
Twelve-Month Outcomes and Optical Coherence Tomography (OCT) Biomarkers After Intravitreal Dexamethasone Implantation in Pseudophakic Eyes with Post-Vitrectomy Cystoid Macular Edema (CME)—Refractory to Medical Therapy

 , , , , and
, , , , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Surgical Procedure
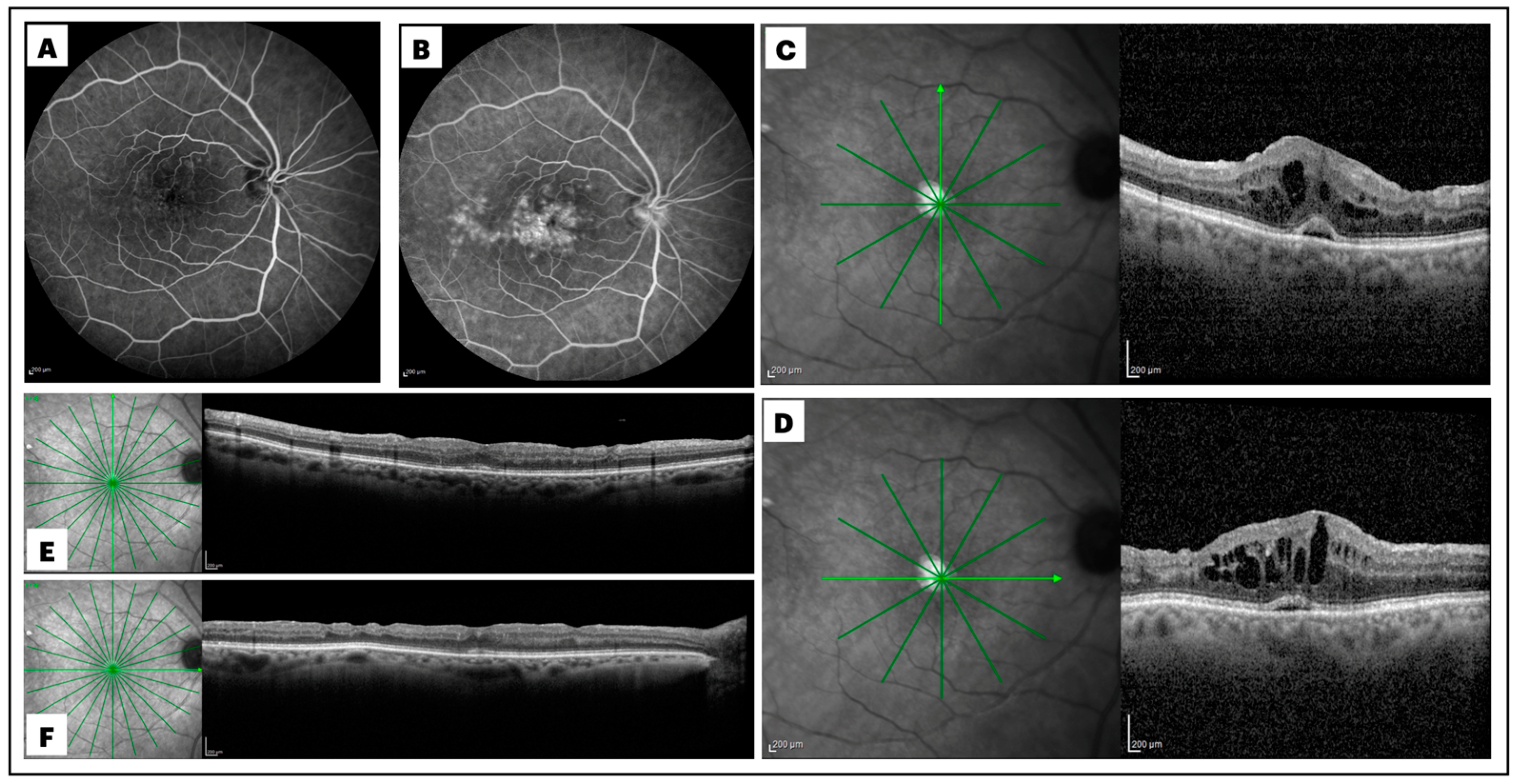
2.2. Definition and Diagnosis of Post-Surgical Macular Edema
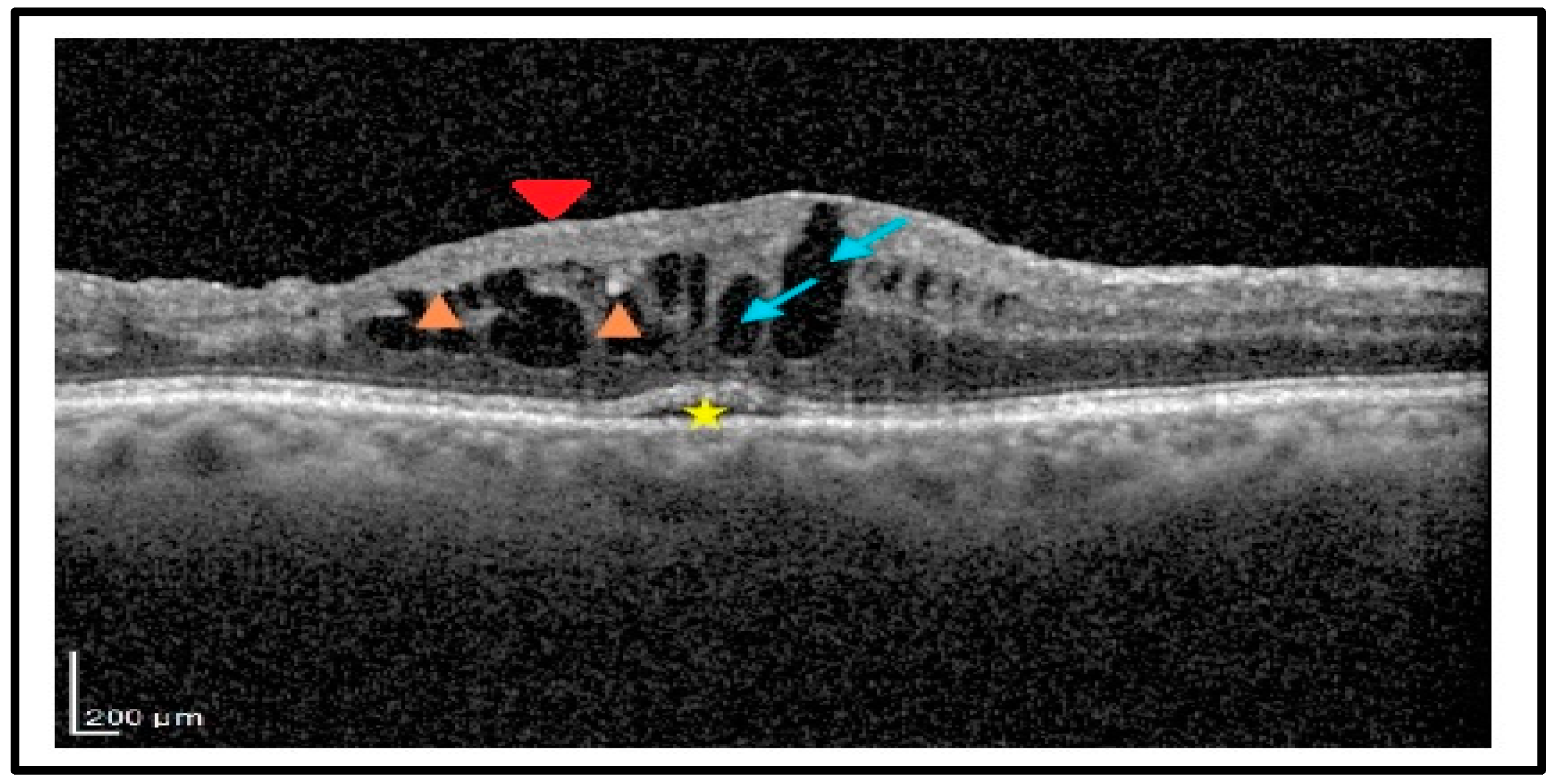
2.3. Analysis of the Biomarkers
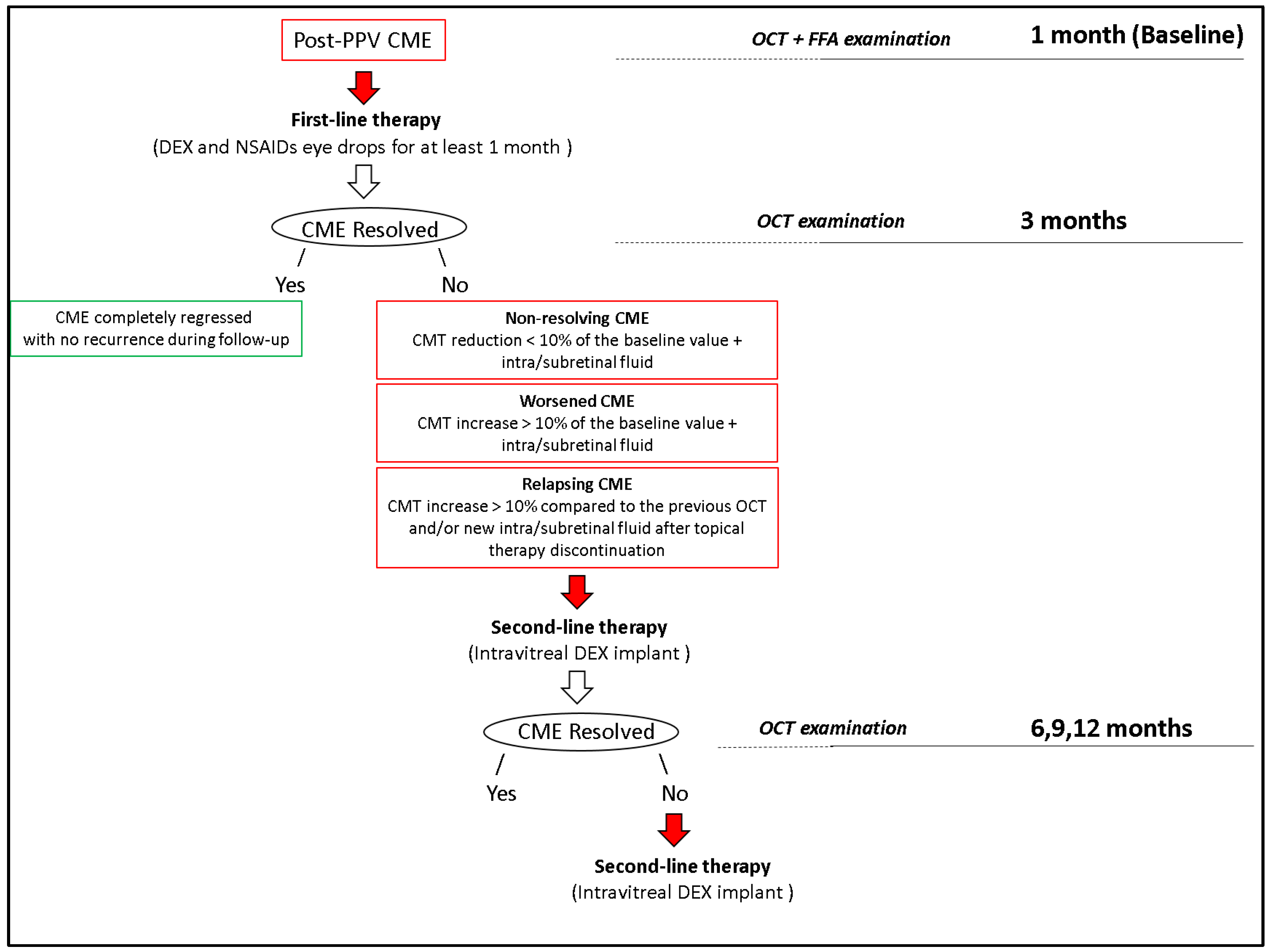
2.4. Treatment of Post-Surgical Macular Edema
2.5. Statistical Analysis
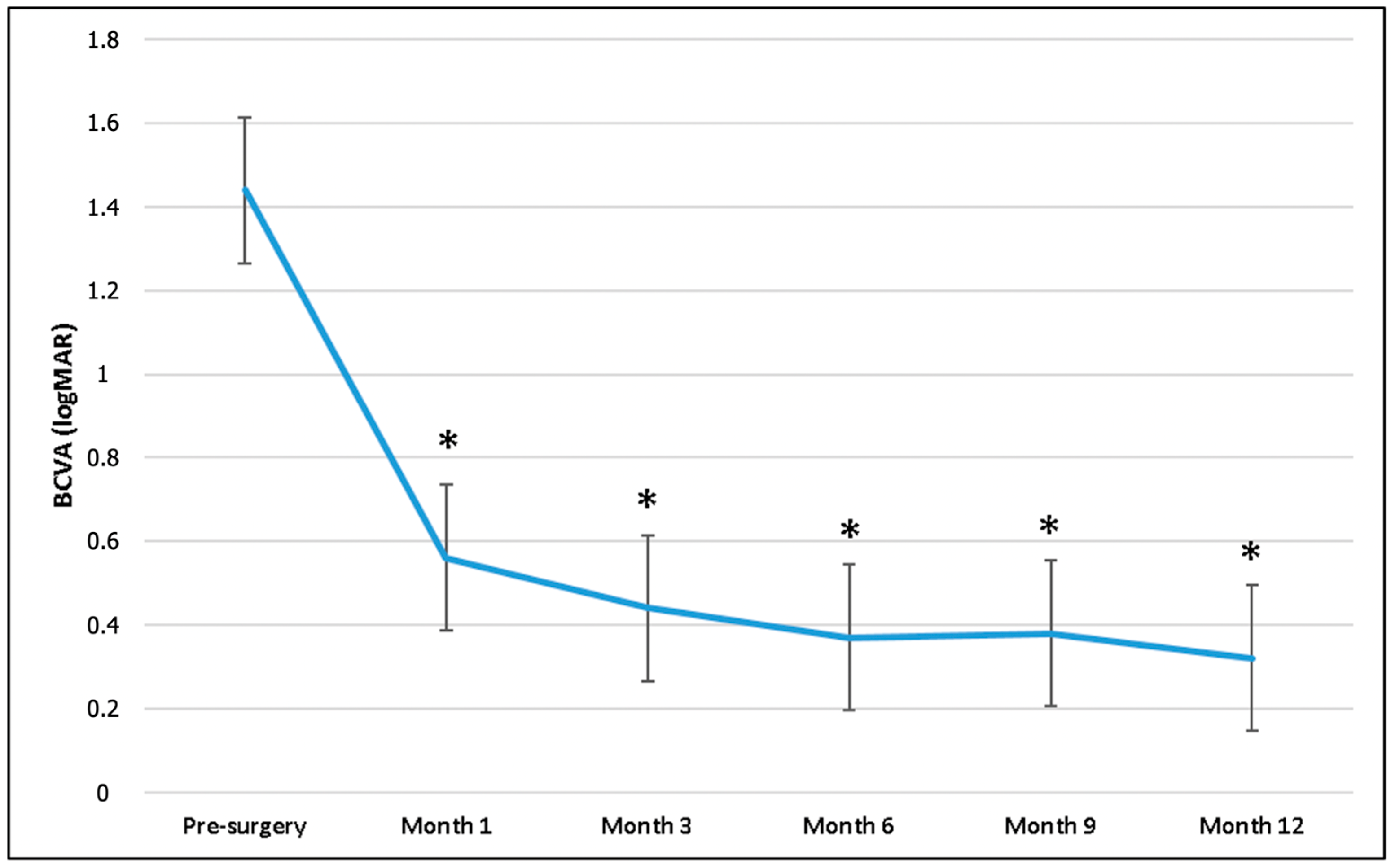
3. Results
3.1. Treatment Exposure
3.2. Analysis of the Correlations
3.3. Safety
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
List of Abbreviations
| AMD | age-related macular degeneration |
| BBG | brilliant blue G |
| BCVA | best-corrected visual acuity |
| BSS | balanced salt solution |
| CME | cystoid macular edema |
| CMT | central macular thickness |
| C3F8 | octafluoropropane |
| DEX | dexamethasone |
| DME | diabetic macular edema |
| DRIL | disorganization of inner retinal layers |
| DROL | disorganization of outer retinal layers |
| ELM | external limiting membrane |
| ERM | epiretinal membrane |
| ETDRS | Early Treatment Diabetic Retinopathy Study |
| EZ | ellipsoid zone |
| HRF | hyper-reflective foci |
| ILM | internal limiting membrane |
| IOP | intraocular pressure |
| IRB | Institutional Review Board |
| IRC | intraretinal cysts |
| IRF | intraretinal fluid |
| LMHs | lamellar macular holes |
| LogMAR | Logarithm of the Minimum Angle of Resolution |
| NSAIDs | nonsteroidal anti-inflammatory drugs |
| OCT | optical coherence tomography |
| PFCL | perfluorcarbon liquid |
| PVD | posterior vitreous detachment |
| PPV | pars plana vitrectomy |
| RVO | retinal vein occlusion |
| PVR | proliferative vitreoretinopathy |
| RRD | rhegmatogenous retinal detachment |
| SD-OCT | spectral domain OCT |
| SF6 | sulfur hexafluoride |
| SO | silicone oil |
| SRF | subretinal fluid |
| TB | trypan blue |
| VEGF | vascular endothelial growth factor |
| VH | vitreous hemorrhage |
References
- Romano, V.; Angi, M.; Scotti, F.; Del Grosso, R.; Romano, D.; Semeraro, F.; Vinciguerra, P.; Costagliola, C.; Romano, M.R. Inflammation and Macular Oedema after Pars Plana Vitrectomy. Mediat. Inflamm. 2013, 2013, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Zur, D.; Loewenstein, A. Postsurgical Cystoid Macular Edema. In Developments in Ophthalmology; Coscas, G., Loewenstein, A., Cunha-Vaz, J., Soubrane, G., Eds.; S. Karger AG: Basel, Switzerland, 2017; Volume 58, pp. 178–190. ISBN 978-3-318-06032-4. [Google Scholar]
