
Prognostic Factors Affecting Mortality Among Patients Admitted to the Intensive Care Unit with Acute Hypoxemic Respiratory Failure

 , , , , ,
, , , , ,
Abstract
1. Introduction
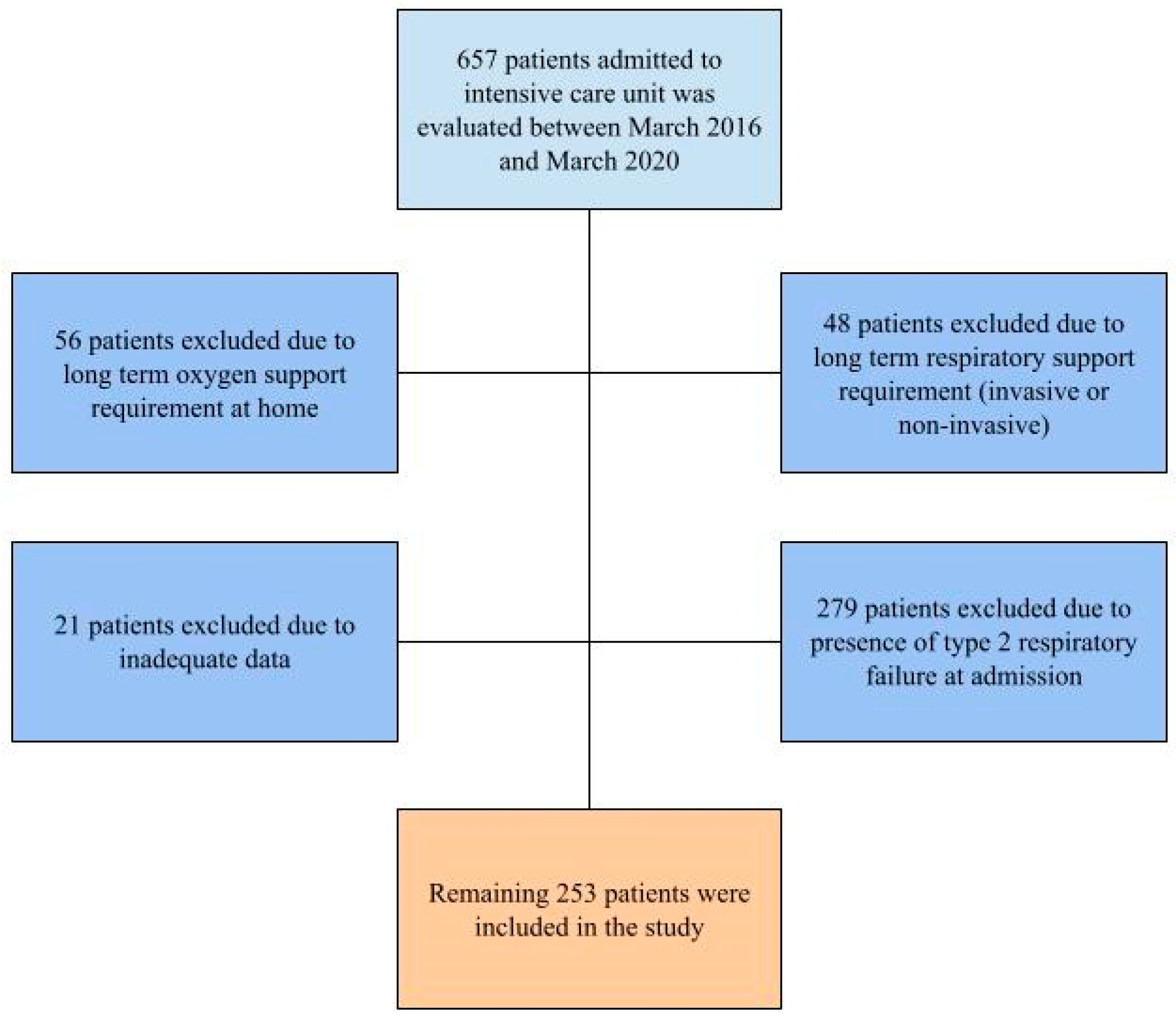
2. Materials and Methods
Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| ICU | intensive care unit |
| MV | mechanical ventilation |
| NIMV | Non-Invasive Mechanical Ventilation |
| COPD | Chronic Obstructive Pulmonary Disease |
| APACHE II | Acute Physiology and Chronic Health Evaluation II |
| SOFA | Sequential Organ Failure Assessment |
| SAPS II | Simplified Acute Physiology Score II |
| mNUTRIC | modified Nutrition Risk in the Critically Ill |
| ABG | arterial blood gas |
| CCI | Charlson Comorbidity Index |
| CRP | C-reactive protein |
| ROC | Receiver Operating Characteristic |
| AUC | area under the curve |
| ARDS | acute respiratory distress syndrome |
| COVID-19 | Coronavirus Disease 2019 |
| ECMO | Extracorporeal Membrane Oxygenation |
References
- Lamba, T.S.; Sharara, R.S.; Singh, A.C.; Balaan, M. Pathophysiology and Classification of Respiratory Failure. Crit. Care Nurs. Q. 2016, 39, 85–93. [Google Scholar] [CrossRef]
- Lagina, M.; Valley, T.S. Diagnosis and Management of Acute Respiratory Failure. Crit. Care Clin. 2024, 40, 235–253. [Google Scholar] [CrossRef]
- Summers, C.; Todd, R.S.; Vercruysse, G.A.; Moore, F.A. Acute Respiratory Failure. In Perioperative Medicine; Elsevier: Amsterdam, The Netherlands, 2022; pp. 576–586. [Google Scholar]
- Roussos, C.; Koutsoukou, A. Respiratory Failure. Eur. Respir. J. 2003, 22, 3s–14s. [Google Scholar] [CrossRef]
- Matthay, M.A.; Arabi, Y.; Arroliga, A.C.; Bernard, G.; Bersten, A.D.; Brochard, L.J.; Calfee, C.S.; Combes, A.; Daniel, B.M.; Ferguson, N.D.; et al. A New Global Definition of Acute Respiratory Distress Syndrome. Am. J. Respir. Crit. Care Med. 2024, 209, 37–47. [Google Scholar] [CrossRef]
