
Low-Grade Endometrial Cancer with Abnormal p53 Expression as a Separate Clinical Entity: Insights from RNA Sequencing and Immunohistochemistry

 , , , , , ,
, , , , , ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Case Selection and Clinicopathological Characteristics
2.2. RNA Sequencing and Data Processing
2.2.1. Total RNA Isolation
2.2.2. RNA Sequencing
2.2.3. Sequencing Data Analysis
2.2.4. Immunohistochemical Staining
- Antibodies
- Procedure
- Immunohistochemical Scoring
2.3. Statistical Analysis
3. Results
3.1. Clinicopathological Characteristics
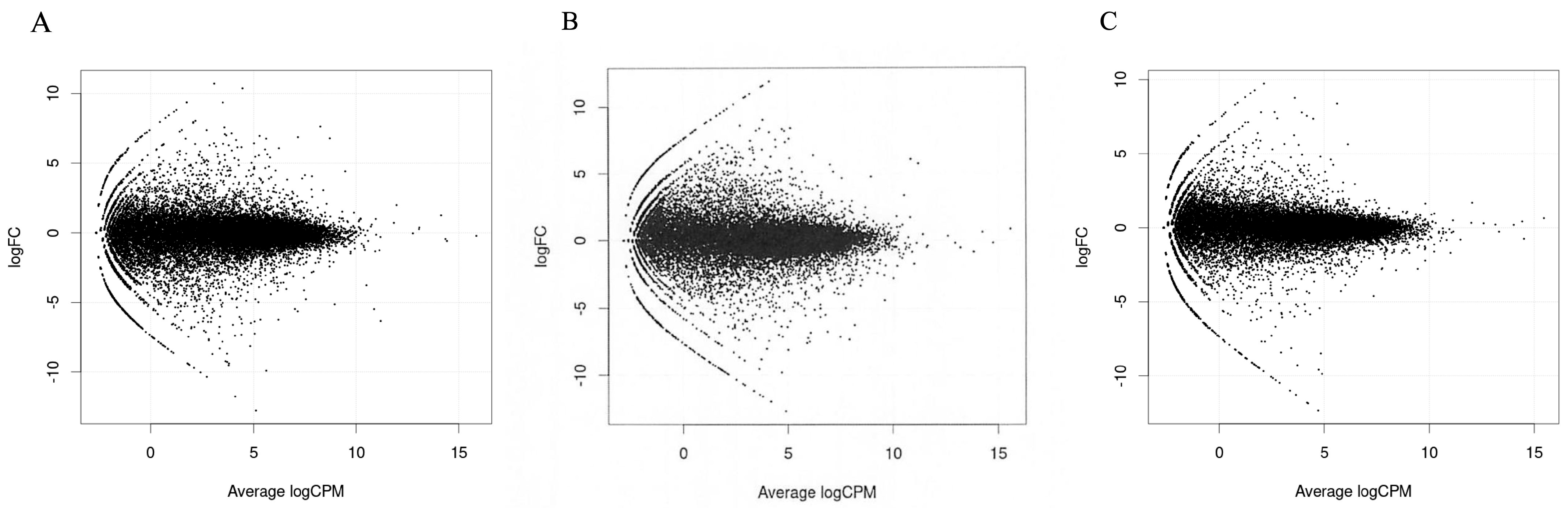
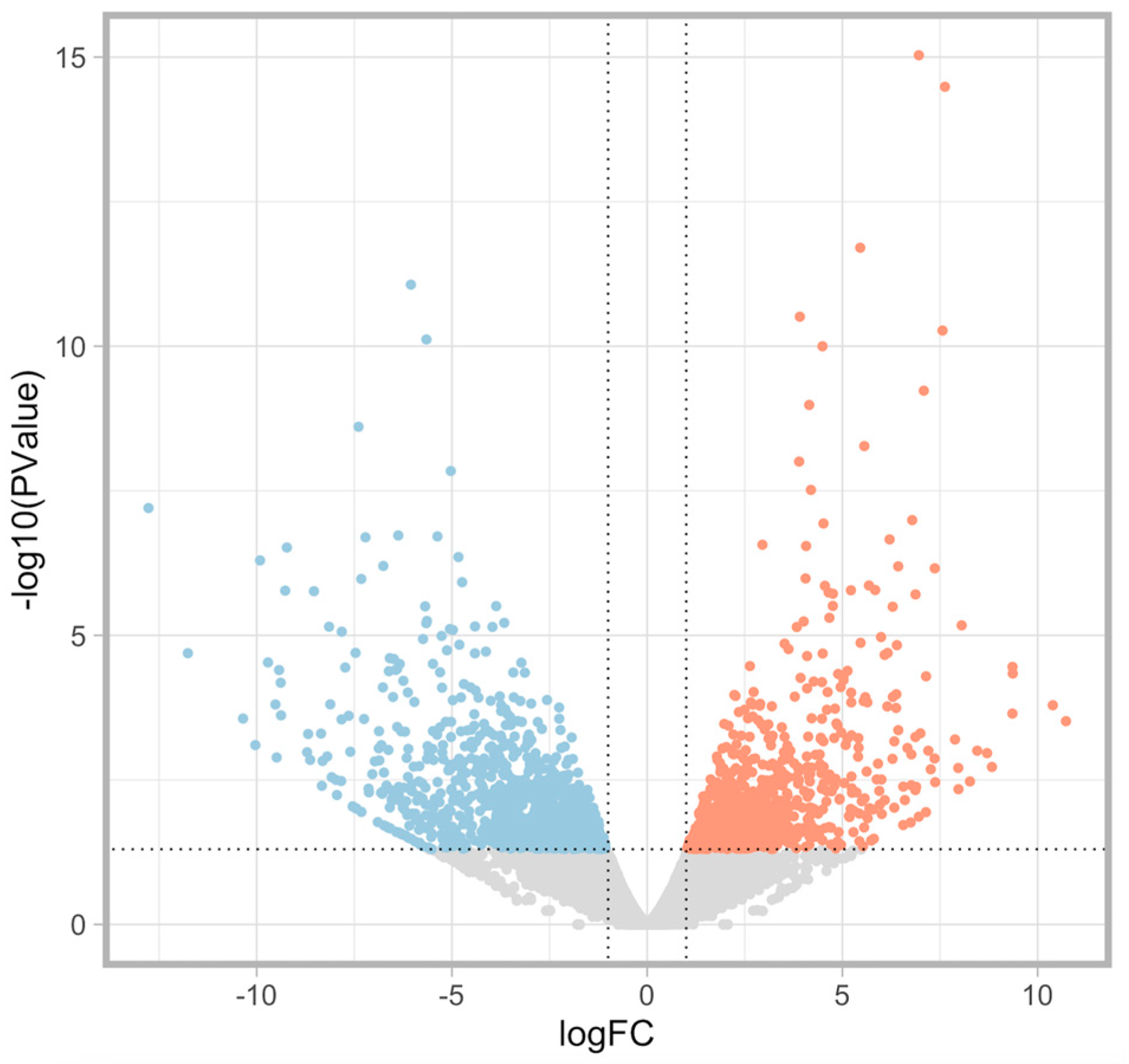
3.2. RNA Sequencing Analysis
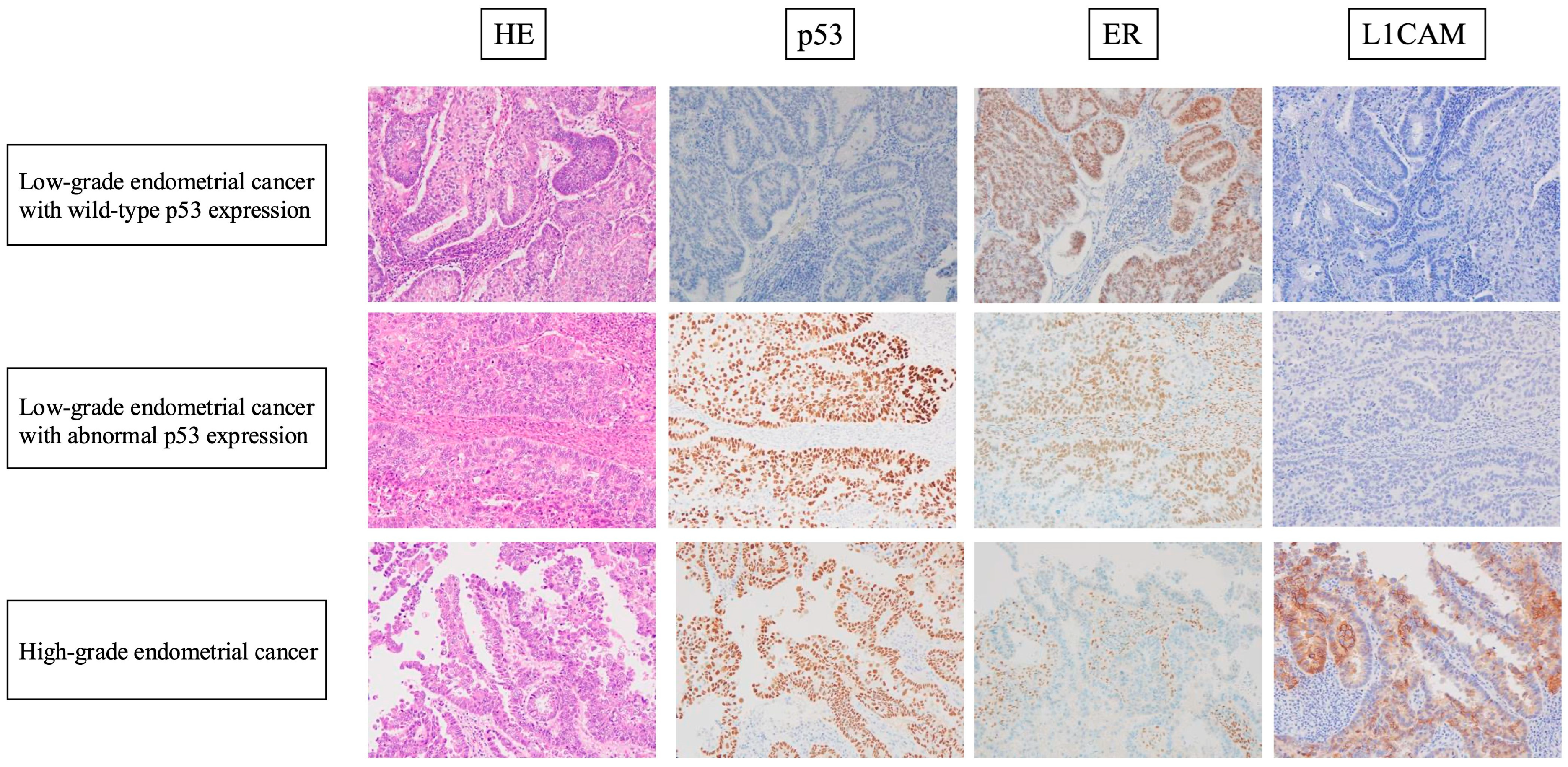
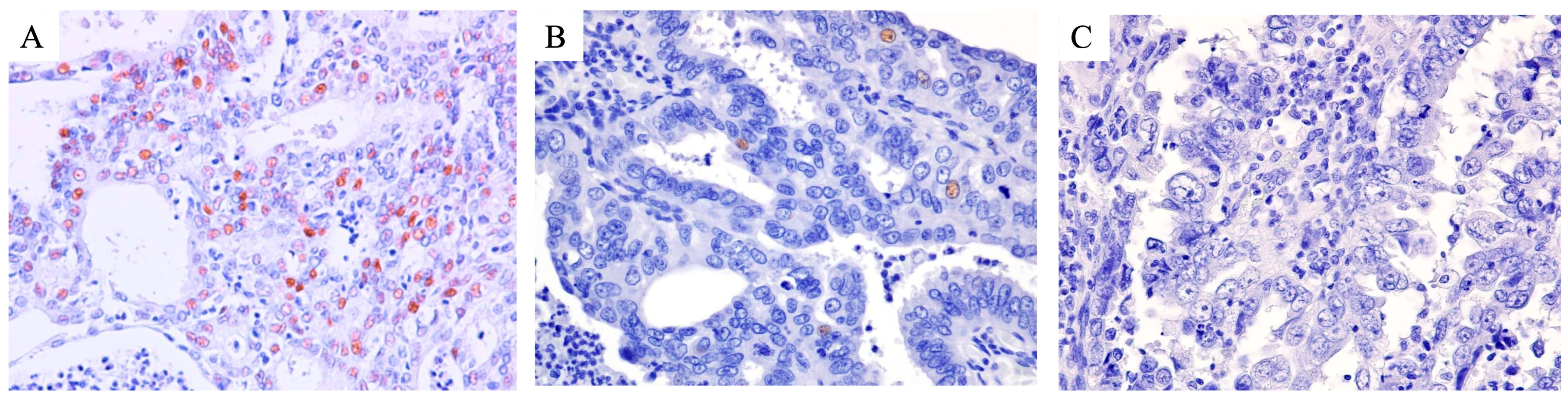
3.3. Immunohistochemical Analysis
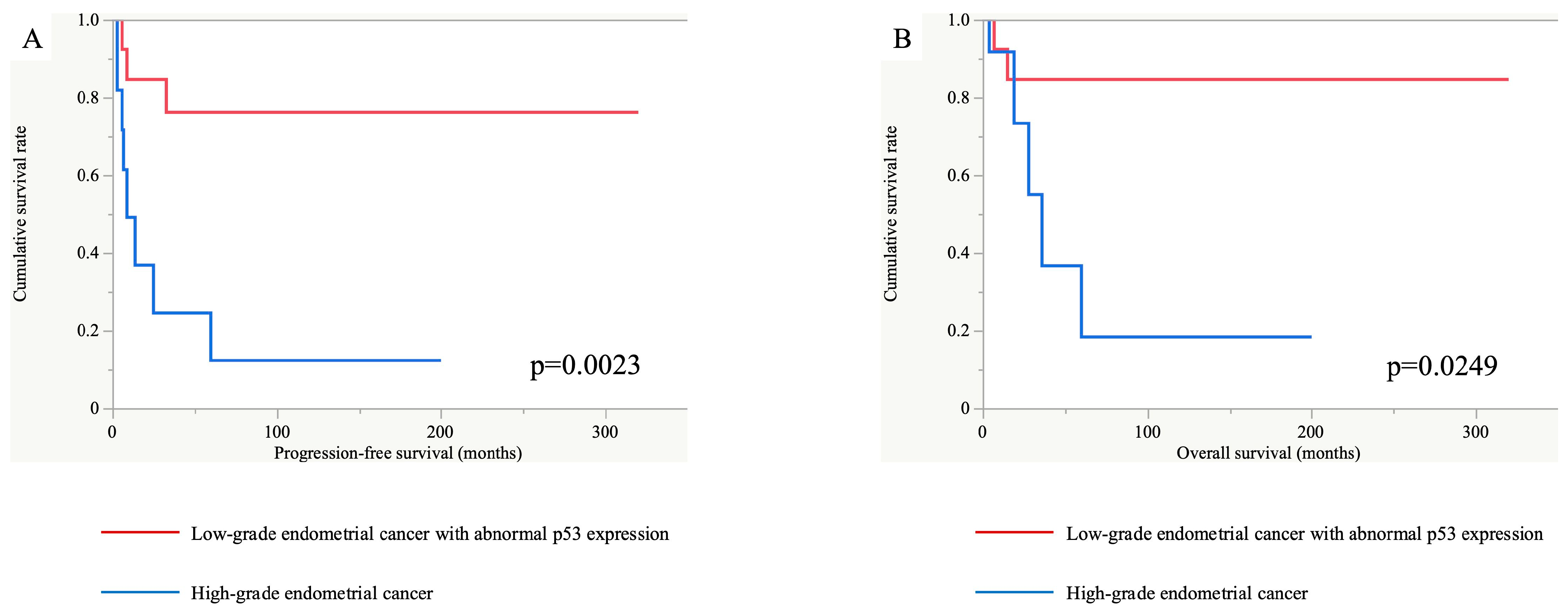
3.4. Survival Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| EClop53wt | low-grade endometrial cancer with wild-type p53 expression |
| EClop53ab | low-grade endometrial cancer with abnormal p53 expression |
| EChi | high-grade endometrial cancer |
| TCGA | The Cancer Genome Atlas |
| HE | hematoxylin and eosin |
| FIGO | International Federation of Gynecology and Obstetrics |
| PFS | progression-free survival |
| OS | overall survival |
| ITCs | isolated tumor cells |
| DEGs | differentially expressed genes |
| CPM | count per million |
| logFC | log fold changes |
References
- Bokhman, J.V. Two pathogenetic types of endometrial carcinoma. Gynecol. Oncol. 1983, 15, 10–17. [Google Scholar] [CrossRef] [PubMed]
- Kandoth, C.; Schultz, N.; Cherniack, A.D.; Akbani, R.; Liu, Y.; Shen, H.; Robertson, A.G.; Pashtan, I.; Shen, R.; Benz, C.C.; et al. Integrated genomic characterization of endometrial carcinoma. Nature 2013, 497, 67–73. [Google Scholar] [PubMed]
