
Evaluation of Corneal Sensitivity: Tools We Have


Abstract
1. Introduction
1.1. The Cornea, Corneal Sensation, and Neurotrophic Keratopathy
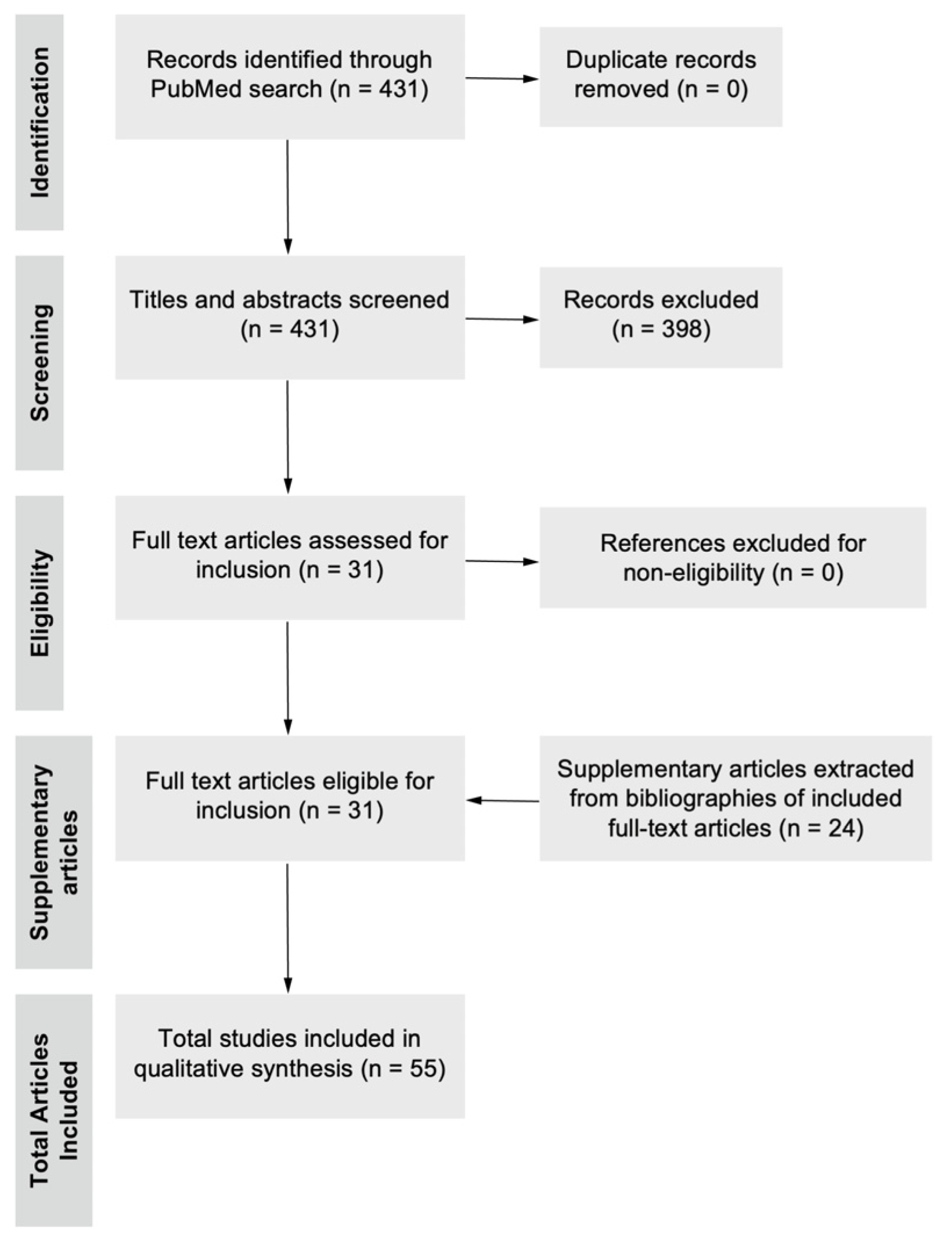
1.2. Search Strategy and Selection Criteria
2. Overview of the History and Types of Aesthesiometers
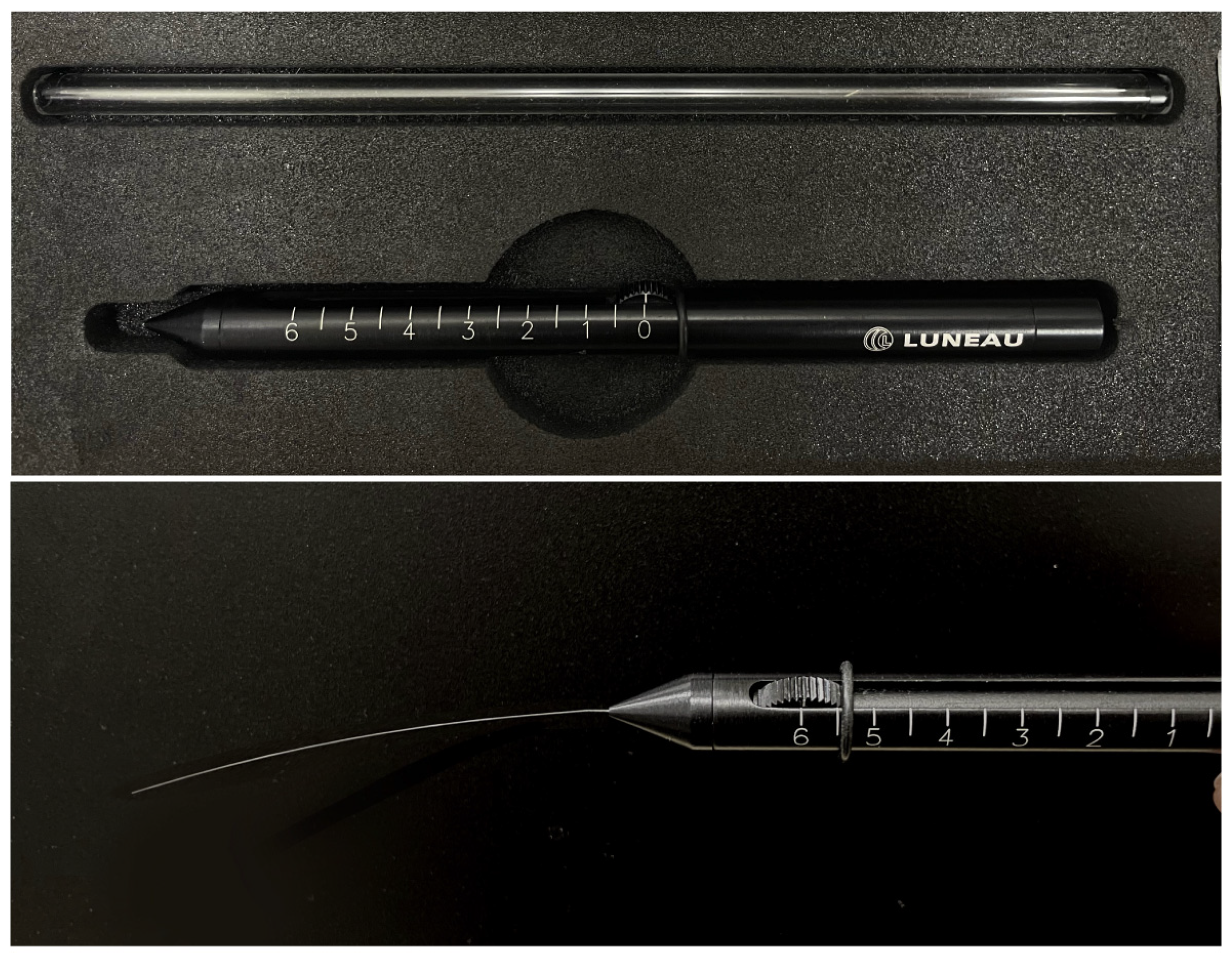
2.1. Cochet–Bonnet Aesthesiometry
2.2. Gas-Based Non-Contact Corneal Aesthesiometers
2.3. Swiss Liquid-Jet Aesthesiometer for Corneal Sensitivity
2.4. Non-Contact Brill Aesthesiometer
3. Correlation Between Corneal Sensitivity and Innervation
4. Conclusions and Future Directions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| NSAIDs | Non-steroidal anti-inflammatory agents |
| IVCM | In vivo confocal microscopy |
| NCCA | Non-contact corneal aesthesiometer |
| SLACS | Swiss liquid-jet aesthesiometer for corneal sensitivity |
| LED | Light-emitting diode |
| LASIK | Laser-assisted in situ keratomileusis |
| LASEK | Laser-assisted epithelial keratomileusis |
References
- Bonini, S.; Rama, P.; Olzi, D.; Lambiase, A. Neurotrophic keratitis. Eye 2003, 17, 989–995. [Google Scholar] [CrossRef] [PubMed]
- Feinberg, K.; Tajdaran, K.; Mirmoeini, K.; Daeschler, S.C.; Henriquez, M.A.; Stevens, K.E.; Mulenga, C.M.; Hussain, A.; Hamrah, P.; Ali, A.; et al. The Role of Sensory Innervation in Homeostatic and Injury-Induced Corneal Epithelial Renewal. Int. J. Mol. Sci. 2023, 24, 12615. [Google Scholar] [CrossRef] [PubMed]
- Crabtree, J.R.; Tannir, S.; Tran, K.; Boente, C.S.; Ali, A.; Borschel, G.H. Corneal Nerve Assessment by Aesthesiometry: History, Advancements, and Future Directions. Vision 2024, 8, 34. [Google Scholar] [CrossRef] [PubMed]
- Sacchetti, M.; Lambiase, A. Diagnosis and management of neurotrophic keratitis. Clin. Ophthalmol. 2014, 8, 571–579. [Google Scholar] [CrossRef] [PubMed]
- Yang, A.Y.; Chow, J.; Liu, J. Corneal Innervation and Sensation: The Eye and Beyond. Yale J. Biol. Med. 2018, 91, 13–21. [Google Scholar] [PubMed]
- Liu, Y.C.; Jung, A.S.J.; Chin, J.Y.; Yang, L.W.Y.; Mehta, J.S. Cross-sectional Study on Corneal Denervation in Contralateral Eyes Following SMILE Versus LASIK. J. Refract. Surg. 2020, 36, 653–660. [Google Scholar] [CrossRef] [PubMed]
- Liu, C.; Lin, M.T.; Lee, I.X.Y.; Wong, J.H.F.; Lu, D.; Lam, T.C.; Zhou, L.; Mehta, J.S.; Ong, H.S.; Ang, M.; et al. Neuropathic Corneal Pain: Tear Proteomic and Neuromediator Profiles, Imaging Features, and Clinical Manifestations. Am. J. Ophthalmol. 2024, 265, 6–20. [Google Scholar] [CrossRef] [PubMed]
