
Advancing Diabetic Retinopathy Screening: A Systematic Review of Artificial Intelligence and Optical Coherence Tomography Angiography Innovations

 , , , ,
, , , ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Eligibility Criteria
2.3. Quality Assesment
2.4. Data Extraction
2.5. Comparing AI Models
2.6. Dataset Imbalance and Its Impact on Model Bias
2.7. Data and Code Accessibility
3. Results
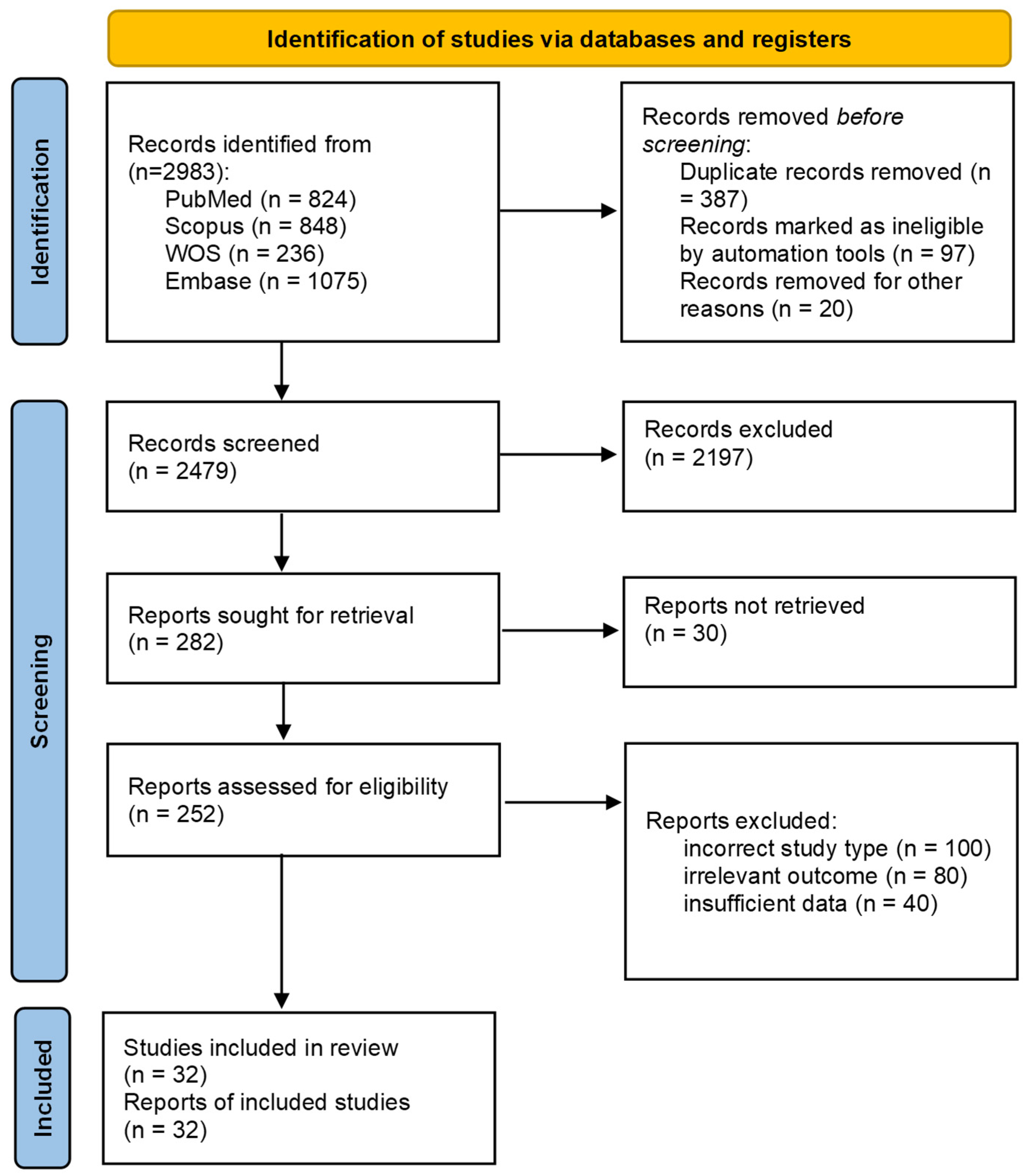
3.1. Literature Search
3.2. Sample Size
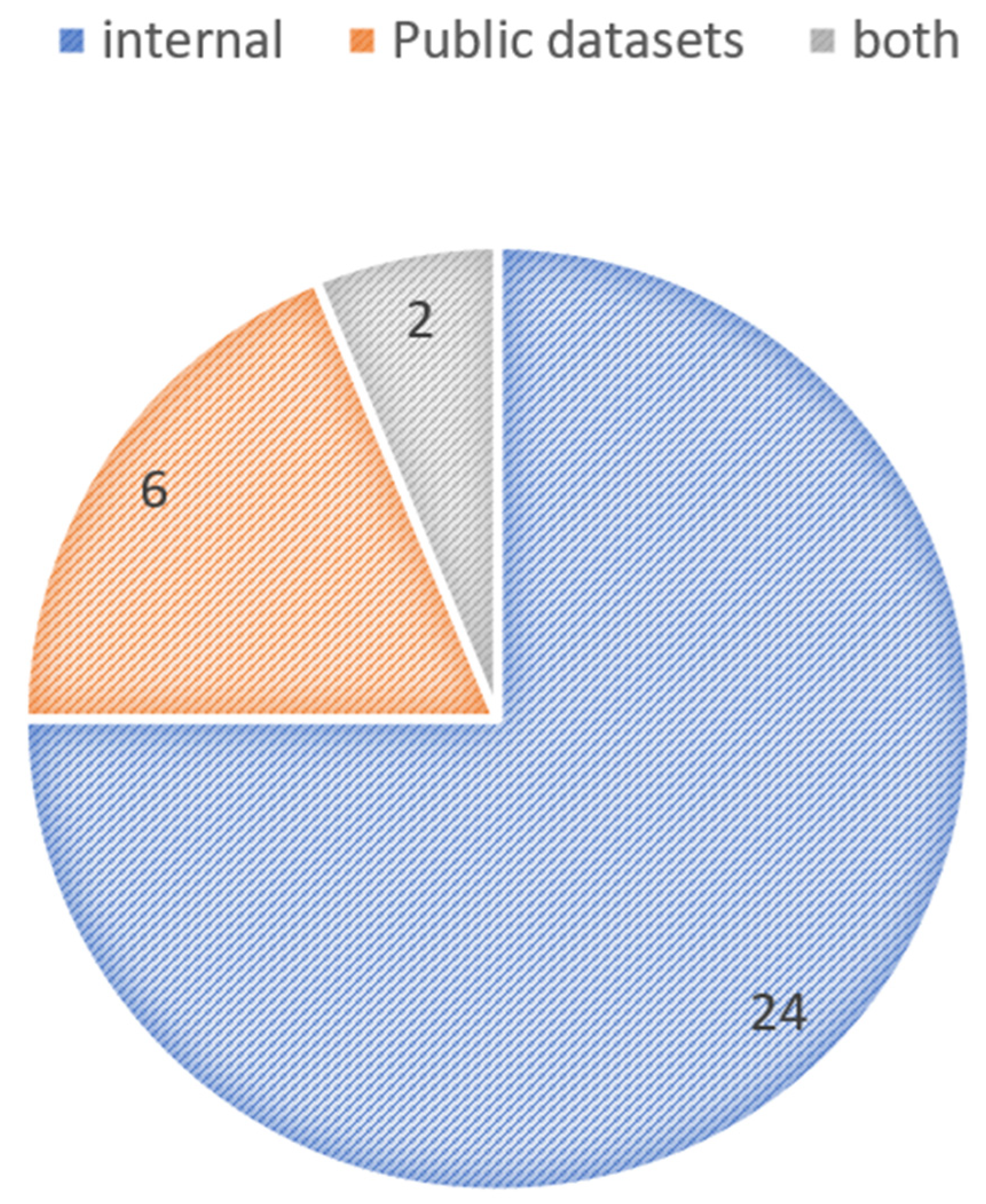
3.3. Training Databases
3.4. Algorithm/Model Used
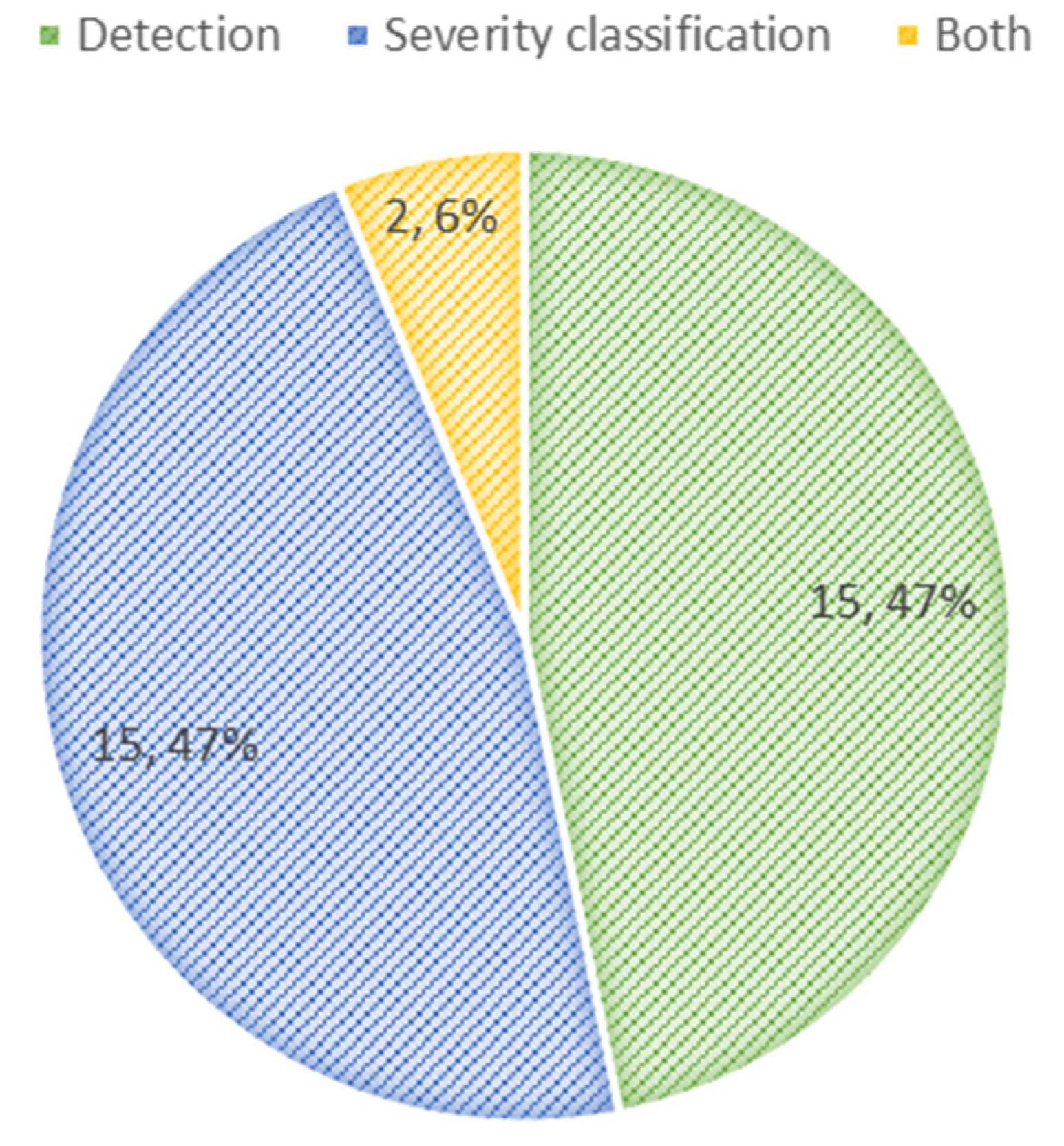
3.5. Detection of DR
3.6. Classification of DR Severity
3.7. Detection and Classification
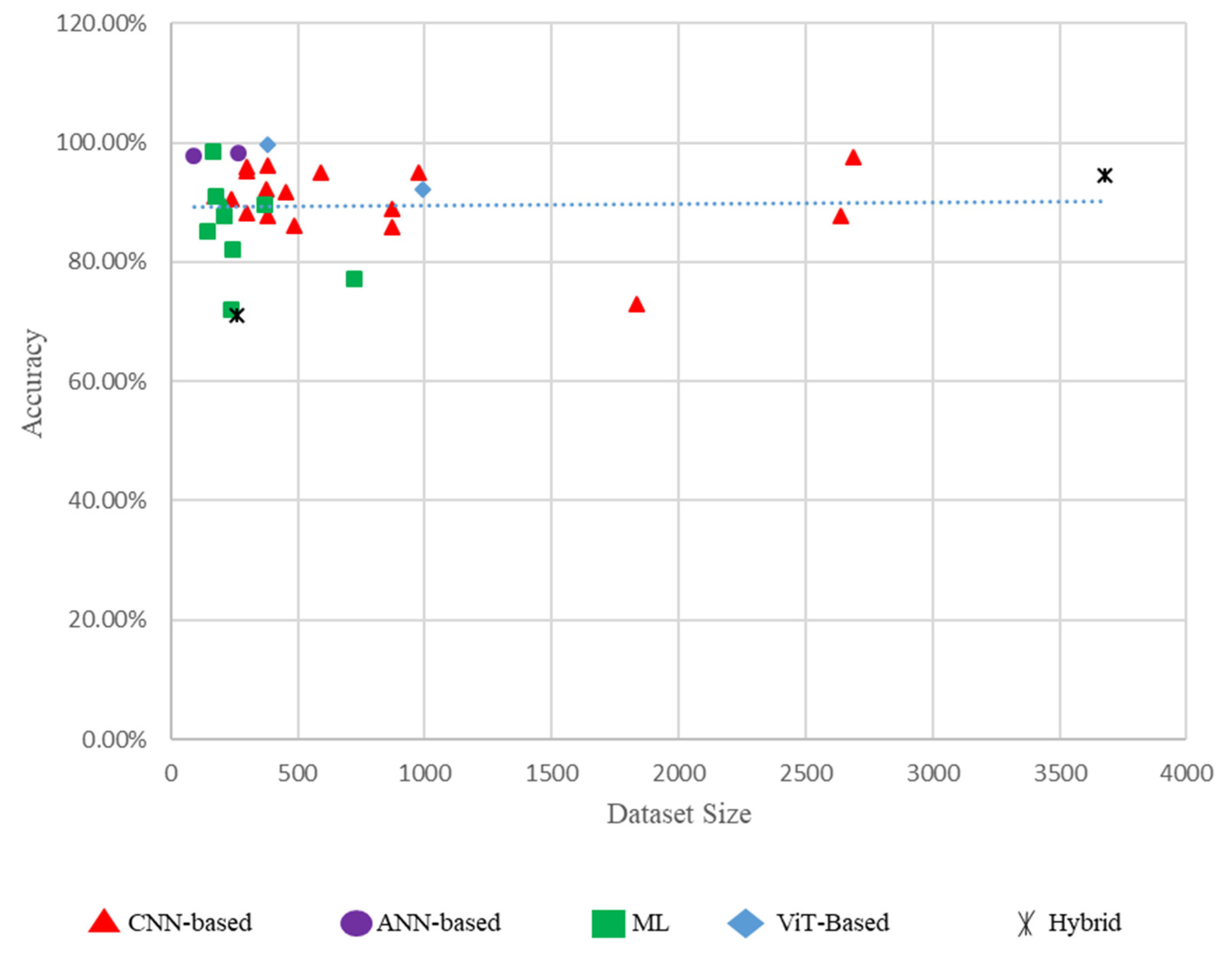
3.8. Performance Comparison of Different Models Based on Dataset Size
3.9. False Positive and False Negative Rates
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
Abbreviations
| AI | Artificial Intelligence |
| ANN | Artificial Neural Network |
| AUC | Area Under the Curve |
| CNN | Convolutional Neural Network |
| DCNN | Deep Convolutional Neural Network |
| DenseNet121 | Dense Convolutional Network 121 |
| DL | Deep Learning |
| DR | Diabetic Retinopathy |
| DRAC | Diabetic Retinopathy and Cataract dataset |
| FA | Fluorescein Angiography |
| KNN | K-Nearest Neighbors |
| LR | Logistic Regression |
| LightGBM | Light Gradient Boosting Machine |
| LDA | Linear Discriminant Analysis |
| ML | Machine Learning |
| NPDR | Non-Proliferative Diabetic Retinopathy |
| OCTA | Optical Coherence Tomography Angiography |
| PDR | Proliferative Diabetic Retinopathy |
| ResNet | Residual Network |
| SFS | Sequential Feature Selection |
| SVM | Support Vector Machine |
| SS-OCTA | Swept-Source Optical Coherence Tomography Angiography |
| TFA-Net | Transformer-based Feature Attention Network |
| UWF-FA | Ultra-Widefield Fluorescein Angiography |
| ViT | Vision Transformer |
| XAI | Explainable Artificial Intelligence |
| XGBoost | Extreme Gradient Boosting |
| VGG16 | Visual Geometry Group 16 |
| SE-ResNet50 | Squeeze-and-Excitation ResNet50 |
References
- Force, U.P.S.T. Screening for Prediabetes and Type 2 Diabetes: US Preventive Services Task Force Recommendation Statement. JAMA 2021, 326, 736–743. [Google Scholar]
- Cao, J.; McLeod, D.S.; Merges, C.A.; Lutty, G.A. Choriocapillaris degeneration and related pathologic changes in human diabetic eyes. Arch. Ophthalmol. 1998, 116, 589–597. [Google Scholar] [CrossRef]
- Duh, E.J.; Sun, J.K.; Stitt, A.W. Diabetic retinopathy: Current understanding, mechanisms, and treatment strategies. JCI Insight 2017, 2, 93751. [Google Scholar] [CrossRef] [PubMed]
- Jiang, Z.; Wang, L.; Wu, Q.; Shao, Y.; Shen, M.; Jiang, W.; Dai, C. Computer-aided diagnosis of retinopathy based on vision transformer. J. Innov. Opt. Health Sci. 2022, 15, 2250009. [Google Scholar] [CrossRef]
- Vaswani, A. Attention is all you need. In Proceedings of the Advances in Neural Information Processing Systems 30 (NIPS 2017), Long Beach, CA, USA, 4–9 December 2017. [Google Scholar]
- Shamshad, F.; Khan, S.; Zamir, S.W.; Khan, M.H.; Hayat, M.; Khan, F.S.; Fu, H. Transformers in medical imaging: A survey. Med. Image Anal. 2023, 88, 102802. [Google Scholar] [CrossRef]
- Hormel, T.T.; Hwang, T.S.; Bailey, S.T.; Wilson, D.J.; Huang, D.; Jia, Y. Artificial intelligence in OCT angiography. Prog. Retin. Eye Res. 2021, 85, 100965. [Google Scholar] [CrossRef]
- Ting, D.S.W.; Pasquale, L.R.; Peng, L.; Campbell, J.P.; Lee, A.Y.; Raman, R.; Tan, G.S.W.; Schmetterer, L.; Keane, P.A.; Wong, T.Y. Artificial intelligence and deep learning in ophthalmology. Br. J. Ophthalmol. 2019, 103, 167–175. [Google Scholar] [CrossRef]
