


Artificial Intelligence-Supported and App-Aided Cephalometric Analysis: Which One Can We Trust?

Abstract
1. Introduction
2. Materials and Methods
- *
- High-quality cephalograms that accurately demonstrated the cephalostat position without any artifacts that could obstruct the identification of anatomical sites.
- *
- Patients in permanent dentition stage with cephalometric radiographs obtained prior to orthodontic treatment.
- *
- Patients who did not have any significant deviations from normal.
- *
- Cephalograms where the landmarks were not clearly defined.
- *
- Cephalograms with significant double borders of the mandible.
- *
- Individuals with craniofacial anomalies, asymmetries, or a history of craniofacial surgery.
- *
- Individuals with significant dental abnormalities, diseases affecting cephalogram analysis, multiple missing teeth, or extensive crown-bridge restoration.
2.1. Study Design
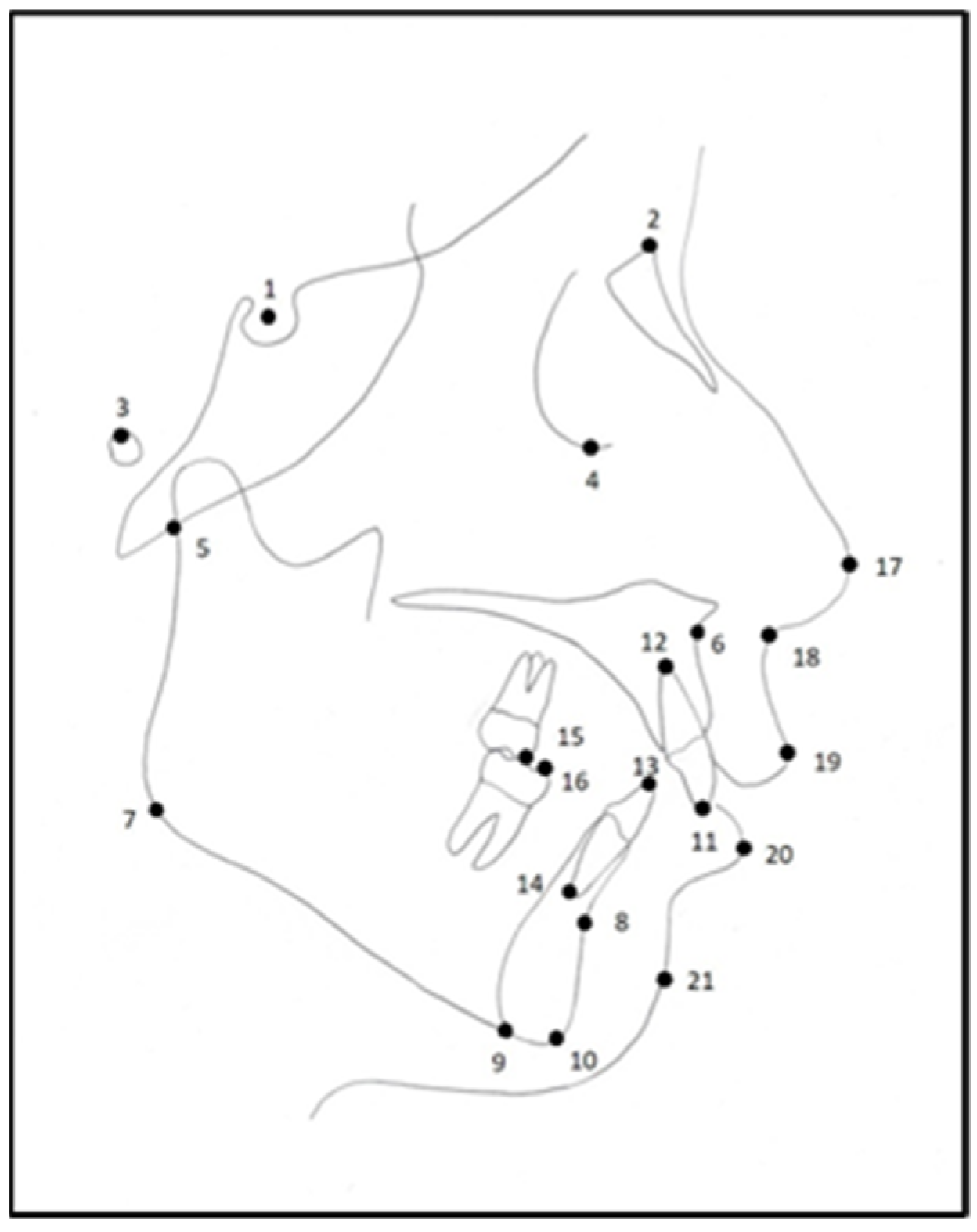
2.1.1. The Cephalometric Points Used in the Study
2.1.2. The Cephalometric Measurements Performed in the Study
2.1.3. The Cephalometric Analysis Methods Used in the Study
- 1.
