Abstract
Non-small cell lung cancer (NSCLC) is the leading cause of cancer-related mortality worldwide. Advances in tissue-based biomarkers have significantly enhanced diagnostic and therapeutic approaches in NSCLC, enabling precision medicine strategies. This review provides a comprehensive analysis of the molecular pathologist’s practical approach to assessing NSCLC biomarkers across various specimen types (liquid biopsy, broncho–alveolar lavage, transbronchial biopsy/endobronchial ultrasound-guided biopsy, and surgical specimen), including challenges such as biological heterogeneity and preanalytical variability. We discuss the role of programmed death ligand 1 (PD-L1) immunohistochemistry in predicting immunotherapy response, the practice of histopathological tumor regression grading after neoadjuvant chemoimmunotherapy, and the application of DNA- and RNA-based techniques for detecting actionable molecular alterations. Finally, we emphasize the critical need for quality management to ensure the reliability and reproducibility of biomarker testing in NSCLC.
1. Introduction
Non-small cell lung cancer (NSCLC) is the leading cause of death from cancer worldwide [1]. Lung cancer represents around 10% of cancer diagnoses and 18% of cancer deaths. While there is an overall decrease in the incidence of lung cancer, reflecting the change in smoking habits, the incidence among women and non-smokers is increasing [2]. The term NSCLC summarizes lung adenocarcinoma (LAC, derived from glandular cells), lung squamous cell carcinoma (SCC, derived from metaplastic squamous epithelium), and large cell carcinoma (LCC), which may also show neuroendocrine differentiation (LCNEC) [3]. Small cell lung cancer (SCLC), on the other hand, arises from neuroendocrine cells in the bronchial or bronchiolar epithelium, which have accumulated genetic damage upon exposure to the carcinogenic components of cigarette smoke. While around 75% of lung cancers are NSCLCs in both females and males, adenocarcinomas are more frequent in women (57% vs. 39%), while squamous cell carcinomas are more frequent in men (25% vs. 12%). Small cell carcinoma and large cell carcinoma show a similar distribution between men and women (11% vs. 9% and 8% vs. 6%) [4]. There are many recent and comprehensive reviews on the epidemiology and risk factors for lung cancer, which we will therefore not discuss here; instead, the focus of this review is the (molecular) pathologist’s practical approach to the assessment of tissue-based biomarkers in NSCLC samples (cytological specimens, liquid and tissue biopsies, or resection specimens). Of note, the stage-specific impact of predictive biomarkers may change over time: while the detection of EGFR/ALK alterations has been a prerequisite for targeted therapy in late stages of lung cancer, the potential negative predictive value of these alterations for the response to neoadjuvant chemoimmunotherapy has moved these biomarkers into early/operable disease stages [5,6].
Since the development of tissue-based biomarkers and associated therapies in NSCLC is evolving so rapidly, this review can only be a snapshot of the current “state of the art” and, obviously, to a certain extent, reflects the policies and methods from the authors’ own experience. However, we will try to not only summarize our own diagnostic approach but also reflect the current literature as well as relevant guidelines in the respective sections. Taken together, the purpose of this review is to provide a concise summary of the current state of biomarker testing in NSCLC from the pathologist’s perspective.
2. Types of Biological Specimens in Neoplastic Lung Pathology
Tissue samples from lung neoplasms can only be obtained invasively by transthoracic (CT-guided) or transbronchial (bronchoscopic) biopsy or by a surgical procedure (atypical/wedge or anatomic resection). Therefore, as much reliable information as possible has to be obtained from the sample that reaches the pathology lab, irrespective of its size, pre-analytics, or tumor cell content. If the patient is unfit for bronchoscopy or surgery, cytology from broncho–alveolar lavage (alveolar washing) or liquid biopsy from peripheral blood may represent valuable alternatives. When considering liquid biopsy, different approaches must be discerned: the isolation of circulating tumor cells (CTCs) and the detection of cell-free (tumor) DNA (cfDNA/ctDNA) in the peripheral blood. CTCs are intact, viable cells that can offer insights into both the spatial and temporal heterogeneity of tumors, as well as their biology—areas that ctDNA mutation signatures cannot fully address. Of note, it has previously been shown that gene fusions can be reliably detected in CTCs from ALK-translocated NSCLC, predicting the clinical outcome [7]. Since CTCs and ctDNA each have distinct advantages and limitations, they have been proposed as complementary cancer biomarkers [8]. Table 1 summarizes the advantages and disadvantages of the respective types of biological specimens in neoplastic lung pathology. In this context, it should be noted that multidisciplinary discussion and planning of the diagnostic procedures that take into account the clinical state of the patient (lung function, comorbidities), the type and localization of the lesion (central vs. peripheral, parenchyma vs. lymph nodes), and the methodology of subsequent biomarker testing are the best approach to ensure that most biological information can be obtained from the respective tissue sample.
In patients who are unfit for any kind of invasive procedure, molecular imaging (the visualization of pathophysiological processes on a molecular level) might represent a valuable tool to obtain biological information in a non-invasive way [9]. One example of this is the correlation between radiomic texture features and POSTN expression levels in a preclinical model of glioblastoma [10]; another example is the correlation between FAPi PET uptake and FAP protein expression in interstitial lung disease [11,12].

Table 1.
Advantages and disadvantages of types of biological specimens in neoplastic lung pathology.
3. Programmed Death Ligand 1 (PD-L1)
Programmed death ligand 1 (PD-L1) is expressed on tumor cells and acts as a suppressor of the antitumoral immune response through interaction with PD-1, which is expressed on immune cells [20,21]. These would normally recognize and attack neoantigen-presenting tumor cells. This can be therapeutically exploited by inhibiting PD-L1 through PD-L1-binding antibodies, thus giving the patient’s immune system the chance to recognize and destroy the malignant cells. The effectiveness of pharmaceutical PD-L1 inhibition depends on the amount of PD-L1 on the surface of tumor cells, with PD-L1-positive tumors showing a better response to (chemo)immunotherapy compared to PD-L1-negative tumors. PD-L1 expression in tumor cells is routinely assessed by PD-L1 immunohistochemistry (IHC), for which different antibody clones and protocols are used by pathologists. Some of these are commercially available assays (SP142, SP263, 28-8, 22C3), while others are laboratory-developed tests (E1L3N) [22]. In general, large comparability studies have shown that these assays provide both comparable and reliable results, given that measures of quality assurance (e.g., ring trials) are adequately employed and rigorously followed [23,24]. Of note, all caveats that apply to the use of IHC, in general (pre-analytics, over-/underfixation, heat treatment, buffers, dilution), as well as the respective antibody clone and staining platform, should be taken into account when interpreting PD-L1 staining. External quality assurance as well as continuous monitoring can help to standardize the methodology between different laboratories [25]. However, PD-L1 staining intensities may not only vary depending on methodology but also for biological reasons. PD-L1 expression in immune cells represents IFN-γ-induced adaptive regulation and is associated with an increase in tumor-infiltrating lymphocytes and effector T cells, while high PD-L1 expression on tumor cells has been linked to epigenetic dysregulation of the PD-L1 gene [26]. Since chemotherapy reduces PD-L1 expression in tumor cells for a subset of patients [27], rebiopsy and reassessment of PD-L1 expression may be necessary to determine eligibility for immune checkpoint inhibitor therapy, but so far, there is no standardized PD-L1 testing strategy. Such a guideline should include optimal reassessment time points, the required number of biopsies, and the evaluation of surgical specimens [28].
The PD-L1 tumor proportion score (TPS) is the ratio between PD-L1-positive tumor cells and all tumor cells in the respective sample; high TP scores are associated with better response to immune checkpoint inhibitors targeting PD-1 or PD-L1 and higher overall survival in NSCLC patients [29,30]. However, the evaluation of PD-L1 staining is challenging due to biological heterogeneity, slightly different performance of antibody clones, and relevant interobserver variation [31,32]. A weighted kappa for interobserver variation between pathologists of 0.71–0.96 when assessing TPS in NSCLC has been described [33]; in the same study, up to 20% of the cases showed discordant classification as positive or negative using TPS ≥ 1% as the cutoff (0–5% when using a cutoff of TPS ≥ 50%). Other studies confirmed relatively high agreement while suggesting that training in predefined areas could improve reproducibility [34]. It has been highlighted that distinguishing “true positive” from “false-positive” artifacts can be difficult, especially in specimens with lower percentages of positive cells and faint staining [35]. This is of utmost clinical relevance since under- or overscoring might result in under- or overtreatment of NSCLC patients.
Artificial intelligence (AI)-assisted TPS scoring in NSCLC has been shown to be feasible, with results comparable to the assessment by experienced pathologists or even outperforming them [36,37]. The reproducibility and efficiency of untrained pathologists could also be improved by AI assistance [38]. However, the use of AI still does not overcome the major challenges in TPS scoring: first, traditional AI approaches rely solely on real patient data. As a result, cases that are highly relevant for training (e.g., those with a TPS of around 1% or 50%) follow a natural biological distribution and may be under-represented in training cohorts, which typically include no more than a few hundred cases. Second, the real-world training cases must be carefully annotated by real pathologists, raising the possibility of perpetuating the above-mentioned biases during AI training. There are recent alternatives to IHC when assessing PD-L1 expression: Soluble PD-1 (sPD-1) and soluble PD-L1 (sPD-L1) are present in the bloodstream as free proteins and can be quantified using enzyme-linked immunosorbent assays (ELISA). However, ELISA relies on monoclonal antibodies, which are expensive to produce and require significant time for isolation and purification [39]. PD-L1 exosomes can be detected by optical technologies such as Surface Plasmon Resonance (SPR) spectroscopy [40]. Regarding non-tissue-based methods, [18F]DK222-PET has been proposed as a non-invasive imaging tool to detect variable PD-L1 expression in tumors [41].