- Iuliano, L.; Cisa Di Gresy, G.; Fogliato, G.; Corbelli, E.; Bandello, F.; Codenotti, M. Increased Risk of Postsurgical Macular Edema in High Stage Idiopathic Epiretinal Membranes. Eye Vis. 2021, 8, 29. [Google Scholar] [CrossRef] [PubMed]
- Bernabei, F.; Marcireau, I.; Frongia, F.; Azan, F.; Vagge, A.; Peiretti, E.; Guerrier, G.; Rothschild, P.-R. Risk Factors of Cystoid Macular Edema After Pars Plana Vitrectomy for Pseudophakic Retinal Detachment. Ophthalmol. Ther. 2023, 12, 1737–1745. [Google Scholar] [CrossRef] [PubMed]
- Bellocq, D.; Korobelnik, J.-F.; Burillon, C.; Voirin, N.; Dot, C.; Souied, E.; Conrath, J.; Milazzo, S.; Massin, P.; Baillif, S.; et al. Effectiveness and Safety of Dexamethasone Implants for Post-Surgical Macular Oedema Including Irvine-Gass Syndrome: The EPISODIC Study. Br. J. Ophthalmol. 2015, 99, 979–983. [Google Scholar] [CrossRef] [PubMed]
- Chu, C.J.; Johnston, R.L.; Buscombe, C.; Sallam, A.B.; Mohamed, Q.; Yang, Y.C. Risk Factors and Incidence of Macular Edema after Cataract Surgery. Ophthalmology 2016, 123, 316–323. [Google Scholar] [CrossRef] [PubMed]
- Yao, H.; Yang, Z.; Cheng, Y.; Shen, X. Macular Changes Following Cataract Surgery in Eyes with Early Diabetic Retinopathy: An OCT and OCT Angiography Study. Front. Med. 2023, 10, 1290599. [Google Scholar] [CrossRef] [PubMed]
- Parisi, G.; Fallico, M.; Avitabile, T.; Longo, A.; Ortisi, E.; Russo, A.; Petrillo, F.; Maugeri, A.; Barchitta, M.; Bonfiglio, V.; et al. Intravitreal Dexamethasone Implant for Postoperative Macular Oedema Secondary to Vitrectomy for Epiretinal Membrane and Retinal Detachment: A Systematic Review and Meta-Analysis. J. Ophthalmol. 2021, 2021, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Chatziralli, I.; Dimitriou, E.; Theodossiadis, G.; Chatzirallis, A.; Kazantzis, D.; Theodossiadis, P. Treatment of Macular Edema after Pars Plana Vitrectomy for Idiopathic Epiretinal Membrane Using Intravitreal Dexamethasone Implant: Long-Term Outcomes. Ophthalmologica 2019, 242, 16–21. [Google Scholar] [CrossRef]
- Freissinger, S.; Vounotrypidis, E.; Wolf, A.; Kortuem, K.U.; Shajari, M.; Sakkias, F.; Herold, T.; Priglinger, S.G.; Mayer, W.J. Evaluation of Functional Outcomes and OCT-Biomarkers after Intravitreal Dexamethasone Implant for Postoperative Cystoid Macular Edema in Vitrectomized Eyes. J. Ophthalmol. 2020, 2020, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Pignatelli, F.; Nacucchi, A.; Niro, A.; Gigliola, S.; Passidomo, F.; Donghia, R.; Addabbo, G. Intravitreal Dexamethasone Implant at the Time of Silicone Oil Removal to Treat Persistent Macular Edema after Rhegmatogenous Retinal Detachment Repair. JCM 2023, 12, 1697. [Google Scholar] [CrossRef]