- Jin, K.; Ye, J. Artificial intelligence and deep learning in ophthalmology: Current status and future perspectives. Adv. Ophthalmol. Pract. Res. 2022, 2, 100078. [Google Scholar] [CrossRef]
- Wu, J.-H.; Koseoglu, N.D.; Jones, C.; Liu, T.A. Vision transformers: The next frontier for deep learning-based ophthalmic image analysis. Saudi J. Ophthalmol. 2023, 37, 173–178. [Google Scholar] [CrossRef]
- Kong, M.; Song, S.J. Artificial Intelligence Applications in Diabetic Retinopathy: What We Have Now and What to Expect in the Future. Endocrinol Metab 2024, 39, 416–424. [Google Scholar] [CrossRef]
- Le, D.; Alam, M.; Yao, C.K.; Lim, J.I.; Hsieh, Y.-T.; Chan, R.V.; Toslak, D.; Yao, X. Transfer learning for automated OCTA detection of diabetic retinopathy. Transl. Vis. Sci. Technol. 2020, 9, 35. [Google Scholar] [CrossRef]
- Yagin, F.H.; Yasar, S.; Gormez, Y.; Yagin, B.; Pinar, A.; Alkhateeb, A.; Ardigò, L.P. Explainable Artificial Intelligence Paves the Way in Precision Diagnostics and Biomarker Discovery for the Subclass of Diabetic Retinopathy in Type 2 Diabetics. Metabolites 2023, 13, 1204. [Google Scholar] [CrossRef]
- Hassija, V.; Chamola, V.; Mahapatra, A.; Singal, A.; Goel, D.; Huang, K.; Scardapane, S.; Spinelli, I.; Mahmud, M.; Hussain, A. Interpreting Black-Box Models: A Review on Explainable Artificial Intelligence. Cogn. Comput. 2024, 16, 45–74. [Google Scholar] [CrossRef]
- Lee, A.Y.; Yanagihara, R.T.; Lee, C.S.; Blazes, M.; Jung, H.C.; Chee, Y.E.; Gencarella, M.D.; Gee, H.; Maa, A.Y.; Cockerham, G.C.; et al. Multicenter, Head-to-Head, Real-World Validation Study of Seven Automated Artificial Intelligence Diabetic Retinopathy Screening Systems. Diabetes Care 2021, 44, 1168–1175. [Google Scholar] [CrossRef] [PubMed]
- Çorbacıoğlu, Ş.K.; Aksel, G. Receiver operating characteristic curve analysis in diagnostic accuracy studies: A guide to interpreting the area under the curve value. Turk. J. Emerg. Med. 2023, 23, 195–198. [Google Scholar] [CrossRef] [PubMed]
- White, N.; Parsons, R.; Collins, G.; Barnett, A. Evidence of questionable research practices in clinical prediction models. BMC Med. 2023, 21, 339. [Google Scholar] [CrossRef]
- Staartjes, V.E.; Kernbach, J.M. Foundations of Machine Learning-Based Clinical Prediction Modeling: Part III—Model Evaluation and Other Points of Significance. In Machine Learning in Clinical Neuroscience; Springer: Cham, Switzerland, 2022; pp. 23–31. [Google Scholar]
- Bidwai, P.; Gite, S.; Pradhan, B.; Gupta, H.; Alamri, A. Harnessing deep learning for detection of diabetic retinopathy in geriatric group using optical coherence tomography angiography-OCTA: A promising approach. MethodsX 2024, 13, 102910. [Google Scholar] [CrossRef]
- Khalili Pour, E.; Rezaee, K.; Azimi, H.; Mirshahvalad, S.M.; Jafari, B.; Fadakar, K.; Faghihi, H.; Mirshahi, A.; Ghassemi, F.; Ebrahimiadib, N.; et al. Automated machine learning–based classification of proliferative and non-proliferative diabetic retinopathy using optical coherence tomography angiography vascular density maps. Graefes Arch. Clin. Exp. Ophthalmol. 2023, 261, 391–399. [Google Scholar] [CrossRef] [PubMed]
- Damrawi, G.; Zahran, M.; Amin, E.; Abdelsalam, M. Enforcing artificial neural network in the early detection of diabetic retinopathy OCTA images analysed by multifractal geometry. J. Taibah Univ. Sci. 2020, 14, 1067–1076. [Google Scholar] [CrossRef]
- Aslam, T.M.; Hoyle, D.C.; Puri, V.; Bento, G. Differentiation of Diabetic Status Using Statistical and Machine Learning Techniques on Optical Coherence Tomography Angiography Images. Transl. Vis. Sci. Technol. 2020, 9, 2. [Google Scholar] [CrossRef]
- Heisler, M.; Karst, S.; Lo, J.; Mammo, Z.; Yu, T.; Warner, S.; Maberley, D.; Beg, M.F.; Navajas, E.V.; Sarunic, M.V. Ensemble deep learning for diabetic retinopathy detection using optical coherence tomography angiography. Transl. Vis. Sci. Technol. 2020, 9, 20. [Google Scholar] [CrossRef] [PubMed]
