
Reproducibility of Breech Progression Angle: Standardization of Transperineal Measurements and Development of Image-Based Checklist for Quality Control †

 , ,
, ,  , , , , , and
, , , , , and 
Abstract
Highlights
- The breech progression angle is a feasible and highly reproducible transperineal parameter when an image-based checklist is used for its evaluation.
- Image-based checklists can be useful for the standardization of transperineal ultrasound and improve reproducibility of intrapartum parameters.
- This contributes to increase diagnostic accuracy when performing an External Cephalic Version maneuver or a breech delivery.
Abstract
1. Introduction
2. Methods
2.1. Study Design and Population
2.2. Statistics
3. Results
4. Discussion
4.1. Main Findings
4.2. Comparison with Previous Studies
4.3. Strengths and Limitations
Clinical Implications
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hofmeyr, G.J.; Kulier, R.; West, H.M. External cephalic version for breech presentation at term. Cochrane Database Syst. Rev. 2015, 4. [Google Scholar] [CrossRef] [PubMed]
- No, G.G. External Cephalic Version and Reducing the Incidence of Term Breech Presentation: Green-top Guideline No. 20a. BJOG Int. J. Obstet. Gynaecol. 2017, 124, e178–e192. [Google Scholar] [CrossRef]
- Hannah, M.E.; Hannah, W.J.; Hewson, S.A.; Hodnett, E.D.; Saigal, S.; Willan, A.R. Planned caesarean section versus planned vaginal birth for breech presentation at term: A randomised multicentre trial. Lancet 2000, 356, 1375–1383. [Google Scholar] [CrossRef] [PubMed]
- Minkoff, H.; Chervenak, F.A. Elective primary cesarean delivery. N. Engl. J. Med. 2003, 348, 946–950. [Google Scholar] [CrossRef]
- Horgan, R.; Abuhamad, A. Placenta Accreta Spectrum: Prenatal Diagnosis and Management. Obstet. Gynecol. Clin. N. Am. 2022, 49, 423–438. [Google Scholar] [CrossRef]
- Devold Pay, A.; Johansen, K.; Staff, A.; Laine, K.; Blix, E.; Økland, I. Effects of external cephalic version for breech presentation at or near term in high-resource settings: A systematic review of randomized and non-randomized studies. Eur. J. Midwifery 2020, 4, 44. [Google Scholar] [CrossRef]
- Velzel, J.; De Hundt, M.; Mulder, F.M.; Molkenboer, J.F.M.; Van Der Post, J.A.M.; Mol, B.W.; Kok, M. Prediction models for successful external cephalic version: A systematic review. Eur. J. Obstet. Gynecol. Reprod. Biol. 2015, 195, 160–167. [Google Scholar] [CrossRef]
- Dupuis, O.; Ruimark, S.; Corinne, D.; Simone, T.; André, D.; René-Charles, R. Fetal head position during the second stage of labor: Comparison of digital vaginal examination and transabdominal ultrasonographic examination. Eur. J. Obstet. Gynecol. Reprod. Biol. 2005, 123, 193–197. [Google Scholar] [CrossRef]
- Sherer, D.M.; Abulafia, O. Intrapartum assessment of fetal head engagement: Comparison between transvaginal digital and transabdominal ultrasound determinations. Ultrasound Obstet. Gynecol. 2003, 21, 430–436. [Google Scholar] [CrossRef]
- Ghi, T.; Farina, A.; Pedrazzi, A.; Rizzo, N.; Pelusi, G.; Pilu, G. Diagnosis of station and rotation of the fetal head in the second stage of labor with intrapartum translabial ultrasound. Ultrasound Obstet. Gynecol. 2009, 33, 331–336. [Google Scholar] [CrossRef]
- Eggebø, T.M.; Wilhelm-Benartzi, C.; Hassan, W.A.; Usman, S.; Salvesen, K.A.; Lees, C.C. A model to predict vaginal delivery in nulliparous women based on maternal characteristics and intrapartum ultrasound. Am. J. Obstet. Gynecol. 2015, 213, e1–e362. [Google Scholar] [CrossRef] [PubMed]