- Markan, A.; Agarwal, A.; Arora, A.; Bazgain, K.; Rana, V.; Gupta, V. Novel Imaging Biomarkers in Diabetic Retinopathy and Diabetic Macular Edema. Ophthalmol. Eye. Dis. 2020, 12, 251584142095051. [Google Scholar] [CrossRef]
- Costanzo, E.; Giannini, D.; De Geronimo, D.; Fragiotta, S.; Varano, M.; Parravano, M. Prognostic Imaging Biomarkers in Diabetic Macular Edema Eyes Treated with Intravitreal Dexamethasone Implant. JCM 2023, 12, 1303. [Google Scholar] [CrossRef]
- Visioli, G.; Alisi, L.; Mastrogiuseppe, E.; Albanese, G.M.; Romano, E.; Iannetti, L.; Armentano, M.; Giovannetti, F.; Gharbiya, M. OCT Biomarkers as Predictors of Visual Improvement in Diabetic Macular Edema Eyes Receiving Dexamethasone Implants. Int. J. Retin. Vitr. 2023, 9, 35. [Google Scholar] [CrossRef]
- Metrangolo, C.; Donati, S.; Mazzola, M.; Fontanel, L.; Messina, W.; D’alterio, G.; Rubino, M.; Radice, P.; Premi, E.; Azzolini, C. OCT Biomarkers in Neovascular Age-Related Macular Degeneration: A Narrative Review. J. Ophthalmol. 2021, 2021, 1–16. [Google Scholar] [CrossRef]
- Castro-Navarro, V.; Monferrer-Adsuara, C.; Navarro-Palop, C.; Montero-Hernández, J.; Cervera-Taulet, E. Optical Coherence Tomography Biomarkers in Patients with Macular Edema Secondary to Retinal Vein Occlusion Treated with Dexamethasone Implant. BMC Ophthalmol. 2022, 22, 191. [Google Scholar] [CrossRef]
- Guigou, S.; Pommier, S.; Meyer, F.; Hajjar, C.; Merite, P.Y.; Parrat, E.; Rouhette, H.; Rebollo, O.; Matonti, F. Efficacy and Safety of Intravitreal Dexamethasone Implant in Patients with Diabetic Macular Edema. Ophthalmologica 2015, 233, 169–175. [Google Scholar] [CrossRef] [PubMed]
- Leisser, C.; Hirnschall, N.; Findl, O. Effect of Phacoemulsification on Outcomes after Vitrectomy with Membrane Peeling Regarding New Intraretinal Cystoid Changes and Transient Macular Edema. Ophthalmologica 2021, 244, 150–158. [Google Scholar] [CrossRef] [PubMed]
- Park, S.W.; Kim, H.K.; Zaidi, M.H.; Byon, I.S.; Lee, J.E.; Nguyen, Q.D. Cystoid Macular Edema after Vitrectomy and after Phacovitrectomy for Epiretinal Membrane. Can. J. Ophthalmol. 2024, 59, e596–e602. [Google Scholar] [CrossRef]
- Leisser, C.; Hirnschall, N.; Hackl, C.; Döller, B.; Varsits, R.; Ullrich, M.; Kefer, K.; Karl, R.; Findl, O. Risk Factors for Postoperative Intraretinal Cystoid Changes after Peeling of Idiopathic Epiretinal Membranes among Patients Randomized for Balanced Salt Solution and Air-tamponade. Acta Ophthalmol. 2018, 96. [Google Scholar] [CrossRef]