- Lai, C.-C.; Tseng, K.-L.; Ho, C.-H.; Chiang, S.-R.; Chen, C.-M.; Chan, K.-S.; Chao, C.-M.; Hsing, S.-C.; Cheng, K.-C. Prognosis of Patients with Acute Respiratory Failure and Prolonged Intensive Care Unit Stay. J. Thorac. Dis. 2019, 11, 2051–2057. [Google Scholar] [CrossRef]
- Pearson, S.D.; Koyner, J.L.; Patel, B.K. Management of Respiratory Failure. Clin. J. Am. Soc. Nephrol. 2022, 17, 572–580. [Google Scholar] [CrossRef]
- Gadre, S.K.; Duggal, A.; Mireles-Cabodevila, E.; Krishnan, S.; Wang, X.-F.; Zell, K.; Guzman, J. Acute Respiratory Failure Requiring Mechanical Ventilation in Severe Chronic Obstructive Pulmonary Disease (COPD). Medicine 2018, 97, e0487. [Google Scholar] [CrossRef]
- Chung, Y.; Garden, F.L.; Marks, G.B.; Vedam, H. Causes of Hypercapnic Respiratory Failure and Associated In-hospital Mortality. Respirology 2023, 28, 176–182. [Google Scholar] [CrossRef]
- Miya, T.R.; Furlong-Dillard, J.M.; Sizemore, J.M.; Meert, K.L.; Dalton, H.J.; Reeder, R.W.; Bailly, D.K. Association Between Mortality and Ventilator Parameters in Children With Respiratory Failure on ECMO. Respir. Care 2023, 68, 592–601. [Google Scholar] [CrossRef]
- Bhurayanontachai, R.; Maneenil, K. Factors Influencing Development and Mortality of Acute Respiratory Failure in Hospitalized Patient with Active Pulmonary Tuberculosis: A 10-Year Retrospective Review. J. Thorac. Dis. 2016, 8, 1721–1730. [Google Scholar] [CrossRef]
- Shi, T.; Feng, L. Blood Biomarkers Associated with Acute Type II Respiratory Failure in COPD: A Meta-analysis. Clin. Respir. J. 2022, 16, 75–83. [Google Scholar] [CrossRef]
- Khilnani, G.; Banga, A.; Sharma, S. Predictors of Mortality of Patients with Acute Respiratory Failure Secondary to Chronic Obstructive Pulmonary Disease Admitted to an Intensive Care Unit: A One Year Study. BMC Pulm. Med. 2004, 4, 12. [Google Scholar] [CrossRef]