- Romero-Díaz de León, L.; Morales-León, J.E.; Ledesma-Gil, J.; Navas, A. Conjunctival and corneal sensitivity in patients under topical antiglaucoma treatment. Int. Ophthalmol. 2016, 36, 299–303. [Google Scholar] [CrossRef] [PubMed]
- Polat, O.A.; Şener, H.; Erkiliç, K. Corneal Nerve Fiber and Sensitivity Loss After Repeated Intravitreal Anti-VEGF Injections: An In Vivo Confocal Microscopy Study. Cornea 2022, 41, 317–321. [Google Scholar] [CrossRef] [PubMed]
- Singer, D.D.; Kennedy, J.; Wittpenn, J.R. Topical NSAIDs effect on corneal sensitivity. Cornea 2015, 34, 541–543. [Google Scholar] [CrossRef] [PubMed]
- Chiang, J.C.B.; Goldstein, D.; Trinh, T.; Au, K.; Mizrahi, D.; Muhlmann, M.; Crowe, P.; O’Neill, S.; Edwards, K.; Park, S.B.; et al. A Cross-Sectional Study of Sub-Basal Corneal Nerve Reduction Following Neurotoxic Chemotherapy. Transl. Vis. Sci. Technol. 2021, 10, 24. [Google Scholar] [CrossRef] [PubMed]
- Mansoor, H.; Tan, H.C.; Lin, M.T.; Mehta, J.S.; Liu, Y.C. Diabetic Corneal Neuropathy. J. Clin. Med. 2020, 9, 3956. [Google Scholar] [CrossRef] [PubMed]
- So, W.Z.; Qi Wong, N.S.; Tan, H.C.; Yu Lin, M.T.; Yu Lee, I.X.; Mehta, J.S.; Liu, Y.C. Diabetic corneal neuropathy as a surrogate marker for diabetic peripheral neuropathy. Neural Regen. Res. 2022, 17, 2172–2178. [Google Scholar] [CrossRef] [PubMed]
- Kim, I.G.; Lee, J.H.; Kim, S.S. Reduced corneal sensitivity in patients with rheumatoid arthritis. Cornea 2012, 31, 1381–1385. [Google Scholar] [CrossRef] [PubMed]
- Rocha, E.M.; Gutierrez, D.R. Hypovitaminosis A: A hidden cause of neurotrophic keratitis. Arq. Bras. Oftalmol. 2024, 87, e2023. [Google Scholar] [CrossRef] [PubMed]
- Nassiri, N.; Assarzadegan, F.; Shahriari, M.; Norouzi, H.; Kavousnezhad, S.; Nassiri, N.; Sheibani, K. Vitamin B12 Deficiency as a Cause of Neurotrophic Keratopathy. Open Ophthalmol. J. 2018, 12, 7–11. [Google Scholar] [CrossRef] [PubMed]
- Roszkowska, A.M.; Colosi, P.; Ferreri, F.M.; Galasso, S. Age-related modifications of corneal sensitivity. Ophthalmologica 2004, 218, 350–355. [Google Scholar] [CrossRef] [PubMed]
- Nosch, D.S.; Käser, E.; Bracher, T.; Joos, R.E. Age-Related Changes in Corneal Sensitivity. Cornea 2023, 42, 1257–1262. [Google Scholar] [CrossRef] [PubMed]