- Frisina, R.; Pinackatt, S.J.; Sartore, M.; Monfardini, A.; Baldi, A.; Cesana, B.M.; Semeraro, F.; Bratu, A.; Parolini, B. Cystoid Macular Edema after Pars Plana Vitrectomy for Idiopathic Epiretinal Membrane. Graefes Arch. Clin. Exp. Ophthalmol. 2015, 253, 47–56. [Google Scholar] [CrossRef] [PubMed]
- Kontou, E.P.; Karakosta, C.; Kounas, K.; Iatropoulos, I.; Tsinopoulos, I.; Kozombolis, V.; Stavrakas, P. Macular Edema Following Silicone Oil Tamponade for Retinal Detachment: A Literature Review. Cureus 2023, 15, e51233. [Google Scholar] [CrossRef] [PubMed]
- Merad, M.; Vérité, F.; Baudin, F.; Ghezala, I.B.; Meillon, C.; Bron, A.M.; Arnould, L.; Eid, P.; Creuzot-Garcher, C.; Gabrielle, P.-H. Cystoid Macular Edema after Rhegmatogenous Retinal Detachment Repair with Pars Plana Vitrectomy: Rate, Risk Factors, and Outcomes. JCM 2022, 11, 4914. [Google Scholar] [CrossRef]
- Pole, C.; Chehaibou, I.; Govetto, A.; Garrity, S.; Schwartz, S.D.; Hubschman, J.-P. Macular Edema after Rhegmatogenous Retinal Detachment Repair: Risk Factors, OCT Analysis, and Treatment Responses. Int. J. Retin. Vitr. 2021, 7, 9. [Google Scholar] [CrossRef] [PubMed]
- Govetto, A.; Su, D.; Farajzadeh, M.; Megerdichian, A.; Platner, E.; Ducournau, Y.; Virgili, G.; Hubschman, J.P. Microcystoid Macular Changes in Association With Idiopathic Epiretinal Membranes in Eyes With and Without Glaucoma: Clinical Insights. Am. J. Ophthalmol. 2017, 181, 156–165. [Google Scholar] [CrossRef]
- Cicinelli, M.V.; Post, M.; Brambati, M.; Rabiolo, A.; Pignatelli, F.; Szaflik, J.P.; Bandello, F.; Coppola, M. Associated Factors And Surgical Outcomes Of Microcystoid Macular Edema And Cone Bouquet Abnormalities In Eyes With Epiretinal Membrane. Retina 2022, 42, 1455–1464. [Google Scholar] [CrossRef] [PubMed]
- Burggraaff, M.C.; Trieu, J.; De Vries-Knoppert, W.A.E.J.; Balk, L.; Petzold, A. The Clinical Spectrum of Microcystic Macular Edema. Invest. Ophthalmol. Vis. Sci. 2014, 55, 952. [Google Scholar] [CrossRef]
- Benhamou, N.; Massin, P.; Haouchine, B.; Audren, F.; Tadayoni, R.; Gaudric, A. Intravitreal Triamcinolone for Refractory Pseudophakic Macular Edema. Am. J. Ophthalmol. 2003, 135, 246–249. [Google Scholar] [CrossRef]
- Williams, G.A.; Haller, J.A.; Kuppermann, B.D.; Blumenkranz, M.S.; Weinberg, D.V.; Chou, C.; Whitcup, S.M. Dexamethasone Posterior-Segment Drug Delivery System in the Treatment of Macular Edema Resulting from Uveitis or Irvine-Gass Syndrome. Am. J. Ophthalmol. 2009, 147, 1048–1054.e2. [Google Scholar] [CrossRef] [PubMed]
- Barone, A.; Russo, V.; Prascina, F.; Noci, N.D. Short-Term Safety And Efficacy Of Intravitreal Bevacizumab For Pseudophakic Cystoid Macular Edema. Retina 2009, 29, 33–37. [Google Scholar] [CrossRef]
