

Role of CT Coronary Angiography at Initial Presentation in Kawasaki Disease—Insights from a Tertiary Care Center in North India

 ,
,  , , , , , , and
, , , , , , and
Abstract
1. Introduction
2. Methodology
3. Results
- (a)
- Patient characteristics:
- (b)
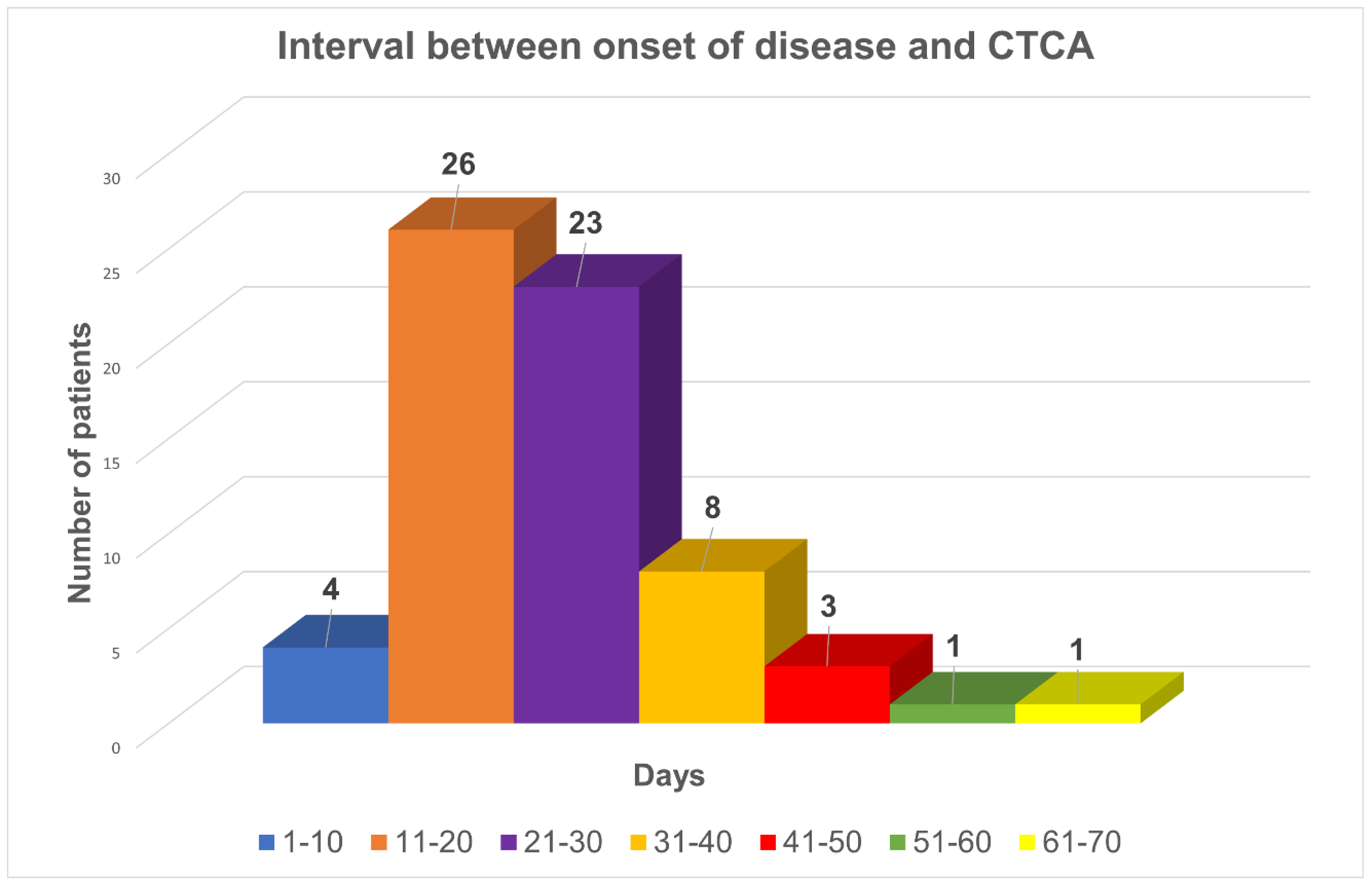