- Benediktsdottir, S.; Salvesen, K.; Hjartardottir, H.; Eggebø, T.M. Reproducibility and acceptability of ultrasound measurements of head–perineum distance. Acta Obstet. Gynecol. Scand. 2018, 97, 97–103. [Google Scholar] [CrossRef]
- Lee, N.M.W.; Lau, S.L.; Yeung, Y.K.; Chiu, C.P.H.; Liu, F.; Lau, Y.Y.; Fidalgo, A.M.; Cuerva, M.J.; Aquise, A.; Nguyen-Hoang, L.; et al. Implementation of sonopartogram: Multicenter feasibility study. Ultrasound Obstet. Gynecol. 2024, 64, 214–221. [Google Scholar] [CrossRef]
- Fidalgo, A.; Miguel, R.; Fernández-Buhigas, I.; Aguado, A.; Cuerva, M.J.; Corrales, E.; Rolle, V.; Santacruz, B.; Gil, M.M.; Poon, L.C. Level of agreement between midwives and obstetricians performing ultrasound examination during labor. Int. J. Gynecol. Obstet. 2024, 164, 131–139. [Google Scholar] [CrossRef]
- Ghi, T.; Eggebø, T.; Lees, C.; Kalache, K.; Rozenberg, P.; Youssef, A.; Salomon, L.J.; Tutschek, B. ISUOG Practice Guidelines: Intrapartum ultrasound. Ultrasound Obstet. Gynecol. 2018, 52, 128–139. [Google Scholar] [CrossRef] [PubMed]
- Mlodawski, J.; Mlodawska, M.; Plusajska, J.; Detka, K.; Bialek, K.; Swiercz, G. Repeatability and Reproducibility of Potential Ultrasonographic Bishop Score Parameters. J. Clin. Med. 2023, 12, 4492. [Google Scholar] [CrossRef]
- Bamberg, C.; Scheuermann, S.; Fotopoulou, C.; Slowinski, T.; Dckelmann, A.M.; Teichgrber, U.; Streitparth, F.; Henrich, W.; Dudenhausen, J.W.; Kalache, K.D. Angle of progression measurements of fetal head at term: A systematic comparison between open magnetic resonance imaging and transperineal ultrasound. Am. J. Obstet. Gynecol. 2012, 206, 161.e1–161.e5. [Google Scholar] [CrossRef]
- Dückelmann, A.M.; Bamberg, C.; Michaelis, S.A.M.; Lange, J.; Nonnenmacher, A.; Dudenhausen, J.W.; Kalache, K.D. Measurement of fetal head descent using the “angle of progression” on transperineal ultrasound imaging is reliable regardless of fetal head station or ultrasound expertise. Ultrasound Obstet. Gynecol. 2010, 35, 216–222. [Google Scholar] [CrossRef] [PubMed]
- Tutschek, B.; Braun, T.; Chantraine, F.; Henrich, W. A study of progress of labour using intrapartum translabial ultrasound, assessing head station, direction, and angle of descent. BJOG 2011, 118, 62–69. [Google Scholar] [CrossRef]
- Molina, F.S.; Terra, R.; Carrillo, M.P.; Puertas, A.; Nicolaides, K.H. What is the most reliable ultrasound parameter for assessment of fetal head descent? Ultrasound Obstet. Gynecol. 2010, 36, 493–499. [Google Scholar] [CrossRef]
- Youssef, A.; Brunelli, E.; Fiorentini, M.; Lenzi, J.; Pilu, G.; El-Balat, A. Breech progression angle: New feasible and reliable transperineal ultrasound parameter for assessment of fetal breech descent in birth canal. Ultrasound Obstet. Gynecol. 2021, 58, 609–615. [Google Scholar] [CrossRef] [PubMed]
- Shrout, P.E.; Fleiss, J.L. Intraclass correlations: Uses in assessing rater reliability. Psychol. Bull. 1979, 86, 420–428. [Google Scholar] [CrossRef]
- Bland, J.M.; Altman, D.G. Statistical methods for assessing agreement between two methods of clinical measurement. Lancet 1986, 1, 307–310. [Google Scholar] [CrossRef]
- R Development Core Team. R: A Language and Environment for Statistical Computing. Vienna: R Foundation for Statistical Computing. 2023. Available online: http://www.r-project.org/index.html (accessed on 5 July 2025).