- Fallico, M.; Maugeri, A.; Romano, G.L.; Bucolo, C.; Longo, A.; Bonfiglio, V.; Russo, A.; Avitabile, T.; Barchitta, M.; Agodi, A.; et al. Epiretinal Membrane Vitrectomy With and Without Intraoperative Intravitreal Dexamethasone Implant: A Systematic Review With Meta-Analysis. Front. Pharmacol. 2021, 12, 635101. [Google Scholar] [CrossRef]
- Pignatelli, F.; Niro, A.; Fallico, M.; Passidomo, F.; Gigliola, S.; Nacucchi, A.; Bonfiglio, V.; Reibaldi, M.; Addabbo, G.; Avitabile, T. Mid-Term Safety and Effectiveness of Macular Peeling One Month after Intravitreal Dexamethasone Implant for Tractional Diabetic Macular Edema. Sci. Rep. 2023, 13, 5990. [Google Scholar] [CrossRef] [PubMed]
- Zhu, R.; Xiao, S.; Zhang, W.; Li, J.; Yang, M.; Zhang, Y.; Gu, X.; Yang, L. Comparison of Hyperreflective Foci in Macular Edema Secondary to Multiple Etiologies with Spectral-Domain Optical Coherence Tomography: An Observational Study. BMC Ophthalmol. 2022, 22, 352. [Google Scholar] [CrossRef] [PubMed]
- Zur, D.; Iglicki, M.; Busch, C.; Invernizzi, A.; Mariussi, M.; Loewenstein, A.; Busch, C.; Cebeci, Z.; Chhablani, J.K.; Chaikitmongkol, V.; et al. OCT Biomarkers as Functional Outcome Predictors in Diabetic Macular Edema Treated with Dexamethasone Implant. Ophthalmology 2018, 125, 267–275. [Google Scholar] [CrossRef] [PubMed]
- Vujosevic, S.; Torresin, T.; Bini, S.; Convento, E.; Pilotto, E.; Parrozzani, R.; Midena, E. Imaging Retinal Inflammatory Biomarkers after Intravitreal Steroid and Anti—VEGF Treatment in Diabetic Macular Oedema. Acta Ophthalmol. 2017, 95, 464–471. [Google Scholar] [CrossRef]
- Grigsby, J.G.; Cardona, S.M.; Pouw, C.E.; Muniz, A.; Mendiola, A.S.; Tsin, A.T.C.; Allen, D.M.; Cardona, A.E. The Role of Microglia in Diabetic Retinopathy. J. Ophthalmol. 2014, 2014, 1–15. [Google Scholar] [CrossRef]
- Zeng, H. Microglial Activation in Human Diabetic Retinopathy. Arch. Ophthalmol. 2008, 126, 227. [Google Scholar] [CrossRef] [PubMed]
- Kim, K.T.; Kim, D.Y.; Chae, J.B. Association between Hyperreflective Foci on Spectral-Domain Optical Coherence Tomography and Early Recurrence of Diabetic Macular Edema after Intravitreal Dexamethasone Implantation. J. Ophthalmol. 2019, 2019, 1–9. [Google Scholar] [CrossRef]
- Das, R.; Spence, G.; Hogg, R.E.; Stevenson, M.; Chakravarthy, U. Disorganization of Inner Retina and Outer Retinal Morphology in Diabetic Macular Edema. JAMA Ophthalmol. 2018, 136, 202. [Google Scholar] [CrossRef]