- Le Gall, J.R.; Lemeshow, S.; Saulnier, F. A New Simplified Acute Physiology Score (SAPS II) Based on a European/North American Multicenter Study. JAMA J. Am. Med. Assoc. 1993, 270, 2957–2963. [Google Scholar] [CrossRef]
- Knaus, W.A.; Draper, E.A.; Wagner, D.P.; Zimmerman, J.E. APACHE II: A Severity of Disease Classification System. Crit. Care Med. 1985, 13, 818–829. [Google Scholar] [CrossRef]
- Seymour, C.W.; Liu, V.X.; Iwashyna, T.J.; Brunkhorst, F.M.; Rea, T.D.; Scherag, A.; Rubenfeld, G.; Kahn, J.M.; Shankar-Hari, M.; Singer, M.; et al. Assessment of Clinical Criteria for Sepsis. JAMA 2016, 315, 762. [Google Scholar] [CrossRef]
- Heyland, D.K.; Dhaliwal, R.; Jiang, X.; Day, A.G. Identifying Critically Ill Patients Who Benefit the Most from Nutrition Therapy: The Development and Initial Validation of a Novel Risk Assessment Tool. Crit. Care 2011, 15, R268. [Google Scholar] [CrossRef]
- Kovacevic, P.; Meyer, F.J.; Gajic, O. Challenges, Obstacles, and Unknowns in Implementing Principles of Modern Intensive Care Medicine in Low-Resource Settings: An Insider’s Perspective. Intensive Care Med. 2024, 50, 141–143. [Google Scholar] [CrossRef]
- Kim, J.H.; Kho, B.-G.; Yoon, C.-S.; Na, Y.-O.; Lee, J.-K.; Park, H.-Y.; Kim, T.-O.; Kwon, Y.-S.; Kim, Y.-I.; Lim, S.-C.; et al. One-Year Mortality and Readmission Risks Following Hospitalization for Acute Exacerbation of Chronic Obstructive Pulmonary Disease Based on the Types of Acute Respiratory Failure: An Observational Study. Medicine 2024, 103, e38644. [Google Scholar] [CrossRef]
- Luhr, O.R.; Antonsen, K.; Karlsson, M.; Aardal, S.; Thorsteinsson, A.; Frostell, C.G.; Bonde, J. Incidence and Mortality after Acute Respiratory Failure and Acute Respiratory Distress Syndrome in Sweden, Denmark, and Iceland. Am. J. Respir. Crit. Care Med. 1999, 159, 1849–1861. [Google Scholar] [CrossRef]
