
Twelve-Month Follow-Up After the Treatment of Periodontal Conditions Using Scaling and Root Planning Alone vs. Laser-Assisted New Attachment Procedure
 , , and
, , and
Abstract
1. Introduction
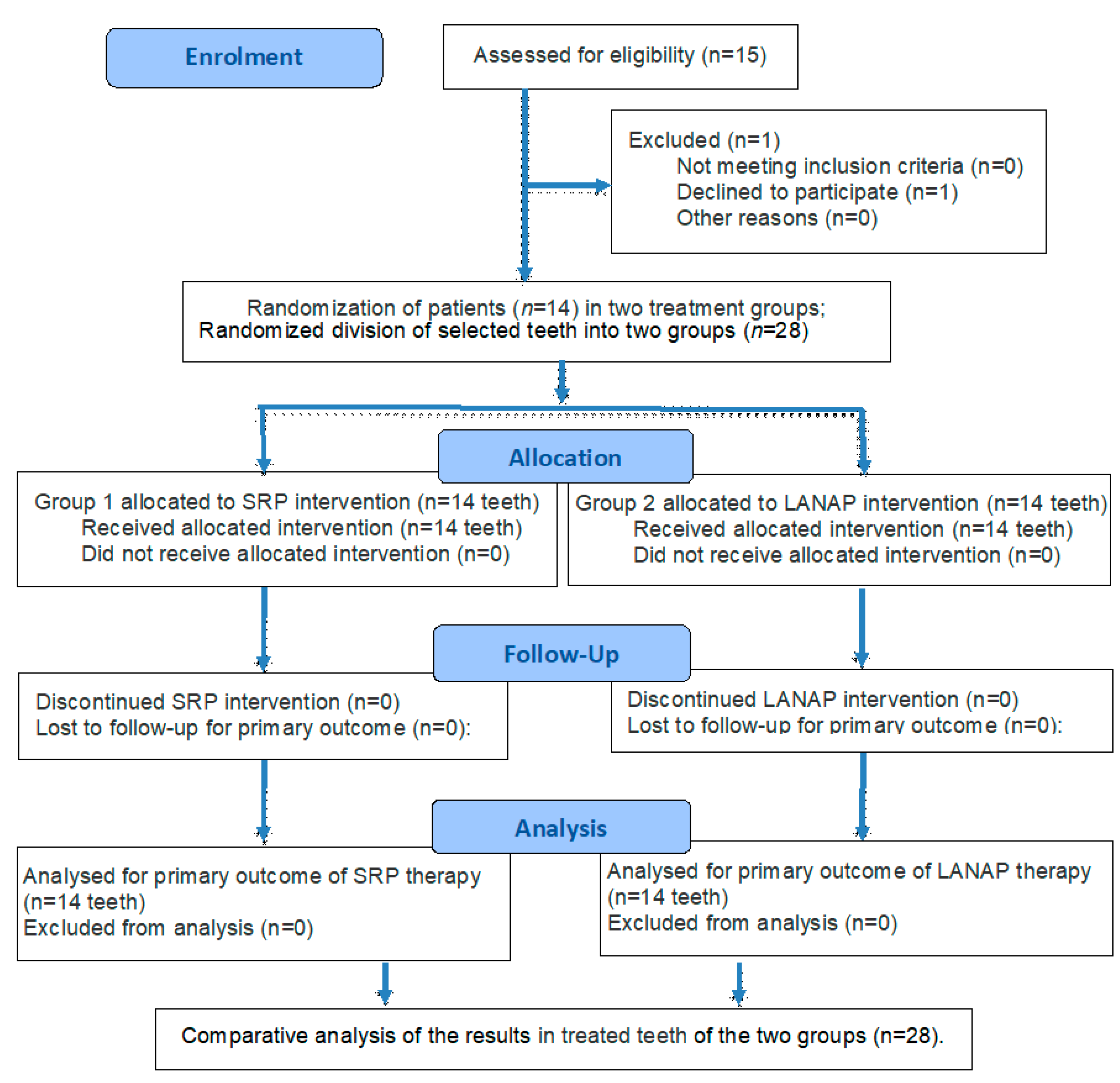
2. Materials and Methods
2.1. Ethical Approval
2.2. Participants
2.3. Inclusion and Exclusion Criteria
2.4. Clinical Procedure
2.5. Statistical Analysis
3. Results
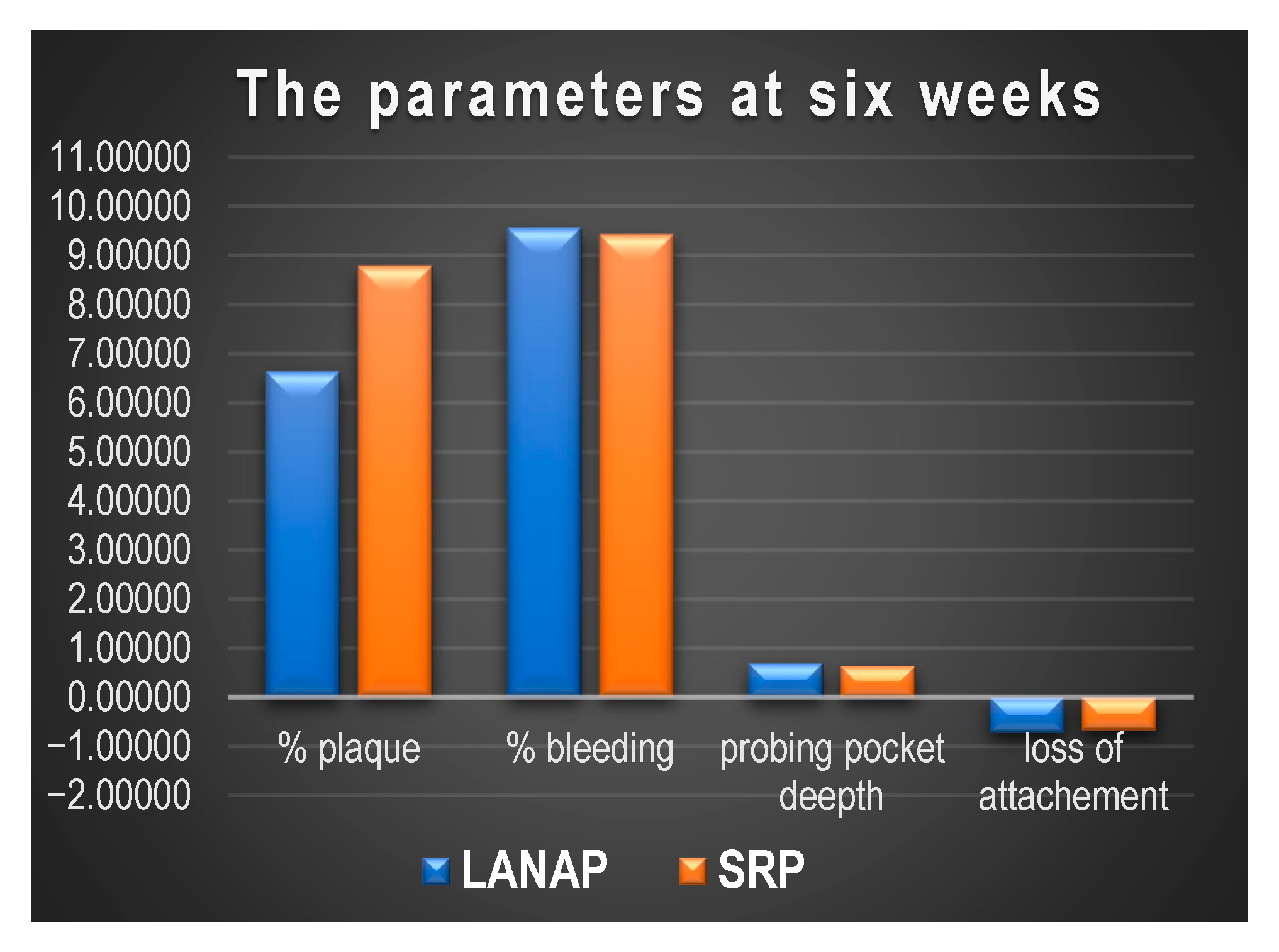
- % plaque index:
- -
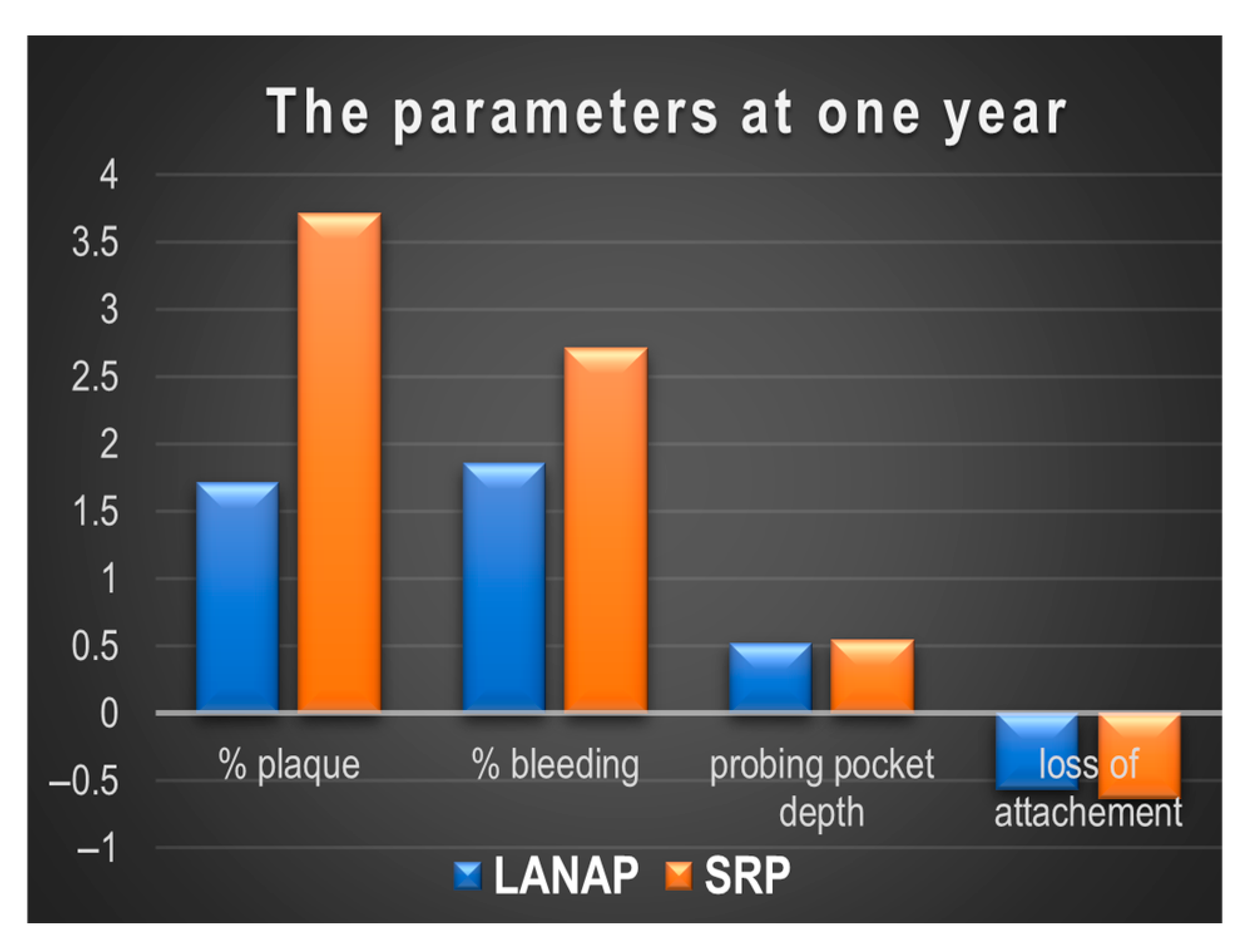
- SRP: The plaque percentage increases significantly from 1.00% at six weeks to 3.71% at one year (p = 0.026). This shows a noticeable increase in plaque accumulation over the 12 months, though it does not return to the original levels before treatment.
- -
- LANAP: The plaque index increases from 0.93% at six weeks to 1.71% at one year. However, this change is not statistically significant (p = 0.102), indicating that there is a slight rise in plaque accumulation over the year, but not a substantial one.
- % bleeding on probing:
- -