- Zur, D.; Iglicki, M.; Sala-Puigdollers, A.; Chhablani, J.; Lupidi, M.; Fraser-Bell, S.; Mendes, T.S.; Chaikitmongkol, V.; Cebeci, Z.; Dollberg, D.; et al. Disorganization of Retinal Inner Layers as a Biomarker in Patients with Diabetic Macular Oedema Treated with Dexamethasone Implant. Acta Ophthalmol. 2020, 98. [Google Scholar] [CrossRef]
- Rajesh, B.; Zarranz-Ventura, J.; Fung, A.T.; Busch, C.; Sahoo, N.K.; Rodriguez-Valdes, P.J.; Sarao, V.; Mishra, S.K.; Saatci, A.O.; Udaondo Mirete, P.; et al. Safety of 6000 Intravitreal Dexamethasone Implants. Br. J. Ophthalmol. 2020, 104, 39–46. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| RRD | SO | ERM | p-Value * | ||
|---|---|---|---|---|---|
| N° (%); patients/eyes | 36 (75) | 10 (20.8) | 2 (4.2) | ||
| Laterality: right/left | 16/20 | 6/4 | 1/1 | 0.29 | |
| Age, year (mean ± SD) | 64.6 ± 4.5 | 63.8 ± 3.6 | 58.5 ± 0.7 | 0.17 | |
| Gender, N° (%) | |||||
| Male | 25 (69.4) | 6 (60) | 1 (50) | ||
| Female | 11 (30.6) | 4 (40) | 1 (50) | ||
| Type 2 Diabetes (controlled with therapy); N° (%) | 3 (8%) | 1 (10%) | 0 (0%) | 0.45 | |
| Time between cataract surgery and PPV; years, mean ± SD (range) | 4.1 ± 2.48 (1–11) | 3 ± 1.5 (2–6) | 2 ± 0.7 (1–2.5) | 0.20 | |
| Macula attached at the time of surgery (RRD group); N° (%) | 31 (86.1%) | - | - | ||
| PVR present: N° (%) | 14 (38.8%) | - | - | ||
| Mild VH associated with RRD; N° (%) | 2 (5.5%) | - | - | ||
| Endotamponade agent used (RRD group) | |||||
| Gas (SF6 24%; C3F8 14%) | 22 (64.7%) | ||||
| Silicone Oil 1000 cst | 10 (29.4%) | ||||
| Densiron | 2 (5.8%) | ||||
| IRC | DRIL | DROL | HRF | SRF | |
|---|---|---|---|---|---|
| RRD n (%) | 20 (41.7) | 7 (14.6) | 8 (16.7) | 7 (14.6) | 7 (14.6) |
| SO n (%) | 10 (20.8) | 4 (8.3) | 2 (4.2) | 2 (4.2) | 4 (8.3) |
| ERM n (%) | 2 (4.2) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 1 (2.1) |
| p | 0.02 | 0.29 | 0.75 | 0.78 | 0.30 |
| RRD | SO | ERM | p | |
|---|---|---|---|---|
| DEX-i at 3 months, n (%) | 10 (20.8) | 5 (10.4) | 1 (2.1) | 0.37 |
| DEX-i at 6 months, n (%) | 3 (6.4) | 2 (4.3) | 0 (0.0) | 0.52 |
| DEX-i at 9 months, n (%) | 11 (22.9) | 5 (10.4) | 0 (0.0) | 0.31 |
| DEX-i at 12 months, n (%) | 4 (8.3) | 0 (0.0) | 0 (0.0) | 0.49 |
| CMT 1 Month | CMT 3 Months | CMT 6 Months | CMT 9 Months | CMT 12 Months | ||
|---|---|---|---|---|---|---|
| CMT 1 month | Spearman’s Rho | — | ||||
| p | — | |||||
| CMT 3 Months | Spearman’s Rho | 0.592 *** | — | |||
| p | <0.001 | — | ||||
| CMT 6 Months | Spearman’s Rho | 0.174 | 0.274 | — | ||
| p | 0.237 | 0.060 | — | |||
| CMT 9 Months | Spearman’s Rho | 0.145 | 0.541 *** | 0.578 *** | — | |
| p | 0.326 | <0.001 | <0.001 | — | ||
| CMT 12 Months | Spearman’s Rho | 0.117 | 0.573 *** | 0.454 ** | 0.662 *** | — |
