alpha, a kinase in cell growth and survival pathways. | Mutations increase cell proliferation and survival. | CRC, Ovarian Cancer, Breast Cancer, Stomach Cancer, Lung Cancer, Brain Cancer |
| P53 | Tumor suppressor controlling cell cycle, apoptosis, and DNA repair. | Mutations contribute to hereditary cancer risks. | Hereditary Cancers |
| KISS1 | Suppressing metastasis formation by Kiss1R binding | Loss of function can enhance metastasis. | CRC |
| SMAD4 | Regulates TGF-β pathway, controls DNA binding for tumor suppression. | Loss of function leads to enhanced tumor progression. | CRC, Polyposis Syndromes, Pancreatic Cancer |
| AKT1 | Involved in oncogenesis, cell proliferation, survival, and angiogenesis processes. | Mutations drive uncontrolled cell growth. | CRC |
| K-RAS | Encodes a GTPase regulating cell division and apoptosis. | Mutations promote persistent cell signaling and growth. | CRC |
| CTNNB1 | Critical for cell adhesion and epithelial layer formation. | Mutations contribute to abnormal cell growth. | CRC, Medulloblastoma, Ovarian Cancer |
| Method | Mechanism | Sensibility | Specificity | Observation |
|---|---|---|---|---|
| Occult blood in feces (Guaiac Test) | Detects peroxidase activity in heme groups present in stool samples. | 30–52% (increases to 90% with yearly use) | 95.2% | Not specific to human hemoglobin, potential false positives from peroxidase-rich foods (e.g., raw vegetables, red meat). Patients should avoid NSAIDs 7 days prior to testing. |
| Feces Immuno- histochemical | Uses monoclonal or polyclonal antibodies to detect human hemoglobin in stool. | 76.5% | 95.3% | Exclusively reacts with human hemoglobin, thus being more specific than Guaiac Test. No dietary restrictions required. Recommended for population-wide screening. |
| DNA Analysis in fecal residues | PCR analysis detecting mutations in KRAS, APC, TP53 and elevated PDX1 levels. | 52% | 94.4% | Used to identify genetic markers associated with CRC risk. |
| Digital Rectal Examination | Initial evaluation method for symptomatic patients. | 4.9% | 97.1% | Not a screening tool, but useful for detecting rectal masses. |
| Flexible Sigmoidoscopy | Uses an endoscope to inspect the rectum, sigmoid colon, and descending colon (up to 60 cm). | 58–75% (small lesions); 72–86% (advanced lesions) | 94% | Reduces CRC mortality; should be performed every 5 years. |
| Colonoscopy | Direct visualization of the colon for polyp and abnormal tissue detection. | 91% | 94% | Gold-standard screening tool. Risks: Perforation (2%), hemorrhage (0.5% post-polypectomy), cardiovascular complications (arrhythmia, hypotension). |
| Endoscopic capsule | Swallowed camera capsule captures images of the digestive tract. | 77% | 59% | Primarily used for small intestine evaluation, limited for colorectal cancer detection. |
| Barium enema | Barium and air introduced into the colon to create contrast-enhanced X-ray images. | 61–100% | 100% | Alternative for patients who cannot undergo colonoscopy. Risks: Perforation (1 in 25,000 cases), mortality (1 in 55,000). |
| CT scan (Virtual Colonoscopy) | Advanced imaging using contrast-enhanced CT scans for colon evaluation. | Varies | Varies | Recommended for patients unable to undergo colonoscopy (e.g., anticoagulant users, those with pulmonary fibrosis, or sedative allergies). |
| Magnetic Resonance Imaging (MRI) | Creates detailed images to assess tumor characteristics and metastases. | 75–90% | 96% | Non-invasive, no ionizing radiation, superior for soft tissue resolution and staging. |
| Endorectal Ultrasound (EUS) | Uses high-frequency ultrasound with a saline balloon for 360° imaging of rectal walls. | 69–97% | Varies | Key method for rectal cancer staging and local recurrence assessment |
