
Immunohistochemical Evaluation of the Tumor Immune Microenvironment in Pancreatic Ductal Adenocarcinoma
 , ,
, ,  ,
,
Abstract
1. Introduction
2. Materials and Methods
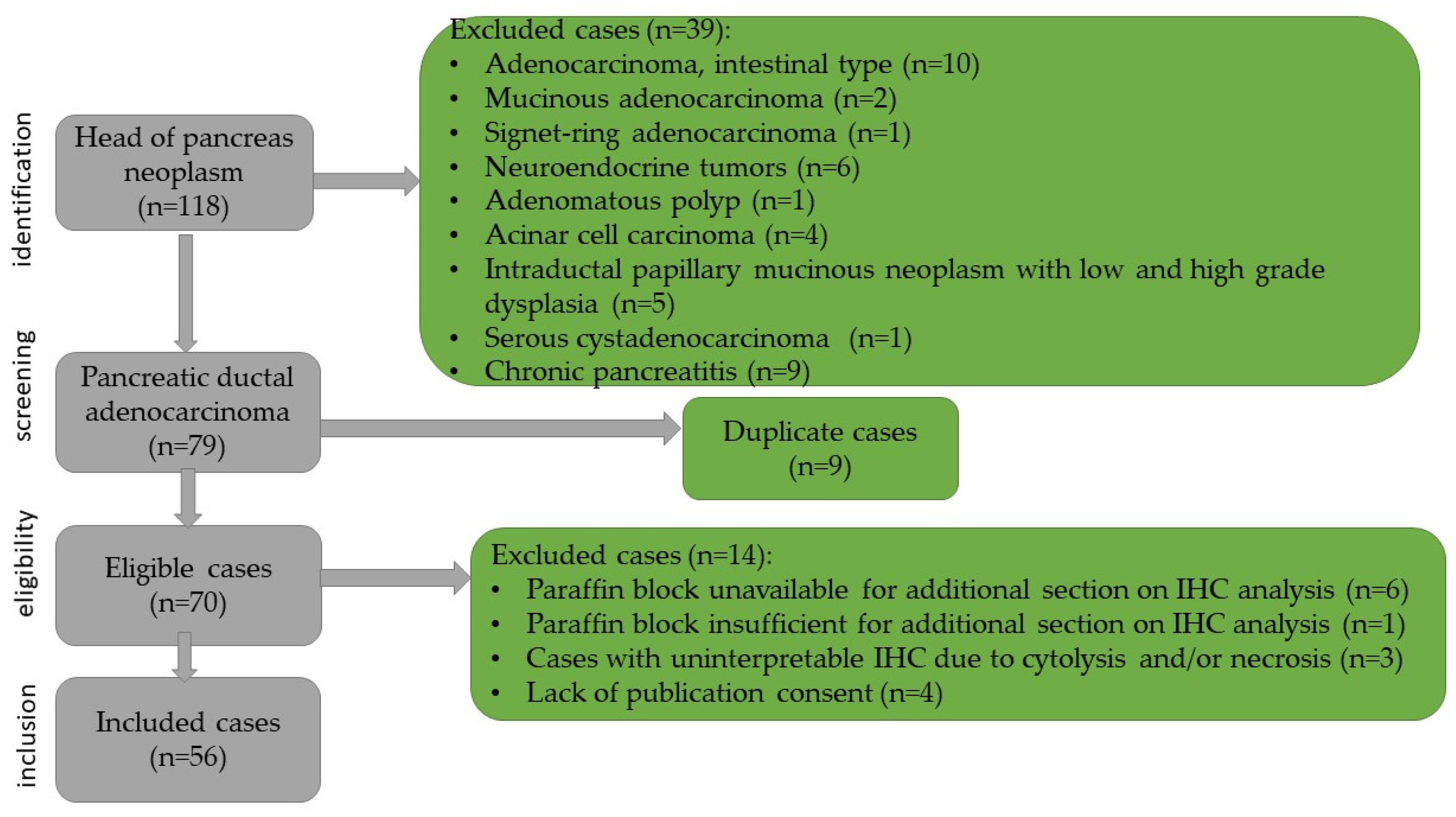
2.1. Patient Selection and Inclusion Criteria
2.2. Ethical Considerations
2.3. Laboratory Technique
2.4. Endpoints
2.5. Statistical Plan
3. Results
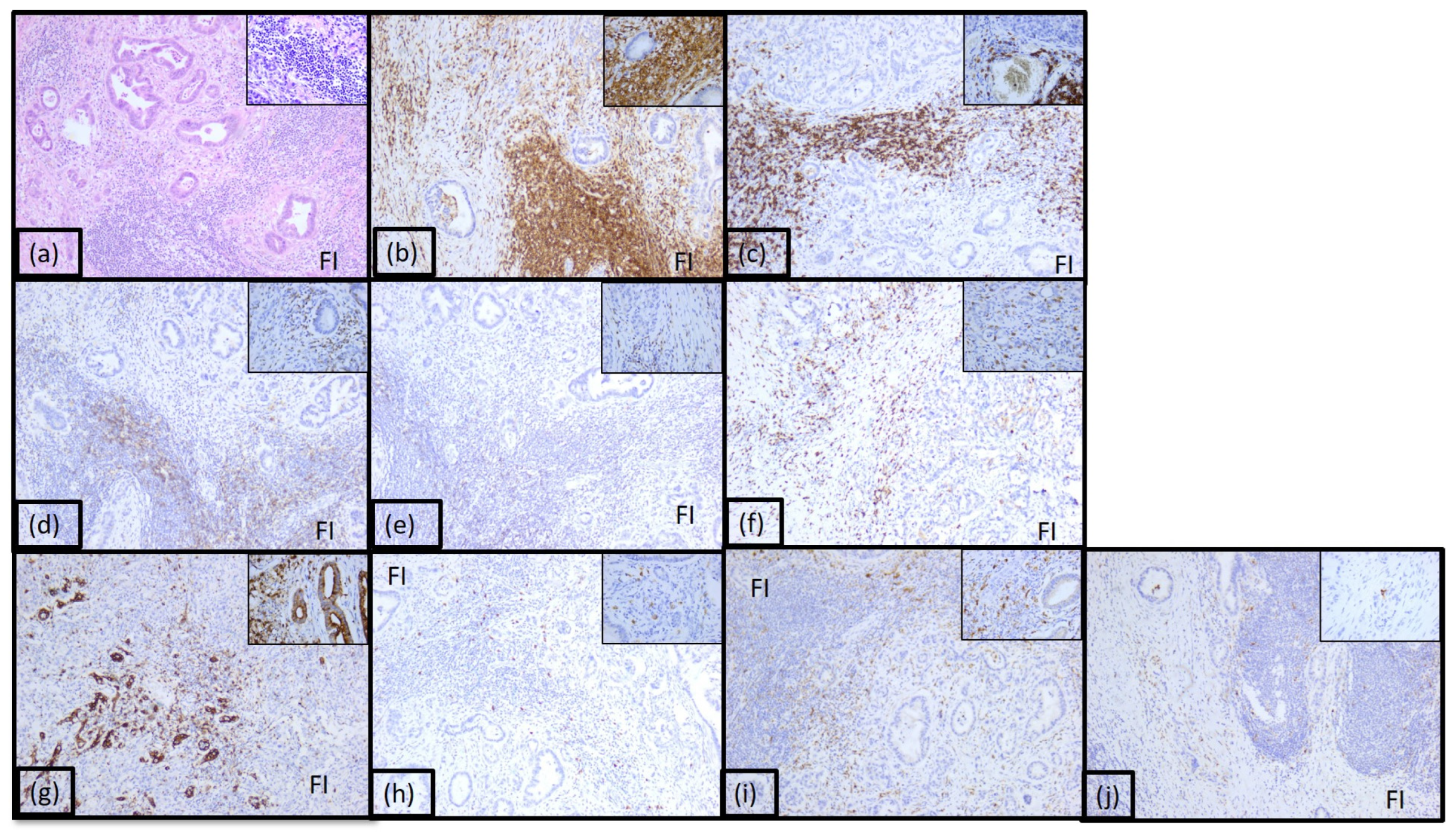
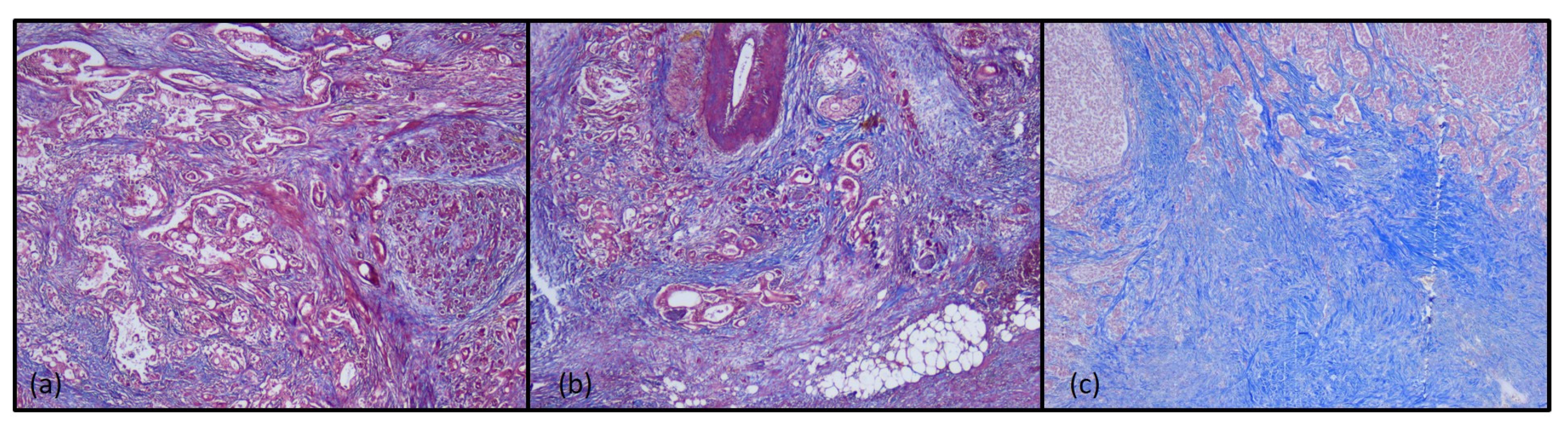
3.1. Histopathological Findings
3.2. Descriptive Statistics
3.3. Analysis of the Complications
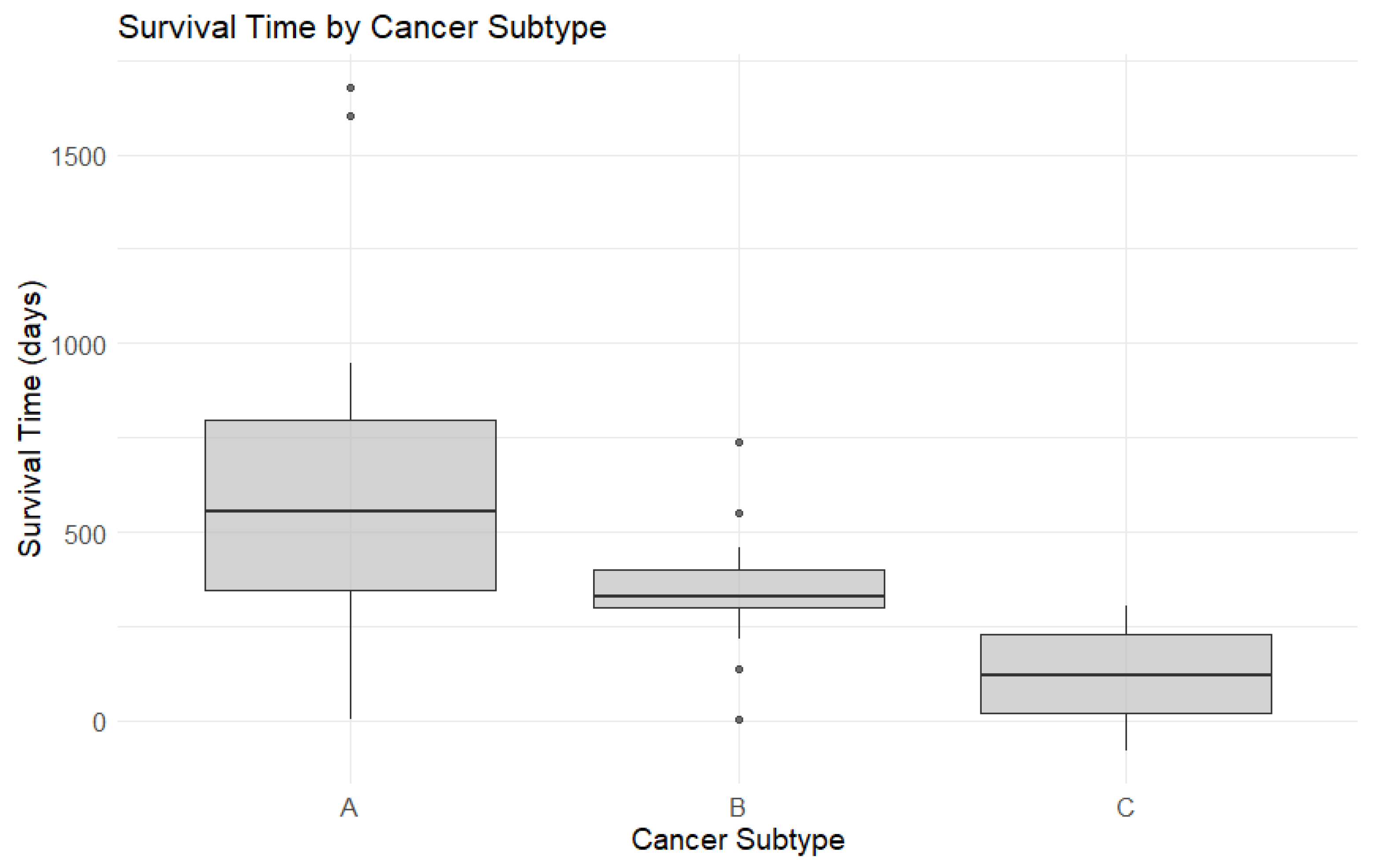
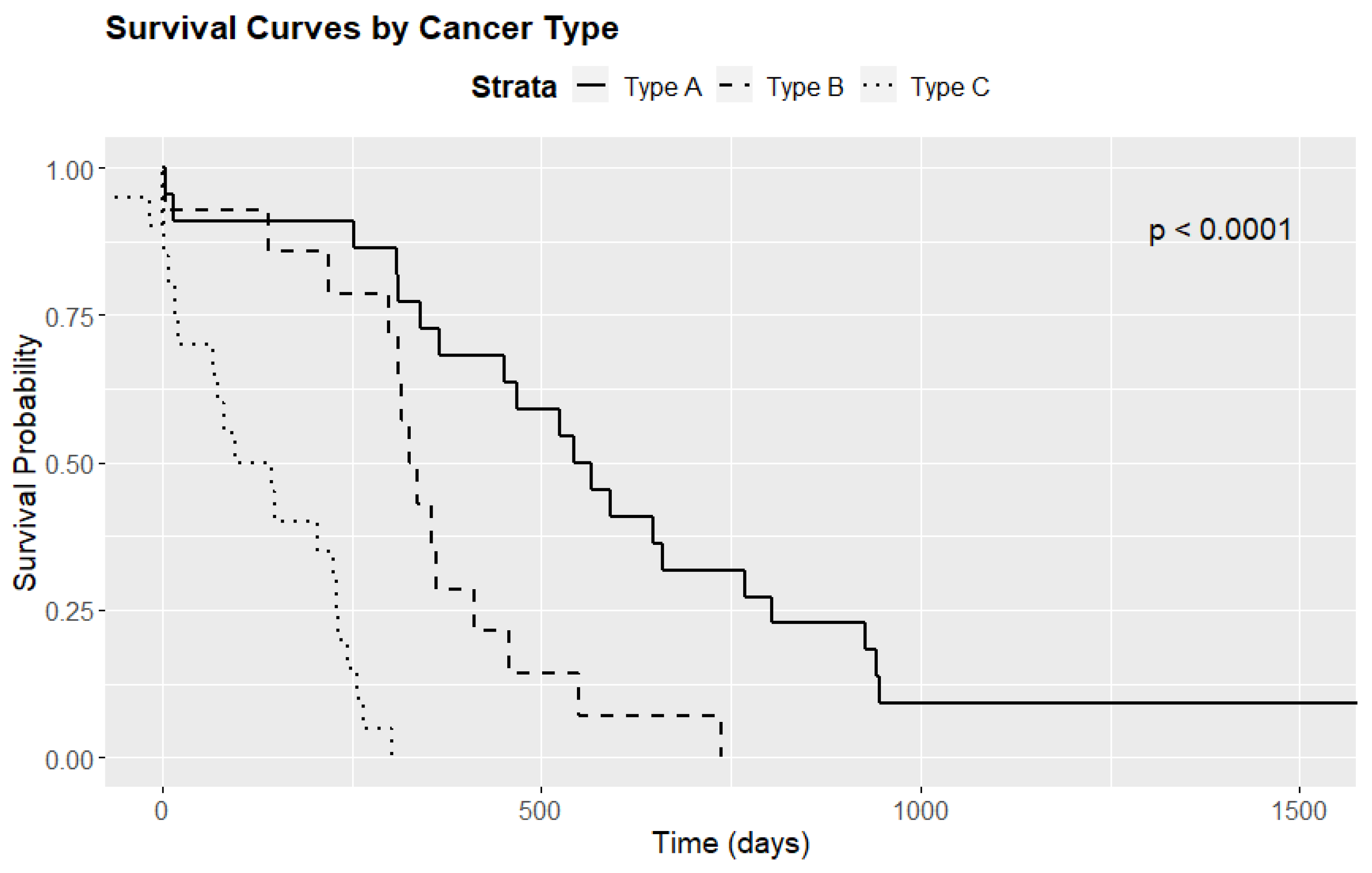