- Acosta, M.C.; Alfaro, M.L.; Borrás, F.; Belmonte, C.; Gallar, J. Influence of age, gender and iris color on mechanical and chemical sensitivity of the cornea and conjunctiva. Exp. Eye Res. 2006, 83, 932–938. [Google Scholar] [CrossRef] [PubMed]
- Dua, H.S.; Said, D.G.; Messmer, E.M.; Rolando, M.; Benitez-Del-Castillo, J.M.; Hossain, P.N.; Shortt, A.J.; Geerling, G.; Nubile, M.; Figueiredo, F.C.; et al. Neurotrophic keratopathy. Prog. Retin. Eye Res. 2018, 66, 107–131. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.C.; Lin, M.T.; Mehta, J.S. Analysis of corneal nerve plexus in corneal confocal microscopy images. Neural Regen. Res. 2021, 16, 690–691. [Google Scholar] [CrossRef] [PubMed]
- Draeger, J. Development of the Various Methods of Esthesiometry. In Corneal Sensitivity: Measurement and Clinical Importance; Draeger, J., Ed.; Springer: Vienna, Austria, 1984; pp. 8–34. [Google Scholar] [CrossRef]
- Murphy, P.J.; Patel, S.; Marshall, J. A new non-contact corneal aesthesiometer (NCCA). Ophthalmic Physiol. Opt. 1996, 16, 101–107. [Google Scholar] [CrossRef] [PubMed]
- Seyed-Razavi, Y.; Kenyon, B.M.; Qiu, F.; Harris, D.L.; Hamrah, P. A novel animal model of neuropathic corneal pain-the ciliary nerve constriction model. Front. Neurosci. 2023, 17, 1265708. [Google Scholar] [CrossRef] [PubMed]
- De Silva, M.E.H.; Hill, L.J.; Downie, L.E.; Chinnery, H.R. The Effects of Aging on Corneal and Ocular Surface Homeostasis in Mice. Investig. Ophthalmol. Vis. Sci. 2019, 60, 2705–2715. [Google Scholar] [CrossRef] [PubMed]
- Mansoor, H.; Lee, I.X.Y.; Lin, M.T.-Y.; Ang, H.P.; Xue, Y.C.; Krishaa, L.; Patil, M.; Koh, S.-K.; Tan, H.C.; Zhou, L.; et al. Topical and oral peroxisome proliferator-activated receptor-α agonist ameliorates diabetic corneal neuropathy. Sci. Rep. 2024, 14, 13435. [Google Scholar] [CrossRef] [PubMed]
- Nosch, D.S.; Käser, E.; Bracher, T.; Joos, R.E. Clinical application of the Swiss Liquid Jet Aesthesiometer for corneal sensitivity measurement. Clin. Exp. Optom. 2024, 107, 14–22. [Google Scholar] [CrossRef] [PubMed]
- Belmonte, C.; Acosta, M.C.; Schmelz, M.; Gallar, J. Measurement of corneal sensitivity to mechanical and chemical stimulation with a CO2 esthesiometer. Investig. Ophthalmol. Vis. Sci. 1999, 40, 513–519. [Google Scholar]
- Stapleton, F.; Tan, M.E.; Papas, E.B.; Ehrmann, K.; Golebiowski, B.; Vega, J.; Holden, B.A. Corneal and conjunctival sensitivity to air stimuli. Br. J. Ophthalmol. 2004, 88, 1547–1551. [Google Scholar] [CrossRef] [PubMed]