- SRP: The percentage of bleeding on probing increases from 1.29% at six weeks to 2.71% at one year (p = 0.05), which is statistically significant. This suggests that the bleeding on probing is still slightly higher at one year, though it is still much lower than before treatment.
- -
- LANAP: The percentage of bleeding on probing increases from 1.29% at six weeks to 1.86% at one year. This change is not statistically significant (p = 0.071), indicating a small rise in bleeding on probing, but it remains relatively low compared to baseline.
- Periodontal probing depth (PPD):
- -
- SRP: The score increases from 0.46 at six weeks to 0.54 at one year (p = 0.006), which is statistically significant.
- -
- LANAP: The score increases from 0.49 at six weeks to 0.52 at one year. This change is not significant (p = 0.165).
- Attachment Loss:
- -
- SRP: Attachment loss worsens slightly from −0.54 mm at six weeks to −0.64 mm at one year (p = 0.016). This change is statistically significant, indicating a slight loss of attachment over the 12-month period after SRP treatment.
- -
- LANAP: Attachment loss remains relatively stable, with a minor improvement from −0.52 mm at six weeks to −0.56 mm at one year. The change is not significant (p = 0.054), indicating that the positive effects on attachment loss from LANAP are maintained over the year.
- % plaque index:
- -
- SRP: The plaque percentage significantly decreases at six weeks (from 8.79% to 1.00%) but increases significantly at one year (3.71%) compared to six weeks (p = 0.026). This suggests a return of plaque to a higher level at one year, though it does not reach the initial values.
- -
- LANAP: Similarly, after a significant reduction in plaque at six weeks (from 6.64% to 0.93%), the plaque percentage slightly increases at one year (1.71%), but this increase is not statistically significant (p = 0.102).
- % bleeding on probing:
- -
- SRP: Bleeding decreases significantly at six weeks (from 9.43% to 1.29%) and increases slightly at one year (2.71%), with a significant difference (p = 0.0498), indicating a return to a higher bleeding level compared to six weeks.