3.4. Survival Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Halbrook, C.J.; Lyssiotis, C.A.; di Magliano, M.P.; Maitra, A. Pancreatic cancer: Advances and challenges. Cell 2023, 186, 1729–1754. [Google Scholar] [CrossRef] [PubMed]
- Hu, J.X.; Zhao, C.F.; Chen, W.B.; Liu, Q.C.; Li, Q.W.; Lin, Y.Y.; Gao, F. Pancreatic cancer: A review of epidemiology, trend, and risk factors. World J. Gastroenterol. 2021, 27, 4298–4321. [Google Scholar] [CrossRef] [PubMed]
- Huang, J.; Lok, V.; Ngai, C.H.; Zhang, L.; Yuan, J.; Lao, X.Q.; Ng, K.; Chong, C.; Zheng, Z.J.; Wong, M.C.S. Worldwide Burden of, Risk Factors for, and Trends in Pancreatic Cancer. Gastroenterology 2021, 160, 744–754. [Google Scholar] [CrossRef] [PubMed]
- Dyba, T.; Randi, G.; Bray, F.; Martos, C.; Giusti, F.; Nicholson, N.; Gavin, A.; Flego, M.; Neamtiu, L.; Dimitrova, N.; et al. The European cancer burden in 2020: Incidence and mortality estimates for 40 countries and 25 major cancers. Eur. J. Cancer 2021, 157, 308–347. [Google Scholar] [CrossRef]
- Sharma, A.; Chari, S.T. Pancreatic cancer and diabetes mellitus. Curr. Treat. Options Gastroenterol. 2018, 16, 466–478. [Google Scholar] [CrossRef]
- Pandol, S.J.; Apte, M.V.; Wilson, J.S.; Gukovskaya, A.S.; Edderkaoui, M. The burning question: Why is smoking a risk factor for pancreatic cancer? Pancreatology 2012, 12, 344–349. [Google Scholar] [CrossRef]
- Bogumil, D.; Stram, D.; Preston, D.L.; Pandol, S.J.; Wu, A.H.; McKean-Cowdin, R.; Conti, D.V.; Setiawan, V.W. Excess pancreatic cancer risk due to smoking and modifying effect of quitting smoking: The Multiethnic Cohort Study. Cancer Causes Control 2024, 35, 541–548. [Google Scholar] [CrossRef]
- National Cancer Institute. Pancreatic Cancer. Available online: https://www.cancer.gov/types/pancreatic (accessed on 25 May 2022).