- Menga, L.S.; Cese, L.D.; Bongiovanni, F.; Lombardi, G.; Michi, T.; Luciani, F.; Cicetti, M.; Timpano, J.; Ferrante, M.C.; Cesarano, M.; et al. High Failure Rate of Noninvasive Oxygenation Strategies in Critically Ill Subjects with Acute Hypoxemic Respiratory Failure Due to COVID-19. Respir. Care 2021, 66, 705–714. [Google Scholar] [CrossRef]
- Lee, H.S.; Kim, H.S.; Lee, S.H.; Lee, S.A.; Hwang, J.J.; Park, J.B.; Kim, Y.H.; Moon, H.J.; Lee, W.S. Clinical Implications of the Initial SAPS II in Veno-Arterial Extracorporeal Oxygenation. J. Thorac. Dis. 2019, 11, 68–83. [Google Scholar] [CrossRef]
- Jegal, Y.; Lee, S.-I.; Lee, K.-H.; Oh, Y.-M.; Shim, T.S.; Lim, C.-M.; Lee, S.D.; Kim, W.S.; Kim, D.-S.; Kim, W.D.; et al. The Clinical Efficacy of GOCA Scoring System in Patients with Acute Respiratory Distress Syndrome. J. Korean Med. Sci. 2008, 23, 383. [Google Scholar] [CrossRef]
- Motiejunaite, J.; Deniau, B.; Blet, A.; Gayat, E.; Mebazaa, A. Inotropes and Vasopressors Are Associated with Increased Short-Term Mortality but Not Long-Term Survival in Critically Ill Patients. Anaesth. Crit. Care Pain Med. 2022, 41, 101012. [Google Scholar] [CrossRef]
- Kulka, P.J.; Tryba, M. Inotropic Support of the Critically Ill Patient. Drugs 1993, 45, 654–667. [Google Scholar] [CrossRef]
- Singer, P.; Blaser, A.R.; Berger, M.M.; Calder, P.C.; Casaer, M.; Hiesmayr, M.; Mayer, K.; Montejo-Gonzalez, J.C.; Pichard, C.; Preiser, J.-C.; et al. ESPEN Practical and Partially Revised Guideline: Clinical Nutrition in the Intensive Care Unit. Clin. Nutr. 2023, 42, 1671–1689. [Google Scholar] [CrossRef]
- Reignier, J.; Rice, T.W.; Arabi, Y.M.; Casaer, M. Nutritional Support in the ICU. BMJ 2025, 388, e077979. [Google Scholar] [CrossRef] [PubMed]