- Ehrmann, K.; Saha, M.; Falk, D. A novel method to stimulate mechanoreceptors and quantify their threshold values. Biomed. Phys. Eng. Express 2018, 4, 025004. [Google Scholar] [CrossRef]
- Nosch, D.S.; Oscity, M.; Steigmeier, P.; Käser, E.; Loepfe, M.; Joos, R.E. Working principle and relevant physical properties of the Swiss Liquid Jet Aesthesiometer for Corneal Sensitivity (SLACS) evaluation. Ophthalmic Physiol. Opt. 2022, 42, 609–618. [Google Scholar] [CrossRef] [PubMed]
- Merayo-Lloves, J.; Gómez Martín, C.; Lozano-Sanroma, J.; Renedo Laguna, C. Assessment and safety of the new esthesiometer BRILL: Comparison with the Cochet-Bonnet Esthesiometer. Eur. J. Ophthalmol. 2024, 34, 1036–1045. [Google Scholar] [CrossRef] [PubMed]
- Lum, E.; Murphy, P.J. Effects of ambient humidity on the Cochet-Bonnet aesthesiometer. Eye 2018, 32, 1644–1651. [Google Scholar] [CrossRef] [PubMed]
- Reinstein, D.Z.; Archer, T.J.; Gobbe, M.; Bartoli, E. Corneal sensitivity after small-incision lenticule extraction and laser in situ keratomileusis. J. Cataract. Refract. Surg. 2015, 41, 1580–1587. [Google Scholar] [CrossRef] [PubMed]
- Bucher, F.; Adler, W.; Lehmann, H.C.; Hos, D.; Steven, P.; Cursiefen, C.; Heindl, L.M. Corneal nerve alterations in different stages of Fuchs’ endothelial corneal dystrophy: An in vivo confocal microscopy study. Graefes Arch. Clin. Exp. Ophthalmol. 2014, 252, 1119–1126. [Google Scholar] [CrossRef] [PubMed]
- Cruzat, A.; Hamrah, P.; Cavalcanti, B.M.; Zheng, L.; Colby, K.; Pavan-Langston, D. Corneal Reinnervation and Sensation Recovery in Patients With Herpes Zoster Ophthalmicus: An In Vivo and Ex Vivo Study of Corneal Nerves. Cornea 2016, 35, 619–625. [Google Scholar] [CrossRef] [PubMed]
- Murphy, P.J.; Lawrenson, J.G.; Patel, S.; Marshall, J. Reliability of the non-contact corneal aesthesiometer and its comparison with the Cochet-Bonnet aesthesiometer. Ophthalmic Physiol. Opt. 1998, 18, 532–539. [Google Scholar] [PubMed]
- Golebiowski, B.; Papas, E.; Stapleton, F. Assessing the sensory function of the ocular surface: Implications of use of a non-contact air jet aesthesiometer versus the Cochet-Bonnet aesthesiometer. Exp. Eye Res. 2011, 92, 408–413. [Google Scholar] [CrossRef] [PubMed]
- Tesón, M.; Calonge, M.; Fernández, I.; Stern, M.E.; González-García, M.J. Characterization by Belmonte’s gas esthesiometer of mechanical, chemical, and thermal corneal sensitivity thresholds in a normal population. Investig. Ophthalmol. Vis. Sci. 2012, 53, 3154–3160. [Google Scholar] [CrossRef] [PubMed]