- Manual Method:
- 2.
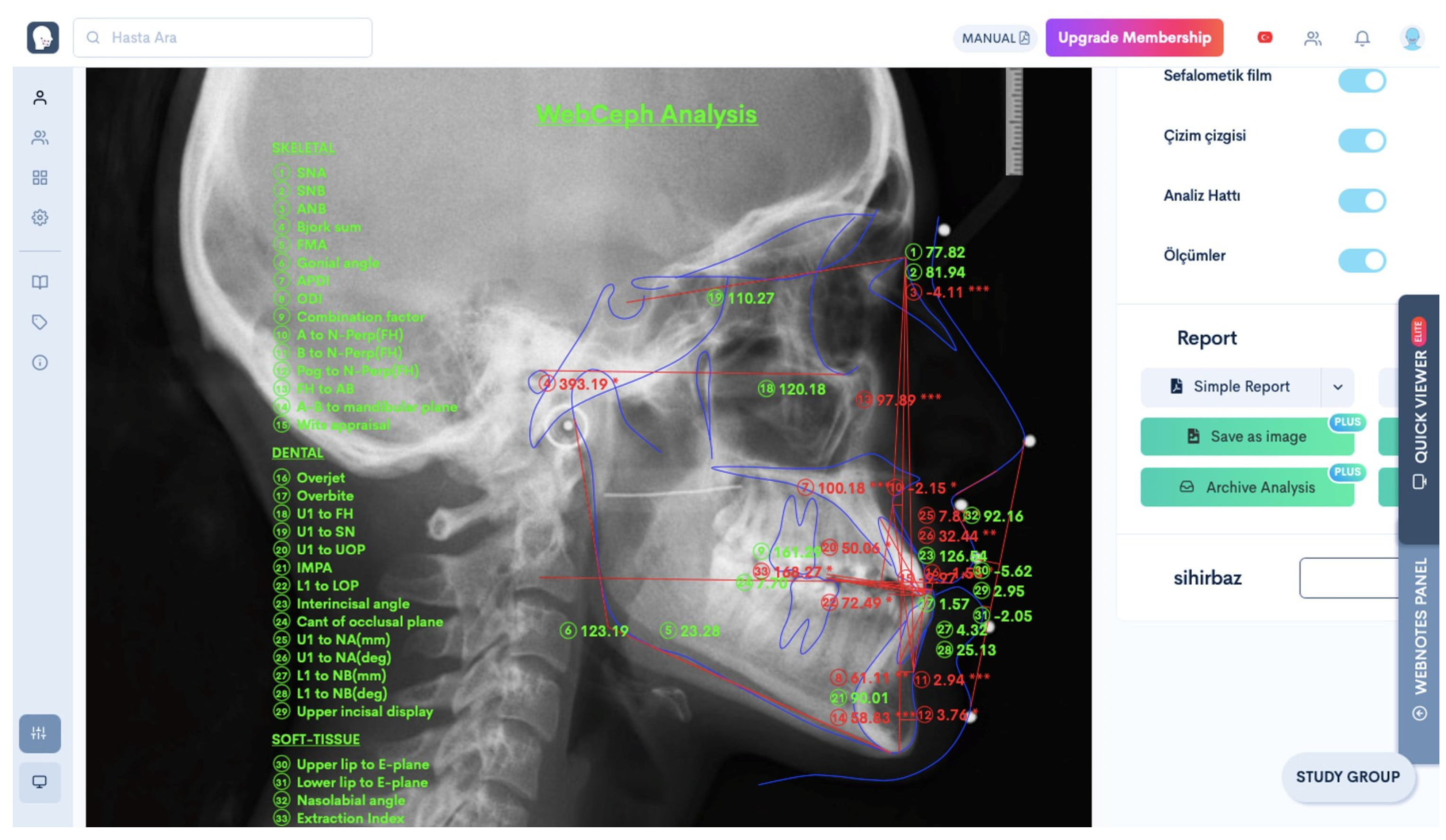
- WebCeph Analysis Software
- 3.