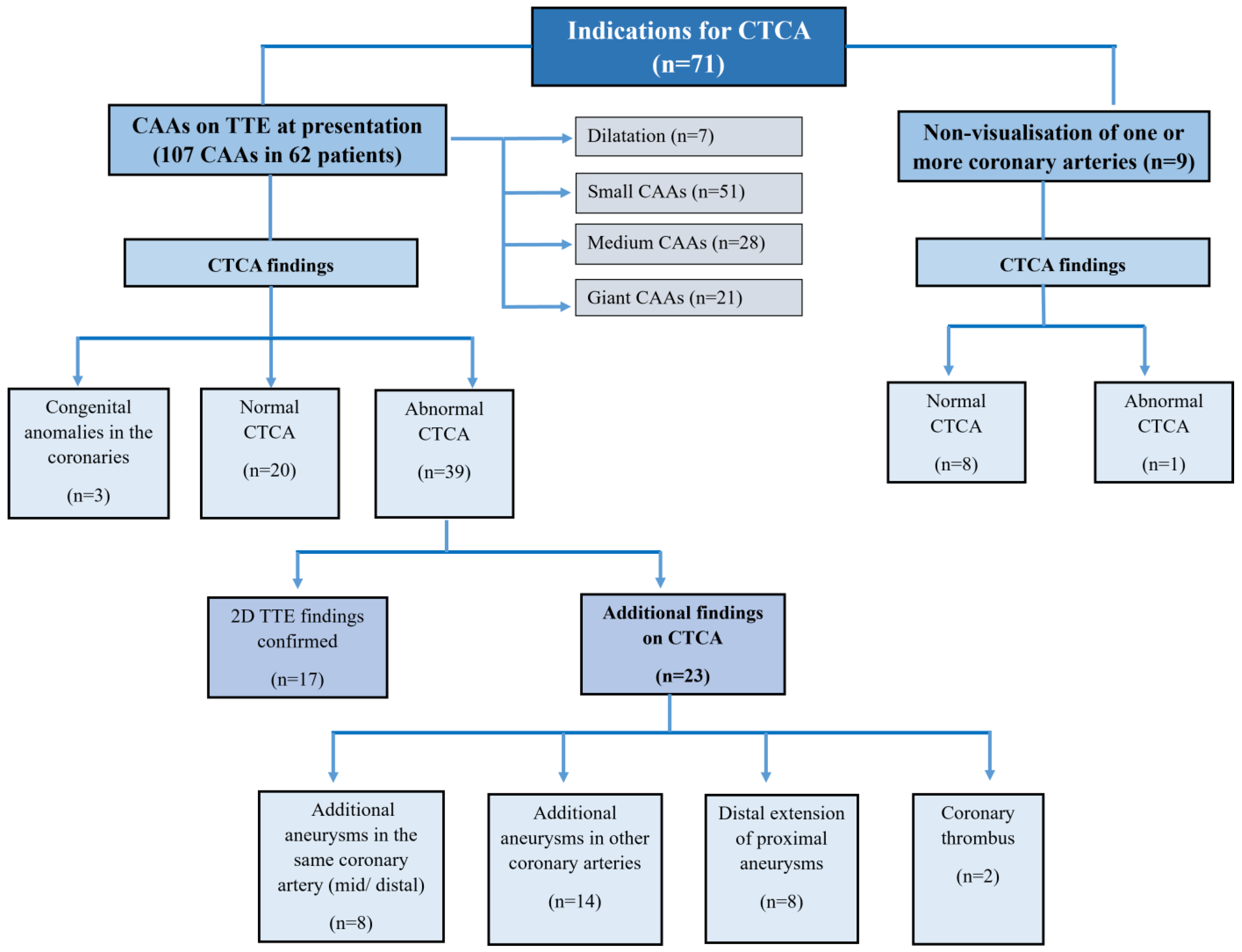
- Indications of CTCA:
- (c)
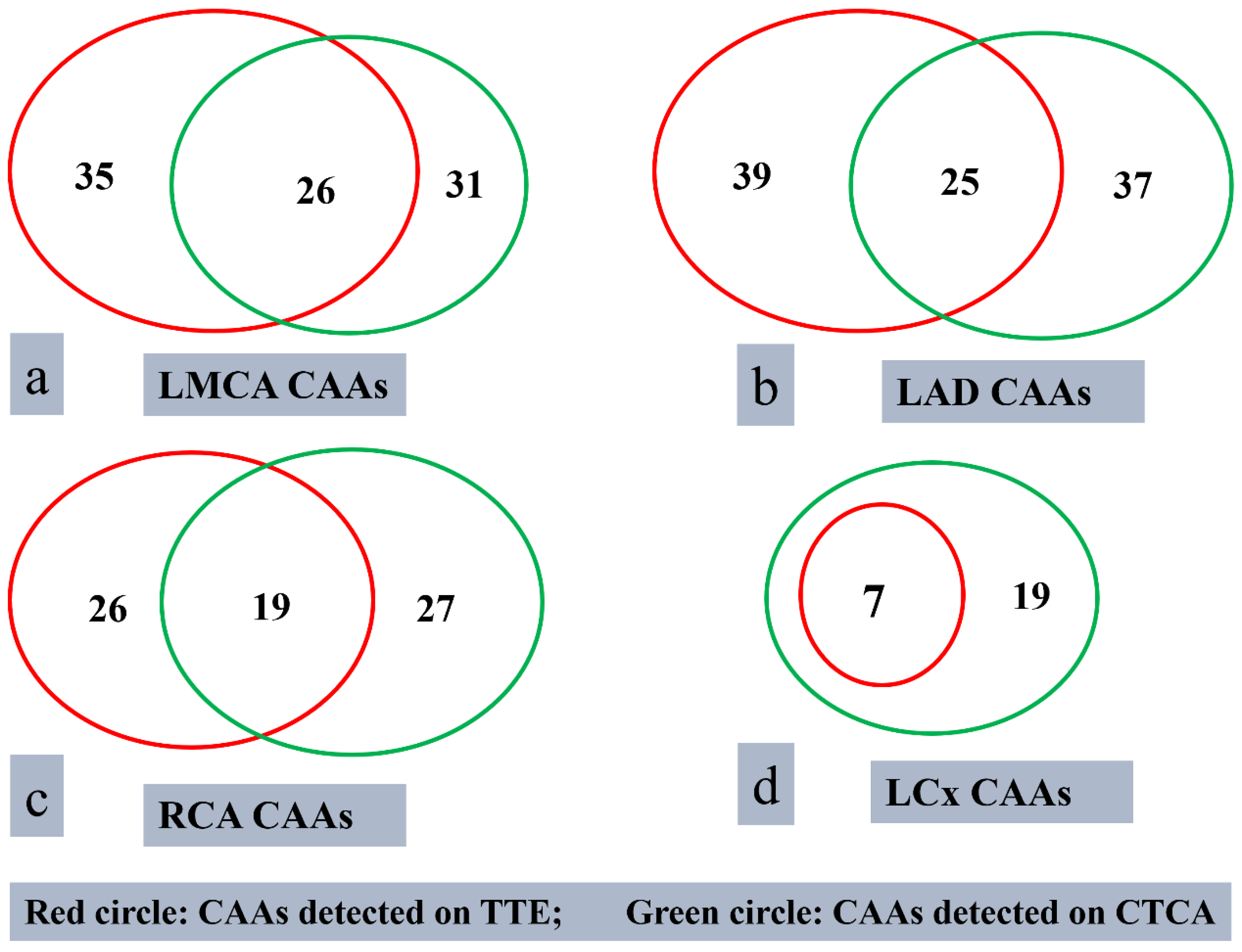
- Findings on TTE and CTCA
- Imaging by TTE:
- ii.