4. Assessment of Tumor Regression
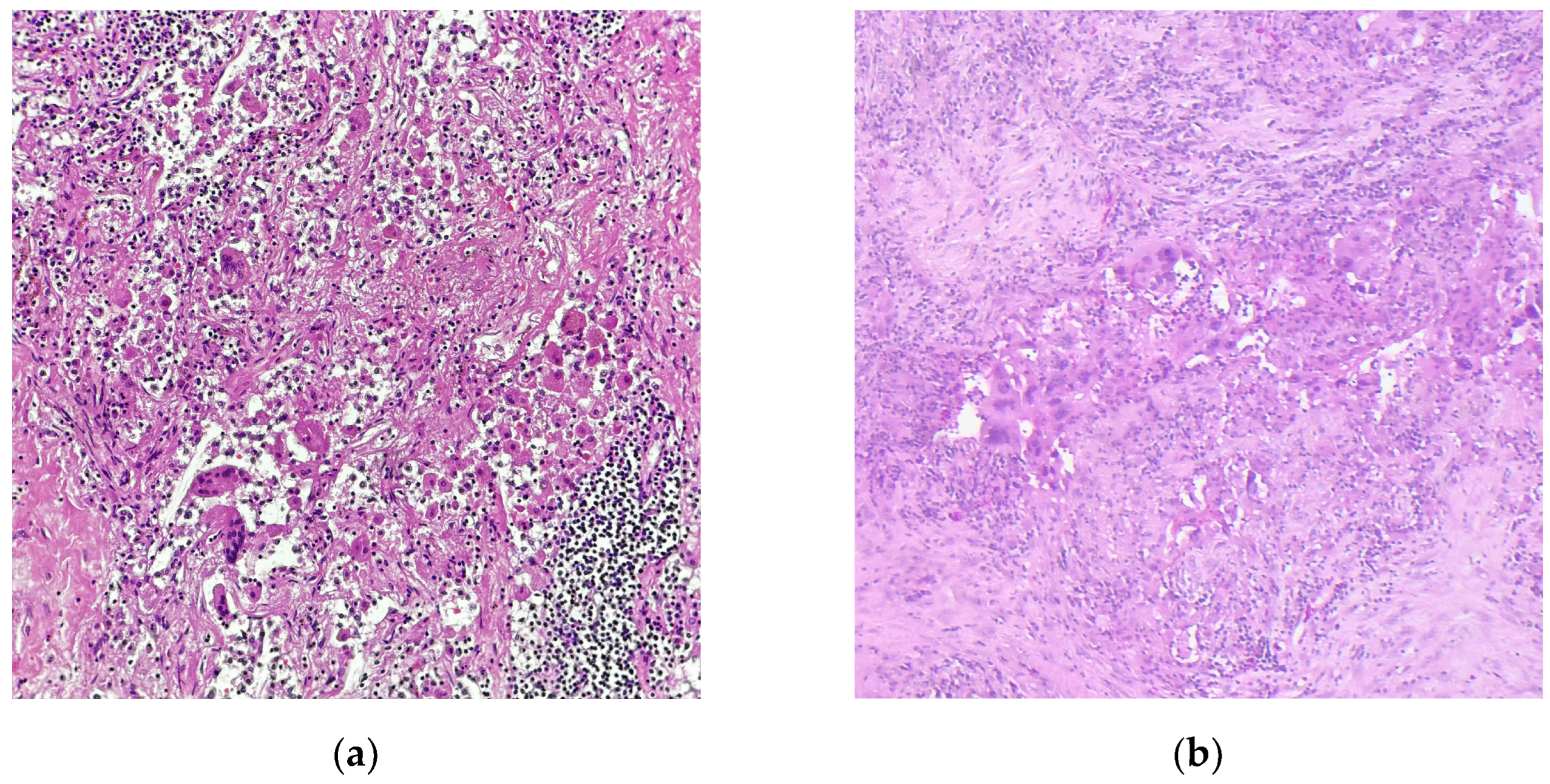
With the approval of neoadjuvant chemoimmunotherapy in NSCLC, it is the pathologists’ task to assess the tumor response to therapy when evaluating the lung resection specimen. There are two main schemes for regression grading after neoadjuvant therapy in NSCLC: the grading system by Junker et al. has originally been published in 1997 to assess the response to neoadjuvant radiochemotherapy in NSCLC [42]; in 2020, the IALSC published an expert consensus for the handling and examination of NSCLC specimens after all neoadjuvant treatment schemes, including targeted therapy and immunotherapy [43]. Complete tumor regression (no residual viable tumor, corresponding to regression grade III (RGIII) in the Junker scheme or pathological complete response (pCR, Figure 1a) in the IASLC scheme) has been shown to predict event-free survival in the CheckMate 816 trial, qualifying tumor regression grading upon neoadjuvant chemoimmunotherapy as a prognostic biomarker in NSCLC [44]. The association between pCR/major pathological response (MPR in the IASLC scheme, RG IIb in the Junker scheme; Figure 1b) and EFS has been confirmed in a recent meta-analysis; however, a significant correlation between pCR/MPR and overall survival could not yet be proven [45]. To enhance robustness of tumor regression as a prognostic biomarker and as an endpoint for the identification of novel predictive biomarkers for the effectivity of chemoimmunotherapy, it is crucial that pathologists perform regression grading in a comprehensive and standardized way, including thorough macroscopic assessment of the resection specimen, embedding of the whole tumor bed (or a representative slide of the largest diameter), examining all lymph nodes, and reporting the percentage of residual vital tumor (% RVT) as a continuous variable. We currently conduct a multicenter study (Re-GraDE Germany) to evaluate the current state of the art of tumor regression grading in NSCLC specimens after neoadjuvant chemoimmunotherapy in Germany (manuscript in preparation).
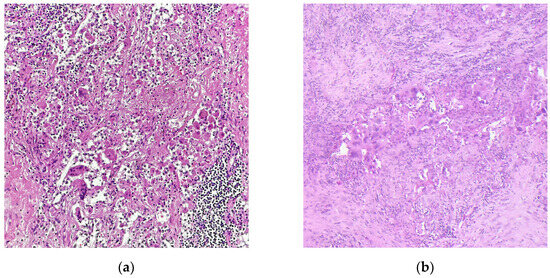
Figure 1.
Representative microphotographs of NSCLC samples after neoadjuvant chemoimmunotherapy. (a) Complete pathological response (pCR); (b) major pathological response (MPR) with residual vital tumor cells. Hematoxylin-Eosin staining; Magnification, 200×; images courtesy of Konrad Steinestel from his personal collection.
5. DNA- and RNA-Based Biomarkers
Tumor-promoting molecular alterations not only underlie tumor formation and progression in NSCLC but also represent targets for personalized treatment [46]. These include driver mutations (e.g., EGFR, BRAF, KRAS, MET), translocations/fusions (e.g., ALK, ROS, RET), and gene amplifications (e.g., ERBB2, FGFR1). The ESCAT classification (ESMO Scale for clinical actionability of molecular targets) classifies biomarkers with approved targeted therapies (EGFR, ALK, ROS) into category I (A, B, C) [47]. While there are comprehensive reviews on the fast-growing list of targeted therapy options for each alteration and while the focus of this review lies on the detection of these alterations in different tissue samples, we will shortly summarize the current knowledge on each mutation. Of note, the distribution of targetable genetic alterations differs significantly between the histologic subtypes of NSCLC. While targetable driver mutations (e.g., EGFR, BRAF) and translocations/fusions (e.g., ALK, ROS, RET) are frequently detected in lung adenocarcinoma (see next paragraph), they are rare (<1%) in squamous cell carcinoma and neuroendocrine neoplasms. Only KRAS G12 mutations and MET amplifications/MET exon 14 skipping mutations are observed in 2.1 and 1.5% of lung squamous cell carcinoma, respectively [48]. Notably, the comparable frequency of KRAS G12C mutations in the “large cell carcinoma” histology group and lung adenocarcinoma supports the hypothesis that a substantial portion of large cell carcinomas are undifferentiated TTF1-negative adenocarcinomas.