- Al-Dorzi, H.M.; Arabi, Y.M. Nutrition Support for Critically Ill Patients. J. Parenter. Enter. Nutr. 2021, 45, S47–S59. [Google Scholar] [CrossRef]
- Mahmoodpoor, A.; Sanaie, S.; Sarfaraz, T.; Shadvar, K.; Fattahi, V.; Hamishekar, H.; Vahedian-Azimi, A.; Samim, A.; Rahimi-Bashar, F. Prognostic Values of Modified NUTRIC Score to Assess Outcomes in Critically Ill Patients Admitted to the Intensive Care Units: Prospective Observational Study. BMC Anesthesiol. 2023, 23, 131. [Google Scholar] [CrossRef]
- Wełna, M.; Adamik, B.; Kübler, A.; Goździk, W. The NUTRIC Score as a Tool to Predict Mortality and Increased Resource Utilization in Intensive Care Patients with Sepsis. Nutrients 2023, 15, 1648. [Google Scholar] [CrossRef]
- Todur, P.; Nileshwar, A.; Chaudhuri, S.; Maddani, S.S.; Rao, S.; Thejesh, S. Utility of the Modified Nutritional Risk in the Critically Ill Score as an Outcome Predictor in All-Cause Acute Respiratory Distress Syndrome and Acute Febrile Illness-Induced Acute Respiratory Distress Syndrome. J. Emerg. Trauma Shock 2022, 15, 173–179. [Google Scholar] [CrossRef]
- Kumar, N.; Kumar, A.; Kumar, A.; Pattanayak, A.; Singh, K.; Singh, P.K. NUTRIC Score as a Predictor of Outcome in COVID-19 ARDS Patients: A Retrospective Observational Study. Indian. J. Anaesth. 2021, 65, 669–675. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Parameters (n, SD) | Survivors (n = 122) | Non-Survivors (n = 131) | Total (n = 253) | p Value | |
|---|---|---|---|---|---|
| Demographics | |||||
| Gender (%) | Female | 46 (37.7) | 41 (31.29) | 87 (34.36) | 0.284 |
| Male | 76 (62.3) | 90 (68.71) | 166 (65.64) | ||
| Age (Years) | 65.85 (17.66) | 75 (11.9) | 70.59 (15.61) | 0.001 | |
| Charlson Comorbidity Index Score | 5.12 (1.86) | 7.57 (2.65) | 6.39 (2.6) | 0.001 | |