- Abdelsalam, M.M.; Zahran, M. A novel approach of diabetic retinopathy early detection based on multifractal geometry analysis for OCTA macular images using support vector machine. IEEE Access 2021, 9, 22844–22858. [Google Scholar] [CrossRef]
- Liu, Z.; Wang, C.; Cai, X.; Jiang, H.; Wang, J. Discrimination of Diabetic Retinopathy From Optical Coherence Tomography Angiography Images Using Machine Learning Methods. IEEE Access 2021, 9, 51689–51694. [Google Scholar] [CrossRef]
- Ryu, G.; Lee, K.; Park, D.; Park, S.H.; Sagong, M. A deep learning model for identifying diabetic retinopathy using optical coherence tomography angiography. Sci. Rep. 2021, 11, 23024. [Google Scholar] [CrossRef]
- Zang, P.; Gao, L.; Hormel, T.T.; Wang, J.; You, Q.; Hwang, T.S.; Jia, Y. DcardNet: Diabetic Retinopathy Classification at Multiple Levels Based on Structural and Angiographic Optical Coherence Tomography. IEEE Trans. Biomed. Eng. 2021, 68, 1859–1870. [Google Scholar] [CrossRef]
- Nagasawa, T.; Tabuchi, H.; Masumoto, H.; Morita, S.; Niki, M.; Ohara, Z.; Yoshizumi, Y.; Mitamura, Y. Accuracy of Diabetic Retinopathy Staging with a Deep Convolutional Neural Network Using Ultra-Wide-Field Fundus Ophthalmoscopy and Optical Coherence Tomography Angiography. J. Ophthalmol. 2021, 2021, 6651175. [Google Scholar] [CrossRef]
- Hua, C.H.; Kim, K.; Thien, H.T.; You, J.I.; Yu, S.Y.; Le-Tien, T.; Bae, S.H.; Lee, S. Convolutional Network With Twofold Feature Augmentation for Diabetic Retinopathy Recognition From Multi-Modal Images. IEEE J. Biomed. Health Inform. 2021, 25, 2686–2697. [Google Scholar] [CrossRef]
- Guo, Y.; Hormel, T.T.; Gao, L.; You, Q.; Wang, B.; Flaxel, C.J.; Bailey, S.T.; Choi, D.; Huang, D.; Hwang, T.S.; et al. Quantification of Nonperfusion Area in Montaged Widefield OCT Angiography Using Deep Learning in Diabetic Retinopathy. Ophthalmol. Sci. 2021, 1, 100027. [Google Scholar] [CrossRef]
- Li, Y.; Zeghlache, R.; Brahim, I.; Xu, H.; Tan, Y.; Conze, P.-H.; Lamard, M.; Quellec, G.; El Habib Daho, M. Segmentation, classification, and quality assessment of UW-octa images for the diagnosis of diabetic retinopathy. In MICCAI Challenge on Mitosis Domain Generalization; Springer: Berlin/Heidelberg, Germany, 2022; pp. 146–160. [Google Scholar]
- Li, Q.; Zhu, X.R.; Sun, G.; Zhang, L.; Zhu, M.; Tian, T.; Guo, C.; Mazhar, S.; Yang, J.K.; Li, Y. Diagnosing Diabetic Retinopathy in OCTA Images Based on Multilevel Information Fusion Using a Deep Learning Framework. Comput. Math. Methods Med. 2022, 2022, 4316507. [Google Scholar] [CrossRef]
- Yao, H.Y.; Wu, S.J.; Zhan, Z.Y.; Li, Z.J. A Classification Tree Model with Optical Coherence Tomography Angiography Variables to Screen Early-Stage Diabetic Retinopathy in Diabetic Patients. J. Ophthalmol. 2022, 2022, 9681034. [Google Scholar] [CrossRef]
- Zang, P.; Hormel, T.T.; Wang, X.; Tsuboi, K.; Huang, D.; Hwang, T.S.; Jia, Y. A Diabetic Retinopathy Classification Framework Based on Deep-Learning Analysis of OCT Angiography. Transl. Vis. Sci. Technol. 2022, 11, 10. [Google Scholar] [CrossRef]
- Hou, J.; Xiao, F.; Xu, J.; Zhang, Y.; Zou, H.; Feng, R. Deep-OCTA: Ensemble Deep Learning Approaches for Diabetic Retinopathy Analysis on OCTA Images. arXiv 2022, arXiv:2210.00515. [Google Scholar]
- Ryu, G.; Lee, K.; Park, D.; Kim, I.; Park, S.H.; Sagong, M. A Deep Learning Algorithm for Classifying Diabetic Retinopathy Using Optical Coherence Tomography Angiography. Transl. Vis. Sci. Technol. 2022, 11, 39. [Google Scholar] [CrossRef] [PubMed]