- -
- LANAP: Similarly, bleeding on probing significantly decreases after treatment at six weeks (from 9.57% to 1.29%) and remains slightly elevated at one year (1.86%), but the difference is not statistically significant (p = 0.071).
- Periodontal pocket depth (PPD):
- -
- SRP: PPD decreases significantly at six weeks (from 0.63 to 0.46), but increases at one year (0.54), with a significant change compared to six weeks (p = 0.006), suggesting an increase in medication use at one year.
- -
- LANAP: PPD significantly decreases at six weeks (from 0.69 to 0.49) but remains almost constant at one year (0.52), with no significant change between six weeks and one year (p = 0.165).
- Attachment Loss:
- -
- SRP: Attachment loss improves significantly at six weeks (from −0.67 mm to −0.54 mm) but improves less at one year (from −0.54 mm to −0.64 mm), with a significant change between six weeks and one year (p = 0.016), suggesting a slight loss of attachment at one year compared to six weeks.
- -
- LANAP: Attachment loss improves significantly at six weeks (from −0.72 mm to −0.52 mm), and this improvement remains almost constant at one year (from −0.52 mm to −0.56 mm), with no significant change (p = 0.054).
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| SRP | Scaling and root planing |
| LANAP | Laser-assisted new attachment procedure |
| Nd:YAG laser | Neodymium-doped yttrium aluminum garnet laser |
| CAL PPD | Clinical attachment loss Periodontal probing depth |
| OPG | Orthopantomogram |
References
- Bhuyan, R.; Bhuyan, S.K.; Mohanty, J.N.; Das, S.; Juliana, N.; Juliana, I.F. Periodontitis and Its Inflammatory Changes Linked to Various Systemic Diseases: A Review of Its Underlying Mechanisms. Biomedicines 2022, 10, 2659. [Google Scholar] [CrossRef] [PubMed]
- Loos, B.G.; Van Dyke, T.E. The role of inflammation and genetics in periodontal disease. Periodontology 2000 2020, 83, 26–39. [Google Scholar] [CrossRef] [PubMed]
- Germen, M.; Baser, U.; Lacin, C.C.; Fıratlı, E.; İşsever, H.; Yalcin, F. Periodontitis Prevalence, Severity, and Risk Factors: A Comparison of the AAP/CDC Case Definition and the EFP/AAP Classification. Int. J. Environ. Res. Public Health 2021, 18, 3459. [Google Scholar] [CrossRef] [PubMed]
- FDI World Dental Federation. The Challenge of Oral Disease—A call for global action. In The Oral Health Atlas, 2nd ed.; Myriad Editions: Brighton, UK, 2015; p. 22. Available online: https://www.fdiworlddental.org/sites/default/files/2021-03/complete_oh_atlas-2_0.pdf (accessed on 25 September 2024).
- Bechir, E.S. The Clinical and Microbiological Effects of LANAP Compared to Scaling and Root Planing Alone in the Management of Periodontal Conditions. Diagnostics 2023, 13, 2450. [Google Scholar] [CrossRef] [PubMed]
- Haque, M.M.; Yerex, K.; Kelekis-Cholakis, A.; Duan, K. Advances in novel therapeutic approaches for periodontal diseases. BMC Oral Health 2022, 22, 492. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Sedghi, L.M.; Bacino, M.; Kapila, Y.L. Periodontal Disease: The Good, The Bad, and The Unknown. Front. Cell. Infect. Microbiol. Sec. Microbiome Health Dis. 2021, 11, 766944. [Google Scholar] [CrossRef] [PubMed]
- Lin, P.; Liu, A.; Tsuchiya, Y.; Noritake, K.; Ohsugi, Y.; Toyoshima, K.; Tsukahara, Y.; Shiba, T.; Nitta, H.; Aoki, A.; et al. Association between periodontal disease and chronic obstructive pulmonary disease. Jpn. Dent. Sci. Rev. 2023, 59, 389–402. [Google Scholar] [CrossRef] [PubMed]
- Wulandari, P. The aging process and its relation to periodontal conditions. Explor. Immunol. 2023, 3, 207–216. [Google Scholar] [CrossRef]
- Zhu, L.; Tang, Z.; Hu, R.; Gu, M.; Yang, Y. Ageing and Inflammation: What Happens in Periodontium? Bioengineering 2023, 10, 1274. [Google Scholar] [CrossRef] [PubMed]