- Kommoss, S.; McConechy, M.K.; Kommoss, F.; Leung, S.; Bunz, A.; Magrill, J.; Britton, H.; Kommoss, F.; Grevenkamp, F.; Karnezis, A.; et al. Final validation of the ProMisE molecular classifier for endometrial carcinoma in a large population-based case series. Ann. Oncol. 2018, 29, 1180–1188. [Google Scholar] [CrossRef]
- Concin, N.; Matias-Guiu, X.; Vergote, I.; Cibula, D.; Mirza, M.R.; Marnitz, S.; Ledermann, J.; Bosse, T.; Chargari, C.; Fagotti, A.; et al. ESGO/ESTRO/ESP guidelines for the management of patients with endometrial carcinoma. Int. J. Gynecol. Cancer 2021, 31, 12–39. [Google Scholar] [CrossRef] [PubMed]
- Berek, J.S.; Matias-Guiu, X.; Creutzberg, C.; Fotopoulou, C.; Gaffney, D.; Kehoe, S.; Lindemann, K.; Mutch, D.; Concin, N. FIGO staging of endometrial cancer: 2023. Int. J. Gynaecol. Obstet. 2023, 162, 383–394. [Google Scholar] [CrossRef]
- Vrede, S.W.; Kasius, J.; Bulten, J.; Teerenstra, S.; Huvila, J.; Colas, E.; Gil-Moreno, A.; Boll, D.; Vos, M.C.; van Altena, A.M.; et al. Relevance of Molecular Profiling in Patients with Low-Grade Endometrial Cancer. JAMA Netw. Open 2022, 5, e2247372. [Google Scholar] [CrossRef]
- Stelloo, E.; Nout, R.A.; Osse, E.M.; Jurgenliemk-Schulz, I.J.; Jobsen, J.J.; Lutgens, L.C.; van der Steen-Banasik, E.M.; Nijman, H.W.; Putter, H.; Bosse, T.; et al. Improved Risk Assessment by Integrating Molecular and Clinicopathological Factors in Early-stage Endometrial Cancer-Combined Analysis of the PORTEC Cohorts. Clin. Cancer Res. 2016, 22, 4215–4224. [Google Scholar] [CrossRef]
- Talhouk, A.; McConechy, M.K.; Leung, S.; Li-Chang, H.H.; Kwon, J.S.; Melnyk, N.; Yang, W.; Senz, J.; Boyd, N.; Karnezis, A.N.; et al. A clinically applicable molecular-based classification for endometrial cancers. Br. J. Cancer 2015, 113, 299–310. [Google Scholar] [CrossRef]