- Dong, B.; Wang, X.; Qiang, X.; Du, F.; Gao, L.; Wu, Q.; Cao, G.; Dai, C. A Multi-Branch Convolutional Neural Network for Screening and Staging of Diabetic Retinopathy Based on Wide-Field Optical Coherence Tomography Angiography. IRBM 2022, 43, 614–620. [Google Scholar] [CrossRef]
- Li, Y.H.; Daho, M.E.H.; Conze, P.H.; Zeghlache, R.; Le Boité, H.; Bonnin, S.; Cosette, D.; Magazzeni, S.; Lay, B.; Le Guilcher, A.; et al. Hybrid Fusion of High-Resolution and Ultra-Widefield OCTA Acquisitions for the Automatic Diagnosis of Diabetic Retinopathy. Diagnostics 2023, 13, 2770. [Google Scholar] [CrossRef]
- Zang, P.; Hormel, T.T.; Hwang, T.S.; Bailey, S.T.; Huang, D.; Jia, Y. Deep-Learning-Aided Diagnosis of Diabetic Retinopathy, Age-Related Macular Degeneration, and Glaucoma Based on Structural and Angiographic OCT. Ophthalmol. Sci. 2023, 3, 100245. [Google Scholar] [CrossRef]
- Carrera-Escalé, L.; Benali, A.; Rathert, A.C.; Martín-Pinardel, R.; Bernal-Morales, C.; Alé-Chilet, A.; Barraso, M.; Marín-Martinez, S.; Feu-Basilio, S.; Rosinés-Fonoll, J.; et al. Radiomics-Based Assessment of OCT Angiography Images for Diabetic Retinopathy Diagnosis. Ophthalmol. Sci. 2023, 3, 100259. [Google Scholar] [CrossRef]
- Damrawi, G.E.; Zahran, M.A.; Amin, E.; Abdelsalam, M.M. Numerical detection of diabetic retinopathy stages by multifractal analysis for OCTA macular images using multistage artificial neural network. J. Ambient Intell. Humaniz. Comput. 2023, 14, 7133–7145. [Google Scholar] [CrossRef]
- Daho, M.E.; Li, Y.H.; Zeghlache, R.; Atse, Y.C.; Le Boité, H.; Bonnin, S.; Cosette, D.; Deman, P.; Borderie, L.; Lepicard, C.; et al. Improved Automatic Diabetic Retinopathy Severity Classification Using Deep Multimodal Fusion of UWF-CFP and OCTA Images. In Proceedings of the 10th International Workshop on Ophthalmic Medical Image Analysis (OMIA), Vancouver, BC, Canada, 12 October 2023; pp. 11–20. [Google Scholar]
- Ma, F.; Wang, S.; Dai, C.; Qi, F.; Meng, J. A new retinal OCT-angiography diabetic retinopathy dataset for segmentation and DR grading. J. Biophotonics 2023, 16, e202300052. [Google Scholar] [CrossRef]
- Zhou, Z.; Yu, H.; Zhao, J.; Wang, X.; Wu, Q.; Dai, C. Automatic diagnosis of diabetic retinopathy using vision transformer based on wide-field optical coherence tomography angiography. J. Innov. Opt. Health Sci. 2024, 17, 2350019. [Google Scholar] [CrossRef]
- Bidwai, P.; Gite, S.; Gupta, A.; Pahuja, K.; Kotecha, K.; Jain, N. Multimodal Image Fusion for the Detection of Diabetic Retinopathy Using Optimized Explainable Ai-Based Light GBM Classifier. Inf. Fusion 2023, 111, 102526. [Google Scholar] [CrossRef]
- Li, X.; Wen, X.; Shang, X.; Liu, J.; Zhang, L.; Cui, Y.; Luo, X.; Zhang, G.; Xie, J.; Huang, T.; et al. Identification of diabetic retinopathy classification using machine learning algorithms on clinical data and optical coherence tomography angiography. Eye 2024, 38, 2813–2821. [Google Scholar] [CrossRef] [PubMed]
- Abtahi, M.; Le, D.; Ebrahimi, B.; Dadzie, A.K.; Rahimi, M.; Hsieh, Y.T.; Heiferman, M.J.; Lim, J.I.; Yao, X. Differential Capillary and Large Vessel Analysis Improves OCTA Classification of Diabetic Retinopathy. Investig. Ophthalmol. Vis. Sci. 2024, 65, 20. [Google Scholar] [CrossRef] [PubMed]
- Abtahi, M.; Le, D.; Ebrahimi, B.; Dadzie, A.K.; Rahimi, M.; Hsieh, Y.T.; Heiferman, M.J.; Lim, J.I.; Yao, X. Differential artery-vein analysis improves the OCTA classification of diabetic retinopathy. Biomed. Opt. Express 2024, 15, 3889–3899. [Google Scholar] [CrossRef]
- Ma, F.; Liu, X.; Wang, S.; Li, S.; Dai, C.; Meng, J. CSANet: A lightweight channel and spatial attention neural network for grading diabetic retinopathy with optical coherence tomography angiography. Quant. Imaging Med. Surg. 2024, 14, 1820–1834. [Google Scholar] [CrossRef]