| Additional Support Requirements | |||||
| Inotropes and Vasopressors | 8 (6.55) | 73 (55.72) | 81 (32) | 0.001 | |
| Mechanical Ventilation | 117 (95.9) | 108 (82.44) | 225 (88.93) | 0.001 | |
| Admission Duration (Days) | |||||
| Intensive Care Unit | 2 (1–5) | 4 (1–7) | 3 (1–6) | 0.01 | |
| Ward | 9 (6–16) | 3 (0–11) | 7 (1–15) | 0.001 | |
| Total Admission | 13 (9–22) | 9 (4–22) | 12 (5.5–22) | 0.015 | |
| ICU Readmission (%) | 10 (8.19) | 8 (6.1) | 18 (7.1) | 0.54 | |
| Scoring Systems | |||||
| APACHE II | 19.56 (5.71) | 27.59 (8.25) | 23.72 (8.18) | 0.001 | |
| SOFA | 5.56 (1.19) | 8.72 (3.07) | 7.19 (2.84) | 0.001 | |
| SAPS II | 42.92 (11.84) | 60.56 (12.86) | 52.05 (15.19) | 0.001 | |
| mNUTRIC | 4.53 (1.72) | 6.79 (1.52) | 5.7 (1.98) | 0.001 | |
| Parameters (n, 25th–75th Percentile) | Survivors (n = 122) | Non-Survivors (n = 131) | Total (n = 253) | p Value |
|---|---|---|---|---|
| Complete Blood Count | ||||
| White Blood Cell (109/L) | 11.05 (8.7–14.5) | 10.1 (6.8–16.5) | 10.6 (7.8–14.7) | 0.672 |
| Lymphocyte (109/L) | 1.17 (0.69–1.8) | 0.7 (0.4–1.26) | 0.9 (0.5–1.79) | 0.001 |
| Neutrophil (109/L) | 7.7 (5.6–12.625) | 9.2 (6–13.6) | 8.7 (5.8–12.9) | 0.318 |
| Platelet (109/L) | 279 (194–339) | 197 (124–290.5) | 230 (153–318) | 0.001 |
| Liver Function Tests | ||||
| Total Bilirubin (mg/dL) | 0.6 (0.4–1) | 0.75 (0.5–1.4) | 0.7 (0.5–1.2) | 0.001 |
| Direct Bilirubin (mg/dL) | 0.2 (0.1–0.3) | 0.3 (0.2–0.7) | 0.2 (0.1–0.5) | 0.001 |
| Alkaline Phosphatase (IU/L) | 86 (68–115) | 89 (69–123) | 86 (68–123) | 0.705 |
| Alanine Aminotransferase (IU/L) | 18 (12–29) | 20 (15–43) | 19 (13–37) | 0.005 |
| Aspartate Transaminase (IU/L) | 24 (17–33) | 35 (23–56) | 27 (20–41.5) | 0.001 |
| Gamma-Glutamyl Transferase (IU/L) | 44 (30–64) | 44 (22–74) | 44 (26–68) | 0.644 |
| Renal Function Tests | ||||