Mutations in epithelial growth factor receptor (EGFR) can be detected in about 15% of NSCLC in Europe and America and in up to 50% of cases in Asia [49]. They are more frequent in lung adenocarcinomas, in women, and in non-smokers. Tyrosine kinase inhibition (TKI)-sensitizing mutations occur in EGFR exons 18–21, with in-frame exon 19 deletions and the exon 21 point mutation L858R (also considered “classical” EGFR mutations) constituting over 90% of all EGFR mutations [50,51]. Of note, rarer EGFR mutations (e.g., exon 20 insertions) are associated with decreased sensitivity to TKI treatment [52]. Targeted therapies targeting EGFR comprise antibodies against the extracellular domain that block the dimerization of the receptor or small molecule tyrosine kinase inhibitors, which bind to EGFR and block signal transduction [53]. The increased ATP-binding affinity of the mutant EGFR protein due to conformational change increases TKI binding and suppresses downstream signaling [50]. There is conflicting evidence on the prognostic role of EGFR mutations; while earlier studies found no differences in prognosis between EGFR wild-type and EGFR-mutant cases, advances in EGFR-targeting tyrosine kinase inhibition have led to improved survival in patients whose tumor harbors an EGFR alteration [54]. There are reports indicating a more aggressive biological behavior of tumors with EGFR exon 19 deletion compared to tumors harboring the EGFR L858R mutation [55]. Like other oncogenes, EGFR mutation is associated with a higher rate of metastatic disease in the central nervous system compared to non-oncogene-addicted NSCLC [56].
In general, EGFR mutations are detected in tumor tissue or liquid biopsies/cfDNA by DNA sequencing, but PCR-based approaches for the targeted detection of specific hotspot mutations also exist. For example, it has been shown that the Amplification Refractory Mutation System (ARMS) that selectively amplifies mutation-containing target sequences has a higher sensitivity compared to tissue-based DNA sequencing [57]; however, additional mutations are not detected by this approach. The same is true for fragment length analysis and pyrosequencing, the latter approach also being limited by the requirement of a relatively high tumor cell fraction (>20%) in the investigated sample. In addition, there are mutation-specific antibodies against exon 19-deleted or L858R-mutant EGFR, but given the multitude of immunohistochemical, DNA-, and RNA-based biomarkers, which have to be evaluated in a limited NSCLC tissue sample, we would abstain from the use of tissue slides for targeted detection of individual mutations. This limitation may one day be overcome by multiplex immunostaining.
V-Raf Murine Sarcoma Viral Oncogene Homolog B (BRAF) mutations, which mostly affect the activation loop (A-loop) around codon 600, are detected in 3–8% of NSCLC cases [58]. In NSCLC, class 1 (V600E, activity independent from upstream RAS signaling), class 2 (non-V600E, functionally active as a dimer, with intrinsic discrete kinase activity, independent from upstream RAS signaling), and class 3 mutations (non-V600E, no enzymatic activity, dependent on upstream RAS stimulation) are evenly distributed. This is in contrast to malignant melanoma where the vast majority of BRAF-mutant tumors harbor V600E (class 1) mutations. Most patients with BRAF-mutant NSCLC are former or current smokers; however, up to 30% have never smoked [59]. Comparable to EGFR mutations, BRAF mutations are associated with a higher rate of metastatic disease to the CNS in NSCLC [60]. While tyrosine kinase inhibition is effective, especially in class 1 (V600E) mutations, patients will eventually acquire additional mutations and develop resistance to therapy [61]. Moreover, treatment of class 2 and 3 mutations is not equally effective [58]. Similar to EGFR, the method of choice for the detection of BRAF mutations is DNA sequencing, mostly with NGS, which can also be applied to liquid biopsies. Given the even distribution of V600E and non-V600E BRAF mutations in NSCLC, it is mandatory that fast-track/targeted sequencing approaches span the entire range of possible mutations.
Kirsten rat sarcoma (KRAS) mutations are the most frequent oncogenic driver alterations in NSCLC, detectable in up to 30% of cases in Caucasian patients, with much lower rates in patients of Asian descent [62]. Activating mutations are associated with smoking history and mostly affect codons 12 (90%) or 13, thus keeping the mutant small GTPase KRAS in a constitutionally active state. They frequently occur together with co-mutations in TP53, STK11, or KEAP1 (see below) [63]. While KRAS mutations have long been deemed undruggable, the recent approval of KRAS G12C-specific inhibitors has proven the principle of effective targeted therapy in that setting [62]. Of note, secondary mutations in KRAS or co-mutations in other genes can lead to therapy resistance. With respect to immunotherapy, KRAS-mutant NSCLC seems to experience higher responses to immune checkpoint inhibition compared to other molecular drivers [64]. The prognostic role of KRAS mutations in NSCLC is still a matter of debate due to conflicting results in the literature [62]. Regarding the methodology of detection, the relatively restricted localization of the most frequent KRAS mutations to certain hotspots (codons 12/13, 61) allows for targeted detection (e.g., PCR-based techniques) [65]. In NSCLC, however, the necessity for comprehensive characterization (including other alterations) will lead to the use of NGS in most cases, including liquid biopsies.
Alterations in the MET oncogene (up to 4% of NSCLC) include MET protein overexpression, mutations leading to MET exon 14 skipping, or MET gene amplification [66]. Not only do these occur as primary driver mutations but also as resistance-mediating secondary mutations upon targeted treatment of oncogene-addicted NSCLC. METex14 mutations are in most cases detected by NGS, with hybrid capture-based panels showing higher sensitivity compared to amplicon-based panels; of note, a DNA-based approach only will not cover the entire spectrum of possible METex14 mutations [66]. MET protein overexpression can be detected by immunohistochemistry, while MET gene amplification will be covered by fluorescence in situ hybridization (FISH) [67].
Alterations in the anaplastic lymphoma kinase (ALK) oncogene are found in around 5% of NSCLC cases and include gene fusions, gene amplifications, and activating point mutations [68]. While there are more than 20 different described fusion partners for ALK, the most frequent fusion in NSCLC is the one between the 3′ region of the ALK gene and the 5′ region of the echinoderm microtubule-associated protein-like 4 (EML4) gene [69]. The fusion enhances ALK activity with subsequent signaling along pro-mitogenic pathways such as the mitogen-activated protein kinase (MAPK), (phosphatidylinositol 3−kinase) PI3K/(protein kinase B) AKT, Janus kinase/signal transducer and activator of transcription (JAK/STAT), and mitogen-activated protein kinase 5–extracellular signal-regulated kinase 5 (MEK5-ERK5) pathways [68]. The diagnosis of ALK rearrangements can be performed by using immunohistochemistry (relying on the upregulation of membranous ALK protein expression upon gene fusion), FISH (by directly visualizing the breaking apart of the ALK gene, with or without probing the suspected fusion partner), or RNA-based NGS. As stated above, each technique has its own advantages and disadvantages and the selection of the method depends on the type and amount of available tissue, the expected turnaround time, and, of course, the local availability and reimbursement regulation of the respective technique. Some laboratories will verify a positive ALK IHC by FISH testing, leading to discordant results in rare cases. For these, it has been shown that patients who were ALK FISH-negative but IHC-positive show a response to ALK-targeted therapy, giving ALK IHC a higher predictive value from a clinical viewpoint [70]. It is possible to detect ALK alterations in liquid biopsies (especially in circulating tumor cells); however, there are some technical hurdles to cfDNA/plasma-based detection by NGS given the rapid RNA degradation in blood samples [71].
Proto-oncogene tyrosine-protein kinase-1 (ROS1; c-Ros oncogene-1)-gene fusions occur in up to 2% of NSCLCs, associated with female gender, non-smokers, and adenocarcinoma histology [72,73]. While the physiologic role of the protein is not yet fully clear, ROS1 seems to play a key role in the embryonic development of epithelial tissue [74]. Upon an oncogenic microdeletion, ROS1 fuses with fused-in-glioblastoma (FIG), leading to ROS1 overexpression and the activation of downstream signaling pathways [75]. This can be exploited by the immunohistochemical detection of oncogenic ROS1 in NSCLC tumor cells [76]; however, recent data have questioned the specificity of the available ROS1 antibodies and advocated for the use of reflex NGS for the detection of ROS1 alterations [77]. Finally, RET (rearranged during transfection) or NTRK (neurotrophic tropomyosin-receptor kinase) alterations that are druggable but comparably rare in NSCLC can be proven by FISH or RNA-based NGS, with panTRK IHC being used as a tissue-agnostic screening marker for NTRK alterations [78].
6. The Role of Co-Mutations
In recent years, there is growing evidence that not only does the presence of a single driver mutation but also of additional/secondary mutations affect the biological behavior, as well as the response to targeted therapy in NSCLC, a phenomenon called “intra-driver heterogeneity” [79]. Co-mutations in STK11, KEAP1, and TP53 are frequently observed in KRAS-mutant lung adenocarcinoma, giving rise to a more aggressive tumor phenotype and representing an independent negative prognostic indicator. In EGFR-mutant lung adenocarcinoma, more than half of the cases harbor mutations in TP53, allowing for greater genetic instability and a larger burden of mutations, which may confer resistance to TKI inhibitors [80]. Of note, TP53 mutations are underrepresented in the group of NSCLC associated with gene fusions (ALK, ROS).