- Imaging by CTCA:
- iii.
- CAAs detected, or confirmed, on CTCA
- iv.
- Patients with congenital coronary artery anomalies on CTCA
- v.
- Patients with no CAAs on CTCA
- (d)
- Impact of CTCA on management:
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Pilania, R.K.; Tremoulet, A.H.; Prinja, S.; Dahdah, N.; Singh, S. Kawasaki disease: The most common cause of acquired heart disease among children globally. Cardiol. Young 2025, 35, 441–443. [Google Scholar] [CrossRef] [PubMed]
- Jone, P.N.; Tremoulet, A.; Choueiter, N.; Dominguez, S.R.; Harahsheh, A.S.; Mitani, Y.; Zimmerman, M.; Lin, M.-T.; Friedman, K.G. Update on Diagnosis and Management of Kawasaki Disease: A Scientific Statement From the American Heart Association. Circulation 2024, 150, e481–e500. [Google Scholar] [CrossRef] [PubMed]
- McCrindle, B.W.; Rowley, A.H.; Newburger, J.W.; Burns, J.C.; Bolger, A.F.; Gewitz, M.; Baker, A.L.; Jackson, M.A.; Takahashi, M.; Shah, P.B.; et al. Diagnosis, Treatment, and Long-Term Management of Kawasaki Disease: A Scientific Statement for Health Professionals From the American Heart Association. Circulation 2017, 135, e927–e999. [Google Scholar] [CrossRef] [PubMed]
- Pilania, R.K.; Jindal, A.K.; Bhattarai, D.; Naganur, S.H.; Singh, S. Cardiovascular Involvement in Kawasaki Disease Is Much More Than Mere Coronary Arteritis. Front. Pediatr. 2020, 8, 526969. [Google Scholar] [CrossRef] [PubMed]
- Pilania, R.K.; Basu, S.; Dixit, J.; Kumrah, R.; Jindal, A.K.; Thangaraj, A.; Nimesh, R.; Kaur, T.; Vignesh, P.; Suri, D.; et al. Incidence of Kawasaki disease among children in Chandigarh, India during 2015–2019: A trend analysis. Lancet Reg. Health—Southeast Asia 2024, 29, 100474. Available online: https://www.thelancet.com/journals/lansea/article/PIIS2772-3682(24)00124-0/fulltext (accessed on 12 September 2024). [CrossRef] [PubMed]
- Tsuda, E.; Singhal, M. Role of imaging studies in Kawasaki disease. Int. J. Rheum. Dis. 2018, 21, 56–63. [Google Scholar] [CrossRef] [PubMed]
- Singhal, M.; Singh, S.; Gupta, P.; Sharma, A.; Khandelwal, N.; Burns, J.C. Computed Tomography Coronary Angiography for Evaluation of Children With Kawasaki Disease. Curr. Probl. Diagn. Radiol. 2018, 47, 238–244. [Google Scholar] [CrossRef] [PubMed]
- Pilania, R.K.; Basu, S.; Singh, S.; Sabui, T.; Singhal, M. Computed tomography coronary angiography for imaging in children with Kawasaki disease: An update. Int. J. Rheum. Dis. 2024, 27, e15331. [Google Scholar] [CrossRef] [PubMed]
- Singhal, M.; Pilania, R.K.; Basu, S.; Sharma, A.; Singh, S. CT coronary angiography in Kawasaki disease: Current perspectives. Arch. Dis. Childhood 2025, 110, 499–500. Available online: https://adc.bmj.com/content/early/2025/03/27/archdischild-2024-327190 (accessed on 18 April 2025). [CrossRef] [PubMed]