- Talhouk, A.; McConechy, M.K.; Leung, S.; Yang, W.; Lum, A.; Senz, J.; Boyd, N.; Pike, J.; Anglesio, M.; Kwon, J.S.; et al. Confirmation of ProMisE: A simple, genomics-based clinical classifier for endometrial cancer. Cancer 2017, 123, 802–813. [Google Scholar] [CrossRef]
- Britton, H.; Huang, L.; Lum, A.; Leung, S.; Shum, K.; Kale, M.; Burleigh, A.; Senz, J.; Yang, W.; McConechy, M.; et al. Molecular classification defines outcomes and opportunities in young women with endometrial carcinoma. Gynecol. Oncol. 2019, 153, 487–495. [Google Scholar] [CrossRef]
- Yano, M.; Ito, K.; Yabuno, A.; Ogane, N.; Katoh, T.; Miyazawa, M.; Miyazawa, M.; Hasegawa, K.; Narahara, H.; Yasuda, M. Impact of TP53 immunohistochemistry on the histological grading system for endometrial endometrioid carcinoma. Mod. Pathol. 2019, 32, 1023–1031. [Google Scholar] [CrossRef] [PubMed]
- Puppo, A.; Fraternali Orcioni, G.; Clignon, V.; Musizzano, Y.; Zavattero, C.A.; Vocino Trucco, G.; Benazzo, G.M.; Vizzielli, G.; Restaino, S.; Mariuzzi, L.; et al. Where Morphological and Molecular Classifications Meet: The Role of p53 Immunohistochemistry in the Prognosis of Low-Risk Endometrial Carcinoma (GLAMOUR Study). Cancers 2024, 16, 1088. [Google Scholar] [CrossRef] [PubMed]
- Hachisuga, K.; Ohishi, Y.; Tomonobe, H.; Yahata, H.; Kato, K.; Oda, Y. Endometrial endometrioid carcinoma, grade 1, is more aggressive in the elderly than in the young. Histopathology 2021, 79, 708–719. [Google Scholar] [CrossRef] [PubMed]
- Union for International Cancer Control. Skin Tumours. In UICC TNM Classification of Malignant Tumours, 8th ed.; Union for International Cancer Control: Geneva, Switzerland, 2016. [Google Scholar]
- World Health Organization. WHO Classification of Tumours Editorial Board. In Female Genital Tumours, WHO Classification of Tumours; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- Bolger, A.M.; Lohse, M.; Usadel, B. Trimmomatic: A flexible trimmer for Illumina sequence data. Bioinformatics 2014, 30, 2114–2120. [Google Scholar] [CrossRef]