- Janakiram, C.; Dye, B.A. A public health approach for prevention of periodontal disease. Periodontology 2000 2020, 84, 202–214. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Clark, D.; Kotronia, E.; Ramsay, S.E. Frailty, aging, and periodontal disease: Basic biologic considerations. Periodontol 2000 2021, 87, 143–156. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Takedachi, M.; Shimabukuro, Y.; Sawada, K.; Koshimizu, M.; Shinada, K.; Asai, H.; Mizoguchi, A.; Hayashi, Y.; Tsukamoto, A.; Miyago, M.; et al. Evaluation of periodontitis-related tooth loss according to the new 2018 classification of periodontitis. Sci. Rep. 2022, 12, 11893. [Google Scholar] [CrossRef] [PubMed]
- Yamazaki, M.; Yamazaki, K.; Baba, Y.; Ito, H.; Loos, B.G.; Takahashi, K. The Stages and Grades of Periodontitis Are Risk Indicators for Peri-Implant Diseases—A Long-Term Retrospective Study. J. Pers. Med. 2022, 12, 1723. [Google Scholar] [CrossRef] [PubMed]
- Rajasekaran, J.J.; Krishnamurthy, H.K.; Bosco, J.; Jayaraman, V.; Krishna, K.; Wang, T.; Wei, K. Oral Microbiome: A Review of Its Impact on Oral and Systemic Health. Microorganisms 2024, 12, 1797. [Google Scholar] [CrossRef] [PubMed]
- Martínez-García, M.; Hernández-Lemus, E. Periodontal Inflammation and Systemic Diseases: An Overview. Front. Physiol. 2021, 12, 709438. [Google Scholar] [CrossRef] [PubMed]
- Di Stefano, M.; Polizzi, A.; Santonocito, S.; Romano, A.; Lombardi, T.; Isola, G. Impact of Oral Microbiome in Periodontal Health and Periodontitis: A Critical Review on Prevention and Treatment. Int. J. Mol. Sci. 2022, 23, 5142. [Google Scholar] [CrossRef] [PubMed]
- Abdulkareem, A.A.; Al-Taweel, F.B.; Al-Sharqi, A.J.B.; Gul, S.S.; Sha, A.; Chapple, I.L.C. Current concepts in the pathogenesis of periodontitis: From symbiosis to dysbiosis. J. Oral Microbiol. 2023, 15, 2197779. [Google Scholar] [CrossRef] [PubMed]
- Heitz-Mayfield, L.J.A. Conventionaldiagnostic criteria for periodontal diseases (plaque-inducedgingivitis and periodontitis). Periodontology 2000 2024, 95, 10–19. [Google Scholar] [CrossRef] [PubMed]
- Sanz, M.; Herrera, D.; Kebschull, M.; Chapple, I.; Jepsen, S.; Beglundh, T.; Sculean, A.; Tonetti, M.S. EFP Workshop Participants and Methodological Consultants. Treatment of stage I-III periodontitis-The EFP S3 level clinical practice guideline. J. Clin. Periodontol. 2020, 47 (Suppl. S22), 4–60, Erratum in J. Clin. Periodontol. 2021, 48, 163. [Google Scholar] [CrossRef] [PubMed]
- Altalhi, A.M.; AlNajdi, L.N.; Al-Harbi, S.G.; Aldohailan, A.M.; Al-Ghadeer, J.Y.; Al-Bahrani, J.I.; Al-Gahnem, Z.J.; Alenezi, A.H.; Al-Majid, A. Laser Therapy Versus Traditional Scaling and Root Planing: A Comparative Review. Cureus 2024, 16, e61997. [Google Scholar] [CrossRef] [PubMed]
- Jha, A.; Gupta, V.; Adinarayan, R. LANAP, Periodontics and Beyond: A Review. J. Lasers Med. Sci. 2018, 9, 76–81. [Google Scholar] [CrossRef] [PubMed]
- Rajesh, K.S.; Siva Pillai, A.S.; Shashikanth, H.; Kumar, A.M.S.; Boloor, V. The LANAP Procedure—An Update. IOSR J. Dent. Med. Sci. IOSR-JDMS 2021, 20, 1–6. [Google Scholar]
- Mahdizade Ari, M.; Amirmozafari, N.; Darbandi, A.; Afifirad, R.; Asadollahi, P.; Irajian, G. Effectiveness of photodynamic therapy on the treatment of chronic periodontitis: A systematic review during 2008–2023. Front. Chem. 2024, 12, 1384344. [Google Scholar] [CrossRef] [PubMed]
- Pardo, A.; Butera, A.; Giordano, A.; Gallo, S.; Pascadopoli, M.; Scribante, A.; Albanese, M. Photodynamic Therapy in Non-Surgical Treatment of Periodontitis: A Systematic Review and Meta-Analysis. Appl. Sci. 2023, 13, 1086. [Google Scholar] [CrossRef]
- Scribante, A.; Gallo, S.; Pascadopoli, M.; Frani, M.; Butera, A. Ozonized gels vs chlorhexidine in non-surgical periodontal treatment: A randomized clinical trial. Oral Dis. 2023, 30, 3993–4000. [Google Scholar] [CrossRef] [PubMed]
- Available online: https://inomedis.lv/en/catalog/brendy/fotona/lightwalker-at-at-s/ (accessed on 28 February 2025).
- Available online: https://www.consort-spirit.org/ (accessed on 3 June 2025).