- Wong, W.; Raufi, A.G.; Safyan, R.A.; Bates, S.E.; Manji, G.A. BRCA mutations in pancreas cancer: Spectrum, current management, challenges and future prospects. Cancer Manag. Res. 2020, 12, 2731–2742. [Google Scholar] [CrossRef]
- Maire, F.; Micard, S.; Hammel, P.; Voitot, H.; Lévy, P.; Cugnenc, P.-H.; Ruszniewski, P.; Puig, P.L. Differential diagnosis between chronic pancreatitis and pancreatic cancer: Value of the detection of KRAS2 mutations in circulating DNA. Br. J. Cancer 2002, 87, 551–554. [Google Scholar] [CrossRef]
- Kolbeinsson, H.M.; Chandana, S.; Wright, G.P.; Chung, M. Pancreatic cancer: A review of current treatment and novel therapies. J. Investig. Surg. 2023, 36, 2129884. [Google Scholar] [CrossRef]
- Nakaoka, K.; Ohno, E.; Kawabe, N.; Kuzuya, T.; Funasaka, K.; Nakagawa, Y.; Nagasaka, M.; Ishikawa, T.; Watanabe, A.; Tochio, T.; et al. Current status of the diagnosis of early-stage pancreatic ductal adenocarcinoma. Diagnostics 2023, 13, 215. [Google Scholar] [CrossRef] [PubMed]
- Bekkali, N.L.H.; Oppong, K.W. Pancreatic ductal adenocarcinoma epidemiology and risk assessment: Could we prevent? Possibility for an early diagnosis. Endosc. Ultrasound 2017, 6, 58–61. [Google Scholar]
- Siegel, R.L.; Giaquinto, A.N.; Jemal, A. Cancer statistics, 2024. CA A Cancer J Clin 2024, 74, 12–49. [Google Scholar] [CrossRef]
- Rahib, L.; Smith, B.D.; Aizenberg, R.; Rosenzweig, A.B.; Fleshman, J.M.; Matrisian, L.M. Projecting cancer incidence and deaths to 2030: The unexpected burden of thyroid, liver, and pancreas cancers in the United States. Cancer Res. 2014, 74, 2913–2921. [Google Scholar] [CrossRef]
- Park, W.; Chawla, A.; O’Reilly, E.M. Pancreatic Cancer: A Review. JAMA 2021, 326, 851–862. [Google Scholar] [CrossRef]
- Heinrich, S.; Lang, H. Neoadjuvant therapy of pancreatic cancer: Definitions and benefits. Int. J. Mol. Sci. 2017, 18, 1622. [Google Scholar] [CrossRef]
- Qian, Y.; Gong, Y.; Fan, Z.; Luo, G.; Huang, Q.; Deng, S.; Cheng, H.; Jin, K.; Ni, Q.; Yu, X.; et al. Molecular alterations and targeted therapy in pancreatic ductal adenocarcinoma. J. Hematol. Oncol. 2020, 13, 130. [Google Scholar] [CrossRef]
- Perko, N.; Mousa, S.A. Management of Pancreatic Cancer and Its Microenvironment: Potential Impact of Nano-Targeting. Cancers 2022, 14, 2879. [Google Scholar] [CrossRef]
- Brown, Z.J.; Cloyd, J.M. Surgery for pancreatic cancer: Recent progress and future directions. Hepatobiliary Surg. Nutr. 2021, 10, 376–378. [Google Scholar] [CrossRef]
- Lei, Z.N.; Tian, Q.; Teng, Q.X.; Wurpel, J.N.D.; Zeng, L.; Pan, Y.; Chen, Z.S. Understanding and targeting resistance mechanisms in cancer. MedComm 2023, 4, 265. [Google Scholar] [CrossRef]
- Peterson, C.; Denlinger, N.; Yang, Y. Recent Advances and Challenges in Cancer Immunotherapy. Cancers 2022, 14, 3972. [Google Scholar] [CrossRef] [PubMed]
- Grossberg, A.J.; Chu, L.C.; Deig, C.R.; Fishman, E.K.; Hwang, W.L.; Maitra, A.; Marks, D.L.; Mehta, A.; Nabavizadeh, N.; Simeone, D.M.; et al. Multidisciplinary standards of care and recent progress in pancreatic ductal adenocarcinoma. CA Cancer J. Clin. 2020, 70, 375–403. [Google Scholar] [CrossRef]
- Hartupee, C.; Nagalo, B.M.; Chabu, C.Y.; Tesfay, M.Z.; Coleman-Barnett, J.; West, J.T.; Moaven, O. Pancreatic cancer tumor microenvironment is a major therapeutic barrier and target. Front. Immunol. 2024, 15, 1287459. [Google Scholar] [CrossRef] [PubMed]
- Ullman, N.A.; Burchard, P.R.; Dunne, R.F.; Linehan, D.C. Immunologic Strategies in Pancreatic Cancer: Making Cold Tumors Hot. J. Clin. Oncol. 2022, 40, 2789–2805. [Google Scholar] [CrossRef] [PubMed]
- Liu, S.L.; Cao, S.G.; Li, Y.; Sun, B.; Chen, D.; Wang, D.S.; Zhou, Y.B. Pancreatic stellate cells facilitate pancreatic cancer cell viability and invasion. Oncol. Lett. 2019, 17, 2057–2062. [Google Scholar] [CrossRef]
- Miyabayashi, K.; Ijichi, H.; Fujishiro, M. The Role of the Microbiome in Pancreatic Cancer. Cancers 2022, 14, 4479. [Google Scholar] [CrossRef]
- MacCurtain, B.M.; Quirke, N.P.; Thorpe, S.D.; Gallagher, T.K. Pancreatic Ductal Adenocarcinoma: Relating Biomechanics and Prognosis. J. Clin. Med. 2021, 10, 2711. [Google Scholar] [CrossRef]