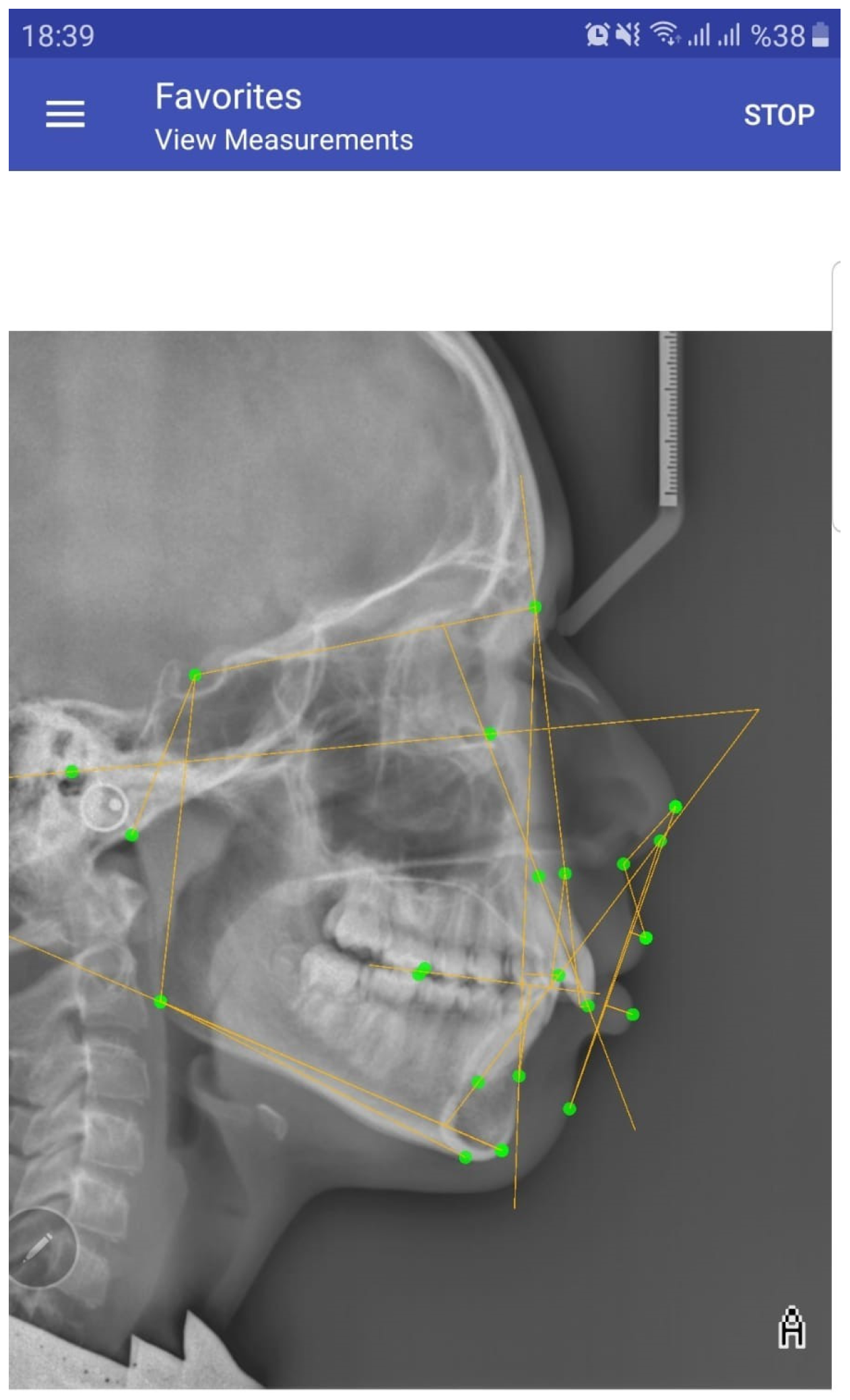
- OneCeph Analysis Application
2.2. Statistical Analysis
2.3. Method Error
3. Results
3.1. Intraobserver Reliability
3.2. Skeletal, Dental, and Soft Tissue Parameters
3.3. Duration of the Analysis
4. Discussion
5. Conclusions
- *
- All three cephalometric analysis methods were found to have a high degree of reproducibility.
- *
- The manual analysis method was found to be very highly compatible with the app-aided OneCeph cephalometric analysis program and highly compatible with the AI-supported WebCeph cephalometric analysis program, except for the SN, SNA, Gonial angle, Articular angle, U1-NA distance, and nasolabial angle measurements.