- Chatzopoulos, G.S.; Jiang, Z.; Marka, N.; Wolff, L.F. Association between Periodontitis Extent, Severity, and Progression Rate with Systemic Diseases and Smoking: A Retrospective Study. J. Pers. Med. 2023, 13, 814. [Google Scholar] [CrossRef] [PubMed]
- Tonetti, M.S.; Sanz, M. Implementation of the new classification of periodontal diseases: Decision-making algorithms for clinical practice and education. J. Clin. Periodontol. 2019, 46, 398–405. [Google Scholar] [CrossRef] [PubMed]
- Soderling, F.; Torabi, J. The A, B, Cs, and I, II, and IIIs of Periodontitis Staging and Grading. CDHA J. 2019, 37, 22–28. [Google Scholar]
- Tsai, C.Y.; Tang, C.Y.; Tan, T.S.; Chen, K.H.; Liao, K.H.; Liou, M.L. Subgingival microbiota in individuals with severe chronic periodontitis. J. Microbiol. Immunol. Infect. 2018, 51, 226–234. [Google Scholar] [CrossRef] [PubMed]
- Gasner, N.S.; Schure, R.S. Periodontal Disease. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2023. [Google Scholar]
- Lazar, L.; Loghin, A.; Bud, E.-S.; Cerghizan, D.; Horvath, E.; Nagy, E.E. Cyclooxygenase-2 and matrix metalloproteinase-9 expressions correlate with tissue inflammation degree in periodontal disease. Rom. J. Morphol. Embryol. 2015, 56, 1441–1446. [Google Scholar] [PubMed]
- Matarese, G.; Ramaglia, L.; Cicciù, M.; Cordasco, G.; Isola, G. The Effects of Diode Laser Therapy as an Adjunct to Scaling and Root Planing in the Treatment of Aggressive Periodontitis: A 1-Year Randomized Controlled Clinical Trial. Photomed. Laser Surg. 2017, 35, 702–709. [Google Scholar] [CrossRef] [PubMed]
- Lalli, A.K.; Dhingra, S.; Lalli, A.S.; Kaur, G.; Gupta, H.; Goyal, S. Clinical Evaluation of Diode Laser as an Adjunct to Scaling and Root Planing in Patients With Chronic Periodontitis and Type II Diabetes Mellitus: A Split-Mouth Study. Cureus 2024, 16, e54178. [Google Scholar] [CrossRef] [PubMed]
- Seyed-Monir, A.; Seyed-Monir, E.; Mihandoust, S. Evaluation of 940-nm diode laser effectiveness on pocket depth, clinical attachment level, and bleeding on probing in chronic periodontitis: A randomized clinical single-masked split-mouth study. Dent. Res. J. 2023, 20, 113. [Google Scholar] [CrossRef]
- Subedi, S.; Patil, S.S.; Baniya, B.K.; Bista, S.; Kafle, B.; Shrestha, N. Assessment of Attachment Level by Laser in Pocket Therapy. J. Nepal. Health Res. Counc. 2022, 20, 436–440. [Google Scholar] [CrossRef] [PubMed]
- Yu, Y.H.; Nevins, M.L. Tooth Retention and Clinical and Radiographic Long-Term Results Among Patients Treated with the Full-Mouth Laser-Assisted New Attachment Procedure (LANAP): A Case Series. Int. J. Periodontics Restor. Dent. 2023, 43, 181a–191a. [Google Scholar] [CrossRef] [PubMed]
- El Mobadder, M.; Namour, A.; Nammour, S. Laser-Assisted Non-Surgical Treatments of Periodontitis. Encyclopedia 2023, 3, 458–467. [Google Scholar] [CrossRef]
- Yukna, R.A. Clinical evaluation of Laser-Assisted New Attachment Procedure® (LANAP®) surgical treatment of chronic periodontitis: A retrospective case series of 1-year results in 22 consecutive patients. J. Periodontal Implant Sci. 2023, 53, 173–183. [Google Scholar] [CrossRef] [PubMed]
- Relvas, M.; López-Jarana, P.; Monteiro, L.; Pacheco, J.J.; Braga, A.C.; Salazar, F. Study of Prevalence, Severity and Risk Factors of Periodontal Disease in a Portuguese Population. J. Clin. Med. 2022, 11, 3728. [Google Scholar] [CrossRef] [PubMed]
- Nazir, M.A. Prevalence of periodontal disease, its association with systemic diseases and prevention. Int J Health Sci. 2017, 2, 72–80. [Google Scholar]
- Cerghizan, D.; Neagu, A.I.; Maris, M.; Buruiana, D.L.; Condurache, G.G.; Topor, G.; Matei, M. Interrelation between prosthetic and orthodontic treatment. Rom. J. Oral Rehabil. 2020, 12, 145–156. [Google Scholar]