7. Genome-Wide Biomarkers: Tumor Mutational Burden and Microsatellite Instability
In addition to alterations in single genes or gene fusions, genome-wide biomarkers such as tumor mutational burden (TMB) and microsatellite instability have been investigated as possible predictive biomarkers for the response to immune checkpoint inhibition. Tumor mutational burden is defined as the number of somatic mutations per megabase and shows great variability between identical tumor entities from different patients as well as between different tumor entities [81]. Tumors with high TMB produce and display a high number of neoantigens, which are then recognized by the immune system, especially under checkpoint inhibitor treatment. Of note, TMB can not only be assessed in tissue samples but also in liquid biopsies, and thus would represent a valuable biomarker that could also be obtained from frail patients at minimal risk [82]. However, the predictive value of TMB for ICI efficiency has so far not been consistently proven [83]. While originally TMB had to be assessed by whole exome sequencing, it has been shown that the results can reliably be obtained by large panel sequencing/comprehensive genomic profiling [81].
Microsatellite instability (MSI-H) and mismatch repair deficiency (dMMR) describe an oncogenic process where somatic or germline mutations in MMR genes lead to an increase in mutations during DNA replication, resulting in high mutational load and tumorigenesis. While rather frequent in colorectal and endometrial carcinoma, MSI-H/dMMR is rare in NSCLC (<1%) and is mostly associated with smoking and adenocarcinoma histology [84]. These tumors show high TMB and are in general vulnerable to ICI treatment, while co-occurring mutations in STK11 and KEAP1 seem to be associated with poor response. While dMMR cases can be identified by IHC for MMR proteins (MLH1, MSH2, MSH6, PMS2), this might be limited by the amount of available tissue, especially given the low rate of NSCLC cases in which dMMR can be expected. A possible solution lies in the use of larger NGS panels, which are capable of detecting both TMB and MSI status in parallel to individual mutation detection.
8. Emerging Biomarkers
In addition to single-gene and genome-wide biomarkers, there are several emerging biomarkers that are currently under investigation in NSCLC, some of which require additional methodological considerations from the (molecular) pathologist. Proteins that are involved in the regulation of the cell cycle (such as p16) and proliferation markers (such as Ki67) that can be assessed with immunohistochemistry have shown promising results as prognostic biomarkers [85]. Antibody–drug conjugates (ADCs) target tumor cell (surface) antigens and deliver a cytotoxic drug load to the tumor cell [86]. The aim of this approach is to reduce unspecific cytotoxic effects that contribute to the toxicity of the treatment, but so far, no ADC has been approved for the treatment of NSCLC. The expression of the respective cellular targets (Her2, Her3, Trop2, Nectin4, MET) is assessed with immunohistochemistry, giving rise to a new group of IHC-based predictive biomarkers for which quality-controlled and reproducible assessment is mandatory. However, the possible requirement to assess a multitude of novel IHC-based biomarkers on a very limited tissue sample should speed up the implementation of multiplex immunohistochemistry so that multiple markers can be assessed on a single slide [87].
9. Technical Aspects
Taken together, as shown in Table 1, (molecular) pathologists encounter a variety of samples, each sample type harboring individual advantages and disadvantages for biomarker testing in NSCLC. The current ESMO guidelines advocate for molecular testing in all lung adenocarcinomas and squamous cell carcinomas in young patients/non-smokers and include the possibility of tumor genetic testing in liquid biopsies, although these are not (yet) regarded as equivalent to tissue [46]. With respect to the recommended method, next-generation sequencing (NGS) has evolved to be the “workhorse” of molecular lung pathology [88]. Both amplicon- and hybrid capture-based techniques are capable of detecting DNA alterations (mutations, copy number alterations) in a large number of samples in a relatively quick laboratory turnaround time [89]. Large NGS panels (comprehensive genomic profiling) are capable of detecting genome-wide biomarkers such as tumor mutational burden and microsatellite instability. Smaller NGS panels are unable to detect genome-wide biomarkers and might not include genes with an emerging role as prognostic and/or predictive biomarkers such as STK11 or KEAP1 [90].
The limitations of NGS testing lie in the amount of sample tumor DNA (>40 ng), which is necessary, especially for hybrid capture-based sequencing techniques as well as in the laboratory turnaround time [91]. In addition, fusions/translocations with unknown partners cannot be detected by DNA-based NGS. RNA-based NGS or fluorescence in situ hybridization (FISH) can be used in addition, with the latter technique requiring additional unstained slides from often very limited material. For ALK and ROS translocations, immunohistochemistry is another alternative, but recent data support the use of RNA NGS due to higher speed and comparable reliability for the detection of ALK fusions and higher reliability for the detection of ROS fusions [77,92]. When performing RNA NGS, however, one has to take into account formalin fixation artifacts and the lower stability of RNA, leading to RNA degradation [93]. With the widespread use of NGS, subsequent testing of individual genes is discouraged since it has been shown that NGS is not only more comprehensive but also more cost-effective compared to single-gene testing [94]. Single-gene testing, however, may have a certain role in a “fast-track” setting when only individual mutations must be ruled out before starting immediate therapy, and the turnaround time for full-scale NGS would be too long. Of note, most of the aspects discussed here concern the situation in countries where NGS technology is available. In countries where a significant number of patients and pathologists do not have access to these technologies, alternative methods of biomarker detection (immunohistochemistry or PCR-based testing) have to be considered. A 2020 IASLC survey among 2537 respondents from 102 countries revealed dissatisfaction with the current state of molecular testing for lung cancer in their respective countries, and of note, 33% of health care professionals were unaware of the current guidelines for molecular testing issued by the College of American Pathologists, IASLC, and Association for Molecular Pathology [95]. Beyond financial and methodological constraints in many regions, these findings underscore the critical need for continuous knowledge dissemination and best practice guidelines on biomarker testing in NSCLC.
10. Quality Management in Biomarker Testing and Outlook
For all discussed biomarkers, it is of utmost importance that (molecular) pathologists make sure that preanalytical requirements are met and that (at least internally) validated tests are used thoroughly. Participation in national or international interlaboratory ring trials should be mandatory [96,97,98]. Correlations between clinical, histopathological, and molecular tumor characteristics, as well as taking into consideration tissue preservation and tumor cell type and content, make the interpretation of the results from biomarker testing both more straightforward and reliable. From our point of view, the outsourcing of (molecular) biomarker tests from pathology institutes as well as the separation of morphological and molecular evaluation of biomarkers, is extremely critical. Instead, we strongly support extended molecular pathology training, as is exemplified by the introduction of the comprehensive Master’s degree program called the “European Masters in Molecular Pathology” (EMMP) by the Pathology Section of the European Union of Medical Specialists and the European Society of Pathology [99]. Well-trained molecular pathologists will be extremely valuable participants in interdisciplinary/molecular tumor boards since they will be able to communicate the pros and cons as well as the limitations of the requested biomarker assay, to interpret them, and to merge the results with morphologic and clinical data. Strengthening the network between (molecular) pathologists throughout Europe and the world will assure continuous high-quality biomarker testing and form the basis for the discovery of novel biomarkers in NSCLC and beyond.
Author Contributions
Conceptualization, K.S. and A.A.; methodology, K.S. and A.A.; writing—original draft preparation, K.S. and A.A.; writing—review and editing, K.S. and A.A. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Data are available from the authors upon request.