- Newburger, J.W.; Takahashi, M.; Gerber, M.A.; Gewitz, M.H.; Tani, L.Y.; Burns, J.C.; Shulman, S.T.; Bolger, A.F.; Ferrieri, P.; Baltimore, R.S.; et al. Diagnosis, Treatment, and Long-Term Management of Kawasaki Disease. Circulation 2004, 110, 2747–2771. [Google Scholar] [CrossRef] [PubMed]
- Dallaire, F.; Dahdah, N. New equations and a critical appraisal of coronary artery Z scores in healthy children. J. Am. Soc. Echocardiogr. 2011, 24, 60–74. [Google Scholar] [CrossRef] [PubMed]
- Pilania, R.K.; Nadig, P.L.; Basu, S.; Tyagi, R.; Thangaraj, A.; Aggarwal, R.; Arora, M.; Sharma, A.; Singh, S.; Singhal, M. Congenital anomalies of coronary artery misdiagnosed as coronary dilatations in Kawasaki disease: A clinical predicament. World J. Clin. Pediatr. 2025, 14, 99177. [Google Scholar] [CrossRef] [PubMed]
- Thangathurai, J.; Kalashnikova, M.; Takahashi, M.; Shinbane, J.S. Coronary Artery Aneurysm in Kawasaki Disease: Coronary CT Angiography through the Lens of Pathophysiology and Differential Diagnosis. Radiol. Cardiothorac. Imaging 2021, 3, e200550. [Google Scholar] [CrossRef] [PubMed]
- Singhal, M.; Pilania, R.K.; Jindal, A.K.; Gupta, A.; Sharma, A.; Guleria, S.; Johnson, N.; Maralakunte, M.; Vignesh, P.; Suri, D.; et al. Distal coronary artery abnormalities in Kawasaki disease: Experience on CT coronary angiography in 176 children. Rheumatology 2023, 62, 815–823. [Google Scholar] [CrossRef] [PubMed]
- Borhanuddin, B.K.; Abdul Latiff, H.; Mohamed Yusof, A.K. CT coronary angiogram in children with Kawasaki disease: Experience in 52 patients. Cardiol. Young 2022, 32, 1994–1998. [Google Scholar] [CrossRef] [PubMed]
- Barman, P.; Pilania, R.K.; Cv, G.; Thangaraj, A.; Arora, M.; Singh, S. Treatment intensification in Kawasaki disease—Current perspectives. Expert. Rev. Clin. Immunol. 2024, 20, 1179–1191. [Google Scholar] [CrossRef] [PubMed]
- Singhal, M.; Pilania, R.K.; Thangaraj, A.; Chaudhary, H.; Gummadi, A.; Soundararajan, R.; Loganathan, S.; Sharma, A.; Gupta, A.; Bhattad, S.; et al. The value of CT coronary angiography for a comprehensive assessment of left circumflex artery in Kawasaki disease: 9 years of experience from a tertiary center. Lancet Reg. Health—Southeast Asia 2024, 29, 100471. [Google Scholar] [CrossRef] [PubMed]
- Carbone, I.; Cannata, D.; Algeri, E.; Galea, N.; Napoli, A.; De Zorzi, A.; Bosco, G.; D’Agostino, R.; Menezes, L.; Catalano, C.; et al. Adolescent Kawasaki disease: Usefulness of 64-slice CT coronary angiography for follow-up investigation. Pediatr. Radiol. 2011, 41, 1165–1173. [Google Scholar] [CrossRef] [PubMed]
- Chakraborty, R.; Singhal, M.; Pandiarajan, V.; Sharma, A.; Pilania, R.K.; Singh, S. Coronary arterial abnormalities detected in children over 10 years following initial Kawasaki disease using cardiac computed tomography. Cardiol. Young 2021, 31, 998–1002. [Google Scholar] [CrossRef] [PubMed]