- Ho, W.J.; Jaffee, E.M.; Zheng, L. The Tumour Microenvironment in Pancreatic Cancer—Clinical Challenges and Opportunities. Nat. Rev. Clin. Oncol. 2020, 17, 527–540. [Google Scholar] [CrossRef]
- Szczepanski, J.M.; Rudolf, M.A.; Shi, J. Clinical Evaluation of the Pancreatic Cancer Microenvironment: Opportunities and Challenges. Cancers 2024, 16, 794. [Google Scholar] [CrossRef]
- Kiryu, S.; Ito, Z.; Suka, M.; Bito, T.; Kan, S.; Uchiyama, K.; Saruta, M.; Hata, T.; Takano, Y.; Fujioka, S.; et al. Prognostic value of immune factors in the tumor microenvironment of patients with pancreatic ductal adenocarcinoma. BMC Cancer 2021, 21, 1197. [Google Scholar] [CrossRef]
- Melzer, M.K.; Arnold, F.; Stifter, K.; Zengerling, F.; Azoitei, N.; Seufferlein, T.; Bolenz, C.; Kleger, A. An Immunological Glance on Pancreatic Ductal Adenocarcinoma. Int. J. Mol. Sci. 2020, 8, 3345. [Google Scholar] [CrossRef] [PubMed]
- Miksch, R.C.; Schoenberg, M.B.; Weniger, M.; Bösch, F.; Ormanns, S.; Mayer, B.; Werner, J.; Bazhin, A.V.; D’Haese, J.G. Prognostic Impact of Tumor-Infiltrating Lymphocytes and Neutrophils on Survival of Patients with Upfront Resection of Pancreatic Cancer. Cancers 2019, 11, 39. [Google Scholar] [CrossRef] [PubMed]
- Ino, Y.; Oguro, S.; Yamazaki-Itoh, R.; Hori, S.; Shimada, K.; Hiraoka, N. Reliable Evaluation of Tumor-Infiltrating Lymphocytes in Pancreatic Cancer Tissue Biopsies. Oncotarget 2019, 10, 1149–1159. [Google Scholar] [CrossRef] [PubMed]
- Tahkola, K.; Leppänen, J.; Ahtiainen, M.; Väyrynen, J.; Haapasaari, K.-M.; Karttunen, T.; Kellokumpu, I.; Helminen, O.; Böhm, J. Immune Cell Score in Pancreatic Cancer-Comparison of Hotspot and Whole-Section Techniques. Virchows Arch. Int. J. Pathol. 2019, 474, 691–699. [Google Scholar] [CrossRef]
- Carstens, J.L.; Correa de Sampaio, P.; Yang, D.; Barua, S.; Wang, H.; Rao, A.; Allison, J.P.; LeBleu, V.S.; Kalluri, R. Spatial Computation of Intratumoral T Cells Correlates with Survival of Patients with Pancreatic Cancer. Nat. Commun. 2017, 8, 15095. [Google Scholar] [CrossRef]
- Balachandran, V.P.; Łuksza, M.; Zhao, J.N.; Makarov, V.; Moral, J.A.; Remark, R.; Herbst, B.; Askan, G.; Bhanot, U.; Senbabaoglu, Y.; et al. Identification of Unique Neoantigen Qualities in Long-Term Survivors of Pancreatic Cancer. Nature 2017, 551, 512–516. [Google Scholar] [CrossRef]
- Hou, Y.C.; Chao, Y.J.; Hsieh, M.H.; Tung, H.L.; Wang, H.C.; Shan, Y.S. Low CD8+ T Cell Infiltration and High PD-L1 Expression Are Associated with Level of CD44+/CD133+ Cancer Stem Cells and Predict an Unfavorable Prognosis in Pancreatic Cancer. Cancers 2019, 11, 541. [Google Scholar] [CrossRef]
- Castino, G.F.; Cortese, N.; Capretti, G.; Serio, S.; Di Caro, G.; Mineri, R.; Magrini, E.; Grizzi, F.; Cappello, P.; Novelli, F.; et al. Spatial Distribution of B Cells Predicts Prognosis in Human Pancreatic Adenocarcinoma. Oncoimmunology 2016, 5, 1085147. [Google Scholar] [CrossRef]
- Marin, M.A.; Closca, R.M.; Marin, A.; Rakitovan, M.; Nicoara, A.; Poenaru, M.; Militaru, M.; Baderca, F. Clinical, Epidemiological, Morphological, and Immunohistochemical Aspects of Nasopharyngeal Carcinoma—4-Year Retrospective Study in the Western Part of Romania. Diagnostics 2024, 14, 722. [Google Scholar] [CrossRef]
- Trandafir, C.M.; Closca, R.M.; Poenaru, M.; Sarau, O.S.; Sarau, C.A.; Rakitovan, M.; Baderca, F.; Sima, L.V. Morphological and Immunohistochemical Aspects with Prognostic Implications and Therapeutic Targets of Primary Sinonasal Mucosal Melanoma: A Retrospective Study. Cancers 2024, 16, 2863. [Google Scholar] [CrossRef]
- Yang, S.; Liu, Q.; Liao, Q. Tumor-Associated Macrophages in Pancreatic Ductal Adenocarcinoma: Origin, Polarization, Function, and Reprogramming. Front. Cell Dev. Biol. 2021, 8, 607209. [Google Scholar] [CrossRef] [PubMed]
- Griesmann, H.; Drexel, C.; Milosevic, N.; Sipos, B.; Rosendahl, J.; Gress, T.M.; Michl, P. Pharmacological macrophage inhibition decreases metastasis formation in a genetic model of pancreatic cancer. Gut 2017, 66, 1278–1285. [Google Scholar] [CrossRef] [PubMed]