- Komorowski, P.; Baniecki, H.; Biecek, P. Towards evaluating explanations of vision transformers for medical imaging. In Proceedings of the IEEE/CVF Conference on Computer Vision and Pattern Recognition, Vancouver, BC, Canada, 17–24 June 2023; pp. 3726–3732. [Google Scholar]
- Miller, A.R.; Roisman, L.; Zhang, Q.; Zheng, F.; de Oliveira Dias, J.R.; Yehoshua, Z.; Schaal, K.B.; Feuer, W.; Gregori, G.; Chu, Z. Comparison between spectral-domain and swept-source optical coherence tomography angiographic imaging of choroidal neovascularization. Investig. Ophthalmol. Vis. Sci. 2017, 58, 1499–1505. [Google Scholar] [CrossRef]
- Burlina, P.; Joshi, N.; Paul, W.; Pacheco, K.D.; Bressler, N.M. Addressing artificial intelligence bias in retinal diagnostics. Transl. Vis. Sci. Technol. 2021, 10, 13. [Google Scholar] [CrossRef]
- Rauniyar, A.; Hagos, D.H.; Jha, D.; Håkegård, J.E.; Bagci, U.; Rawat, D.B.; Vlassov, V. Federated learning for medical applications: A taxonomy, current trends, challenges, and future research directions. IEEE Internet Things J. 2023, 11, 7374–7398. [Google Scholar] [CrossRef]
- Pesapane, F.; Volonté, C.; Codari, M.; Sardanelli, F. Artificial intelligence as a medical device in radiology: Ethical and regulatory issues in Europe and the United States. Insights Into Imaging 2018, 9, 745–753. [Google Scholar] [CrossRef]
- Hu, W.; Joseph, S.; Li, R.; Woods, E.; Sun, J.; Shen, M.; Jan, C.L.; Zhu, Z.; He, M.; Zhang, L. Population impact and cost-effectiveness of artificial intelligence-based diabetic retinopathy screening in people living with diabetes in Australia: A cost effectiveness analysis. EClinicalMedicine 2024, 67, 102387. [Google Scholar] [CrossRef]
- World Health Organization. Prevention of Blindness from Diabetes Mellitus: Report of a WHO Consultation in Geneva, Switzerland, 9–11 November 2005; World Health Organization: Geneva, Switzerland, 2006. [Google Scholar]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Database | Search String | Results |
|---|---|---|
| Pubmed | (((((((((“Neural Networks, Computer”) OR “Deep Learning”) OR “Artificial Intelligence”) OR (“Machine Learning” OR “Unsupervised Machine Learning” OR “Supervised Machine Learning”)) OR (neural network)) OR (convolutional neural network)) OR (“Computers”)) OR (predictive markers[Title/Abstract])) AND (((((“Retinal Diseases” OR “Hypertensive Retinopathy” OR “Diabetic Retinopathy”) OR (“Diabetes Mellitus” OR “Diabetes, Gestational” OR “Diabetes Mellitus, Type 1” OR “Diabetes Mellitus, Type 2”)) OR (“Eye Diseases”)) OR (“Eye”)) OR (“Neovascularization, Pathologic”))) AND ((((((((((OCTA) OR (oct angiography)) OR (oct-angiography)) OR (Optical coherence tomography angiography)) OR ((“Angiography/classification” OR “Angiography/methods”))) OR (“Tomography, Optical Coherence/methods”)) OR (En Face OCT)) OR (Swept-Source OCT)) OR (OCT angiogram[Title/Abstract])) OR (angiographic OCT)) | 824 |
| Scopus | (TITLE-ABS-KEY(“Neural Networks, Computer” OR “Deep Learning” OR “Artificial Intelligence” OR “Machine Learning” OR “Unsupervised Machine Learning” OR “Supervised Machine Learning” OR “neural network” OR “convolutional neural network” OR “Computers” OR “predictive markers”)) AND (TITLE-ABS-KEY(“Retinal Diseases” OR “Hypertensive Retinopathy” OR “Diabetic Retinopathy” OR “Diabetes Mellitus” OR “Gestational Diabetes” OR “Type 1 Diabetes Mellitus” OR “Type 2 Diabetes Mellitus” OR “Eye Diseases” OR “Eye” OR “Pathologic Neovascularization”)) AND (TITLE-ABS-KEY(OCTA OR “oct angiography” OR “oct-angiography” OR “Optical Coherence Tomography Angiography” OR “Angiography classification” OR “Angiography methods” OR “Optical Coherence Tomography methods” OR “En Face OCT” OR “Swept-Source OCT” OR “OCT angiogram” OR “angiographic OCT”)) | 848 |