- *
- Both analysis methods can be reliably used as alternatives to the manual analysis method.
- *
- It was determined that the AI-supported WebCeph cephalometric analysis program was the fastest analysis program when compared to the other two analysis methods.
- *
- The app-aided OneCeph cephalometric analysis application is much more compatible with the ‘gold standard’ manual analysis method and allows for quicker analysis.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Broadbent, B.H. A new X-ray technique and its application to orthodontia. Angle Orthod. 1931, 1, 45–66. [Google Scholar]
- Baumrind, S.; Frantz, R. The reliability of head film measurements. Am. J. Orthod. 1971, 60, 111–127. [Google Scholar] [CrossRef] [PubMed]
- İşman, O. İki Farklı Sefalometrik Çizim ve Analiz Tekniğinin Sert ve Yumuşak Doku Analiz Sonuçlarının Karşılaştırılması. Ph.D. Thesis, Yeditepe University, Istanbul, Turkey, 2010. [Google Scholar]
- Houston, W.J.B.; Maher, R.E.; McElroy, D.; Sherriff, M. Sources of error in measurements from cephalometric radiographs. Eur. J. Orthod. 1986, 8, 149–151. [Google Scholar] [CrossRef] [PubMed]
- Levy-Mandel, A.D.; Venetsanopoulos, A.N.; Tsotsos, J.K. Knowledge-based landmarking of cephalograms. Comput. Biomed. Res. 1986, 3, 282–309. [Google Scholar] [CrossRef]
- Mahto, R.K. Evaluation of fully automated cephalometric measurements obtained from web-based artificial intelligence driven platform. BMC Oral Health 2022, 22, 132–140. [Google Scholar] [CrossRef]
- Barbhuiya, M.H.; Kumar, P.; Thakral, R.; Krishnapriya, R. Reliability of mobile application based cephalometric analysis for chair side Evaluation of orthodontic patient in clinical practice. J. Orthodont. Sci. 2021, 10, 16–21. [Google Scholar] [CrossRef]
- Zamrik, O.M.; İşeri, H. The reliability and reproducibility of an Android cephalometric smartphone application in comparison with the conventional method. Angle Orthod. 2021, 91, 236–242. [Google Scholar] [CrossRef]
- Meriç, P.; Nauomova, J. Web-based Fully Automated Cephalometric Analysis: Comparisons between App-aided, Computerized and Manual Tracings. Turkish J. Orthod. 2020, 33, 142–149. [Google Scholar] [CrossRef]
- Gottlieb, E.L.; Nelson, A.H.; Vogels, D.S., 3rd. Study of Orthodontic Diagnosis and Treatment Procedures. Part 1. Results and trends. J. Clin. Orthod. 1996, 30, 615–629. [Google Scholar]
- Schulze, R.K.W.; Gloede, M.B.; Doll, G.M. Landmark identification on direct digital versus film based cephalometric radiographs: A human skull study. Am. J. Orthod. Dentofacial. Orthop. 2002, 122, 635–642. [Google Scholar] [CrossRef]
- Paixão, M.B.; Sobra, M.C.; Vogel, C.J.; De Araujo, T.M. Comparative study between manual and digital cephalometric tracing using Dolphin Imaging software with lateral radiographs. Dent. Press. J. Orthod. 2010, 15, 123–130. [Google Scholar]
- Lagravère, M.O.; Low, C.; Flores-Mir, C.; Chung, R.; Carey, J.P.; Heo, G.; Major, P.W. Intraexaminer and interexaminer reliabilities of landmark identification on digitized lateral cephalograms and formatted 3-dimensional cone-beam computerized tomography images. Am. J. Orthod. Dentofacial Orthop. 2010, 137, 598–604. [Google Scholar] [CrossRef]