- Li, B.; Dewey, C.N. RSEM: Accurate transcript quantification from RNA-Seq data with or without a reference genome. BMC Bioinform. 2011, 12, 323. [Google Scholar] [CrossRef]
- Langmead, B.; Salzberg, S.L. Fast gapped-read alignment with Bowtie 2. Nat. Methods 2012, 9, 357–359. [Google Scholar] [CrossRef]
- Robinson, M.D.; McCarthy, D.J.; Smyth, G.K. edgeR: A Bioconductor package for differential expression analysis of digital gene expression data. Bioinformatics 2010, 26, 139–140. [Google Scholar] [CrossRef]
- Köbel, M.; Ronnett, B.M.; Singh, N.; Soslow, R.A.; Gilks, C.B.; McCluggage, W.G. Interpretation of P53 Immunohistochemistry in Endometrial Carcinomas: Toward Increased Reproducibility. Int. J. Gynecol. Pathol. 2019, 38 (Suppl. S1), S123–S131. [Google Scholar] [CrossRef]
- Zeimet, A.G.; Reimer, D.; Huszar, M.; Winterhoff, B.; Puistola, U.; Azim, S.A.; Muller-Holzner, E.; Ben-Arie, A.; van Kempen, L.C.; Petru, E.; et al. L1CAM in early-stage type I endometrial cancer: Results of a large multicenter evaluation. J. Natl. Cancer Inst. 2013, 105, 1142–1150. [Google Scholar] [CrossRef]
- Kommoss, F.K.; Karnezis, A.N.; Kommoss, F.; Talhouk, A.; Taran, F.A.; Staebler, A.; Gilks, C.B.; Huntsman, D.G.; Krämer, B.; Brucker, S.Y.; et al. L1CAM further stratifies endometrial carcinoma patients with no specific molecular risk profile. Br. J. Cancer 2018, 119, 480–486. [Google Scholar] [CrossRef]
- Harada, N.; Gansauge, S.; Gansauge, F.; Gause, H.; Shimoyama, S.; Imaizumi, T.; Mattfeld, T.; Schoenberg, M.H.; Beger, H.G. Nuclear accumulation of p53 correlates significantly with clinical features and inversely with the expression of the cyclin-dependent kinase inhibitor p21(WAF1/CIP1) in pancreatic cancer. Br. J. Cancer 1997, 76, 299–305. [Google Scholar] [CrossRef] [PubMed]