| Web Of Science | TS = ((“artificial intelligence” OR “machine learning” OR “deep learning” OR “neural network*” OR “convolutional neural network*”) AND (“diabetes” OR “type 1 diabetes” OR “type 2 diabetes” OR “diabetic complication*” OR “diabetic management”) AND (“optical coherence tomography angiography” OR “optical coherence tomography” OR “angiography” OR “retinal imaging”)) | 236 |
| Embase | (‘artificial intelligence’/exp OR ‘machine learning’/exp OR ‘deep learning’/exp OR ‘neural networks’/exp OR ‘convolutional neural network’/exp) AND (‘diabetes’/exp OR ‘type 1 diabetes’/exp OR ‘type 2 diabetes’/exp OR ‘diabetic complications’/exp OR ‘diabetic management’) AND (‘optical coherence tomography angiography’/exp OR ‘angiography’/exp OR ‘retinal imaging’/exp) | 1075 |
| Author | Year | Training Database | Type Image | Imaging Modality | Number of Images | Outcome | Algorithm/Model Used | Performance Metrics |
|---|---|---|---|---|---|---|---|---|
| Le et al. [12] | 2020 | Internal | OCTA | AngioVue, Optovue, Fremont, CA, USA | 177 | Healthy, No DR, DR | CNN-Based: VGG16 CNN | ACC: 90.84 SPE: 95.83 |
| El Damrawi et al. [21] | 2020 | Internal | OCT-A | OCTA (Triton Topcon SS-OCTA, 1050 nm wavelength, Topcon Corporation, Tokyo, Japan)) | 90 | Normal, No DR, NPDR (mild to moderate) | ANN-Based: Multistage ANN (MANN) | ACC: 97.78% SEN: 96.67% |
| Aslam et al. [22] | 2020 | Internal | SS-OCTA | OCTA (Topcon Swept-Source Triton DRI-OCT, 100,000 A-scan rate, Topcon Corporation, Tokyo, Japan)) | 182 | No Diabetes, No DR, DR | Traditional ML: Random Forest | AUC: 91% |
| Heisler et al. [23] | 2020 | Internal | Multi-modal (OCTA + Structural OCT) | OCTA (Zeiss Plex Elite, 3 × 3 mm protocol, Carl Zeiss Meditec AG, Jena, Germany) | 380 | Referable, non-referable DR | CNN-Based: Ensemble (4× VGG19 CNNs)—Majority Soft Voting | ACC: 92.00% AUC: 92% SEN: 90.40% SPE: 93.30% |
| Abdelsalam et al. [24] | 2021 | Internal | OCTA | Not specified | 170 | Early NPDR vs. Healthy Eyes | Traditional ML: SVM | ACC: 98.50% SEN: 100% SPE: 97.30% |
| Liu et al. [25] | 2021 | Internal | OCTA | Optovue OCTA, Optovue Inc., Fremont, CA, USA | 246 | DR, Healthy Eyes | Traditional ML: Wavelet Features + LR-EN, LR, SVM, XGBoost | ACC: 82% AUC: 84% SEN: 84% SPE: 80% |
| Ryu et al. [26] | 2021 | Internal | Multimodal (OCTA and UWF-FA) | OCTA: Optovue RTVue XR AVANTI, Optovue Inc., Fremont, CA, USA; UWF FA: Optos California, Optos plc, Dunfermline, UK | 240 | Healthy eyes, mild NPDR, moderate NPDR, severe NPDR, PDR | CNN-Based: ResNet101 CNN | ACC: 90.40% AUC: 94.6% SEN: 93.10% SPE: 85.00% |
| Zang et al. [27] | 2021 | Internal | Multi-modal (OCT and OCTA) | RTVue-XR Avanti SD-OCT, Optovue Inc., Fremont, CA, USA | 303 | Three classification levels based on the International Clinical DR scale: -Level 1: 2 classes (non-referable DR, referable DR) -Level 2: 3 classes (no DR, NPDR, PDR) -Level 3: 4 classes (no DR, mild/moderate NPDR, severe NPDR, PDR) | CNN-Based: DcardNet-36 (Dense CNN) | ACC: 95.70% SEN: 91.00% SPE: 98.00% |
| Nagasawa et al. [28] | 2021 | Internal | Multimodal (UWF-FA and OCTA) | UWF Fundus Ophthalmoscopy: Optos 200Tx®, Nikon Corporation, Tokyo, Japan; OCTA: OCT Triton Plus®, Topcon Corporation, Tokyo, Japan | 491 | No DR, Mild and moderate NPDR, Severe NPDR, PDR | CNN-Based: Deep CNN (VGG16) | ACC: 86% AUC: 92.8% SEN: 74.50% SPE: 97.00% |
| Hua et al. [29] | 2021 | Internal and Messidor dataset | Multimodal (Fundus images and SS-OCTA) | Fundus Imaging: Optos 200Tx®, Nikon Corporation, Tokyo, Japan; SS-OCTA: OCT Triton Plus®, Topcon Corporation, Tokyo, Japan | 594 | No DR, Mild and moderate NPDR, Severe NPDR, PDR | CNN-Based: TFA-Net (ResNet-18 Backbone) | ACC: 94.80% AUC: 99.4% |