- Signorell, A. DescTools: Tools for Descriptive Statistics, R Package Version 0.99.48; 2023. Available online: https://cran.r-project.org/package=DescTools (accessed on 5 July 2025).
- Lehnert, B. CRAN.Package.BlandAltmanLeh, Version 0.3.1; 2015. Available online: https://cran.r-project.org/web/packages/BlandAltmanLeh/index.html (accessed on 5 July 2025).
- Lehnert, B. CRAN.Package.ICC.Sample.Size. 2015. Available online: https://cran.r-project.org/web/packages/ICC.Sample.Size/index.html (accessed on 5 July 2025).
- Wickham, H. Ggpolt2 Elegant Graphics for Data Analysis; Use R! Ser.; Springer: Berlin/Heidelberg, Germany, 2016; Volume 211. [Google Scholar]
- Sainz, J.A.; Fernández-Palacín, A.; Borrero, C.; Aquise, A.; Ramos, Z.; García-Mejido, J.A. Intra and interobserver variability of intrapartum transperineal ultrasound measurements with contraction and pushing. J. Obstet. Gynaecol. 2018, 38, 333–338. [Google Scholar] [CrossRef] [PubMed]
- Jennewein, L.; Heemann, R.; Hoock, S.C.; Hentrich, A.E.; Eichbaum, C.; Feidicker, S.; Louwen, F. Sonographic examination at the beginning of the second stage of labor predicts birth outcome in vaginally intended breech deliveries: A blinded prospective study. Arch. Gynecol. Obstet. 2024, 309, 1333–1340. [Google Scholar] [CrossRef]
- Isakov, O.; Reicher, L.; Lavie, A.; Yogev, Y.; Maslovitz, S. Prediction of success in external cephalic version for breech presentation at term. Obstet. Gynecol. 2019, 133, 857–866. [Google Scholar] [CrossRef] [PubMed]
- Haas, D.M.; Magann, E.F. External cephalic version with an amniotic fluid index ≤ 10: A systematic review. J. Matern. Neonatal Med. 2005, 18, 249–252. [Google Scholar] [CrossRef]
- Ducarme, G. Breech Presentation: CNGOF Guidelines for Clinical Practice—External Cephalic Version and other Interventions to turn Breech Babies to Cephalic Presentation. Gynecol. Obstet. Fertil. Senol. 2020, 48, 81–94. [Google Scholar] [CrossRef]
- Felemban, A.S.; Arab, K.; Algarawi, A.; Abdulghaffar, S.K.; Aljahdali, K.M.; Alotaifi, M.A.; Bafail, S.A.; Bakhudayd, T.M. Assessment of the Successful External Cephalic Version Prognostic Parameters Effect on Final Mode of Delivery. Cureus 2021, 13, e16637. [Google Scholar] [CrossRef]