- Golebiowski, B.; Lim, M.; Papas, E.; Stapleton, F. Understanding the stimulus of an air-jet aesthesiometer: Computerised modelling and subjective interpretation. Ophthalmic Physiol. Opt. 2013, 33, 104–113. [Google Scholar] [CrossRef] [PubMed]
- Villalba, M.; Sabates, V.; Orgul, S.; Perez, V.L.; Swaminathan, S.S.; Sabater, A.L. Detection of Subclinical Neurotrophic Keratopathy by Noncontact Esthesiometry. Ophthalmol. Ther. 2024, 13, 2393–2404. [Google Scholar] [CrossRef] [PubMed]
- Ruiz-Lozano, R.E.; Quiroga-Garza, M.E.; Ramos-DÁVila, E.M.; PantaleÓN-GarcÍA, J.; Khodor, A.L.I.; Komai, S.; Rodriguez-Gutierrez, L.A.; Ma, S.; Mousa, H.M.; Mattes, R.; et al. Comparative Evaluation of the Corneal Sensitivity Thresholds between the Novel Non-Contact and Cochet-Bonnet Esthesiometers. Am. J. Ophthalmol. 2025, 271, 407–416. [Google Scholar] [CrossRef] [PubMed]
- Surico, P.L.; Saricay, L.Y.; Singh, R.B.; Kahale, F.; Romano, F.; Dana, R. Corneal Sensitivity and Neuropathy in Patients With Ocular Graft-Versus-Host Disease. Cornea 2022, 44, 838–844. [Google Scholar] [CrossRef] [PubMed]
- Benítez-Del-Castillo, J.M.; Acosta, M.C.; Wassfi, M.A.; Díaz-Valle, D.; Gegúndez, J.A.; Fernandez, C.; García-Sánchez, J. Relation between corneal innervation with confocal microscopy and corneal sensitivity with noncontact esthesiometry in patients with dry eye. Investig. Ophthalmol. Vis. Sci. 2007, 48, 173–181. [Google Scholar] [CrossRef] [PubMed]
- Martone, G.; Frezzotti, P.; Tosi, G.M.; Traversi, C.; Mittica, V.; Malandrini, A.; Pichierri, P.; Balestrazzi, A.; Motolese, P.A.; Motolese, I.; et al. An in vivo confocal microscopy analysis of effects of topical antiglaucoma therapy with preservative on corneal innervation and morphology. Am. J. Ophthalmol. 2009, 147, 725–735.el. [Google Scholar] [CrossRef] [PubMed]
- Patel, D.V.; Ku, J.Y.; Johnson, R.; McGhee, C.N. Laser scanning in vivo confocal microscopy and quantitative aesthesiometry reveal decreased corneal innervation and sensation in keratoconus. Eye 2009, 23, 586–592. [Google Scholar] [CrossRef] [PubMed]
- Hamrah, P.; Cruzat, A.; Dastjerdi, M.H.; Zheng, L.; Shahatit, B.M.; Bayhan, H.A.; Dana, R.; Pavan-Langston, D. Corneal sensation and subbasal nerve alterations in patients with herpes simplex keratitis: An in vivo confocal microscopy study. Ophthalmology 2010, 117, 1930–1936. [Google Scholar] [CrossRef] [PubMed]