- Poyia, F.; Neophytou, C.M.; Christodoulou, M.I.; Papageorgis, P. The Role of Tumor Microenvironment in Pancreatic Cancer Immunotherapy: Current Status and Future Perspectives. Int. J. Mol. Sci. 2024, 25, 9555. [Google Scholar] [CrossRef] [PubMed]
- Nielsen, S.R.; Strøbech, J.E.; Horton, E.R.; Jackstadt, R.; Laitala, A.; Bravo, M.C.; Maltese, G.; Jensen, A.R.D.; Reuten, R.; Rafaeva, M.; et al. Suppression of tumor-associated neutrophils by lorlatinib attenuates pancreatic cancer growth and improves treatment with immune checkpoint blockade. Nat. Commun. 2021, 12, 3414. [Google Scholar] [CrossRef]
- Plesca, I.; Benešová, I.; Beer, C.; Sommer, U.; Müller, L.; Wehner, R.; Heiduk, M.; Aust, D.; Baretton, G.; Bachmann, M.P.; et al. Clinical Significance of Tumor-Infiltrating Conventional and Plasmacytoid Dendritic Cells in Pancreatic Ductal Adenocarcinoma. Cancers 2022, 14, 1216. [Google Scholar] [CrossRef]
- Lichterman, J.N.; Reddy, S.M. Mast Cells: A New Frontier for Cancer Immunotherapy. Cells 2021, 10, 1270. [Google Scholar] [CrossRef]
- Guo, X.; Zhai, L.; Xue, R.; Shi, J.; Zeng, Q.; Gao, C. Mast Cell Tryptase Contributes to Pancreatic Cancer Growth through Promoting Angiogenesis via Activation of Angiopoietin-1. Int. J. Mol. Sci. 2016, 17, 834. [Google Scholar] [CrossRef]
- Ammendola, M.; Currò, G.; Laface, C.; Zuccalà, V.; Memeo, R.; Luposella, F.; Laforgia, M.; Zizzo, N.; Zito, A.; Loisi, D.; et al. Mast Cells Positive for c-Kit Receptor and Tryptase Correlate with Angiogenesis in Cancerous and Adjacent Normal Pancreatic Tissue. Cells 2021, 10, 444. [Google Scholar] [CrossRef]
- Tabbekh, M.; Mokrani-Hammani, M.B.; Bismuth, G.; Mami-Chouaib, F. T cell modulatory properties of CD5 and its role in antitumor immune responses. Oncoimmunology 2013, 2, e22841. [Google Scholar] [CrossRef]
- Meierhofer, C.; Fuegger, R.; Biebl, M.; Schoefl, R. Pancreatic Fistulas: Current Evidence and Strategy—A Narrative Review. J. Clin. Med. 2023, 12, 5046. [Google Scholar] [CrossRef]
- Bassi, C.; Dervenis, C.; Butturini, G.; Fingerhut, A.; Yeo, C.; Izbicki, J.; Neoptolemos, J.; Sarr, M.; Traverso, W.; Buchler, M.; et al. Postoperative pancreatic fistula: An international study group (ISGPF) definition. Surgery 2005, 138, 8–13. [Google Scholar] [CrossRef] [PubMed]
- Weniger, M.; Honselmann, K.C.; Liss, A.S. The extracellular matrix and pancreatic cancer: A complex relationship. Cancers 2018, 10, 316. [Google Scholar] [CrossRef] [PubMed]
- Suklabaidya, S.; Dash, P.; Das, B.; Suresh, V.; Sasmal, P.K.; Senapati, S. Experimental models of pancreatic cancer desmoplasia. Lab. Investig. 2018, 98, 27–40. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Antibody | Substrate | Clone | Dilution | Cell Type |
|---|---|---|---|---|
| LCA 1 | Monoclonal, mouse | X16/99 | 1:40 | Lymphocyte |
| CD3 2 | Monoclonal, mouse | LN10 | 1:500 | T lymphocyte |
| CD4 3 | Monoclonal, mouse | 4B12 | 1:100 | T helper lymphocyte |
| CD8 4 | Monoclonal, mouse | 4B11 | 1:500 | T cytotoxic lymphocyte |
| CD20 5 | Monoclonal, mouse | L26 | RTU 6 | B lymphocyte |
| CD68 7 | Monoclonal, mouse | 514H12 | 1:100 | Macrophage |
| CD1a 8 | Monoclonal, mouse | MTB1 | RTU | Dendritic cell |
| CD117 9 | Monoclonal, rabbit | EP10 | 1:200 | Mast cell |
| Tumor Type | ImC 1 | Ly 2 LCA+ | LyB CD20+ | LyT CD4+ | T CD8+ | T CD3+ | T CD5+ | Mph 3 CD68+ | Mast 4 CD117+ | DCs 5 CD1a+ | Other Cells | MTS 12 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Type A | +++ 6 | 60% | 35% | 10% | 5% | 30% | 20% | 20% | 10% | 5% | 5% GN 7 | + |
| Type B | ++ 8 | 55% | 15% | 10% | 40% | 15% | 20% | 20% | 5% | 0% | 10% Pl 9, 5% GN, 5% Eo 10 | ++ |
| Type C | + 11 | 90% | 60% | 5% | 20% | 5% | 10% | <0.1% | <0.1% | 0% | 10% Pl | +++ |
| Variable | All Patients (n = 56) | Type A (n = 22) | Type B (n = 14) | Type C (n = 20) | p-Value *,** | |
|---|---|---|---|---|---|---|
| Age (years) (a) | 64 (59–70) | 64 (61.25–67) | 59 (53.5–69.75) | 65 (61–71.25) | 0.633 | |
| Survival time (days) (a) | 310.5 (142.8–529.2) | 553.5 (346.2–795.8) | 331.5 (301.5–399.2) | 120.5 (19.25–229.75) | <0.001 ** | |