- Kiełczykowski, M.; Kaminski, K.; Perkowski, K.; Zadurska, M.; Czochrowska, E. Application of Artificial Intelligence (AI) in a Cephalometric Analysis: A Narrative Review. Diagnostics 2023, 13, 2640. [Google Scholar] [CrossRef] [PubMed]
- Sayinsu, K.; Işık, F.; Trakyalı, G.; Arun, T. An evaluation of the errors in cephalometric measurements on scanned cephalometric images and conventional tracings. Eur. J. Orthod. 2007, 29, 105–108. [Google Scholar] [CrossRef] [PubMed]
- Alessandri-Bonetti, A.; Sangalli, L.; Salerno, M.; Gallenzi, P. Reliability of Artificial Intelligence- Assisted Cephalometric Analysis- A Pilot Study. Biomedinformatics 2023, 3, 44–53. [Google Scholar] [CrossRef]
- Subramanian, A.K.; Chen, Y.; Almalki, A.; Sivamurty, G. Cephalometric Analysis in Orthodontics Using Artificial Intelligence-A Comprehensive Review. BioMed Res. Int. 2022, 6, 1880113. [Google Scholar] [CrossRef] [PubMed]
- Duran, G.S.; Gökmen, Ş.; Topsakal, K.G.; Görgülü, S. Evaluation of the accuracy of fully automatic cephalometric analysis software with artificial intelligence algorithm. Orthod. Craniofac. Res. 2023, 26, 481–490. [Google Scholar] [CrossRef] [PubMed]
- Çoban, G.; Öztürk, T.; Hashimi, N.; Yagci, A. Comparison between cephalometric measurements using digital manual and web-based artificial intelligence cephalometric tracing software. Dental Press. J. Orthod. 2022, 27, 222112. [Google Scholar] [CrossRef]
- Chen, Y.J.; Chen, S.K.; Yao, J.C.C.; Chang, H.F. The effects of differences in landmark identification on the cephalometric measurements in traditional versus digitized cephalometry. Angle Orthod. 2004, 74, 155–161. [Google Scholar]
- Sekiguchi, T.; Savara, B.S. Variability of cephalometric landmarks used for face growth studies. Am. J. Orthod. 1972, 61, 603–618. [Google Scholar] [CrossRef]
- Prince, S.T.T.; Dilip, S.; Sangeetha, D.; Ravi, K.; Krishnaraj, R. Reproducibility of linear and angular cephalometric measurements obtained by an artificial-intelligence assisted software (WebCeph) in comparison with digital software (AutoCEPH) and manual tracing method. Dental Press. J. Orthod. 2023, 28, 2321214. [Google Scholar] [CrossRef]
- Junaid, N.; Khan, N.; Ahmed, N.; Abbasi, M.S.; Das, G.; Maqsood, A.; Ahmed, A.R.; Marya, A.; Alam, M.K.; Heboyan, A. Development, Application, and Performance of Artificial Intelligence in Cephalometric Landmark Identification and Diagnosis: A Systematic Review. Healthcare 2022, 10, 2454. [Google Scholar] [CrossRef] [PubMed]
- Shettigar, P.; Shetty, S.; Naik, R.D.; Basavaraddi, S.M.; Patil, A.K. A comparative evaluation of reliability of an android-based app and computerized cephalometric tracing program for orthodontic cephalometric analysis. Biomed. Pharmacol. J. 2019, 12, 341–346. [Google Scholar] [CrossRef]
- Shrestha, R.; Kandel, S. A Comparative Study on Use of Manual Versus Digital Method using Mobile Application for Cephalometric Measurements Orthodontic. J. Nepal 2020, 10, 11–16. [Google Scholar]
- Aksakallı, S.; Yılancı, H.; Görükmez, E.; Ramoğlu, S.İ. Reliability Assesment of Orthodontic Apps for Cephalometrics. Turkish J. Orthod. 2016, 9, 98–102. [Google Scholar]