- Huszar, M.; Pfeifer, M.; Schirmer, U.; Kiefel, H.; Konecny, G.E.; Ben-Arie, A.; Edler, L.; Münch, M.; Müller-Holzner, E.; Jerabek-Klestil, S.; et al. Up-regulation of L1CAM is linked to loss of hormone receptors and E-cadherin in aggressive subtypes of endometrial carcinomas. J. Pathol. 2010, 220, 551–561. [Google Scholar] [CrossRef] [PubMed]
- Colas, E.; Pedrola, N.; Devis, L.; Ertekin, T.; Campoy, I.; Martinez, E.; Llaurado, M.; Rigau, M.; Olivan, M.; Garcia, M.; et al. The EMT signaling pathways in endometrial carcinoma. Clin. Transl. Oncol. 2012, 14, 715–720. [Google Scholar] [CrossRef]
- Fogel, M.; Gutwein, P.; Mechtersheimer, S.; Riedle, S.; Stoeck, A.; Smirnov, A.; Edler, L.; Ben-Arie, A.; Huszar, M.; Altevogt, P. L1 expression as a predictor of progression and survival in patients with uterine and ovarian carcinomas. Lancet 2003, 362, 869–875. [Google Scholar] [CrossRef]
- Karnezis, A.N.; Leung, S.; Magrill, J.; McConechy, M.K.; Yang, W.; Chow, C.; Kobel, M.; Lee, C.H.; Huntsman, D.G.; Talhouk, A.; et al. Evaluation of endometrial carcinoma prognostic immunohistochemistry markers in the context of molecular classification. J. Pathol. Clin. Res. 2017, 3, 279–293. [Google Scholar] [CrossRef] [PubMed]
- El-Deiry, W.S.; Tokino, T.; Velculescu, V.E.; Levy, D.B.; Parsons, R.; Trent, J.M.; Lin, D.; Mercer, W.E.; Kinzler, K.W.; Vogelstein, B. WAF1, a potential mediator of p53 tumor suppression. Cell 1993, 75, 817–825. [Google Scholar] [CrossRef]
- Ogane, N.; Hori, S.I.; Yano, M.; Katoh, T.; Kamoshida, S.; Kato, H.; Kameda, Y.; Yasuda, M. Preponderance of endometrial carcinoma in elderly patients. Mol. Clin. Oncol. 2018, 9, 269–273. [Google Scholar] [CrossRef]
- Creasman, W.T.; Odicino, F.; Maisonneuve, P.; Quinn, M.A.; Beller, U.; Benedet, J.L.; Heintz, A.P.; Ngan, H.Y.; Pecorelli, S. Carcinoma of the corpus uteri. FIGO 26th Annual Report on the Results of Treatment in Gynecological Cancer. Int. J. Gynaecol. Obstet. 2006, 95 (Suppl. S1), S105–S143. [Google Scholar]