- Sande, J.A.; Ioannou, C.; Sarris, I.; Ohuma, E.O.; Papageorghiou, A.T. Reproducibility of measuring amniotic fluid index and single deepest vertical pool throughout gestation. Prenat. Diagn. 2015, 35, 434–439. [Google Scholar] [CrossRef]
- Yerrabelli, R.S.; Lee, C.; Palsgaard, P.K.; Lauinger, A.R.; Abdelsalam, O.; Jennings, V. Prediction Models for Successful External Cephalic Version: An Updated Systematic Review. Am. J. Perinatol. 2024, 41, 3210–3240. [Google Scholar] [CrossRef] [PubMed]
- Sium, A.F.; Gudu, W.; Urgie, T.; Masresha, G. External cephalic version success rate and associated factors: Experience from a tertiary center in Sub-Saharan Africa: A cross-sectional study. PLoS ONE 2023, 18, e0280404. [Google Scholar] [CrossRef] [PubMed]
- Correia Costa, S.; Raposo, M.I.; Machado, A.P.; Ramalho, C.; Ayres-de-Campos, D.; Montenegro, N. External cephalic version: Predictors of success and influence on caesarean rates. Eur. J. Obstet. Gynecol. Reprod. Biol. 2021, 256, 211–214. [Google Scholar] [CrossRef]
- Pattinson, R.C.; Cuthbert, A.; Vannevel, V. Pelvimetry for fetal cephalic presentations at or near term for deciding on mode of delivery. Cochrane Database Syst. Rev. 2017, 3. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
| Score | Image Acquisition Criteria |
|---|---|
| 1 | Midsagittal plane: not seeing the posterior shadow of the pubic ramus |
| 2 | Accurately identify the whole limits of the oval-shaped symphysis (“almond” shape), not just the white hyperechogenic cartilage |
| 3 | 1st line: line along the longitudinal axis of the symphysis, dividing it into two equal parts |
| 4 | 1st line: take it to the edge of the bone |
| 5 | 2nd line: from the edge of the bone, tangentially to the lowest recognizable fetal part in the maternal pelvis |
| Site 1, operator 1 | Site 1, operator 2 | Site 2, operator 1 | Site 2, operator 2 | Site 3, operator 1 | Site 3, operator 2 | Site 4, operator 1 | Site 4, operator 2 | |
|---|---|---|---|---|---|---|---|---|