- Dietz SM: Tacke, C.E.; Kuipers, I.M.; Wiegman, A.; de Winter, R.J.; Burns, J.C.; Gordon, J.B.; Groenink, M.; Kuijpers, T.W. Cardiovascular imaging in children and adults following Kawasaki disease. Insights Imaging 2015, 6, 697–705. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | N = 71 |
|---|---|
| Demographics | |
| Age at presentation (median, range) | 39 months (2–360) |
| Male sex | 50 (70.4%) |
| Clinical characteristics | |
| Duration of fever (median, range) | 11 days (3–60) |
| Delay in diagnosis (median, range) | 15 days (4–60) |
| Interval between onset of disease and CTCA (median, range) | 23 days (9–85) |
| Fever | 71 (100%) |
| Rash | 57 (80.3%) |
| Mucosal changes | 57 (80.3%) |
| Extremity changes | 27 (38%) |
| Eye changes | 39 (54.9%) |
| Cervical lymphadenopathy | 21 (29.6%) |
| Complete KD | 49 (69%) |
| Peeling | 9 (12.7%) |
| Beau’s lines | 13 (18.3%) |
| Laboratory features | |
| Hemoglobin, g/L (median, range) | 92.5 (58–138) |
| Total leukocyte count, cells/mm3 (median, range) | 16,015 (3220–53,020) |
| Neutrophil, % (median, range) | 57% (13–98) |
| Platelet count, cells/mm3 (median, range) | 694,000 (230,000–1,635,000) |
| AST, U/L (median, range) | 41.0 (12–1236) |
| ALT, U/L (median, range) | 30.5 (6–428) |
| Albumin, g/dL (median, range) | 3.15 (1.2–6.4) |
| Serum sodium, mmol/L (median, range) | 134.0 (123–140) |
| ESR, mm in 1st hr (median, range) | 42.0 (2–115) |
| CRP, mg/L (median, range) | 44.5 (0.1–279) |
| Treatment | |
| Standard of care | |
| IVIg | 71 (100%) |
| Aspirin | 71 (100%) |
| Treatment intensification | |
| Infliximab | 46 (64.8%) |
| Steroids | 31 (43.7%) |
| Repeat IVIg | 7 (9.9%) |
| Cyclosporine | 21 (29.6%) |
| Anti-coagulation | |
| LMWH | 28 (39.4%) |
| Warfarin | 4 (5.6%) |
| S.no. | Age (Months)/Sex | TTE Findings (Measurement in mm/Z-Score) | Interval Between Diagnosis and CTCA (Days) | CTCA Findings | Detailed Description of Findings on CTCA | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| LMCA | LAD | RCA | LCx | LMCA (mm) | LAD (mm) | RCA (mm) | LCx (mm) | ||||
| 1 | 8/M | 4.8 (8.36) | 7 (26.24) | 8.3 (23.52) | NV | 15 | 8 | 7 | 6.4 | Fusiform and saccular aneurysms in proximal and distal RCA, respectively. Saccular aneurysm involving distal LCA, incorporating/involving the origin of proximal LAD and LCX. No e/o thrombosis | |
| 2 | 55/F | 2.9 (1.8) | 2.5 (2.2) | 2.6 (1.7) | NV | 18 | Normal | 2.4 | Normal | Normal | Segmental areas of dilatations in the proximal and mid LAD |
| 3 | 7/M | 5 (10.3) | 4.7 (11.3) | 4.2 (8.50) | 1.7 (1.7) | 19 | 7.9 | 3.5 | 4.6 | 3.2 | Fusiform aneurysm involving all the coronary arteries; entire course of RCA with extension into PDA; LMCA, proximal and mid LAD, and proximal LCX with involvement of OM1 branch |