Conflicts of Interest
K.S. has received consulting fees, payments, or honoraria from AstraZeneca, Merck Sharp & Dohme, Bristol Meyers Squibb, Sanofi, and Boehringer Ingelheim, and participated on a Data Safety Monitoring Board or Advisory Board for Merck Sharp & Dohme, Bristol Meyers Squibb, and AstraZeneca. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
Abbreviations
The following abbreviations are used in this manuscript:
| NSCLC | Non-small cell lung cancer |
| LAC | Lung adenocarcinoma |
| SCC | Squamous cell carcinoma |
| LCC | Large cell carcinoma |
| LCNEC | Large cell neuroendocrine carcinoma |
| SCLC | Small cell carcinoma |
| EBUS | Endobronchial ultrasound-guided biopsy |
| IHC | Immunohistochemistry |
| LN | Lymph node |
| TPS | Tumor proportion/positivity score |
| AI | Artificial intelligence |
| IASLC | International Association for the Study of Lung Cancer |
| pCR | Pathological complete response |
| MPR | Major pathological response |
| RG | Regression grade |
| RVT | Residual vital tumor |
| ESMO | European Society of Medical Oncology |
| ESCAT | ESMO Scale for clinical actionability of molecular targets |
| NGS | Next-Generation Sequencing |
| FISH | Fluorescene in situ hybridization |
| EMMP | European Masters in Molecular Pathology |
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Meza, R.; Meernik, C.; Jeon, J.; Cote, M.L. Lung cancer incidence trends by gender, race and histology in the United States, 1973–2010. PLoS ONE 2015, 10, e0121323. [Google Scholar] [CrossRef] [PubMed]
- Travis, W.D. Pathology of lung cancer. Clin. Chest Med. 2002, 23, 65–81. [Google Scholar] [CrossRef]
- Zhang, Y.; Vaccarella, S.; Morgan, E.; Li, M.; Etxeberria, J.; Chokunonga, E.; Manraj, S.S.; Kamate, B.; Omonisi, A.; Bray, F. Global variations in lung cancer incidence by histological subtype in 2020: A population-based study. Lancet Oncol. 2023, 24, 1206–1218. [Google Scholar] [CrossRef]
- Muthusamy, B.; Pennell, N. Chemoimmunotherapy for EGFR-mutant NSCLC: Still no clear answer. J. Thorac. Oncol. 2022, 17, 179–181. [Google Scholar] [CrossRef]
- Budczies, J.; Kirchner, M.; Kluck, K.; Kazdal, D.; Glade, J.; Allgäuer, M.; Kriegsmann, M.; Heußel, C.-P.; Herth, F.J.; Winter, H. Deciphering the immunosuppressive tumor microenvironment in ALK-and EGFR-positive lung adenocarcinoma. Cancer Immunol. Immunother. 2022, 71, 251–265. [Google Scholar] [CrossRef]
- Rossi, E.; Aieta, M.; Tartarone, A.; Pezzuto, A.; Facchinetti, A.; Santini, D.; Ulivi, P.; Ludovini, V.; Possidente, L.; Fiduccia, P. A fully automated assay to detect the expression of pan-cytokeratins and of EML4-ALK fusion protein in circulating tumour cells (CTCs) predicts outcome of non-small cell lung cancer (NSCLC) patients. Transl. Lung Cancer Res. 2021, 10, 80. [Google Scholar] [CrossRef]
- Kapeleris, J.; Bark, J.M.; Ranjit, S.; Irwin, D.; Hartel, G.; Warkiani, M.E.; Leo, P.; O’Leary, C.; Ladwa, R.; O’Byrne, K. Prognostic value of integrating circulating tumour cells and cell-free DNA in non-small cell lung cancer. Heliyon 2022, 8, e09971. [Google Scholar] [CrossRef]
- Tian, M.; He, X.; Jin, C.; He, X.; Wu, S.; Zhou, R.; Zhang, X.; Zhang, K.; Gu, W.; Wang, J. Transpathology: Molecular imaging-based pathology. Eur. J. Nucl. Med. Mol. Imaging 2021, 48, 2338–2350. [Google Scholar] [CrossRef]
- Zinn, P.O.; Singh, S.K.; Kotrotsou, A.; Hassan, I.; Thomas, G.; Luedi, M.M.; Elakkad, A.; Elshafeey, N.; Idris, T.; Mosley, J. A coclinical radiogenomic validation study: Conserved magnetic resonance radiomic appearance of periostin-expressing glioblastoma in patients and xenograft models. Clin. Cancer Res. 2018, 24, 6288–6299. [Google Scholar] [CrossRef]
- Hotta, M.; Kim, G.H.J.; Rerkpichaisuth, V.; Teng, P.Y.; Armstrong, W.R.; Carlucci, G.; Dahlbom, M.; Abtin, F.; Lari, S.M.; Fishbein, G.A. Correlation of FAPI PET uptake with immunohistochemistry in explanted lungs from patients with advanced interstitial lung disease. J. Nucl. Med. 2024, 65, 1789–1794. [Google Scholar] [CrossRef]
- Yang, P.; Luo, Q.; Wang, X.; Fang, Q.; Fu, Z.; Li, J.; Lai, Y.; Chen, X.; Xu, X.; Peng, X. Comprehensive analysis of fibroblast activation protein expression in interstitial lung diseases. Am. J. Respir. Crit. Care Med. 2023, 207, 160–172. [Google Scholar] [CrossRef]
- Rolfo, C.; Mack, P.; Scagliotti, G.V.; Aggarwal, C.; Arcila, M.E.; Barlesi, F.; Bivona, T.; Diehn, M.; Dive, C.; Dziadziuszko, R. Liquid biopsy for advanced NSCLC: A consensus statement from the international association for the study of lung cancer. J. Thorac. Oncol. 2021, 16, 1647–1662. [Google Scholar] [CrossRef] [PubMed]
- Liam, C.K.; Mallawathantri, S.; Fong, K.M. Is tissue still the issue in detecting molecular alterations in lung cancer? Respirology 2020, 25, 933–943. [Google Scholar] [CrossRef]
- Davidson, K.R.; Ha, D.M.; Schwarz, M.I.; Chan, E.D. Bronchoalveolar lavage as a diagnostic procedure: A review of known cellular and molecular findings in various lung diseases. J. Thorac. Dis. 2020, 12, 4991. [Google Scholar] [CrossRef] [PubMed]
- Kalkanis, A.; Papadopoulos, D.; Testelmans, D.; Kopitopoulou, A.; Boeykens, E.; Wauters, E. Bronchoalveolar lavage fluid-isolated biomarkers for the diagnostic and prognostic assessment of lung cancer. Diagnostics 2022, 12, 2949. [Google Scholar] [CrossRef] [PubMed]
- Sticht, F.; Malfertheiner, M.V.; Wiest, C.; Schulz, C.; Fisser, C.; Mamilos, A. Comparison of transbronchial biopsy techniques using needle and forceps biopsies in lung cancer for molecular diagnostics: A prospective, randomized crossover trial. Transl. Cancer Res. 2024, 13, 2464. [Google Scholar] [CrossRef]
- Velasco-Albendea, F.J.; Cruz-Rueda, J.J.; Gil-Belmonte, M.J.; Pérez-Rodríguez, Á.; López-Pardo, A.; Agredano-Ávila, B.; Lozano-Paniagua, D.; Nievas-Soriano, B.J. The contribution of mediastinal transbronchial nodal cryobiopsy to morpho-histological and molecular diagnosis. Diagnostics 2023, 13, 3476. [Google Scholar] [CrossRef]
- Momozane, T.; Shigetsu, K.; Kimura, Y.; Kishima, H.; Kodama, K. The histological diagnosis and molecular testing of lung cancer by surgical biopsy for intrathoracic lesions. Gen. Thorac. Cardiovasc. Surg. 2021, 69, 1185–1191. [Google Scholar] [CrossRef]
- Ricciuti, B.; Wang, X.; Alessi, J.V.; Rizvi, H.; Mahadevan, N.R.; Li, Y.Y.; Polio, A.; Lindsay, J.; Umeton, R.; Sinha, R. Association of high tumor mutation burden in non–small cell lung cancers with increased immune infiltration and improved clinical outcomes of PD-L1 blockade across PD-L1 expression levels. JAMA Oncol. 2022, 8, 1160–1168. [Google Scholar] [CrossRef]
- Salmaninejad, A.; Valilou, S.F.; Shabgah, A.G.; Aslani, S.; Alimardani, M.; Pasdar, A.; Sahebkar, A. PD-1/PD-L1 pathway: Basic biology and role in cancer immunotherapy. J. Cell. Physiol. 2019, 234, 16824–16837. [Google Scholar] [CrossRef] [PubMed]
- Lantuejoul, S.; Sound-Tsao, M.; Cooper, W.A.; Girard, N.; Hirsch, F.R.; Roden, A.C.; Lopez-Rios, F.; Jain, D.; Chou, T.-Y.; Motoi, N. PD-L1 testing for lung cancer in 2019: Perspective from the IASLC pathology committee. J. Thorac. Oncol. 2020, 15, 499–519. [Google Scholar] [CrossRef]
- Rimm, D.L.; Han, G.; Taube, J.M.; Eunhee, S.Y.; Bridge, J.A.; Flieder, D.B.; Homer, R.; West, W.W.; Wu, H.; Roden, A.C. A prospective, multi-institutional, pathologist-based assessment of 4 immunohistochemistry assays for PD-L1 expression in non–small cell lung cancer. JAMA Oncol. 2017, 3, 1051–1058. [Google Scholar] [CrossRef]