| Sex (female) (b) | 24 (42.9%) | 11 (50%) | 3 (21.4%) | 10 (50%) | 0.174 | |
| Preoperatory biliary stent (b) | 29 (51.8%) | 11 (50%) | 9 (64.3%) | 9 (45%) | 0.529 | |
| Classic technique (b) | 26 (46.4%) | 6 (27.27%) | 5 (37.71%) | 15 (75%) | 0.005 ** | |
| Modified technique (b) | 30 (53.6%) | 16 (72.7%) | 9 (64.3%) | 5 (25%) | ||
| Pancreatic fistula (b) | 20 (35.7%) | 1 (4.55%) | 8 (57.14%) | 11 (55%) | <0.001 ** | |
| Biliary fistula (b) | 2 (3.6%) | 2 (9.09%) | - | - | 0.2 | |
| Acute pancreatitis (b) | 20 (35.7%) | 1 (4.55%) | 3 (21.43%) | 16 (80%) | <0.001 ** | |
| Stage (b) | ||||||
| IA | 4 (7.1%) | 2 (9.1%) | - | 2 (10%) | 0.08 | |
| IB | 4 (7.1%) | 3 (13.6%) | 1 (7.1%) | - | ||
| IIA | 11 (19.6%) | 1 (4.6%) | 3 (21.4%) | 7 (35%) | ||
| IIB | 29 (51.8%) | 13 (59.1%) | 10 (71.4%) | 6 (30%) | ||
| III | 4 (7.1%) | 2 (9.1%) | - | 2 (10%) | ||
| IV | 4 (7.1%) | 1 (4.6%) | - | 3 (15%) | ||
| T1 (b) | 8 (14.3%) | 4 (18.2%) | - | 4 (20%) | 0.09 | |
| T2 (b) | 14 (25%) | 7 (31.8%) | 3 (21.4%) | 4 (20%) | ||
| T3 (b) | 31 (55.4%) | 8 (36.4%) | 11 (78.6%) | 12 (60%) | ||
| T4 (b) | 3 (5.4%) | 3 (13.64%) | - | - | ||
| N0 (b) | 14 (25%) | 2 (9.1%) | 3 (21.4%) | 9 (45%) | 0.144 | |
| N1 (b) | 31 (55.4%) | 13 (59.1%) | 9 (64.3%) | 9 (45%) | ||
| N2 (b) | 1 (1.8%) | 1 (4.6%) | - | - | ||
| NX (b) | 10 (17.9%) | 6 (27.3%) | 2 (14.3%) | 2 (10%) | ||
| M0 (b) | 17 (30.4%) | 6 (27.3%) | 3 (21.4%) | 8 (40%) | 0.226 | |
| M1 (b) | 4 (7.1%) | 1 (4.6%) | - | 3 (15%) | ||
| MX (b) | 35 (62.5%) | 15 (68.2%) | 11 (78.6%) | 9 (45%) | ||
| Variable | OR | SD | 95% CI | p Value |
|---|---|---|---|---|
| Pancreatic fistulas ~ type + grade + age + sex (a) Nagelkerke R2 = 0.58 | ||||
| Intercept | −4.01 | 1.66 | −7.9, −1.02 | 0.015 * |
| Immunotype B | 3.68 | 1.23 | 1.59, 6.81 | 0.003 ** |
| Immunotype C | 3.94 | 1.23 | 1.89, 7.07 | 0.001 ** |
| Grade G2 | −0.3 | 1.43 | - | 0.834 |
| Grade G3 | −18.84 | 1906 | - | 0.992 |
| Sex (Male) | 1.81 | 0.86 | 1.22, 38.94 | 0.037 * |
| Acute pancreatitis ~ type + stage + grade + age + sex (b) Nagelkerke R2 = 0.88 | ||||
| Intercept | −88.82 | 10178 | - | 0.993 |
| Immunotype B | 7.25 | 4.28 | 1.56, 20.81 | 0.09 |
| Immunotype C | 44.98 | 6487 | - | 0.995 |
| Stage IB | 46.04 | 6487 | - | 0.994 |
| Stage IIA | 44.21 | 6487 | - | 0.995 |
| Stage IIB | 39.45 | 6487 | - | 0.995 |
| Stage III | 1.27 | 6.46 | - | 0.844 |
| Stage IV | 0.39 | 2.99 | - | 0.895 |
| Grade G2 | 24.74 | 4529 | - | 0.995 |
| Grade G3 | 25.3 | 4259 | - | 0.996 |
| Age | 0.29 | 0.142 | 0.072, 0.68 | 0.042 * |
| Sex (Male) | −4.84 | 3.21 | - | 0.132 |
| Variable | All Patients (N = 56) | Type A (N = 22) | Type B (N = 14) | Type C (N = 20) |
|---|---|---|---|---|
| OS 28 days | 84% | 91% | 93% | 75% |
| OS 365 days | 34% | 68% | 29% | - |
| OS 730 days | 13% | 32% | 7% | - |
| OS 1095 days | 3.6% | 9% | - | - |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Breaza, G.M.; Closca, R.M.; Cindrea, A.C.; Hut, F.E.; Cretu, O.; Sima, L.V.; Rakitovan, M.; Zara, F. Immunohistochemical Evaluation of the Tumor Immune Microenvironment in Pancreatic Ductal Adenocarcinoma. Diagnostics 2025, 15, 646. https://doi.org/10.3390/diagnostics15050646
Breaza GM, Closca RM, Cindrea AC, Hut FE, Cretu O, Sima LV, Rakitovan M, Zara F. Immunohistochemical Evaluation of the Tumor Immune Microenvironment in Pancreatic Ductal Adenocarcinoma. Diagnostics. 2025; 15(5):646. https://doi.org/10.3390/diagnostics15050646
Chicago/Turabian StyleBreaza, Gelu Mihai, Raluca Maria Closca, Alexandru Cristian Cindrea, Florin Emil Hut, Octavian Cretu, Laurentiu Vasile Sima, Marina Rakitovan, and Flavia Zara. 2025. "Immunohistochemical Evaluation of the Tumor Immune Microenvironment in Pancreatic Ductal Adenocarcinoma" Diagnostics 15, no. 5: 646. https://doi.org/10.3390/diagnostics15050646
APA StyleBreaza, G. M., Closca, R. M., Cindrea, A. C., Hut, F. E., Cretu, O., Sima, L. V., Rakitovan, M., & Zara, F. (2025). Immunohistochemical Evaluation of the Tumor Immune Microenvironment in Pancreatic Ductal Adenocarcinoma. Diagnostics, 15(5), 646. https://doi.org/10.3390/diagnostics15050646