- Isola, G.; Santonocito, S.; Lupi, S.M.; Polizzi, A.; Sclafani, R.; Patini, R.; Marchetti, E. Periodontal Health and Disease in the Context of Systemic Diseases. Mediat. Inflamm. 2023, 2023, 9720947. [Google Scholar] [CrossRef] [PubMed]
- Acatrinei, D.; Forna, N.; Acatrinei, B.-S.; Acatrinei, D.I.; Rosoiu, N. Comparative study of treatment of non-surgical periodontal disease: SRP & Laser therapy vs. Plasma. Rom. J. Oral Rehabil. 2023, 15, 256–271. [Google Scholar]
- Dolińska, E.; Skurska, A.; Pietruska, M.; Dymicka-Piekarska, V.; Milewski, R.; Sculean, A. Effect of nonsurgical periodontal therapy with additional photodynamic therapy on the level of MMP-9 and TIMP-1 in GCF in chronic periodontitis patients-a preliminary pilot study. Adv. Med. Sci. 2024, 69, 362–367. [Google Scholar] [CrossRef] [PubMed]
- Alwael, A.; Kim, I.; Steffensen, B.; Hawley, C.; Uzel, G.; Karimbux, N.; Pagni, S.; Gyurko, R. Clinical and Microbiological Outcomes of Er:YAG Laser Used as an Adjunct in Non-Surgical Periodontal Therapy: A Randomized Clinical Trial. J Clin Res Med. 2021, 4, 1–6. [Google Scholar]
- Markou, N.; Papadelli, A.; Nikolidakis, D.; Pepelassi, E.; Madianos, P.; Karoussis, I.K. Adjunctive Nd:YAG laser irradiation in the treatment of stage III/IV periodontitis: A 12-month, randomized, controlled trial. Clin. Oral Investig. 2023, 27, 3045–3056. [Google Scholar] [CrossRef] [PubMed]
- Ciurescu, C.E.; Dima, L.; Ciurescu, V.A.; Noja, G.G.; Istodor, A.V.; Moga, M.A.; Ardelean, L.C.; Rusu, L.C.; Leretter, M.T. Laser Therapy Effects on Periodontal Status: A Randomized Study Using Gaussian Network Analysis and Structural Equation Modeling Approach. Medicina 2024, 60, 437. [Google Scholar] [CrossRef] [PubMed]
- Sareen, S.; Gupta, S.; Goyal, L. Ozone therapy as a complementary approach in periodontal therapeutics. Evid. Based Dent. 2025, 26, 91–92. [Google Scholar] [CrossRef] [PubMed]
- Hashim, N.T.; Babiker, R.; Dasnadi, S.P.; Islam, M.S.; Chaitanya, N.C.; Mohammed, R.; Farghal, N.S.; Gobara, B.; Rahman, M.M. The Impact of Ozone on Periodontal Cell Line Viability and Function. Curr. Issues Mol. Biol. 2025, 47, 72. [Google Scholar] [CrossRef] [PubMed]
- Scribante, A.; Butera, A.; Alovisi, M. Customized Minimally Invasive Protocols for the Clinical and Microbiological Management of the Oral Microbiota. Microorganisms 2022, 10, 675. [Google Scholar] [CrossRef] [PubMed]
- Butera, A.; Gallo, S.; Pascadopoli, M.; Taccardi, D.; Scribante, A. Home Oral Care of Periodontal Patients Using Antimicrobial Gel with Postbiotics, Lactoferrin, and Aloe Barbadensis Leaf Juice Powder vs. Conventional Chlorhexidine Gel: A Split-Mouth Randomized Clinical Trial. Antibiotics 2022, 11, 118. [Google Scholar] [CrossRef] [PubMed]
- Castro, S.; Garay, S.; Espinoza-Carhuancho, F.; Medina, J.; Mendoza, R.; Mauricio, F.; Mayta-Tovalino, F. Exploring the potential of probiotics in dentistry: A literature review. Odovtos Int. J. Dent. Sci. 2024, 26, 28–40. [Google Scholar] [CrossRef]
- Sachelarie, L.; Scrobota, I.; Romanul, I.; Iurcov, R.; Potra Cicalau, G.I.; Todor, L. Probiotic Therapy as an Adjuvant in the Treatment of Periodontal Disease: An Innovative Approach. Medicina 2025, 61, 126. [Google Scholar] [CrossRef] [PubMed]
- Roccuzzo, A.; De Ry, S.P.; Sculean, A.; Roccuzzo, M.; Salvi, G.E. Current Approaches for the Non-surgical Management of Peri-implant Diseases. Curr. Oral Health Rep. 2020, 7, 274–282. [Google Scholar] [CrossRef]
- Salehuddin, N.Q.; Sabri, B.A.M.; Ariffin, F. Patients’ view on non-surgical and surgical periodontal therapy in relation to oral health: A narrative review. Dent. Rev. 2022, 2, 100058. [Google Scholar] [CrossRef]