- Stachs, O.; Zhivov, A.; Kraak, R.; Hovakimyan, M.; Wree, A.; Guthoff, R. Structural-functional correlations of corneal innervation after LASIK and penetrating keratoplasty. J. Refract. Surg. 2010, 26, 159–167. [Google Scholar] [CrossRef] [PubMed]
- Rosenberg, M.E.; Tervo, T.M.; Immonen, I.J.; Müller, L.J.; Grönhagen-Riska, C.; Vesaluoma, M.H. Corneal structure and sensitivity in type 1 diabetes mellitus. Investig. Ophthalmol. Vis. Sci. 2000, 41, 2915–2921. [Google Scholar]
- Aggarwal, S.; Cavalcanti, B.M.; Regali, L.; Cruzat, A.; Trinidad, M.; Williams, C.; Jurkunas, U.V.; Hamrah, P. In Vivo Confocal Microscopy Shows Alterations in Nerve Density and Dendritiform Cell Density in Fuchs’ Endothelial Corneal Dystrophy. Am. J. Ophthalmol. 2018, 196, 136–144. [Google Scholar] [CrossRef] [PubMed]
- Tavakoli, M.; Kallinikos, P.A.; Efron, N.; Boulton, A.J.; Malik, R.A. Corneal sensitivity is reduced and relates to the severity of neuropathy in patients with diabetes. Diabetes Care 2007, 30, 1895–1897. [Google Scholar] [CrossRef] [PubMed]
- Dikmetas, O.; Kocabeyoglu, S.; Mocan, M.C.; Karahan, S.; İrkec, M. The relationship between corneal subbasal nerve density and corneal sensitivity in patients with Fuchs endothelial corneal dystrophy. Indian J. Ophthalmol. 2021, 69, 1730–1734. [Google Scholar] [CrossRef] [PubMed]
- Labbé, A.; Alalwani, H.; Van Went, C.; Brasnu, E.; Georgescu, D.; Baudouin, C. The relationship between subbasal nerve morphology and corneal sensation in ocular surface disease. Investig. Ophthalmol. Vis. Sci. 2012, 53, 4926–4931. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.J.; Kim, J.K.; Seo, K.Y.; Kim, E.K.; Lee, H.K. Comparison of corneal nerve regeneration and sensitivity between LASIK and laser epithelial keratomileusis (LASEK). Am. J. Ophthalmol. 2006, 141, 1009–1015.el. [Google Scholar] [CrossRef] [PubMed]
- Han, S.B.; Liu, Y.C.; Liu, C.; Mehta, J.S. Applications of Imaging Technologies in Fuchs Endothelial Corneal Dystrophy: A Narrative Literature Review. Bioengineering 2024, 11, 271. [Google Scholar] [CrossRef] [PubMed]
- Chin, J.Y.; Yang, L.W.Y.; Ji, A.J.S.; Nubile, M.; Mastropasqua, L.; Allen, J.C.; Mehta, J.S.; Liu, Y.C. Validation of the Use of Automated and Manual Quantitative Analysis of Corneal Nerve Plexus Following Refractive Surgery. Diagnostics 2020, 10, 493. [Google Scholar] [CrossRef] [PubMed]