| Creatinine (mg/dL) | 0.8 (0.7–1.2) | 1.1 (0.7–1.9) | 0.8 (0.7–1.5) | 0.001 |
| Glomerular Filtration Rate (mL/min/1.73 m2) | 83 (50–99) | 60 (31–87) | 79 (39–91) | 0.001 |
| Blood Urea Nitrogen (mg/dL) | 19 (14–38) | 42 (30–59) | 33 (17–51) | 0.001 |
| Nutritional Status and Inflammatory Markers | ||||
| C-Reactive Protein (mg/dL) | 66.5 (20.5–108.75) | 101 (39–204) | 85 (24–175.9) | 0.001 |
| Procalcitonin (ng/mL) | 0.24 (0.08–0.87) | 0.85 (0.205–8.9) | 0.39 (0.12–3.18) | 0.001 |
| Albumin (g/dL) | 3.22 (0.6) | 2.64 (0.52) | 2.92 (0.63) | 0.001 |
| Prealbumin (mg/dL) | 14 (9–16) | 7 (5–11.5) | 10 (6–14) | 0.001 |
| Predictor Parameters | Estimate | 95% Confidence Interval | Standard Error | Z Score | p Value | |
|---|---|---|---|---|---|---|
| Lower | Upper | |||||
| CCI Score | 0.12424 | −0.11256 | 0.36105 | 0.12082 | 1.0283 | 0.304 |
| SAPS II | 0.07473 | 0.02528 | 0.12418 | 0.02523 | 2.9618 | 0.003 |
| Ionotropic Support | 1.11374 | 0.01119 | 2.21629 | 0.56253 | 1.9799 | 0.048 |
| Mechanical Ventilation | −1.06962 | −2.38678 | 0.24754 | 0.67203 | −1.5916 | 0.111 |
| mNUTRIC Score | 0.36256 | 0.07218 | 0.65294 | 0.14816 | 2.4471 | 0.014 |
| Lymphocyte Count | −0.01131 | −0.4374 | 0.41477 | 0.2174 | −0.052 | 0.958 |
| Platelet Count | −0.00225 | −0.00592 | 0.00141 | 0.00187 | −1.2046 | 0.228 |
| Total Bilirubin | 0.57963 | −0.09052 | 1.24977 | 0.34192 | 1.6952 | 0.09 |
| Creatinine | −0.1594 | −0.58614 | 0.26733 | 0.21773 | −0.7321 | 0.464 |
| Albumin | −1.52366 | −2.3776 | −0.66973 | 0.43569 | −3.4971 | 0.001 |
| Intercept | −1.13633 | −5.02448 | 2.75182 | 1.98379 | −0.5728 | 0.567 |
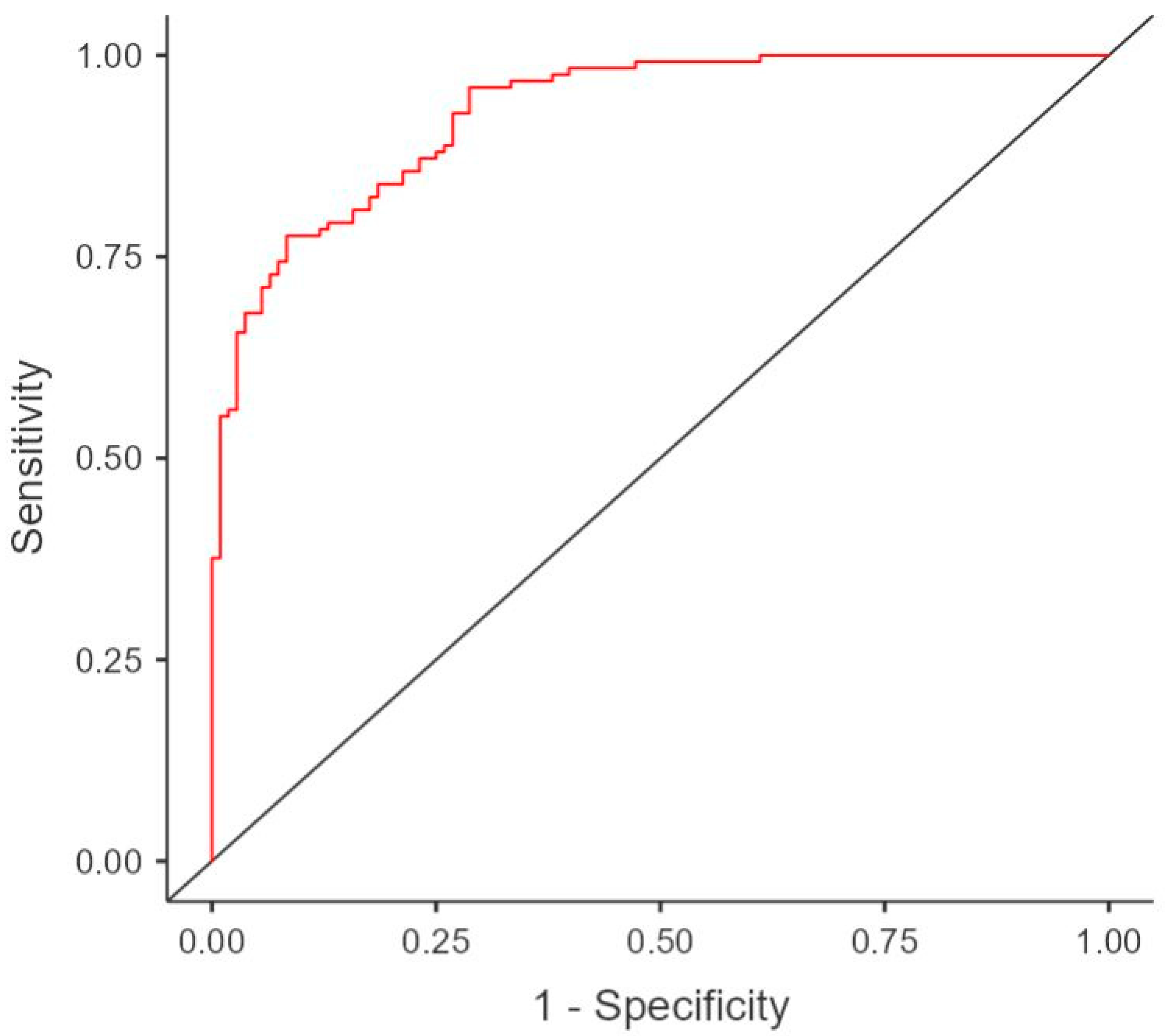
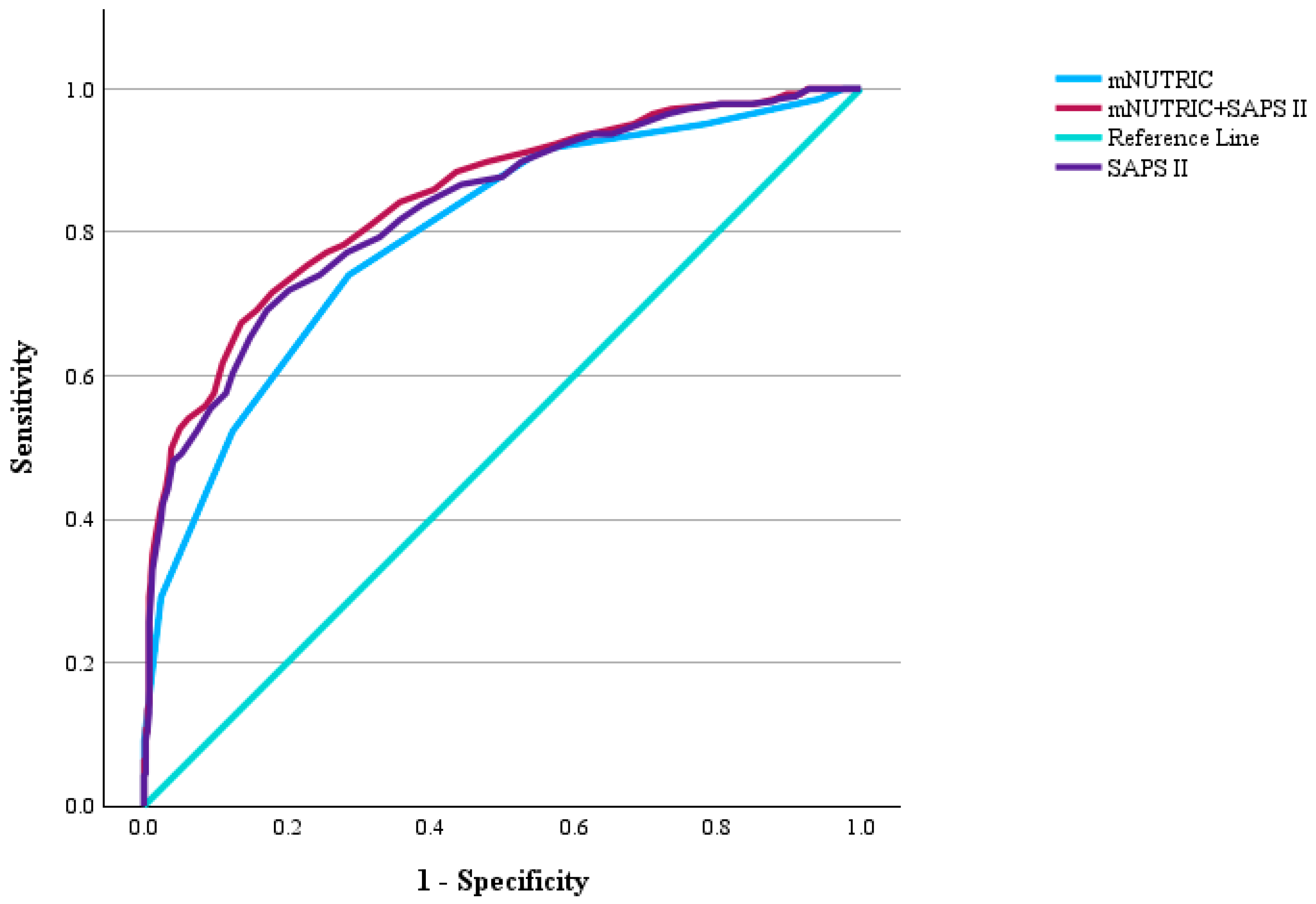
| Scoring System | AUC | 95% Confidence Interval | Standard Error | p Value | ||
|---|---|---|---|---|---|---|
| Lower | Upper | |||||