| 4 | 39/M | 3.3 (2.9) | 5.1 (10.5) | 0.8 (−2.83) | 0.8 (−2.11) | 16 | 5.2 | 5.4 | 3 | Saccular aneurysm in mid LAD; areas of dilatations in RCA, LCA, proximal LAD | |
| 5 | 20/M | 2.4 (2.03) | 2.9 (4.98) | 1.5 (−0.49) | 1.2 (−0.12) | 12 | 2.7 | 2.7 | 1.9 | 1.5 | Dilated distal LCA and proximal LAD |
| 6 | 64/M | 3.1 (1.6) | 1.7 −0.5 | 1.4 (−1.80) | 1 (−1.98) | 24 | 2.6 | 1.8 | 1.4 | 1.5 | Dilated mild LAD |
| 7 | 156/M | 6.17 (7.42) | 4.68 (6) | 7.5 (10.63) | NV | 41 | 6.3 | 5 | 6.6 | 4.6 | Fusiform aneurysms in all coronaries: LMCA, proximal and mid RCA, LAD, and LCX. |
| 8 | 132/M | 2.89 (−0.37) | 3.9 (3.62) | 2.14 (−1.26) | NV | 38 | 3.8 | 2.7 | 1.8 | 2.7 | Dilated all coronary arteries: Diffuse LMCA and LAD; proximal and mid segments of RCA and proximal LCX |
| 9 | 42/M | 3.1 (3.85) | 2.7 (2.5) | 3.85 (6.43) | NV | 14 | 3 | 3.2 | 4.4 | 2.7 | Fusiform aneurysms in all coronaries: LMCA, entire RCA, including PDA and PLV branches, and proximal LAD and LCX. |
| 10 | 43/M | 5.2 (7.6) | 3.2 (4.1) | 3.2 (3.00) | NV | 10 | 7 | 3.5 | 2.4 | 2.4 | Fusiform aneurysm in LMCA with extension into origins of LAD and LCX. Dilated the entire RCA and LCX. |
| 11 | 14/F | 5.2 (9.93) | 3.6 (4.03) | 3.3 (2.76) | 1.6 (2.76) | 26 | 6.4 | 3.6 | 1 | 2 | LMCA saccular aneurysm, which is extending into the proximal LAD and proximal LCX |
| 12 | 2/F | 2.6 (4.41) | 3.1 (7.53) | 2.8 (5.75) | NV | 24 | 2.4 | 3.8 | 2.7 | 2.5 | Fusiform aneurysm of LMCA with extension into osteo-proximal segments of LAD and LCX; another non-contiguous aneurysm was seen in mid-LAD LAD |
| 13 | 204/M | 3.2 (−0.33) | 2.96 (0.84) | 2.7 (−0.62) | NV | 28 | 3.2 | 3.1 | 2.3 | Normal | Dilated LMCA and proximal LAD |
| 14 | 7/M | 2.97 (5.33) | 3.2 (5.91) | 4.9 (6.88) | NV | 19 | 2.7 | 4.2 | 5.8 | 3.3 | Fusiform aneurysms in RCA (2 in number). Fusiform aneurysms in LCx (2 in number) |
| 15 | 76/M | 3 (1.13) | 6.68 (12.33) | 6.5 (9.89) | 2 (0.22) | 58 | 1.8 | 6.4 | 5.1 | 12.6 × 4.1 |
|
| 16 | 44/M | 4.5 (6.4) | 4.2 (7.35) | 4.2 (6.06) | 2.3 (1.97) | 33 | Normal | 5 | 8.2 | 4 | Fusiform aneurysm in proximal RCA (8.2 mm W ∗ 31 mm L giant aneurysm), LAD (5 mm W ∗ 25 mm L), LCx (4 mm W ∗ 25 mm L). No e/o thrombus |
| 17 | 132/M | 4.2 (3.15) | 3.6 (3.5) | 2 (−1.13) | 1.5 (−1.36) | 32 | 5.8 | 9.1 | 12.6 | 6.1 | Multiple aneurysms in the entire course of RCA, with a giant aneurysm in its proximal segment; fusiform giant aneurysm in proximal LAD; fusiform aneurysm in proximal LCx; and a dilated LMCA |
| 18 | 60/M | 3.5 (2.23) | 6.8 (16.05) | 5.7 (10.04) | NV | 26 | 3.6 | 7.7 | 6 | 3.1 | LMCA normal; proximal LAD: fusiform aneurysm (7.7 mm W ∗ 50 mm L), with involvement of diagonal branch (3.6 mm), mid-segment: skip areas of dilatation. Distal segment: dilated (3.6 mm). RCA proximal segment dilated (6.6 mm for a length of 40 mm). AM branch: multiple skip aneurysms. LCx: proximal segment fusiform aneurysm (3.6 mm) with extension into OM branch (3.9 mm) |
