
In-Bore MRI-Guided Ureteral Stent Placement During Prostate Cancer Cryoablation—A Case Series

 ,
,
Abstract
1. Introduction
2. Methods
2.1. Indications for Ureteral Stent Placement During MRI-Guided Cryoablation
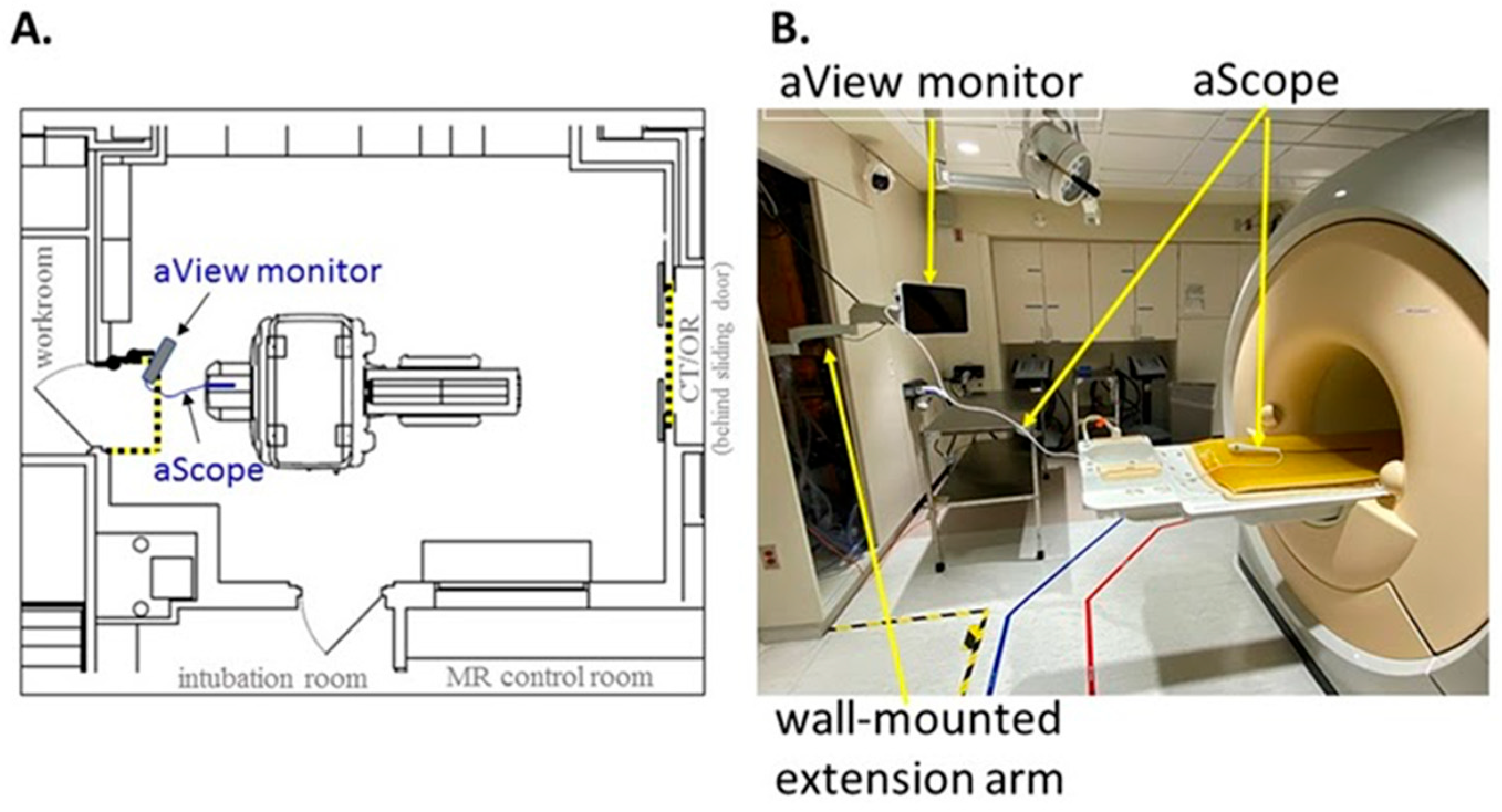
2.2. Pre-Procedural MRI Physics Safety Testing
2.3. Ureteral Stent Placement Procedure
2.4. Stent Removal
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Pansota, M.S.; Rasool, M.; Saleem, M.S.; Tabassum, S.A.; Hussain, A. Indications and complications of double J ureteral stenting: Our experience. Gomal J. Med. Sci. 2013, 11, 8–12. Available online: https://link.gale.com/apps/doc/A368422517/AONE?u=minit_train&sid=googleScholar&xid=7b42c555 (accessed on 1 July 2023).