| Site 1, operator 1 | 0.89 (0.74 to 0.96) | 0.61 (−0.06 to 0.89) | 0.49 (−0.04 to 0.84) | 0.69 (−0.06 to 0.91) | 0.71 (−0.07 to 0.92) | 0.61 (0.11 to 0.84) | 0.54 (−0.09 to 0.84) | |
| Site 1, operator 2 | 0.75 (0.20 to 0.92) | 0.58 (−0.10 to 0.86) | 0.46 (−0.08 to 0.81) | 0.63 (0.10 to 0.86) | 0.69 (0.06 to 0.89) | 0.57 (0.17 to 0.81) | 0.49 (−0.03 to 0.78) | |
| Site 2, operator 1 | 0.73 (−0.06 to 0.93) | 0.87 (0.68 to 0.95) | 0.85 (0.22 to 0.96) | 0.90 (0.68 to 0.97) | 0.92 (0.39 to 0.98) | 0.63 (0.26 to 0.84) | 0.74 (0.46 to 0.89) | |
| Site 2, operator 2 | 0.75 (−0.07 to 0.94) | 0.87 (0.70 to 0.95) | 0.97 (0.93 to 0.99) | 0.73 (−0.02 to 0.92) | 0.74 (−0.07 to 0.93) | 0.57 (−0.04 to 0.84) | 0.73 (0.41 to 0.89) | |
| Site 3, operator 1 | 0.93 (0.81 to 0.97) | 0.74 (0.26 to 0.91) | 0.72 (−0.08 to 0.93) | 0.74 (−0.05 to 0.93) | 0.90 (0.77 to 0.96) | 0.66 (0.31 to 0.85) | 0.68 (0.36 to 0.86) | |
| Site 3, operator 2 | 0.77 (−0.02 to 0.94) | 0.88 (0.70 to 0.95) | 0.94 (0.85 to 0.98) | 0.94 (0.85 to 0.98) | 0.77 (0.05 to 0.93) | 0.74 (0.46 to 0.89) | 0.72 (0.42 to 0.88) | |
| Site 4, operator 1 | 0.91 (0.78 to 0.97) | 0.73 (0.37 to 0.90) | 0.76 (−0.05 to 0.94) | 0.80 (−0.003 to 0.95) | 0.88 (0.70 to 0.95) | 0.83 (0.17 to 0.95) | 0.63 (0.27 to 0.83) | |
| Site 4, operator 2 | 0.83 (0.61 to 0.93) | 0.78 (0.49 to 0.91) | 0.77 (0.16 to 0.93) | 0.78 (0.31 to 0.92) | 0.80 (0.54 to 0.92) | 0.82 (0.47 to 0.93) | 0.85 (0.64 to 0.94) |
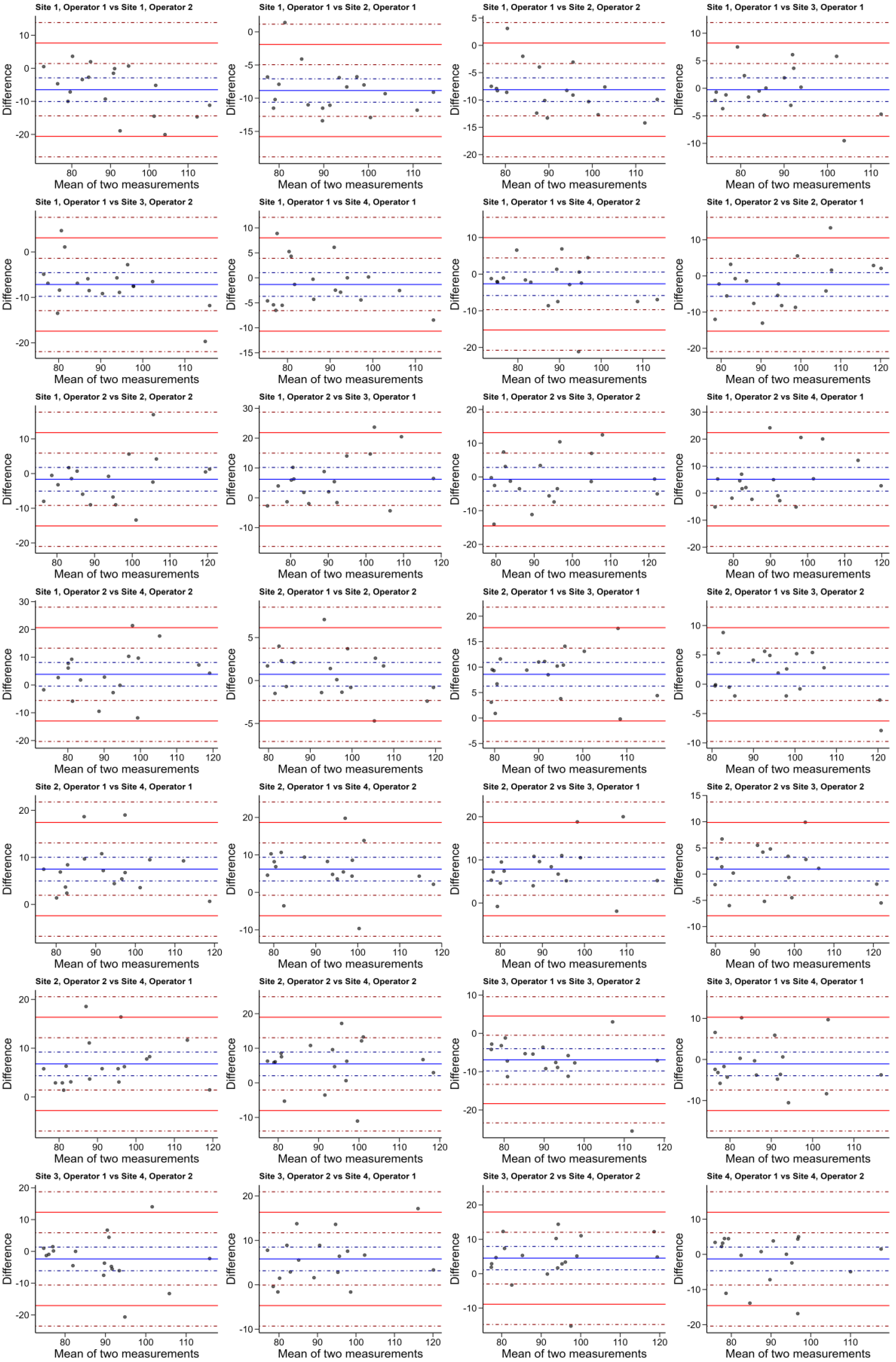
| Comparison | Mean Difference (95% CI) | Lower LoA (95% CI) | Upper LoA (95% CI) |
|---|---|---|---|
| Site 1, Operator 1 vs. Site 1, Operator 2 | −6.47 (−10.05 to −2.89) | −20.59 (−26.8 to −14.39) | 7.65 (1.44 to 13.85) |
| Site 1, Operator 1 vs. Site 2, Operator 1 | −8.84 (−10.6 to −7.08) | −15.79 (−18.84 to −12.73) | −1.9 (−4.95 to 1.15) |
| Site 1, Operator 1 vs. Site 2, Operator 2 | −8.12 (−10.28 to −5.95) | −16.66 (−20.42 to −12.91) | 0.43 (−3.33 to 4.18) |
| Site 1, Operator 1 vs. Site 3, Operator 1 | −0.26 (−2.41 to 1.89) | −8.73 (−12.45 to −5.01) | 8.21 (4.49 to 11.94) |
| Site 1, Operator 1 vs. Site 3, Operator 2 | −7.16 (−9.76 to −4.55) | −17.43 (−21.94 to −12.92) | 3.11 (−1.4 to 7.63) |