- Singh, N.; Piskorz, A.M.; Bosse, T.; Jimenez-Linan, M.; Rous, B.; Brenton, J.D.; Gilks, C.B.; Köbel, M. p53 immunohistochemistry is an accurate surrogate for TP53 mutational analysis in endometrial carcinoma biopsies. J. Pathol. 2020, 250, 336–345. [Google Scholar] [CrossRef]
- León-Castillo, A.; Gilvazquez, E.; Nout, R.; Smit, V.T.; McAlpine, J.N.; McConechy, M.; Kommoss, S.; Brucker, S.Y.; Carlson, J.W.; Epstein, E.; et al. Clinicopathological and molecular characterisation of ‘multiple-classifier’ endometrial carcinomas. J. Pathol. 2020, 250, 312–322. [Google Scholar] [CrossRef]
- McCluggage, W.G.; Bosse, T.; Gilks, C.B.; Howitt, B.E.; McAlpine, J.N.; Nucci, M.R.; Rabban, J.T.; Singh, N.; Talia, K.L.; Parra-Herran, C. FIGO 2023 endometrial cancer staging: Too much, too soon? Int. J. Gynecol. Cancer 2023, 34, 138–143. [Google Scholar] [CrossRef] [PubMed]
- Jamieson, A.; Vermij, L.; Kramer, C.J.H.; Jobsen, J.J.; Jurgemlienk-Schulz, I.; Lutgens, L.; Mens, J.W.; Haverkort, M.A.D.; Slot, A.; Nout, R.A.; et al. Clinical Behavior and Molecular Landscape of Stage I p53-Abnormal Low-Grade Endometrioid Endometrial Carcinomas. Clin. Cancer Res. 2023, 29, 4949–4957. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Low-Grade Endometrial Cancer with Wild-Type p53 Expression (n = 16) | Low-Grade Endometrial Cancer with Abnormal p53 Expression (n = 13) | High-Grade Endometrial Cancer (n = 15) | |
|---|---|---|---|
| Age, n (%) | |||
| <60 years | 5 (31.3%) | 4 (30.8%) | 2 (13.3%) |
| ≥60 years | 11 (68.7%) | 9 (69.2%) | 13 (86.7%) |
| Myometrial invasion, n (%) | |||
| <1/2 | 4 (25.0%) | 9 (69.2%) | 5 (33.3%) |
| ≥1/2 | 12 (75.0%) | 4 (30.8%) | 10 (66.7%) |
| FIGO 2023 stage, n (%) | |||
| Early (I+II) | 12 (75.0%) | 10 (76.9%) | 5 (33.3%) |