- Zimskind, P.D.; Fetter, T.R.; Wilkerson, J.L. Clinical use of long-term indwelling silicone rubber ureteral splints inserted cystoscopically. J. Urol. 1967, 97, 840–844. [Google Scholar] [CrossRef] [PubMed]
- Luks, V.L.; Merola, J.; Arnold, B.; Ibarra, C.; Pei, K.Y. Prophylactic Ureteral Stenting in Laparoscopic Colectomy: Revisiting Traditional Practice. J. Surg. Res. 2019, 234, 161–166. [Google Scholar] [CrossRef]
- Fiuk, J.; Bao, Y.; Calleary, J.G.; Schwartz, B.F.; Denstedt, J.D. The use of internal stents in chronic ureteral obstruction. J. Urol. 2015, 193, 1092–1100. [Google Scholar] [CrossRef]
- Sedaghat, F.; Tuncali, K. Enabling Technology for MRI-Guided Intervention. Top. Magn. Reson. Imaging 2018, 27, 5–8. [Google Scholar] [CrossRef] [PubMed]
- Hushek, S.G.; Martin, A.J.; Steckner, M.; Bosak, E.; Debbins, J.; Kucharzyk, W. MR systems for MRI-guided interventions. J Magn. Reason. Imaging 2008, 27, 253–266. [Google Scholar] [CrossRef] [PubMed]
- Ehdaie, B.; Tempany, C.M.; Holland, F.; Sjoberg, D.D.; Kibel, A.S.; Trinh, Q.-D.; Durack, J.C.; Akin, O.; Vickers, A.J.; Scardino, P.T.; et al. MRI-guided focused ultrasound focal therapy for patients with intermediate-risk prostate cancer: A phase 2b, multicenter study. Lancet Oncol. 2022, 23, 910–918. [Google Scholar] [CrossRef]
- Thompson, S.; Knavel Koepsel, E.M.; Powell, G.M.; Bendel, E.C.; Bjarnason, H.; Polites, S.F.; Adamo, D.A.; Howe-Clayton, D.L.; Favazza, C.P.; Lu, A.; et al. Prospective Observational Study of Pain Severity and Pain Interference Outcomes Following Percutaneous MRI-guided Laser Ablation or Cryoablation for Focal Painful Peripheral, Soft Tissue Vascular Malformations: 12-month Outcomes. J. Vasc. Anom. 2023, 4, e055. [Google Scholar] [CrossRef]
- Woodrum, D.A.; Kawashima, A.; Karnes, R.J.; Davis, B.J.; Frank, I.; Engen, D.E.; Gorny, K.R.; Felmlee, J.P.; Callstrom, M.R.; Mynderse, L.A. Magnetic Resonance Imaging-guided Cryoablation of Recurrent Prostate Cancer After Radical Prostatectomy: Initial Single Institution Experience. Urology 2013, 82, 870–875. [Google Scholar] [CrossRef]
- Kitajima, K.; Hartman, R.P.; Froemming, A.T.; Hagen, C.E.; Takahashi, N.; Kawashima, A. Detection of Local Recurrence of Prostate Cancer After Radical Prostatectomy Using Endorectal Coil MRI at 3 T: Addition of DWI and Dynamic Contrast Enhancement to T2-Weighted MRI. Am. J. Roentgenol. 2015, 205, 807–816. [Google Scholar] [CrossRef]
- Kitajima, K.; Murphy, R.C.; Nathan, M.A.; Froemming, A.T.; Hagen, C.E.; Takahashi, N.; Kawashima, A. Detection of recurrent prostate cancer after radical prostatectomy: Comparison of 11C-choline PET/CT with pelvic multiparametric MR imaging with endorectal coil. J. Nucl. Med. 2014, 55, 223–232. [Google Scholar] [CrossRef] [PubMed]
- Kinsman, K.A.; White, M.L.; Mynderse, L.A.; Kawashima, A.; Rampton, K.; Gorny, K.R.; Atwell, T.D.; Felmlee, J.P.; Callstrom, M.R.; Woodrum, D.A. Whole-Gland Prostate Cancer Cryoablation with Magnetic Resonance Imaging Guidance: One-Year Follow-Up. Cardiovasc. Intervent. Radiol. 2018, 41, 344–349. [Google Scholar] [CrossRef] [PubMed]
- Woodrum, D.A.; Kawashima, A.; Gorny, K.R.; Mynderse, L.A. Magnetic Resonance-Guided Thermal Therapy for Localized and Recurrent Prostate Cancer. Magn. Reson. Imaging Clin. 2015, 23, 607–619. [Google Scholar] [CrossRef] [PubMed]
- Lange, D.; Bidnur, S.; Hoag, N.; Chew, B.H. Ureteral stent-associated complications-where we are and where we are going. Nat. Rev. Urol. 2015, 12, 17–25. [Google Scholar] [CrossRef]