| Positron Emission Tomography (PET Scan) | Assesses tumor staging, lymph node involvement, and distant metastases. | Varies | Varies | Used for comprehensive CRC staging, especially extrahepatic metastases. |
| Circulating Tumor DNA (ctDNA) | Circulating Tumor Cells (CTCs) | MicroRNAs (miRNAs) | Extracellular Vehicles (EVs) |
|---|---|---|---|
| ctDNA has gained prominence as a highly specific biomarker for CRC detection. It allows for mutation profiling, treatment response assessment, and minimal residual disease (MRD) detection. | CTCs are cells shed by the primary tumor into the bloodstream, providing real-time insights into metastasis and treatment response. | miRNAs such as hsa-miR-21-5p and miR-221-3p have been identified as potential diagnostic biomarkers in CRC [51]. | EVs secreted by tumor cells carry oncogenic cargo, including proteins, DNA, and RNA, which can serve as diagnostic tools for early-stage CRC detection [52]. |
| Recent studies suggest that ctDNA analysis can detect KRAS, BRAF, and TP53 mutations, which play a critical role in CRC progression [53]. | Studies suggest that a higher CTC count correlates with poorer survival outcomes in metastatic CRC [54]. | ||
| ctDNA-guided surveillance has shown superior sensitivity compared to carcinoembryonic antigen (CEA) levels in predicting disease recurrence [55]. | Advances in single-cell sequencing of CTCs enable better molecular characterization of CRC subtypes, improving personalized treatment strategies. |
| AI Model Type | Accuracy (%) | False Positive Rate | Sensitivity (%) | Specificity (%) | Notable Applications |
|---|---|---|---|---|---|
| CNN-Based Models | ~90% | Moderate | High (85–92%) | Moderate (80–88%) | Polyp detection, segmentation |
| Transformer Models | 85–93% | Low | Moderate (80–88%) | High (90–95%) | Real-time video analysis, polyp localization |
| Hybrid AI Models (CNN + Transformer) | 92–96% | Lowest | Very High (90–97%) | High (92–98%) | Combined polyp detection and classification |
| Dataset | Findings | Size | Reference |
|---|---|---|---|
| CVC-ClinicDB (also named CVC-612) | Polyps | 612 images | [69] |
| Endoscopy Artifact detection 2019 | Endoscopic Artifacts | 5138 images | [70] |
| ETIS-Larib Polyp DB | Polyps | 196 images | [71] |
| KID | Angiectasia, bleeding, inflammations, polyps | 2371 images and 47 videos | [72] |
| GASTROLAB | GI lesions | Some 100 s of images and few videos | [73] |
| El salvador atlas of gastrointestinal video endoscopy | GI lesions | 5154 video clips | [74] |
| Kvasir | Polyps, esophagitis, ulcerative colitis, Z-line, pylorus, cecum, dyed polyp, dyed resection margins, stool | 8000 images | [75] |
| Kvasir-SEG | Polyps | 1000 images | [76] |
| Nerthus | Stool—categorization of bowel cleanliness | 21 videos | [77] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chitca, D.-D.; Popescu, V.; Dumitrescu, A.; Botezatu, C.; Mastalier, B. Advancing Colorectal Cancer Diagnostics from Barium Enema to AI-Assisted Colonoscopy. Diagnostics 2025, 15, 974. https://doi.org/10.3390/diagnostics15080974
Chitca D-D, Popescu V, Dumitrescu A, Botezatu C, Mastalier B. Advancing Colorectal Cancer Diagnostics from Barium Enema to AI-Assisted Colonoscopy. Diagnostics. 2025; 15(8):974. https://doi.org/10.3390/diagnostics15080974
Chicago/Turabian StyleChitca, Dumitru-Dragos, Valentin Popescu, Anca Dumitrescu, Cristian Botezatu, and Bogdan Mastalier. 2025. "Advancing Colorectal Cancer Diagnostics from Barium Enema to AI-Assisted Colonoscopy" Diagnostics 15, no. 8: 974. https://doi.org/10.3390/diagnostics15080974
APA StyleChitca, D.-D., Popescu, V., Dumitrescu, A., Botezatu, C., & Mastalier, B. (2025). Advancing Colorectal Cancer Diagnostics from Barium Enema to AI-Assisted Colonoscopy. Diagnostics, 15(8), 974. https://doi.org/10.3390/diagnostics15080974