- Stewart, S.; Liu, Y.C.; Lin, M.T.; Mehta, J.S. Clinical Applications of In Vivo Confocal Microscopy in Keratorefractive Surgery. J. Refract. Surg. 2021, 37, 493–503. [Google Scholar] [CrossRef] [PubMed]
- Patel, D.V.; Tavakoli, M.; Craig, J.P.; Efron, N.; McGhee, C.N. Corneal sensitivity and slit scanning in vivo confocal microscopy of the subbasal nerve plexus of the normal central and peripheral human cornea. Cornea 2009, 28, 735–740. [Google Scholar] [CrossRef] [PubMed]
- Müller, L.J.; Marfurt, C.F.; Kruse, F.; Tervo, T.M. Corneal nerves: Structure, contents and function. Exp. Eye Res. 2003, 76, 521–542. [Google Scholar] [CrossRef] [PubMed]
- Erie, J.C.; McLaren, J.W.; Hodge, D.O.; Bourne, W.M. The effect of age on the corneal subbasal nerve plexus. Cornea 2005, 24, 705–709. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
| Etiology of Corneal Neuropathy | |
|---|---|
| Ocular | Herpetic, viral or bacterial infections Chemical burns, physical injuries Corneal surgery Corneal dystrophies Limbal stem cell deficiency Keratoconus Long-term contact lens use Pharmacological agents (anti-glaucoma eyedrops, intravitreal injections, topical NSAIDs) |
| Systemic | Acquired neuropathy: diabetic corneal neuropathy, chemotherapy-induced Inherited neuropathies: Charcot-Marie-Tooth Autoimmune: rheumatoid arthritis, fibromyalgia Metabolic: vitamin A deficiency, vitamin B12 deficiency |
| Intracranial | Neoplasm: meningioma, neuroma Aneurysm Stroke Neurosurgery, surgical injury to the trigeminal nerve |
| Genetic | Riley-Day syndrome Goldenhar syndrome Familial corneal neuropathy |
| Instrument | Mechanism/Principle | Advantages | Disadvantages |
|---|---|---|---|
| Cochet–Bonnet aesthesiometer | Mechanical stimulus using a nylon filament with modifiable length (5 to 60 mm), being able to exert a pressure of 11 mm/g to 200 mm/g |
|
|
| Gas-based non-contact corneal aesthesiometer | Generating a controlled jet of air directed towards the corneal surface which exerts mechanical pressure on the surface while producing a cooling effect on the cornea |
|
|
| Swiss liquid-jet aesthesiometer | Liquid jet with an isotonic saline solution released from a microvalve mounted on a slit lamp with a temperature sensor |
|
|
| Brill aesthesiometer | Ambient air pulse emitted from an outlet nozzle placed 4 mm away from the corneal surface |
|
|
| Diseases | Studies | Study Design | Aesthesiometer | Study Findings |