- Bechir, E.S. Comparative oral health outcomes before and after periodontitis treatment: Scaling and root planning alone versus Nd: YAG Laser Assisted New Attachment Procedure. Acta Stomatol. Marisiensis 2023, 6, 4–13. [Google Scholar] [CrossRef]
- Cobb, C.M.; Sottosanti, J.S. A re-evaluation of scaling and root planning. J. Periodontol. 2021, 92, 1370–1378. [Google Scholar] [CrossRef] [PubMed]
- Bartold, P.M.; Ivanovski, S. P4 Medicine as a model for precision periodontal care. Clin. Oral. Investig. 2022, 26, 5517–5533. [Google Scholar] [CrossRef] [PubMed]
- Kikuchi, T.; Hayashi, J.-i.; Mitani, A. Next-Generation Examination, Diagnosis, and Personalized Medicine in Periodontal Disease. J. Pers. Med. 2022, 12, 1743. [Google Scholar] [CrossRef] [PubMed]
- Juncar, R.I.; Moca, A.E.; Juncar, M.; Moca, R.T.; Țenț, P.A. Clinical patterns and treatment of pediatric facial fractures: A 10-year retrospective Romanian study. Children 2023, 10, 800. [Google Scholar] [CrossRef] [PubMed]
- Neha, H.N.; Nagarathna, D.V. Predictive, Preventive, Personalized and Participatory Medicine as a Model for Precision Periodontal Health Care. Int. J. Innov. Sci. Res. Technol. 2024, 9, 2921–2925. [Google Scholar]
- Kwon, T.; Lamster, I.B.; Levin, L. Current Concepts in the Management of Periodontitis. Int. Dent. J. 2021, 71, 462–476. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
| Inclusion Criteria | Exclusion Criteria |
|---|---|
|
|
| Variable | SRP | p Values SRP | LANAP | p Values LANAP |
|---|---|---|---|---|
| % plaque | 1.00 | 0.0003 | 0.929 | 0.0007 |
| % bleeding | 1.286 | 3.406 | 1.286 | 8.177 |
| Periodontal probing depth (PPD) | 0.464 | 1.667 | 0.493 | 3.101 |
| Loss of attachment | −0.536 | 0.001 | −0.521 | 1.372 |
| Variable | SRP Mean | p Values SRP | LANAP Mean | p Values LANAP |
|---|---|---|---|---|
| % plaque | 3.714 | 0.026 | 1.714 | 0.102 |
| % bleeding | 2.714 | 0.050 * | 1.857 | 0.071 |
| Periodontal probing depth (PPD) | 0.543 | 0.006 * | 0.521 | 0.165 |
| Loss of attachment | −0.636 | 0.016 | −0.564 | 0.054 |
| Variable | Mean Before Treatments | After 1 Year Post-Treatments | ||||
|---|---|---|---|---|---|---|
| SRP Group | LANAP Group | SRP | p Values SRP | LANAP | p Values LANAP | |
| % plaque | 8.786 | 6.643 | 3.714 | 0.026 | 1.714 | 0.102 |
| % bleeding | 9.429 | 9.571 | 2.714 | 0.05 * | 1.857 | 0.071 |
| Periodontal probing depth (PPD) | 0.629 | 0.693 | 0.543 | 0.006 * | 0.521 | 0.165 |
| Loss of attachment | −0.671 | −0.721 | −0.636 | 0.016 | −0.564 | 0.054 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bechir, E.S.; Bechir, F.; Suciu, M.; Bechir, A.; Nicolau, A.C. Twelve-Month Follow-Up After the Treatment of Periodontal Conditions Using Scaling and Root Planning Alone vs. Laser-Assisted New Attachment Procedure. Diagnostics 2025, 15, 1799. https://doi.org/10.3390/diagnostics15141799
Bechir ES, Bechir F, Suciu M, Bechir A, Nicolau AC. Twelve-Month Follow-Up After the Treatment of Periodontal Conditions Using Scaling and Root Planning Alone vs. Laser-Assisted New Attachment Procedure. Diagnostics. 2025; 15(14):1799. https://doi.org/10.3390/diagnostics15141799
Chicago/Turabian StyleBechir, Edwin Sever, Farah Bechir, Mircea Suciu, Anamaria Bechir, and Andrada Camelia Nicolau. 2025. "Twelve-Month Follow-Up After the Treatment of Periodontal Conditions Using Scaling and Root Planning Alone vs. Laser-Assisted New Attachment Procedure" Diagnostics 15, no. 14: 1799. https://doi.org/10.3390/diagnostics15141799
APA StyleBechir, E. S., Bechir, F., Suciu, M., Bechir, A., & Nicolau, A. C. (2025). Twelve-Month Follow-Up After the Treatment of Periodontal Conditions Using Scaling and Root Planning Alone vs. Laser-Assisted New Attachment Procedure. Diagnostics, 15(14), 1799. https://doi.org/10.3390/diagnostics15141799