| mNUTRIC | 0.922 | 0.762 | 0.828 | 0.017 | 0.001 | |
| SAPS II | 0.975 | 0.8 | 0.862 | 0.016 | 0.001 | |
| mNUTRIC + SAPS II | 0.735 | 0.815 | 0.874 | 0.015 | 0.001 | |
| Pairwise Delong Comparison | AUC Difference | 95% Confidence Interval | Standard Score | Standard Error Difference 1 | p Value | |
| Lower | Upper | |||||
| mNUTRIC—SAPS II | −0.036 | −0.073 | 0.001 | −1.951 | 0.18 | 0.051 |
| mNUTRIC—Combined | −0.05 | 0.083 | −0.017 | −2.967 | 0.178 | 0.003 |
| SAPS II—Combined | −0.013 | −0.018 | −0.009 | −5.449 | 0.175 | 0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ensarioğlu, K.; Doğancı, M.; Cırık, M.Ö.; Ensarioğlu, M.; Tüksal, E.; Babayiğit, M.; Hazer, S. Prognostic Factors Affecting Mortality Among Patients Admitted to the Intensive Care Unit with Acute Hypoxemic Respiratory Failure. Diagnostics 2025, 15, 1784. https://doi.org/10.3390/diagnostics15141784
Ensarioğlu K, Doğancı M, Cırık MÖ, Ensarioğlu M, Tüksal E, Babayiğit M, Hazer S. Prognostic Factors Affecting Mortality Among Patients Admitted to the Intensive Care Unit with Acute Hypoxemic Respiratory Failure. Diagnostics. 2025; 15(14):1784. https://doi.org/10.3390/diagnostics15141784
Chicago/Turabian StyleEnsarioğlu, Kerem, Melek Doğancı, Mustafa Özgür Cırık, Mesher Ensarioğlu, Erbil Tüksal, Münire Babayiğit, and Seray Hazer. 2025. "Prognostic Factors Affecting Mortality Among Patients Admitted to the Intensive Care Unit with Acute Hypoxemic Respiratory Failure" Diagnostics 15, no. 14: 1784. https://doi.org/10.3390/diagnostics15141784
APA StyleEnsarioğlu, K., Doğancı, M., Cırık, M. Ö., Ensarioğlu, M., Tüksal, E., Babayiğit, M., & Hazer, S. (2025). Prognostic Factors Affecting Mortality Among Patients Admitted to the Intensive Care Unit with Acute Hypoxemic Respiratory Failure. Diagnostics, 15(14), 1784. https://doi.org/10.3390/diagnostics15141784