| Guo et al. [30] | 2021 | Internal and Messidor dataset | Fundus Imaging: Optos 200Tx® by Nikon; SS-OCTA: OCT Triton Plus® by Topcon | OCTA (AngioVue, Optovue, Fremont, CA, USA)) | 978 | No DR, Mild and moderate NPDR, Severe NPDR, PDR | CNN-Based: U-Net-like CNN (ResNet Residual Modules) | ACC: 94.8% AUC: 99.4% |
| Li et al. [31] | 2022 | Internal | Multimodal (Fundus images and SS-OCTA) | Fundus Imaging: Optos 200Tx®, Nikon Corporation, Tokyo, Japan; SS-OCTA: VG200D, SVision Imaging, Ltd., Luoyang, China | 386 | Normal, NPDR, PDR | CNN-Based: DenseNet121, EfficientNet-b3 | AUC: 87.61% |
| Li et al. [32] | 2022 | OCTA-500 dataset | OCTA | SS-OCTA system: VG200D, SVision Imaging, Ltd., Luoyang, China | 301 | Normal, NPDR, PDR | CNN-Based: ResNet50 CNN | ACC: 88.10% AUC: 92% SEN: 51.80% SPE: 96.30% |
| Yao et al. [33] | 2022 | Internal | OCTA | SS-OCTA System: VG200D, SVision Imaging, Ltd., Luoyang, China | 241 | 1. Diabetes, Healthy 2. Referable DR, Non-referable DR 3. Severe DR, Non severe DR | Traditional ML: Classification Tree | AUC: 72% SEN: 66% SPE: 76% |
| Zang et al. [34] | 2022 | Internal | Multi-modal (OCT and OCTA) | SD-OCT system RTVue-XR Avanti, Optovue Inc., Fremont, CA, USA | 456 | non-referable DR, referable DR, vision-threatening DR, NPDR, referable DR but non-vision threatening DR, vision-threatening DR | CNN-Based: 3D CNN | ACC: 91.52% AUC: 96% SEN: 90.77% SPE: 92.50% |
| Hou et al. [35] | 2022 | DRAC dataset | Multimodal (OCTA, Color Fundus Photography) | SD-OCT system RTVue-XR Avanti, Optovue Inc., Fremont, CA, USA | 997 | Non-referable DR, Referable DR, Vision threatening DR | ViT-Based: Pre-trained on EyePACS & DDR | ACC: N/A AUC: 92% SEN: N/A SPE: 86% |
| Khalili Pour et al. [20] | 2022 | Internal | OCTA | OCTA (RTVue XR 100 Avanti, Optovue Inc., Fremont, CA, USA) | 148 | NPDR, PDR | Traditional ML: SVM Optimized by Genetic Algorithm | ACC: 85% AUC: N/A SEN: N/A SPE: N/A |
| Ryu et al. [36] | 2022 | Internal | Multimodal (OCTA and demographic data (age and gender)) | Optovue RTVue XR Avanti, Optovue Inc., Fremont, CA, USA | 1835 | Normal, No DR, Mild NPDR, Moderate NPDR, Severe NPDR, PDR | CNN-Based: ResNet101 CNN | ACC: 72.80% SEN: 67.50% SPE: 94.40% |
| Dong et al. [37] | 2022 | Internal | OCTA, UWF-FA | SS-OCT system RTVue-XR Avanti, Optovue Inc., Fremont, CA, USA | 385 | No DR, Mild NPDR, Moderate to Severe NPDR, PDR | CNN-Based: Multi-Branch CNN (Inception-V3 & VGG16) | ACC: 96.11% AUC: 94.6% SEN: 93.10% SPE: 85.00% |
| Li et al. [38] | 2023 | EviRed dataset | OCTA | OCTA (PLEX®Elite 9000, Carl Zeiss Meditec Inc., Dublin, CA, USA) | 875 | No DR, Mild NPDR, Moderate to Severe NPDR, PDR | CNN-Based: 3D CNN Ensemble (ResNet, DenseNet, EfficientNet) + Hierarchical Fusion | ACC: 88.68% AUC: 88.68% |
| Zang et al. [39] | 2023 | Internal | Multi-modal (Structural OCT and OCTA) | OCTA (Avanti RTVue-XR, Optovue Inc., Fremont, CA, USA) | 302 | Normal, DR, Age-related macular degeneration, Glaucoma | CNN-Based: Custom 16-Layer 3D CNN | ACC: 95% |
| Carrera-Escalé et al. [40] | 2023 | Internal | Multimodal (Fundus Retinography, OCT, and OCTA) | Topcon DRI-Triton, Topcon Corporation, Tokyo, Japan; Cirrus 5000, Carl Zeiss Meditec AG, Jena, Germany; Angioplex Zeiss, Carl Zeiss Meditec AG, Jena, Germany | 726 | Normal, DM, DR, Referable DR | Traditional ML: LR, LDA, SVC, RF | AUC: 77% |
| El Damrawi et al. [41] | 2023 | Internal | SS-OCTA | SS-OCTA (Triton TopCon SS-OCTA, Topcon Corporation, Tokyo, Japan) | 270 | Normal, No DR, NPDR, PDR | ANN-Based: Multistage ANN | ACC: 98.10% SEN: 96.67–100% SPE: 96–100% |
| Daho et al. [42] | 2023 | EviRed dataset | Multi-modal (UWF Color Fundus Photography and OCTA) | OCTA (Clarus 500, Carl Zeiss Meditec, Dublin, CA, USA; PLEX Elite 9000, Carl Zeiss Meditec, Dublin, CA, USA) | 875 | Normal, Mild NPDR, Moderate NPDR, Severe NPDR, PDR, Pan-Retinal Photocoagulation | CNN-Based: Multimodal Deep Fusion (SE-ResNet50 & SE-3D-ResNet50) | ACC: 85.66% AUC: 80.37% SEN: 79.22% SPE: 88.20% |