- Dindo, D.; Demartines, N.; Clavien, P.A. Classification of surgical complications: A new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann. Surg. 2004, 240, 205–213. [Google Scholar] [CrossRef]
- Busse, H.; Kahn, T.; Moche, M. Techniques for Interventional MRI Guidance in Closed-Bore Systems. Top. Magn. Reson. Imaging. 2018, 27, 9–18. [Google Scholar] [CrossRef]
- Lomas, D.J.; Woodrum, D.A.; Mynderse, L.A. Salvage ablation for locally recurrent prostate cancer. Curr. Opin. Urol. 2021, 31, 188–193. [Google Scholar] [CrossRef]
- Woodrum, D.A.; Gorny, K.R.; Mynderse, L.A. MR-Guided Prostate Interventions. Top. Magn. Reson. Imaging 2018, 27, 141–151. [Google Scholar] [CrossRef]
- Thompson, S.M.; Gorny, K.R.; Koepsel, E.M.K.; Welch, B.T.; Mynderse, L.; Lu, A.; Favazza, C.P.; Felmlee, J.P.; Woodrum, D.A. Body Interventional MRI for Diagnostic and Interventional Radiologists: Current Practice and Future Prospects. RadioGraphics 2021, 41, 1785–1801. [Google Scholar] [CrossRef]
- Mosayyebi, A.; Manes, C.; Carugo, D.; Somani, B.K. Advances in Ureteral Stent Design and Materials. Curr. Urol. Rep. 2018, 19, 35. [Google Scholar] [CrossRef]
- Samadi, K.; Arellano, R.S. Ureteral protection during microwave ablation of renal cell carcinoma: Combined use of pyeloperfusion and hydrodissection. Diagn. Interv. Radiol. 2018, 24, 388–391. [Google Scholar] [CrossRef] [PubMed]
- Marion, J.T.; Schmitz, J.J.; Schmit, G.D.; Kurup, A.N.; Welch, B.T.; Pasternak, J.J.; Boorjian, S.A.; Leibovich, B.C.; Atwell, T.D.; Thompson, R.H. Safety and Efficacy of Retrograde Pyeloperfusion for Ureteral Protection during Renal Tumor Cryoablation. J. Vasc. Interv. Radiol. 2020, 31, 1249–1255. [Google Scholar] [CrossRef] [PubMed]
- Geavlete, P.; Georgescu, D.; Mulțescu, R.; Stanescu, F.; Cozma, C.; Geavlete, B. Ureteral stent complications—Experience on 50,000 procedures. J. Med. Life 2021, 14, 769–775. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Demographics and Disease Characteristics | |
|---|---|
| Mean Age (years) | 73.5 |
| Mean BMI (kg/m2) | 28.73 |
| Mean PSA (ng/mL) | 2.75 |
| Disease Location | |
| Left | 4/7 (57.1%) |
| Right | 3/7 (42.9%) |
| Disease Involvement | |
| Seminal Vesicle Remnant or Bed | 5/7 (71.4%) |
| Obturator Lymph Node | 1/7 (14.3%) |
| Adjacent Bladder | 1/7 (14.3%) |
| Prostate Cancer Treatment History | |
| Prostatectomy | 7/7 (100%) |
| Salvage Pelvic Lymphadenectomy | 2/7 (28.5%) |
| Adjuvant/Salvage Radiation | 5/7 (85.7%) |
| Chemotherapy | 2/7 (28.5%) |
| Androgen-Deprivation | 2/7 (28.5%) |
| Prior Ablation | 3/7 (42.9%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Whalen, S.; Woodrum, D.; Thompson, S.; Adamo, D.; Lomas, D.; Mynderse, L. In-Bore MRI-Guided Ureteral Stent Placement During Prostate Cancer Cryoablation—A Case Series. Diagnostics 2025, 15, 1781. https://doi.org/10.3390/diagnostics15141781
Whalen S, Woodrum D, Thompson S, Adamo D, Lomas D, Mynderse L. In-Bore MRI-Guided Ureteral Stent Placement During Prostate Cancer Cryoablation—A Case Series. Diagnostics. 2025; 15(14):1781. https://doi.org/10.3390/diagnostics15141781
Chicago/Turabian StyleWhalen, Sydney, David Woodrum, Scott Thompson, Dan Adamo, Derek Lomas, and Lance Mynderse. 2025. "In-Bore MRI-Guided Ureteral Stent Placement During Prostate Cancer Cryoablation—A Case Series" Diagnostics 15, no. 14: 1781. https://doi.org/10.3390/diagnostics15141781
APA StyleWhalen, S., Woodrum, D., Thompson, S., Adamo, D., Lomas, D., & Mynderse, L. (2025). In-Bore MRI-Guided Ureteral Stent Placement During Prostate Cancer Cryoablation—A Case Series. Diagnostics, 15(14), 1781. https://doi.org/10.3390/diagnostics15141781