- Leonardi, R.; Giordano, D.; Maiorana, F.; Spampinato, C. Automatic cephalometric analysis. Angle Orthod. 2008, 78, 145–151. [Google Scholar] [CrossRef]
- Geelen, W.; Wenzel, A.; Gotfredsen, E.; Kruger, M.; Hansson, L.G. Reproducibility of cephalometric landmarks on conventional film, hard- copy, and monitor-displayed images obtained by the storage phosphor technique. Eur. J. Orthod. 1998, 20, 331–340. [Google Scholar] [CrossRef]
- Chen, S.K.; Chen, Y.J.; Yao, C.C.; Chang, H.F. Enhanced speed and precision of measurement in a computer-assisted digital cephalometric analysis system. Angle Orthod. 2004, 74, 501–507. [Google Scholar]
- Sayar, G.; Kilinc, D.D. Manual tracing versus smartphone application (app) tracing: A comparative study. Acta Odontol. Scand. 2017, 75, 588–594. [Google Scholar] [CrossRef]
- Hwang, H.W.; Park, J.H.; Moon, J.H. Automated identification of cephalometric landmarks: Part 2-Might it be better than human? Angle Orthod. 2020, 90, 69–76. [Google Scholar] [CrossRef]
- Bao, H.; Zhang, K.; Yu, C.; Li, H.; Cao, D.; Shu, H.; Liu, L.; Yan, B. Evaluating the accuracy of automated cephalometric analysis based on artificial intelligence. BMC Oral Health 2023, 23, 191–201. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Skeletal Measurements | |
| S-N (mm) | Distance between the Sella point and Nasion point |
| SNA (°) | Angle between the Sella–Nasion line and the Nasion–Point A line |
| SNB (°) | Angle between the Sella–Nasion line and the Nasion–Point B line |
| ANB (°) | Angle between the Nasion–A and Nasion–B lines |
| WITTS (mm) | Distance between the perpendiculars drawn from Points A and B to the occlusal plane |
| GOGN-SN (°) | Angle between the Sella–Nasion line and the Gonion–Gnation line |
| FMA (°) | Angle between the Porion–Orbitale line and the Gonion–Menton line |
| SADDLE (°) | Angle between the Sella, Nasion, and Articular points |
| GONIAL (°) | Angle between the Articular, Gonion, and Menton points |
| ARTICULAR (°) | Angle between the Sella, Articular, and Gonion points |
| SUM (°) | Sum of the Saddle angle, Gonial angle, and Articular angle |
| Dental Measurements | |
| U1-NA ANGLE (°) | Angle between the long axis of the upper first incisor tooth and the N–A line |
| U1-NA DISTANCE (mm) | Sagittal distance from the most anterior point of the crown of the upper first incisor tooth to the N–A line |
| L1-NB ANGLE (°) | Angle between the long axis of the lower first incisor tooth and the N–B line |
| L1-NB DISTANCE (mm) | Sagittal distance from the most anterior point of the crown of the lower first incisor tooth to the N–B line |
| IMPA (°) | Angle between the long axis of the lower first incisor and the mandibular plane |
| INTERINCISAL ANGLE (°) | Angle between the long axis of the upper first incisor tooth and the long axis of the lower first incisor tooth |
| Soft Tissue Measurements | |
| LS-E (mm) | Distance from the Labium Superior point to Plane E |
| LI-E (mm) | Distance from the Labium Inferior point to Plane E |
| NASOLABIAL ANGLE (°) | Angle between the Pronasale, Subnasale, and Labium Superior points |
| Skeletal Parameters | Correlation Coefficients Between the Methods | |||||