| 19 | 7/F | 2.1 (2.06) | 1.8 (0.65) | 1.8 (3.30) | 1.5 (0.16) | 27 | 2.3 | 1.6 | 2.2 | 1.5 | Dilated proximal and distal LAD with normal intervening segment |
| 20 | 27/M | 3.2 (2.95) | 3.5 (5.42) | 2.6 (1.98) | 13 | 3.5 | 5.1 | 3.6 | Fusiform aneurysm of LMCA extending to proximal LAD and LCx. No e/o thrombus | ||
| 21 | 6/M | 3.1 (4.6) | 6.7 (16.82) | 9.4 (24.00) | NV | 35 | 3.8 | 6.6 | 8 | 4.1 | Fusiform aneurysmal dilatation of all coronary arteries, no thrombus |
| 22 | 96/M | 4.85 (0.63) | 8 (34) | 7.5 (14.3) | NV | 85 | 4.5 | 13 | 5.1 | 10 | Fusiform aneurysm LMCA with extension into osteo-proximal segments of LAD and LCX and involving septal and diagonal branches of LAD and obtuse marginal branch of LCX; fusiform aneurysm in the entire course of RCA with an eccentric thrombus in mid RCA |
| 23 | 7/M | 2.47 (3.46) | 14.9 (47.2) | 4.17 (9.50) | 4.39 (11.48) | 51 | 2 | 18.3 | 3.5 | 7.2 | Giant aneurysm in proximal LAD with partial thrombus (detected on TTE), proximal RCA saccular aneurysm with thrombus (not detected on TTE), LCx fusiform aneurysm (not detected on TTE) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Singhal, M.; Pilania, R.K.; Basu, S.; Desai, D.; Thangaraj, A.; Singh, R.; Semwal, R.; Kaur, T.; Sri, G.; Sudhakar, M.; et al. Role of CT Coronary Angiography at Initial Presentation in Kawasaki Disease—Insights from a Tertiary Care Center in North India. Diagnostics 2025, 15, 1806. https://doi.org/10.3390/diagnostics15141806
Singhal M, Pilania RK, Basu S, Desai D, Thangaraj A, Singh R, Semwal R, Kaur T, Sri G, Sudhakar M, et al. Role of CT Coronary Angiography at Initial Presentation in Kawasaki Disease—Insights from a Tertiary Care Center in North India. Diagnostics. 2025; 15(14):1806. https://doi.org/10.3390/diagnostics15141806
Chicago/Turabian StyleSinghal, Manphool, Rakesh Kumar Pilania, Suprit Basu, Dev Desai, Abarna Thangaraj, Ripudaman Singh, Radhika Semwal, Taranpreet Kaur, Gopika Sri, Murugan Sudhakar, and et al. 2025. "Role of CT Coronary Angiography at Initial Presentation in Kawasaki Disease—Insights from a Tertiary Care Center in North India" Diagnostics 15, no. 14: 1806. https://doi.org/10.3390/diagnostics15141806
APA StyleSinghal, M., Pilania, R. K., Basu, S., Desai, D., Thangaraj, A., Singh, R., Semwal, R., Kaur, T., Sri, G., Sudhakar, M., Sharma, A., Vignesh, P., Suri, D., & Singh, S. (2025). Role of CT Coronary Angiography at Initial Presentation in Kawasaki Disease—Insights from a Tertiary Care Center in North India. Diagnostics, 15(14), 1806. https://doi.org/10.3390/diagnostics15141806