- Scheel, A.H.; Dietel, M.; Heukamp, L.C.; Jöhrens, K.; Kirchner, T.; Reu, S.; Rueschoff, J.; Schildhaus, H.-U.; Schirmacher, P.; Tiemann, M. Predictive PD-L1 immunohistochemistry for non-small cell lung cancer: Current state of the art and experiences of the first German harmonization study. Der Pathol. 2016, 37, 557–567. [Google Scholar] [CrossRef] [PubMed]
- Yu, S.-L.; Hsiao, Y.-J.; Cooper, W.A.; Choi, Y.-L.; Avilés-Salas, A.; Chou, T.-Y.; Coudry, R.; Raskin, G.A.; Fox, S.B.; Huang, C.-C. The Ring Study: An international comparison of PD-L1 diagnostic assays and their interpretation in non-small cell lung cancer, head and neck squamous cell cancer and urothelial cancer. Pathology 2023, 55, 19–30. [Google Scholar] [CrossRef]
- Kowanetz, M.; Zou, W.; Gettinger, S.N.; Koeppen, H.; Kockx, M.; Schmid, P.; Kadel, E.E., III; Wistuba, I.; Chaft, J.; Rizvi, N.A. Differential regulation of PD-L1 expression by immune and tumor cells in NSCLC and the response to treatment with atezolizumab (anti–PD-L1). Proc. Natl. Acad. Sci. USA 2018, 115, E10119–E10126. [Google Scholar] [CrossRef]
- Rojkó, L.; Reiniger, L.; Téglási, V.; Fábián, K.; Pipek, O.; Vágvölgyi, A.; Agócs, L.; Fillinger, J.; Kajdácsi, Z.; Tímár, J. Chemotherapy treatment is associated with altered PD-L1 expression in lung cancer patients. J. Cancer Res. Clin. Oncol. 2018, 144, 1219–1226. [Google Scholar] [CrossRef] [PubMed]
- John, N.; Schlintl, V.; Sassmann, T.; Lindenmann, J.; Fediuk, M.; Wurm, R.; Douschan, P.; Zacharias, M.; Kalson, L.; Posch, F. Longitudinal analysis of PD-L1 expression in patients with relapsed NSCLC. J. Immunother. Cancer 2024, 12, e008592. [Google Scholar] [CrossRef]
- Reck, M.; Rodríguez–Abreu, D.; Robinson, A.G.; Hui, R.; Csőszi, T.; Fülöp, A.; Gottfried, M.; Peled, N.; Tafreshi, A.; Cuffe, S. Updated analysis of KEYNOTE-024: Pembrolizumab versus platinum-based chemotherapy for advanced non–small-cell lung cancer with PD-L1 tumor proportion score of 50% or greater. J. Clin. Oncol. 2019, 37, 537–546. [Google Scholar] [CrossRef]
- Doroshow, D.B.; Wei, W.; Gupta, S.; Zugazagoitia, J.; Robbins, C.; Adamson, B.; Rimm, D.L. Programmed death-ligand 1 tumor proportion score and overall survival from first-line pembrolizumab in patients with nonsquamous versus squamous NSCLC. J. Thorac. Oncol. 2021, 16, 2139–2143. [Google Scholar] [CrossRef]
- Cree, I.A.; Booton, R.; Cane, P.; Gosney, J.; Ibrahim, M.; Kerr, K.; Lal, R.; Lewanski, C.; Navani, N.; Nicholson, A.G. PD-L1 testing for lung cancer in the UK: Recognizing the challenges for implementation. Histopathology 2016, 69, 177–186. [Google Scholar] [CrossRef]
- Haragan, A.; Field, J.K.; Davies, M.P.; Escriu, C.; Gruver, A.; Gosney, J.R. Heterogeneity of PD-L1 expression in non-small cell lung cancer: Implications for specimen sampling in predicting treatment response. Lung Cancer 2019, 134, 79–84. [Google Scholar] [CrossRef]
- Brunnström, H.; Johansson, A.; Westbom-Fremer, S.; Backman, M.; Djureinovic, D.; Patthey, A.; Isaksson-Mettävainio, M.; Gulyas, M.; Micke, P. PD-L1 immunohistochemistry in clinical diagnostics of lung cancer: Inter-pathologist variability is higher than assay variability. Mod. Pathol. 2017, 30, 1411–1421. [Google Scholar] [CrossRef] [PubMed]
- Cooper, W.A.; Russell, P.A.; Cherian, M.; Duhig, E.E.; Godbolt, D.; Jessup, P.J.; Khoo, C.; Leslie, C.; Mahar, A.; Moffat, D.F. Intra-and interobserver reproducibility assessment of PD-L1 biomarker in non–small cell lung cancer. Clin. Cancer Res. 2017, 23, 4569–4577. [Google Scholar] [CrossRef] [PubMed]
- Troncone, G.; Gridelli, C. The reproducibility of PD-L1 scoring in lung cancer: Can the pathologists do better? Transl. Lung Cancer Res. 2017, 6, S74. [Google Scholar] [CrossRef]
- Huang, Z.; Chen, L.; Lv, L.; Fu, C.-C.; Jin, Y.; Zheng, Q.; Wang, B.; Ye, Q.; Fang, Q.; Li, Y. A new AI-assisted scoring system for PD-L1 expression in NSCLC. Comput. Methods Programs Biomed. 2022, 221, 106829. [Google Scholar] [CrossRef]
- Choi, S.; Cho, S.I.; Ma, M.; Park, S.; Pereira, S.; Aum, B.J.; Shin, S.; Paeng, K.; Yoo, D.; Jung, W. Artificial intelligence–powered programmed death ligand 1 analyser reduces interobserver variation in tumour proportion score for non–small cell lung cancer with better prediction of immunotherapy response. Eur. J. Cancer 2022, 170, 17–26. [Google Scholar] [CrossRef]
- Wu, J.; Liu, C.; Liu, X.; Sun, W.; Li, L.; Gao, N.; Zhang, Y.; Yang, X.; Zhang, J.; Wang, H. Artificial intelligence-assisted system for precision diagnosis of PD-L1 expression in non-small cell lung cancer. Mod. Pathol. 2022, 35, 403–411. [Google Scholar] [CrossRef]
- Niu, M.; Liu, Y.; Yi, M.; Jiao, D.; Wu, K. Biological characteristics and clinical significance of soluble PD-1/PD-L1 and exosomal PD-L1 in cancer. Front. Immunol. 2022, 13, 827921. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Mao, Z.; Chen, Q.; Koh, K.; Hu, X.; Chen, H. Rapid and sensitive detection of PD-L1 exosomes using Cu-TCPP 2D MOF as a SPR sensitizer. Biosens. Bioelectron. 2022, 201, 113954. [Google Scholar] [CrossRef]
- Mishra, A.; Gupta, K.; Kumar, D.; Lofland, G.; Sharma, A.K.; Solnes, L.B.; Rowe, S.P.; Forde, P.M.; Pomper, M.G.; Gabrielson, E.W. Non-invasive PD-L1 quantification using [18F] DK222-PET imaging in cancer immunotherapy. J. Immunother. Cancer 2023, 11, e007535. [Google Scholar] [CrossRef] [PubMed]
- Junker, K.; Thomas, M.; Schulmann, K.; Klinke, F.; Bosse, U.; Müller, K.-M. Tumour regression in non-small-cell lung cancer following neoadjuvant therapy. Histological assessment. J. Cancer Res. Clin. Oncol. 1997, 123, 469–477. [Google Scholar] [CrossRef]
- Travis, W.D.; Dacic, S.; Wistuba, I.; Sholl, L.; Adusumilli, P.; Bubendorf, L.; Bunn, P.; Cascone, T.; Chaft, J.; Chen, G. IASLC multidisciplinary recommendations for pathologic assessment of lung cancer resection specimens after neoadjuvant therapy. J. Thorac. Oncol. 2020, 15, 709–740. [Google Scholar] [CrossRef] [PubMed]
- O’Brien, M.; Paz-Ares, L.; Marreaud, S.; Dafni, U.; Oselin, K.; Havel, L.; Esteban, E.; Isla, D.; Martinez-Marti, A.; Faehling, M. Pembrolizumab versus placebo as adjuvant therapy for completely resected stage IB–IIIA non-small-cell lung cancer (PEARLS/KEYNOTE-091): An interim analysis of a randomised, triple-blind, phase 3 trial. Lancet Oncol. 2022, 23, 1274–1286. [Google Scholar] [CrossRef]
- Hines, J.B.; Cameron, R.B.; Esposito, A.; Kim, L.; Porcu, L.; Nuccio, A.; Viscardi, G.; Ferrara, R.; Veronesi, G.; Forde, P.M. Evaluation of MPR and pCR as surrogate endpoints for survival in randomized controlled trials of neoadjuvant immune checkpoint blockade in resectable in non-small cell lung cancer. J. Thorac. Oncol. 2024, 19, 1108–1116. [Google Scholar] [CrossRef]
- Hendriks, L.; Kerr, K.; Menis, J.; Mok, T.; Nestle, U.; Passaro, A.; Peters, S.; Planchard, D.; Smit, E.; Solomon, B. Oncogene-addicted metastatic non-small-cell lung cancer: ESMO Clinical Practice Guideline for diagnosis, treatment and follow-up. Ann. Oncol. 2023, 34, 339–357. [Google Scholar] [CrossRef]
- Mosele, F.; Remon, J.; Mateo, J.; Westphalen, C.; Barlesi, F.; Lolkema, M.; Normanno, N.; Scarpa, A.; Robson, M.; Meric-Bernstam, F. Recommendations for the use of next-generation sequencing (NGS) for patients with metastatic cancers: A report from the ESMO Precision Medicine Working Group. Ann. Oncol. 2020, 31, 1491–1505. [Google Scholar] [CrossRef]