|---|---|---|---|---|---|---|
| Correlation Between the Methods | Confidence Interval of 95% | |||||
| Lower Threshold | Upper Threshold | p | ||||
| 1 | SN-MAN (mm) | SN MAN-SN WEB | 0.215 | −0.137 | 0.473 | 0.005 |
| 2 | SN-WEB (mm) | SN MAN-SN ONE | 0.939 | 0.911 | 0.958 | 0.000 |
| 3 | SN-ONE (mm) | SN WEB-SN ONE | 0.175 | −0.125 | 0.413 | 0.021 |
| 1 | SNA-MAN (°) | SNA MAN-SNA WEB | 0.692 | 0.390 | 0.826 | 0.000 |
| 2 | SNA-WEB (°) | SNA MAN-SNA ONE | 0.875 | 0.808 | 0.917 | 0.000 |
| 3 | SNA-ONE (°) | SNA WEB-SNA ONE | 0.798 | 0.681 | 0.869 | 0.000 |
| 1 | SNB-MAN (°) | SNB MAN-SNB WEB | 0.883 | 0.829 | 0.920 | 0.000 |
| 2 | SNB-WEB (°) | SNB MAN-SNB ONE | 0.912 | 0.862 | 0.943 | 0.000 |
| 3 | SNB-ONE (°) | SNB WEB-SNB ONE | 0.911 | 0.870 | 0.939 | 0.000 |
| 1 | ANB-MAN (°) | ANB MAN-ANB WEB | 0.845 | 0.434 | 0.934 | 0.000 |
| 2 | ANB-WEB (°) | ANB MAN-ANB ONE | 0.944 | 0.919 | 0.962 | 0.000 |
| 3 | ANB-ONE (°) | ANB WEB-ANB ONE | 0.873 | 0.482 | 0.948 | 0.000 |
| 1 | Witts-MAN (mm) | Witts MAN–Witts WEB | 0.906 | 0.863 | 0.936 | 0.000 |
| 2 | Witts-WEB (mm) | Witts MAN–Witts ONE | 0.892 | 0.821 | 0.932 | 0.000 |
| 3 | Witts-ONE (mm) | Witts WEB–Witts ONE | 0.915 | 0.781 | 0.957 | 0.000 |
| 1 | GoGn/SN-MAN (°) | GoGn/SN MAN-GoGn/SN WEB | 0.953 | 0.931 | 0.968 | 0.000 |
| 2 | GoGn/SN-WEB (°) | GoGn/SN MAN-GoGn/SN ONE | 0.963 | 0.946 | 0.975 | 0.000 |
| 3 | GoGn/SN-ONE (°) | GoGn/SN WEB-GoGn/SN ONE | 0.952 | 0.917 | 0.970 | 0.000 |
| 1 | FMA-MAN (°) | FMA MAN-FMA WEB | 0.933 | 0.700 | 0.973 | 0.000 |
| 2 | FMA-WEB (°) | FMA MAN-FMA ONE | 0.827 | 0.263 | 0.932 | 0.000 |
| 3 | FMA-ONE (°) | FMA WEB-FMA ONE | 0.891 | 0.805 | 0.934 | 0.000 |
| 1 | Saddle-MAN (°) | Saddle MAN–Saddle WEB | 0.849 | 0.468 | 0.935 | 0.000 |
| 2 | Saddle-WEB (°) | Saddle MAN–Saddle ONE | 0.866 | 0.358 | 0.949 | 0.000 |
| 3 | Saddle-ONE (°) | Saddle WEB–Saddle ONE | 0.928 | 0.895 | 0.950 | 0.000 |
| 1 | Gonial-MAN (°) | GoniaL-MAN–Gonial WEB | 0.706 | −0.188 | 0.898 | 0.000 |
| 2 | Gonial-WEB (°) | Gonial-MAN–Gonial ONE | 0.916 | 0.867 | 0.945 | 0.000 |
| 3 | Gonial-ONE (°) | Gonial-WEB–Gonial ONE | 0.78 | −0.135 | 0.927 | 0.000 |
| 1 | Articular-MAN (°) | Articular MAN–Articular WEB | 0.732 | −0.129 | 0.904 | 0.000 |
| 2 | Articular-WEB (°) | Articular MAN–Articular ONE | 0.892 | 0.623 | 0.953 | 0.000 |
| 3 | Articular-ONE (°) | Articular WEB–Articular ONE | 0.825 | 0.558 | 0.913 | 0.000 |
| 1 | SUM-MAN (°) | SUM MAN-SUM WEB | 0.890 | 0.840 | 0.925 | 0.000 |
| 2 | SUM-WEB (°) | SUM MAN-SUM ONE | 0.883 | 0.845 | 0.927 | 0.000 |
| 3 | SUM-ONE (°) | SUM WEB-SUM ONE | 0.943 | 0.858 | 0.971 | 0.000 |
| Dental Parameters | Correlation Coefficients Between the Methods | |||||
|---|---|---|---|---|---|---|
| ICC | Confidence Interval of 95% | |||||
| Lower Threshold | Upper Threshold | p | ||||
| 1 | U1/NA-MAN (°) | U1/NA MAN-U1/NA WEB | 0.89 | 0.673 | 0.949 | 0.000 |
| 2 | U1/NA-WEB (°) | U1/NA MAN-U1/NA ONE | 0.94 | 0.790 | 0.973 | 0.000 |
| 3 | U1/NA-ONE (°) | U1/NA WEB-U1/NA ONE | 0.911 | 0.869 | 0.939 | 0.000 |
| 1 | U1-NA-MAN (mm) | U1-NA MAN-U1-NA WEB | 0.767 | 0.576 | 0.861 | 0.000 |
| 2 | U1-NA-WEB (mm) | U1-NA MAN-U1-NA ONE | 0.901 | 0.856 | 0.932 | 0.000 |