| Site 1, Operator 1 vs. Site 4, Operator 1 | −1.33 (−3.7 to 1.04) | −10.67 (−14.77 to −6.57) | 8.01 (3.9 to 12.11) |
| Site 1, Operator 1 vs. Site 4, Operator 2 | −2.63 (−5.83 to 0.56) | −15.24 (−20.77 to −9.7) | 9.97 (4.43 to 15.51) |
| Site 1, Operator 2 vs. Site 2, Operator 1 | −2.37 (−5.64 to 0.9) | −15.27 (−20.93 to −9.6) | 10.53 (4.86 to 16.19) |
| Site 1, Operator 2 vs. Site 2, Operator 2 | −1.64 (−5.06 to 1.77) | −15.09 (−21.01 to −9.18) | 11.8 (5.89 to 17.72) |
| Site 1, Operator 2 vs. Site 3, Operator 1 | 6.21 (2.24 to 10.18) | −9.43 (−16.31 to −2.56) | 21.86 (14.99 to 28.74) |
| Site 1, Operator 2 vs. Site 3, Operator 2 | −0.69 (−4.2 to 2.83) | −14.53 (−20.61 to −8.44) | 13.15 (7.07 to 19.24) |
| Site 1, Operator 2 vs. Site 4, Operator 1 | 5.14 (0.76 to 9.52) | −12.12 (−19.71 to −4.54) | 22.41 (14.82 to 29.99) |
| Site 1, Operator 2 vs. Site 4, Operator 2 | 3.84 (−0.42 to 8.1) | −12.96 (−20.34 to −5.58) | 20.64 (13.25 to 28.02) |
| Site 2, Operator 1 vs. Site 2, Operator 2 | 0.72 (−0.65 to 2.1) | −4.71 (−7.09 to −2.32) | 6.16 (3.77 to 8.54) |
| Site 2, Operator 1 vs. Site 3, Operator 1 | 8.58 (6.26 to 10.91) | −0.58 (−4.61 to 3.45) | 17.75 (13.72 to 21.77) |
| Site 2, Operator 1 vs. Site 3, Operator 2 | 1.68 (−0.33 to 3.7) | −6.27 (−9.76 to −2.77) | 9.64 (6.14 to 13.13) |
| Site 2, Operator 1 vs. Site 4, Operator 1 | 7.51 (4.99 to 10.03) | −2.41 (−6.77 to 1.95) | 17.43 (13.07 to 21.79) |
| Site 2, Operator 1 vs. Site 4, Operator 2 | 6.21 (3.05 to 9.37) | −6.25 (−11.72 to −0.77) | 18.66 (13.19 to 24.13) |
| Site 2, Operator 2 vs. Site 3, Operator 1 | 7.86 (5.12 to 10.6) | −2.95 (−7.7 to 1.8) | 18.67 (13.92 to 23.42) |
| Site 2, Operator 2 vs. Site 3, Operator 2 | 0.96 (−1.3 to 3.22) | −7.94 (−11.85 to −4.03) | 9.86 (5.95 to 13.77) |
| Site 2, Operator 2 vs. Site 4, Operator 1 | 6.79 (4.36 to 9.21) | −2.78 (−6.99 to 1.42) | 16.35 (12.15 to 20.56) |
| Site 2, Operator 2 vs. Site 4, Operator 2 | 5.48 (2.06 to 8.91) | −8.01 (−13.94 to −2.08) | 18.97 (13.04 to 24.9) |
| Site 3, Operator 1 vs. Site 3, Operator 2 | −6.9 (−9.8 to −4) | −18.34 (−23.37 to −13.31) | 4.54 (−0.49 to 9.57) |