| p | 0.428 | <0.001 | 0.001 | <0.001 | — | |
| (A) DEX-i at 3 months as dependent variable | ||||
| Parameters | β | SE (β) | p | OR |
| Age | 0.10 | 0.07 | 0.17 | 1.11 |
| Gender (male) | −3.67 × 10−16 | 0.66 | 0.99 | 0.99 |
| Disease | ||||
| SO—RRD | 0.95 | 0.73 | 0.19 | 2.6 |
| ERM—RRD | 0.95 | 1.46 | 0.51 | 2.6 |
| CMT 1 month | 0.01 | 0.003 | 0.005 | 1.01 |
| IRC (No) | 1.69 | 0.83 | 0.04 | 5.44 |
| DRIL (No) | 2.27 | 0.78 | 0.004 | 9.66 |
| HRF (No) | 1.76 | 0.79 | 0.02 | 5.80 |
| DROL (No) | 1.44 | 0.74 | 0.05 | 4.20 |
| SRF (No) | 0.95 | 0.68 | 0.16 | 2.60 |
| (B) DEX-i at 3 months as dependent variable | ||||
| Parameters | β | SE (β) | p | OR |
| Age | 0.09 | 0.1 0 | 0.35 | 1.1 0 |
| Gender (male) | −0.18 | 0.87 | 0.83 | 0.83 |
| Disease | ||||
| SO—RRD | 0.49 | 0.98 | 0.61 | 1.64 |
| ERM—RRD | 0.77 | 2.44 | 0.75 | 2.17 |
| CMT 1 month | 0.008 | 0.005 | 0.09 | 1 .0 |
| IRC (No) | −0.33 | 1.26 | 0.78 | 0.71 |
| DRIL (No) | 1.62 | 0.92 | 0.08 | 5.08 |
| HRF (No) | 1.33 | 1.03 | 0.19 | 3.8 0 |
| (A) DEX-i at 6 months as dependent variable | ||||
| Parameters | β | SE (β) | p | OR |
| Age | 0.04 | 0.1 0 | 0.69 | 1.03 |
| Gender (male) | 0.39 | 0.97 | 0.68 | 1.5 |
| Disease | ||||
| SO—RRD | 0.98 | 0.99 | 0.32 | 2.66 |
| ERM—RRD | −15.2 | 2797.4 | 0.99 | 2.51 × 10−7 |
| IRC (No) | −0.28 | 0.96 | 0.76 | 0.75 |
| DRIL (No) | −17.7 | 3242.4 | 0.99 | 2.04 × 10−8 |
| HRF (No) | 1.23 | 1 .00 | 0.21 | 3.42 |
| DROL (No) | 0.06 | 1.18 | 0.96 | 1.06 |
| SRF (No) | −0.22 | 1.17 | 0.84 | 0.8 0 |
| (A) DEX-i at 9 months as dependent variable | ||||
| Parameters | β | SE (β) | p | OR |
| Age | 0.02 | 0.07 | 0.74 | 1.02 |
| Gender (male) | 0.42 | 0.64 | 0.51 | 1.5 |
| Disease | ||||
| SO—RRD | 0.87 | 0.73 | 0.23 | 2.27 |
| ERM—RRD | −15.7 | 1696.7 | 0.99 | 1.45 × 10−7 |
| CMT 3 months | 0.006 | 0.003 | 0.07 | 1 .00 |
| CMT 6 months | 0.007 | 0.004 | 0.11 | 1 .00 |
| IRC (No) | 0.14 | 0.65 | 0.82 | 1.15 |
| DRIL (No) | 0.67 | 0.7 0 | 0.33 | 1.97 |
| HRF (No) | 1.76 | 0.79 | 0.02 | 5.8 0 |
| DROL (No) | 2.02 | 0.78 | 0.01 | 7.51 |
| SRF (No) | 0.95 | 0.68 | 0.16 | 2.6 0 |
| (B) DEX-i at 9 months as dependent variable | ||||
| Parameters | β | SE (β) | p | OR |
| Age | −0.02 | 0.09 | 0.85 | 0.97 |
| Gender (male) | 0.01 | 0.83 | 0.99 | 1.01 |
| Disease | ||||
| SO—RRD | 1.01 | 0.84 | 0.22 | 2.75 |
| ERM—RRD | −14.9 | 1696.7 | 0.99 | 3.23 × 10−7 |
| HRF (No) | 1.71 | 0.9 0 | 0.04 | 5.53 |
| DROL (No) | 1.96 | 0.87 | 0.02 | 7.11 |
| (A) DEX-i at 12 months as dependent variable | ||||
| Parameters | β | SE (β) | p | OR |
| Age | −0.20 | 0.15 | 0.18 | 0.81 |
| Gender (male) | −0.33 | 1.19 | 0.77 | 0.71 |
| Disease | ||||