|---|---|---|---|---|
| Type 1 diabetes | Rosenberg et al. [49] | Cross-sectional study; n = 23 | Cochet–Bonnet aesthesiometer |
|
| Type 1/type 2 diabetes | Tavakoli et al. [51] | Cross-sectional controlled study; n = 165 | Cochet–Bonnet aesthesiometer and non-contact corneal aesthesiometer |
|
| Fuchs’ endothelial dystrophy | Aggarwal et al. [50] | Prospective, cross-sectional, controlled study; n = 30 | Cochet–Bonnet aesthesiometer |
|
| Dikmetas et al. [52] | Retrospective, cross-sectional study; n = 49 | Cochet–Bonnet aesthesiometer |
| |
| Dry eye disease | Labbé et al. [53] | Cross-sectional study; n = 22 | Cochet–Bonnet aesthesiometer |
|
| Benítez-Del-Castillo et al. [44] | Prospective, cross-sectional, controlled study; n = 41 | Non-contact corneal aesthesiometer |
| |
| Glaucoma | Martone et al. [45] | Comparative retrospective study; n = 104 | Cochet–Bonnet aesthesiometer |
|
| Labbé et al. [53] | Cross-sectional study; n = 24 | Cochet–Bonnet aesthesiometer |
| |
| Keratoconus | Patel et al. [46] | Cross-sectional study; n = 58 | Non-contact corneal aesthesiometer |
|
| Herpes simplex keratitis | Hamrah et al. [47] | Prospective, cross-sectional, controlled study; n = 46 | Cochet–Bonnet aesthesiometer |
|
| Post-refractive surgery | Lee et al. [54] | Prospective, nonrandomised comparative clinical trial; n = 54 | Cochet–Bonnet aesthesiometer |
|
| Ocular graft-versus-host disease | Surico et al. [43] | Retrospective study; n = 36 | Brill aesthesiometer |
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Eio, E.; Yu, M.; Liu, C.; Lee, I.X.Y.; Wong, R.K.T.; Wong, J.H.F.; Liu, Y.-C. Evaluation of Corneal Sensitivity: Tools We Have. Diagnostics 2025, 15, 1785. https://doi.org/10.3390/diagnostics15141785
Eio E, Yu M, Liu C, Lee IXY, Wong RKT, Wong JHF, Liu Y-C. Evaluation of Corneal Sensitivity: Tools We Have. Diagnostics. 2025; 15(14):1785. https://doi.org/10.3390/diagnostics15141785
Chicago/Turabian StyleEio, Ezra, Mingyi Yu, Chang Liu, Isabelle Xin Yu Lee, Regina Kay Ting Wong, Jipson Hon Fai Wong, and Yu-Chi Liu. 2025. "Evaluation of Corneal Sensitivity: Tools We Have" Diagnostics 15, no. 14: 1785. https://doi.org/10.3390/diagnostics15141785
APA StyleEio, E., Yu, M., Liu, C., Lee, I. X. Y., Wong, R. K. T., Wong, J. H. F., & Liu, Y.-C. (2025). Evaluation of Corneal Sensitivity: Tools We Have. Diagnostics, 15(14), 1785. https://doi.org/10.3390/diagnostics15141785