- Adib, E.; Nassar, A.H.; Abou Alaiwi, S.; Groha, S.; Akl, E.W.; Sholl, L.M.; Michael, K.S.; Awad, M.M.; Jänne, P.A.; Gusev, A. Variation in targetable genomic alterations in non-small cell lung cancer by genetic ancestry, sex, smoking history, and histology. Genome Med. 2022, 14, 39. [Google Scholar] [CrossRef]
- Tan, A.C.; Tan, D.S. Targeted therapies for lung cancer patients with oncogenic driver molecular alterations. J. Clin. Oncol. 2022, 40, 611–625. [Google Scholar] [CrossRef]
- Lynch, T.J.; Bell, D.W.; Sordella, R.; Gurubhagavatula, S.; Okimoto, R.A.; Brannigan, B.W.; Harris, P.L.; Haserlat, S.M.; Supko, J.G.; Haluska, F.G. Activating mutations in the epidermal growth factor receptor underlying responsiveness of non–small-cell lung cancer to gefitinib. N. Engl. J. Med. 2004, 350, 2129–2139. [Google Scholar] [CrossRef]
- Pao, W.; Miller, V.; Zakowski, M.; Doherty, J.; Politi, K.; Sarkaria, I.; Singh, B.; Heelan, R.; Rusch, V.; Fulton, L. EGF receptor gene mutations are common in lung cancers from “never smokers” and are associated with sensitivity of tumors to gefitinib and erlotinib. Proc. Natl. Acad. Sci. USA 2004, 101, 13306–13311. [Google Scholar] [CrossRef]
- Robichaux, J.P.; Le, X.; Vijayan, R.; Hicks, J.K.; Heeke, S.; Elamin, Y.Y.; Lin, H.Y.; Udagawa, H.; Skoulidis, F.; Tran, H. Structure-based classification predicts drug response in EGFR-mutant NSCLC. Nature 2021, 597, 732–737. [Google Scholar] [CrossRef] [PubMed]
- Zubair, T.; Bandyopadhyay, D. Small molecule EGFR inhibitors as anti-cancer agents: Discovery, mechanisms of action, and opportunities. Int. J. Mol. Sci. 2023, 24, 2651. [Google Scholar] [CrossRef]
- Remon, J.; Saw, S.P.; Cortiula, F.; Singh, P.K.; Menis, J.; Mountzios, G.; Hendriks, L.E. Perioperative treatment strategies in EGFR-mutant early-stage NSCLC: Current evidence and future challenges. J. Thorac. Oncol. 2024, 19, 199–215. [Google Scholar] [CrossRef] [PubMed]
- Suda, K.; Mitsudomi, T.; Shintani, Y.; Okami, J.; Ito, H.; Ohtsuka, T.; Toyooka, S.; Mori, T.; Watanabe, S.-I.; Asamura, H. Clinical impacts of EGFR mutation status: Analysis of 5780 surgically resected lung cancer cases. Ann. Thorac. Surg. 2021, 111, 269–276. [Google Scholar] [CrossRef]
- Shin, D.-Y.; Kim, C.H.; Park, S.; Baek, H.; Yang, S.H. EGFR mutation and brain metastasis in pulmonary adenocarcinomas. J. Thorac. Oncol. 2014, 9, 195–199. [Google Scholar] [CrossRef] [PubMed]
- Ellison, G.; Zhu, G.; Moulis, A.; Dearden, S.; Speake, G.; McCormack, R. EGFR mutation testing in lung cancer: A review of available methods and their use for analysis of tumour tissue and cytology samples. J. Clin. Pathol. 2013, 66, 79–89. [Google Scholar] [CrossRef]
- Tabbò, F.; Pisano, C.; Mazieres, J.; Mezquita, L.; Nadal, E.; Planchard, D.; Pradines, A.; Santamaria, D.; Swalduz, A.; Ambrogio, C. How far we have come targeting BRAF-mutant non-small cell lung cancer (NSCLC). Cancer Treat. Rev. 2022, 103, 102335. [Google Scholar] [CrossRef]
- Planchard, D.; Smit, E.F.; Groen, H.J.; Mazieres, J.; Besse, B.; Helland, Å.; Giannone, V.; D’Amelio, A.M.; Zhang, P.; Mookerjee, B. Dabrafenib plus trametinib in patients with previously untreated BRAFV600E-mutant metastatic non-small-cell lung cancer: An open-label, phase 2 trial. Lancet Oncol. 2017, 18, 1307–1316. [Google Scholar] [CrossRef]
- Dagogo-Jack, I.; Martinez, P.; Yeap, B.Y.; Ambrogio, C.; Ferris, L.A.; Lydon, C.; Nguyen, T.; Jessop, N.A.; Iafrate, A.J.; Johnson, B.E. Impact of BRAF mutation class on disease characteristics and clinical outcomes in BRAF-mutant lung cancer. Clin. Cancer Res. 2019, 25, 158–165. [Google Scholar] [CrossRef]
- Chan, X.Y.; Singh, A.; Osman, N.; Piva, T.J. Role played by signalling pathways in overcoming BRAF inhibitor resistance in melanoma. Int. J. Mol. Sci. 2017, 18, 1527. [Google Scholar] [CrossRef]
- Cascetta, P.; Marinello, A.; Lazzari, C.; Gregorc, V.; Planchard, D.; Bianco, R.; Normanno, N.; Morabito, A. KRAS in NSCLC: State of the art and future perspectives. Cancers 2022, 14, 5430. [Google Scholar] [CrossRef]
- Scheffler, M.; Ihle, M.A.; Hein, R.; Merkelbach-Bruse, S.; Scheel, A.H.; Siemanowski, J.; Brägelmann, J.; Kron, A.; Abedpour, N.; Ueckeroth, F. K-ras mutation subtypes in NSCLC and associated co-occuring mutations in other oncogenic pathways. J. Thorac. Oncol. 2019, 14, 606–616. [Google Scholar] [CrossRef] [PubMed]
- Mazieres, J.; Drilon, A.; Lusque, A.; Mhanna, L.; Cortot, A.; Mezquita, L.; Thai, A.; Mascaux, C.; Couraud, S.; Veillon, R. Immune checkpoint inhibitors for patients with advanced lung cancer and oncogenic driver alterations: Results from the IMMUNOTARGET registry. Ann. Oncol. 2019, 30, 1321–1328. [Google Scholar] [CrossRef]
- Li, J.; Gan, S.; Blair, A.; Min, K.; Rehage, T.; Hoeppner, C.; Halait, H.; Brophy, V.H. A highly verified assay for KRAS mutation detection in tissue and plasma of lung, colorectal, and pancreatic cancer. Arch. Pathol. Lab. Med. 2019, 143, 183–189. [Google Scholar] [CrossRef] [PubMed]
- Remon, J.; Hendriks, L.E.; Mountzios, G.; García-Campelo, R.; Saw, S.P.; Uprety, D.; Recondo, G.; Villacampa, G.; Reck, M. MET alterations in NSCLC—Current perspectives and future challenges. J. Thorac. Oncol. 2023, 18, 419–435. [Google Scholar] [CrossRef] [PubMed]
- Guo, R.; Luo, J.; Chang, J.; Rekhtman, N.; Arcila, M.; Drilon, A. MET-dependent solid tumours—Molecular diagnosis and targeted therapy. Nat. Rev. Clin. Oncol. 2020, 17, 569–587. [Google Scholar] [CrossRef]
- Peng, L.; Zhu, L.; Sun, Y.; Stebbing, J.; Selvaggi, G.; Zhang, Y.; Yu, Z. Targeting ALK rearrangements in NSCLC: Current state of the art. Front. Oncol. 2022, 12, 863461. [Google Scholar] [CrossRef]
- Soda, M.; Choi, Y.L.; Enomoto, M.; Takada, S.; Yamashita, Y.; Ishikawa, S.; Fujiwara, S.-I.; Watanabe, H.; Kurashina, K.; Hatanaka, H. Identification of the transforming EML4–ALK fusion gene in non-small-cell lung cancer. Nature 2007, 448, 561–566. [Google Scholar] [CrossRef]
- Cabillic, F.; Hofman, P.; Ilie, M.; Peled, N.; Hochmair, M.; Dietel, M.; Von Laffert, M.; Gosney, J.R.; Lopez-Rios, F.; Erb, G. ALK IHC and FISH discordant results in patients with NSCLC and treatment response: For discussion of the question—To treat or not to treat? ESMO Open 2018, 3, e000419. [Google Scholar] [CrossRef]
- Hofman, P. ALK status assessment with liquid biopsies of lung cancer patients. Cancers 2017, 9, 106. [Google Scholar] [CrossRef]
- Yu, Z.-Q.; Wang, M.; Zhou, W.; Mao, M.-X.; Chen, Y.-Y.; Li, N.; Peng, X.-C.; Cai, J.; Cai, Z.-Q. ROS1-positive non-small cell lung cancer (NSCLC): Biology, diagnostics, therapeutics and resistance. J. Drug Target. 2022, 30, 845–857. [Google Scholar] [CrossRef]
- Gendarme, S.; Bylicki, O.; Chouaid, C.; Guisier, F. ROS-1 fusions in non-small-cell lung cancer: Evidence to date. Curr. Oncol. 2022, 29, 641–658. [Google Scholar] [CrossRef] [PubMed]
- Acquaviva, J.; Wong, R.; Charest, A. The multifaceted roles of the receptor tyrosine kinase ROS in development and cancer. Biochim. Biophys. Acta Rev. Cancer 2009, 1795, 37–52. [Google Scholar] [CrossRef]
- Charest, A.; Lane, K.; McMahon, K.; Park, J.; Preisinger, E.; Conroy, H.; Housman, D. Fusion of FIG to the receptor tyrosine kinase ROS in a glioblastoma with an interstitial del (6)(q21q21). Genes Chromosomes Cancer 2003, 37, 58–71. [Google Scholar] [CrossRef]