| Advanced (III+IV) | 4 (25.0%) | 3 (23.1%) | 10 (66.7%) |
| Distant metastasis, n (%) | |||
| Present | 1 (6.3%) | 1 (7.7%) | 5 (33.3%) |
| Absent | 15 (93.7%) | 12 (92.3%) | 10 (66.7%) |
| Lymph node metastasis, n (%) | |||
| Present (n = 9) | |||
| ITCs | 1 (6.7%) | 0 (0%) | 0 (0%) |
| Micro-metastasis | 2 (13.3%) | 0 (0%) | 2 (18.2%) |
| Macro-metastasis | 1 (6.7%) | 1 (8.3%) | 2 (18.2%) |
| Absent (n = 29) | 11 (73.3%) | 11 (91.7%) | 7 (63.6%) |
| Uterine cervical invasion, n (%) | |||
| Present | 2 (12.5%) | 2 (15.4%) | 2 (13.3%) |
| Absent | 14 (87.5%) | 11 (84.6%) | 13 (86.7%) |
| Peritoneal cytology, n (%) | |||
| Positive | 1 (6.3%) | 1 (7.7%) | 8 (53.5%) |
| Negative | 15 (93.7%) | 12 (92.3%) | 7 (46.7%) |
| Lymphovascular invasion, n (%) | |||
| None | 6 (37.5%) | 10 (76.9%) | 7 (46.7%) |
| Focal | 4 (25.0%) | 2 (15.4%) | 3 (20.0%) |
| Substantial | 6 (37.5%) | 1 (7.7%) | 5 (33.3%) |
| Hysterectomy, n (%) | |||
| Yes | 16 (100%) | 13 (100%) | 15 (100%) |
| No | 0 (0%) | 0 (0%) | 0 (0%) |
| Lymphadenectomy, n (%) | |||
| Yes | 15 (93.8%) | 13 (100%) | 13 (86.7%) |
| No | 1 (6.2%) | 0 (0%) | 2 (13.3%) |
| Recurrence, n (%) | |||
| Yes (n = 10) | 0 (0%) | 3 (23.1%) | 7 (58.3%) |
| No (n = 31) | 16 (100%) | 10 (76.9%) | 5 (41.7%) |
| Low-Grade Endometrial Cancer with Wild-Type p53 Expression (n = 16) | Low-Grade Endometrial Cancer with Abnormal p53 Expression (n = 13) | High-Grade Endometrial Cancer (n = 15) | |
|---|---|---|---|
| L1CAM immunohistochemical scoring, n (%) | |||
| 0 | 10 (62.5%) | 7 (53.8%) | 0 (0%) |
| 1 | 6 (37.5%) | 4 (30.8%) | 1 (6.7%) |
| 2 | 0 (0%) | 1 (7.7%) | 5 (33.3%) |
| 3 | 0 (0%) | 1 (7.7%) | 9 (60.0%) |
| L1CAM expression, n (%) | |||
| positive | 0 (0%) | 2 (15.4%) * | 14 (93.3%) * |
| negative | 16 (100%) | 11 (84.6%) * | 1 (6.7%) * |