| 3 | U1-NA-ONE (mm) | U1-NA WEB-U1-NA ONE | 0.745 | 0.589 | 0.837 | 0.000 |
| 1 | L1/NB-MAN (°) | L1/NB MAN-L1/NB WEB | 0.862 | 0.527 | 0.940 | 0.000 |
| 2 | L1/NB-WEB (°) | L1/NB MAN-L1/NB ONE | 0.948 | 0.809 | 0.978 | 0.000 |
| 3 | L1/NB-ONE (°) | L1/NB WEB-L1/NB ONE | 0.91 | 0.862 | 0.940 | 0.000 |
| 1 | L1-NB-MAN (mm) | L1-NB MAN-L1-NB WEB | 0.947 | 0.921 | 0.964 | 0.000 |
| 2 | L1-NB-WEB (mm) | L1-NB MAN-L1-NB ONE | 0.96 | 0.942 | 0.973 | 0.000 |
| 3 | L1-NB-ONE (mm) | L1-NB WEB-L1-NB ONE | 0.959 | 0.929 | 0.974 | 0.000 |
| 1 | IMPA-MAN (°) | IMPA MAN-IMPA WEB | 0.902 | 0.767 | 0.949 | 0.000 |
| 2 | IMPA-WEB (°) | IMPA MAN-IMPA ONE | 0.937 | 0.896 | 0.960 | 0.000 |
| 3 | IMPA-ONE (°) | IMPA WEB-IMPA ONE | 0.833 | 0.508 | 0.923 | 0.000 |
| 1 | Interincisal-MAN (°) | Interincisal MAN–Interinc WEB | 0.914 | 0.392 | 0.971 | 0.000 |
| 2 | Interincisal-WEB (°) | Interincisal MAN–Interinc ONE | 0.943 | 0.579 | 0.980 | 0.000 |
| 3 | Interincisal-ONE (°) | Interincisal WEB–Interinc ONE | 0.955 | 0.934 | 0.969 | 0.000 |
| Soft Tissue Parameters | Correlation Coefficients | |||||
|---|---|---|---|---|---|---|
| ICC | Confidence Interval of 95% | |||||
| Lower Threshold | Upper Threshold | p | ||||
| 1 | Ls-E MAN (mm) | Ls-E MAN-LS-E WEB | 0.93 | 0.898 | 0.952 | 0.000 |
| 2 | Ls-E WEB (mm) | Ls-E MAN-LS-E ONE | 0.949 | 0.917 | 0.967 | 0.000 |
| 3 | Ls-E ONE (mm) | Ls-E WEB-LS-E ONE | 0.955 | 0.908 | 0.975 | 0.000 |
| 1 | Li-E MAN (mm) | Li-E MAN-Li-E WEB | 0.937 | 0.872 | 0.964 | 0.000 |
| 2 | Li-E WEB (mm) | Li-E MAN-Li-E ONE | 0.964 | 0.937 | 0.978 | 0.000 |
| 3 | Li-E ONE (mm) | Li-E WEB-Li-E ONE | 0.966 | 0.949 | 0.977 | 0.000 |
| 1 | NL-MAN (°) | NL MAN-NL WEB | 0.588 | −0.099 | 0.813 | 0.000 |
| 2 | NL-WEB (°) | NL MAN-NL ONE | 0.678 | 0.530 | 0.780 | 0.000 |
| 3 | NL-ONE (°) | NL WEB-NL ONE | 0.505 | −0.177 | 0.769 | 0.000 |
| Group | Kruskal–Wallis H Test | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| n | Mean | Median | Min | Max | Standard Deviation | H | p | Paired Comparison | ||
| Time (min) | 1 = MANUAL | 30 | 9.10 | 9.11 | 8.55 | 9.38 | 0.17 | 79.419 | 0.0001 | 2–1 |
| 2 = WEBCEPH | 30 | 1.25 | 1.24 | 1.23 | 1.35 | 0.03 | 2–3 | |||
| 3 = ONECEPH | 30 | 2.14 | 2.14 | 2.10 | 2.20 | 0.02 | 3–1 | |||
| TOTAL | 90 | 4.16 | 2.14 | 1.23 | 9.38 | 3.53 | ||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Koz, S.; Uslu-Akcam, O. Artificial Intelligence-Supported and App-Aided Cephalometric Analysis: Which One Can We Trust? Diagnostics 2025, 15, 559. https://doi.org/10.3390/diagnostics15050559
Koz S, Uslu-Akcam O. Artificial Intelligence-Supported and App-Aided Cephalometric Analysis: Which One Can We Trust? Diagnostics. 2025; 15(5):559. https://doi.org/10.3390/diagnostics15050559
Chicago/Turabian StyleKoz, Senol, and Ozge Uslu-Akcam. 2025. "Artificial Intelligence-Supported and App-Aided Cephalometric Analysis: Which One Can We Trust?" Diagnostics 15, no. 5: 559. https://doi.org/10.3390/diagnostics15050559
APA StyleKoz, S., & Uslu-Akcam, O. (2025). Artificial Intelligence-Supported and App-Aided Cephalometric Analysis: Which One Can We Trust? Diagnostics, 15(5), 559. https://doi.org/10.3390/diagnostics15050559