- Hofman, V.; Rouquette, I.; Long-Mira, E.; Piton, N.; Chamorey, E.; Heeke, S.; Vignaud, J.M.; Yguel, C.; Mazières, J.; Lepage, A.-L. Multicenter evaluation of a novel ROS1 immunohistochemistry assay (SP384) for detection of ROS1 rearrangements in a large cohort of lung adenocarcinoma patients. J. Thorac. Oncol. 2019, 14, 1204–1212. [Google Scholar] [CrossRef] [PubMed]
- Hofman, V.; Goffinet, S.; Bontoux, C.; Long-Mira, E.; Lassalle, S.; Ilié, M.; Hofman, P. A real-world experience from a single center (LPCE, nice, France) highlights the urgent need to abandon immunohistochemistry for ROS1 rearrangement screening of advanced non-squamous non-small cell lung cancer. J. Pers. Med. 2023, 13, 810. [Google Scholar] [CrossRef] [PubMed]
- Tan, A.C.; Seet, A.O.; Lai, G.G.; Lim, T.H.; Lim, A.S.; San Tan, G.; Takano, A.; Tai, D.W.; Tan, T.J.; Lam, J.Y. Molecular characterization and clinical outcomes in RET-rearranged NSCLC. J. Thorac. Oncol. 2020, 15, 1928–1934. [Google Scholar] [CrossRef]
- Skoulidis, F.; Heymach, J.V. Co-occurring genomic alterations in non-small-cell lung cancer biology and therapy. Nat. Rev. Cancer 2019, 19, 495–509. [Google Scholar] [CrossRef]
- Canale, M.; Petracci, E.; Delmonte, A.; Chiadini, E.; Dazzi, C.; Papi, M.; Capelli, L.; Casanova, C.; De Luigi, N.; Mariotti, M. Impact of TP53 mutations on outcome in EGFR-mutated patients treated with first-line tyrosine kinase inhibitors. Clin. Cancer Res. 2017, 23, 2195–2202. [Google Scholar] [CrossRef]
- Sha, D.; Jin, Z.; Budczies, J.; Kluck, K.; Stenzinger, A.; Sinicrope, F.A. Tumor mutational burden as a predictive biomarker in solid tumors. Cancer Discov. 2020, 10, 1808–1825. [Google Scholar] [CrossRef]
- Friedlaender, A.; Nouspikel, T.; Christinat, Y.; Ho, L.; McKee, T.; Addeo, A. Tissue-plasma TMB comparison and plasma TMB monitoring in patients with metastatic non-small cell lung cancer receiving immune checkpoint inhibitors. Front. Oncol. 2020, 10, 142. [Google Scholar] [CrossRef]
- Galvano, A.; Gristina, V.; Malapelle, U.; Pisapia, P.; Pepe, F.; Barraco, N.; Castiglia, M.; Perez, A.; Rolfo, C.; Troncone, G. The prognostic impact of tumor mutational burden (TMB) in the first-line management of advanced non-oncogene addicted non-small-cell lung cancer (NSCLC): A systematic review and meta-analysis of randomized controlled trials. ESMO Open 2021, 6, 100124. [Google Scholar] [CrossRef]
- Yang, S.-R.; Gedvilaite, E.; Ptashkin, R.; Chang, J.; Ziegler, J.; Mata, D.A.; Villafania, L.B.; Nafa, K.; Hechtman, J.F.; Benayed, R. Microsatellite instability and mismatch repair deficiency define a distinct subset of lung cancers characterized by smoking exposure, high tumor mutational burden, and recurrent somatic MLH1 inactivation. J. Thorac. Oncol. 2024, 19, 409–424. [Google Scholar] [CrossRef] [PubMed]
- Pezzuto, A.; Cappuzzo, F.; D’arcangelo, M.; Ciccozzi, M.; Navarini, L.; Guerrini, S.; Ricci, A.; D’ascanio, M.; Carico, E. Prognostic value of p16 protein in patients with surgically treated non-small cell lung cancer; relationship with Ki-67 and PD-L1. Anticancer Res. 2020, 40, 983–990. [Google Scholar] [CrossRef]
- Abuhelwa, Z.; Alloghbi, A.; Nagasaka, M. A comprehensive review on antibody-drug conjugates (ADCs) in the treatment landscape of non-small cell lung cancer (NSCLC). Cancer Treat. Rev. 2022, 106, 102393. [Google Scholar] [CrossRef] [PubMed]
- Harms, P.W.; Frankel, T.L.; Moutafi, M.; Rao, A.; Rimm, D.L.; Taube, J.M.; Thomas, D.; Chan, M.P.; Pantanowitz, L. Multiplex immunohistochemistry and immunofluorescence: A practical update for pathologists. Mod. Pathol. 2023, 36, 100197. [Google Scholar] [CrossRef]
- De Maglio, G.; Pasello, G.; Dono, M.; Fiorentino, M.; Follador, A.; Sciortino, M.; Malapelle, U.; Tiseo, M. The storm of NGS in NSCLC diagnostic-therapeutic pathway: How to sun the real clinical practice. Crit. Rev. Oncol. Hematol. 2022, 169, 103561. [Google Scholar] [CrossRef]
- Treichler, G.; Hoeller, S.; Rueschoff, J.; Rechsteiner, M.; Britschgi, C.; Arnold, F.; Zoche, M.; Hiltbrunner, S.; Moch, H.; Akhoundova, D. Improving the turnaround time of molecular profiling for advanced non-small cell lung cancer: Outcome of a new algorithm integrating multiple approaches. Pathol. Res. Pract. 2023, 248, 154660. [Google Scholar] [CrossRef] [PubMed]
- Papillon-Cavanagh, S.; Doshi, P.; Dobrin, R.; Szustakowski, J.; Walsh, A.M. STK11 and KEAP1 mutations as prognostic biomarkers in an observational real-world lung adenocarcinoma cohort. ESMO Open 2020, 5, e000706. [Google Scholar] [CrossRef]
- Lazzari, C.; Bulotta, A.; Cangi, M.G.; Bucci, G.; Pecciarini, L.; Bonfiglio, S.; Lorusso, V.; Ippati, S.; Arrigoni, G.; Grassini, G. Next generation sequencing in non-small cell lung cancer: Pitfalls and opportunities. Diagnostics 2020, 10, 1092. [Google Scholar] [CrossRef] [PubMed]
- Ilié, M.; Goffinet, S.; Rignol, G.; Lespinet-Fabre, V.; Lalvée, S.; Bordone, O.; Zahaf, K.; Bonnetaud, C.; Washetine, K.; Lassalle, S. Shifting from Immunohistochemistry to Screen for ALK Rearrangements: Real-World Experience in a Large Single-Center Cohort of Patients with Non-Small-Cell Lung Cancer. Cancers 2024, 16, 2219. [Google Scholar] [CrossRef]
- Kaya, C.; Dorsaint, P.; Mercurio, S.; Campbell, A.M.; Eng, K.W.; Nikiforova, M.N.; Elemento, O.; Nikiforov, Y.E.; Sboner, A. Limitations of detecting genetic variants from the RNA sequencing data in tissue and fine-needle aspiration samples. Thyroid 2021, 31, 589–595. [Google Scholar] [CrossRef] [PubMed]
- Zou, D.; Ye, W.; Hess, L.M.; Bhandari, N.R.; Ale-Ali, A.; Foster, J.; Quon, P.; Harris, M. Diagnostic value and cost-effectiveness of next-generation sequencing–based testing for treatment of patients with advanced/metastatic non-squamous non–small-cell lung cancer in the United States. J. Mol. Diagn. 2022, 24, 901–914. [Google Scholar] [CrossRef]
- Smeltzer, M.P.; Wynes, M.W.; Lantuejoul, S.; Soo, R.; Ramalingam, S.S.; Varella-Garcia, M.; Taylor, M.M.; Richeimer, K.; Wood, K.; Howell, K.E. The International Association for the Study of Lung Cancer global survey on molecular testing in lung cancer. J. Thorac. Oncol. 2020, 15, 1434–1448. [Google Scholar] [CrossRef] [PubMed]
- Jurmeister, P.; Vollbrecht, C.; Jöhrens, K.; Aust, D.; Behnke, A.; Stenzinger, A.; Penzel, R.; Endris, V.; Schirmacher, P.; Fisseler-Eckhoff, A. Status quo of ALK testing in lung cancer: Results of an EQA scheme based on in-situ hybridization, immunohistochemistry, and RNA/DNA sequencing. Virchows Arch. 2021, 479, 247–255. [Google Scholar] [CrossRef]
- Vyberg, M.; Nielsen, S. Proficiency testing in immunohistochemistry—Experiences from nordic immunohistochemical quality control (NordiQC). Virchows Arch. 2016, 468, 19–29. [Google Scholar] [CrossRef]
- Pisapia, P.; Malapelle, U.; Roma, G.; Saddar, S.; Zheng, Q.; Pepe, F.; Bruzzese, D.; Vigliar, E.; Bellevicine, C.; Luthra, R. Consistency and reproducibility of next-generation sequencing in cytopathology: A second worldwide ring trial study on improved cytological molecular reference specimens. Cancer Cytopathol. 2019, 127, 285–296. [Google Scholar] [CrossRef]
- Ilié, M.; Lake, V.; de Alava, E.; Bonin, S.; Chlebowski, S.; Delort, A.; Dequeker, E.; Al-Dieri, R.; Diepstra, A.; Carpén, O. Standardization through education of molecular pathology: A spotlight on the European Masters in Molecular Pathology. Virchows Arch. 2024, 485, 761–775. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).