| Low-Grade Endometrial Cancer with Wild-Type p53 Expression (n = 16) | Low-Grade Endometrial Cancer with Abnormal p53 Expression (n = 13) | High-Grade Endometrial Cancer (n = 15) | |
|---|---|---|---|
| p21 immunohistochemical expression, n (%) | |||
| positive | 13 (81.3%) * | 6 (46.2%) * | 4 (26.7%) |
| negative | 3 (18.7%) * | 7 (53.8%) * | 11 (73.3%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hachisuga, K.; Kawakami, M.; Tomonobe, H.; Maenohara, S.; Kodama, K.; Yagi, H.; Yasunaga, M.; Onoyama, I.; Asanoma, K.; Yahata, H.; et al. Low-Grade Endometrial Cancer with Abnormal p53 Expression as a Separate Clinical Entity: Insights from RNA Sequencing and Immunohistochemistry. Diagnostics 2025, 15, 671. https://doi.org/10.3390/diagnostics15060671
Hachisuga K, Kawakami M, Tomonobe H, Maenohara S, Kodama K, Yagi H, Yasunaga M, Onoyama I, Asanoma K, Yahata H, et al. Low-Grade Endometrial Cancer with Abnormal p53 Expression as a Separate Clinical Entity: Insights from RNA Sequencing and Immunohistochemistry. Diagnostics. 2025; 15(6):671. https://doi.org/10.3390/diagnostics15060671
Chicago/Turabian StyleHachisuga, Kazuhisa, Minoru Kawakami, Hiroshi Tomonobe, Shoji Maenohara, Keisuke Kodama, Hiroshi Yagi, Masafumi Yasunaga, Ichiro Onoyama, Kazuo Asanoma, Hideaki Yahata, and et al. 2025. "Low-Grade Endometrial Cancer with Abnormal p53 Expression as a Separate Clinical Entity: Insights from RNA Sequencing and Immunohistochemistry" Diagnostics 15, no. 6: 671. https://doi.org/10.3390/diagnostics15060671
APA StyleHachisuga, K., Kawakami, M., Tomonobe, H., Maenohara, S., Kodama, K., Yagi, H., Yasunaga, M., Onoyama, I., Asanoma, K., Yahata, H., Oda, Y., & Kato, K. (2025). Low-Grade Endometrial Cancer with Abnormal p53 Expression as a Separate Clinical Entity: Insights from RNA Sequencing and Immunohistochemistry. Diagnostics, 15(6), 671. https://doi.org/10.3390/diagnostics15060671