| Ma et al. [43] | 2023 | ROAD dataset | OCTA | OCTA (Widefield SS-OCT System, VG200D; SVision Imaging, Ltd., Luoyang, China) | 2640 (OCTA-DR data) | Normal, Mild NPDR, PDR | CNN-Based: PACNet (Projective Map Attention CNN) | ACC: 87.5% AUC: N/A SEN: N/A SPE: N/A |
| Zhou et al. [44] | 2023 | Internal | WF-OCTA | WF-OCTA (SS-OCT System, VG200D; SVision Imaging, Ltd., Luoyang, China) | 385 | No DR, Mild NPDR, Moderate to Severe NPDR, PDR | ViT-Based | ACC: 99.55% SEN: 99.49% SPE: 99.57% |
| Bidwai et al. [45] | 2024 | Internal | Multimodal (UWF Color Fundus Photography and OCTA) | UWF Color Fundus Photography and OCTA (Eidon Machine, iCare Finland Oy, Vantaa, Finland; Optovue Avanti, Optovue, Inc., Fremont, CA, USA) | 3680(UWF Color Fundus Photography) 3288(OCTA) | Normal DR (various severity levels) | Hybrid: ResNet-101 CNN + DkSO-Optimized LightGBM | ACC: 94.32% SEN: 94.94% SPE: 94.78% |
| Li et al. [46] | 2024 | Internal | Multimodal (OCTA and Clinical data) | OCTA (Optovue, Inc., Fremont, CA, USA) | 372 | No DR, Mild NPDR, Moderate NPDR, Severe NPDR, Referable DR, Vision threatening DR | Traditional ML: Random forest | ACC: 89.40% AUC: 96.65% |
| Bidwai et al. [19] | 2024 | Internal | Multi-modal (UWF Color Fundus and OCTA) | OCTA (Optovue Avanti Edition, Optovue, Inc., Fremont, CA, USA)) | 262 | Normal DR (various severity levels) | Hybrid: Pre-trained DenseNet201 CNN + Neural Network Classifier | ACC: 71% AUC: 100% SEN: 84% SPE: N/A |
| Abtahi et al. [47] | 2024 | Internal | OCTA | OCTA (AngioVue SD-OCT, Optovue, Fremont, CA, USA) | 212 | Normal, No DR, Mild NPDR, Moderate NPDR, Severe NPDR | Traditional ML: SVM + SFS + CLV | ACC (Binary): 87.63% SEN (Binary): 89.70% |
| Abtahi et al. [48] | 2024 | Internal | OCTA | OCTA (AngioVue SD-OCT, Optovue, Inc., Fremont, CA, USA)) | 212 | Normal, No DR, Mild NPDR, Moderate NPDR, Severe NPDR | Traditional ML: SVM + SFS + AVA-Net | ACC: 89.26% (Binary) AUC: 87.23% |
| Ma et al. [49] | 2024 | ROAD dataset | OCTA | OCTA (SS-OCT System, manufacturer details not specified)) | 2693 (OCTA-DR data) | Normal, Mild NPDR, PDR | CNN-Based: CSANet (Channel & Spatial Attention CNN) | ACC: 97.41% AUC: N/A SEN: N/A SPE: N/A |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hayati, A.; Abdol Homayuni, M.R.; Sadeghi, R.; Asadigandomani, H.; Dashtkoohi, M.; Eslami, S.; Soleimani, M. Advancing Diabetic Retinopathy Screening: A Systematic Review of Artificial Intelligence and Optical Coherence Tomography Angiography Innovations. Diagnostics 2025, 15, 737. https://doi.org/10.3390/diagnostics15060737
Hayati A, Abdol Homayuni MR, Sadeghi R, Asadigandomani H, Dashtkoohi M, Eslami S, Soleimani M. Advancing Diabetic Retinopathy Screening: A Systematic Review of Artificial Intelligence and Optical Coherence Tomography Angiography Innovations. Diagnostics. 2025; 15(6):737. https://doi.org/10.3390/diagnostics15060737
Chicago/Turabian StyleHayati, Alireza, Mohammad Reza Abdol Homayuni, Reza Sadeghi, Hassan Asadigandomani, Mohammad Dashtkoohi, Sajad Eslami, and Mohammad Soleimani. 2025. "Advancing Diabetic Retinopathy Screening: A Systematic Review of Artificial Intelligence and Optical Coherence Tomography Angiography Innovations" Diagnostics 15, no. 6: 737. https://doi.org/10.3390/diagnostics15060737
APA StyleHayati, A., Abdol Homayuni, M. R., Sadeghi, R., Asadigandomani, H., Dashtkoohi, M., Eslami, S., & Soleimani, M. (2025). Advancing Diabetic Retinopathy Screening: A Systematic Review of Artificial Intelligence and Optical Coherence Tomography Angiography Innovations. Diagnostics, 15(6), 737. https://doi.org/10.3390/diagnostics15060737