| SO—RRD | −17.5 | 3400.7 | 0.99 | 2.39 × 10−8 |
| ERM—RRD | −17.5 | 7604.2 | 0.99 | 2.39 × 10−8 |
| CMT 3 months | −0.01 | 0.01 | 0.21 | 0.98 |
| CMT 6 months | 0.007 | 0.004 | 0.1 0 | 1 .00 |
| CMT 9 months | 0.005 | 0.004 | 0.2 0 | 1 .00 |
| IRC (No) | −1.97 | 1.2 0 | 0.1 0 | 0.14 |
| DRIL (No) | −17.4 | 3242.4 | 0.99 | 2.62 × 10−8 |
| HRF (No) | −17.4 | 3584.6 | 0.99 | 2.78 × 10−8 |
| DROL (No) | 0.26 | 1.21 | 0.83 | 1.29 |
| SRF (No) | −17.4 | 3104.4 | 0.99 | 2.54 × 10−8 |
| Intraocular Pressure (IOP, mmHg) at Different Time Points | mmHg | p |
|---|---|---|
| IOP Baseline * | 15.6 ± 3.9 | |
| IOP 1 Month | 15.6 ± 2.8 | 0.90 † |
| IOP 3 Months | 15.0 ± 2.4 | 0.32 |
| IOP 6 Months | 15.9 ± 3.1 | 0.31 |
| IOP 9 Months | 15.8 ± 2.1 | 0.71 |
| IOP 12 Months | 15.6 ± 1.9 | 0.80 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pignatelli, F.; Niro, A.; Addabbo, G.; Viggiano, P.; Boscia, G.; Grassi, M.O.; Boscia, F.; Iaculli, C.; Clima, G.M.E.; Barone, A.; et al. Twelve-Month Outcomes and Optical Coherence Tomography (OCT) Biomarkers After Intravitreal Dexamethasone Implantation in Pseudophakic Eyes with Post-Vitrectomy Cystoid Macular Edema (CME)—Refractory to Medical Therapy. Diagnostics 2025, 15, 147. https://doi.org/10.3390/diagnostics15020147
Pignatelli F, Niro A, Addabbo G, Viggiano P, Boscia G, Grassi MO, Boscia F, Iaculli C, Clima GME, Barone A, et al. Twelve-Month Outcomes and Optical Coherence Tomography (OCT) Biomarkers After Intravitreal Dexamethasone Implantation in Pseudophakic Eyes with Post-Vitrectomy Cystoid Macular Edema (CME)—Refractory to Medical Therapy. Diagnostics. 2025; 15(2):147. https://doi.org/10.3390/diagnostics15020147
Chicago/Turabian StylePignatelli, Francesco, Alfredo Niro, Giuseppe Addabbo, Pasquale Viggiano, Giacomo Boscia, Maria Oliva Grassi, Francesco Boscia, Cristiana Iaculli, Giulia Maria Emilia Clima, Antonio Barone, and et al. 2025. "Twelve-Month Outcomes and Optical Coherence Tomography (OCT) Biomarkers After Intravitreal Dexamethasone Implantation in Pseudophakic Eyes with Post-Vitrectomy Cystoid Macular Edema (CME)—Refractory to Medical Therapy" Diagnostics 15, no. 2: 147. https://doi.org/10.3390/diagnostics15020147
APA StylePignatelli, F., Niro, A., Addabbo, G., Viggiano, P., Boscia, G., Grassi, M. O., Boscia, F., Iaculli, C., Clima, G. M. E., Barone, A., & Giancipoli, E. (2025). Twelve-Month Outcomes and Optical Coherence Tomography (OCT) Biomarkers After Intravitreal Dexamethasone Implantation in Pseudophakic Eyes with Post-Vitrectomy Cystoid Macular Edema (CME)—Refractory to Medical Therapy. Diagnostics, 15(2), 147. https://doi.org/10.3390/diagnostics15020147