| Site 3, Operator 1 vs. Site 4, Operator 1 | −1.07 (−3.96 to 1.81) | −12.43 (−17.43 to −7.44) | 10.29 (5.3 to 15.28) |
| Site 3, Operator 1 vs. Site 4, Operator 2 | −2.38 (−6.1 to 1.35) | −17.06 (−23.51 to −10.61) | 12.31 (5.85 to 18.76) |
| Site 3, Operator 2 vs. Site 4, Operator 1 | 5.83 (3.16 to 8.49) | −4.68 (−9.3 to −0.06) | 16.33 (11.72 to 20.95) |
| Site 3, Operator 2 vs. Site 4, Operator 2 | 4.52 (1.12 to 7.93) | −8.89 (−14.79 to −3) | 17.94 (12.04 to 23.83) |
| Site 4, Operator 1 vs. Site 4, Operator 2 | −1.3 (−4.67 to 2.06) | −14.57 (−20.4 to −8.74) | 11.96 (6.13 to 17.79) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fidalgo, A.M.; Aquise, A.; Molina, F.S.; Youssef, A.; González-Vanegas, O.; Brunelli, E.; Cataneo, I.; Segata, M.; Cuerva, M.J.; Rolle, V.; et al. Reproducibility of Breech Progression Angle: Standardization of Transperineal Measurements and Development of Image-Based Checklist for Quality Control. Diagnostics 2025, 15, 1757. https://doi.org/10.3390/diagnostics15141757
Fidalgo AM, Aquise A, Molina FS, Youssef A, González-Vanegas O, Brunelli E, Cataneo I, Segata M, Cuerva MJ, Rolle V, et al. Reproducibility of Breech Progression Angle: Standardization of Transperineal Measurements and Development of Image-Based Checklist for Quality Control. Diagnostics. 2025; 15(14):1757. https://doi.org/10.3390/diagnostics15141757
Chicago/Turabian StyleFidalgo, Ana M., Adriana Aquise, Francisca S. Molina, Aly Youssef, Otilia González-Vanegas, Elena Brunelli, Ilaria Cataneo, Maria Segata, Marcos J. Cuerva, Valeria Rolle, and et al. 2025. "Reproducibility of Breech Progression Angle: Standardization of Transperineal Measurements and Development of Image-Based Checklist for Quality Control" Diagnostics 15, no. 14: 1757. https://doi.org/10.3390/diagnostics15141757
APA StyleFidalgo, A. M., Aquise, A., Molina, F. S., Youssef, A., González-Vanegas, O., Brunelli, E., Cataneo, I., Segata, M., Cuerva, M. J., Rolle, V., & Gil, M. M. (2025). Reproducibility of Breech Progression Angle: Standardization of Transperineal Measurements and Development of Image-Based Checklist for Quality Control. Diagnostics, 15(14), 1757. https://doi.org/10.3390/diagnostics15141757