
The Prognostic Value of the EASIX Score in Patients with Metastatic Pancreatic Cancer

 , , and
, , and
Abstract
1. Introduction
2. Material and Methods
2.1. Patient Group
2.2. Data Collection
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2018. CA Cancer J. Clin. 2018, 68, 7–30. [Google Scholar] [PubMed]
- Stathis, A.; Moore, M.J. Advanced pancreatic carcinoma: Current treatment and future challenges. Nat. Rev. Clin. Oncol. 2010, 7, 163–172. [Google Scholar] [CrossRef]
- Gulturk, I.; Yilmaz, M.; Tacar, S.Y.; Bakkaloglu, O.K.; Sonmezoz, G.B.; Erdal, G.S.; Ozmen, A.; Tural, D. Naples prognostic score may predict overall survival in metastatic pancreatic cancer. J. Cancer Res. Ther. 2024, 20, 249–254. [Google Scholar] [CrossRef] [PubMed]
- Nakagawa, N.; Yamada, S.; Sonohara, F.; Takami, H.; Hayashi, M.; Kanda, M.; Kobayashi, D.; Tanaka, C.; Nakayama, G.; Koike, M.; et al. Clinical Implications of Naples Prognostic Score in Patients with Resected Pancreatic Cancer. Ann. Surg. Oncol. 2020, 27, 887–895. [Google Scholar] [CrossRef]
- Wu, D.; Wang, X.; Shi, G.; Sun, H.; Ge, G. Prognostic and clinical significance of modified glasgow prognostic score in pancreatic cancer: A meta-analysis of 4629 patients. Aging 2021, 13, 1410–1421. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.; Ren, D.; Jin, X.; Wu, H. The prognostic value of modified Glasgow Prognostic Score in pancreatic cancer: A meta-analysis. Cancer Cell Int. 2020, 20, 462. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Zhou, Y.; Wei, Q.; Fan, J.; Cheng, S.; Ding, W.; Hua, Z. Prognostic role of the neutrophil-to-lymphocyte ratio in pancreatic cancer: A meta-analysis containing 8252 patients. Clin. Chim. Acta. 2018, 479, 181–189. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Y.; Cheng, S.; Fathy, A.H.; Qian, H.; Zhao, Y. Prognostic value of platelet-to-lymphocyte ratio in pancreatic cancer: A comprehensive meta-analysis of 17 cohort studies. Onco Targets Ther. 2018, 11, 1899–1908. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Li, X.; Lin, H.; Ouyang, R.; Yang, Y.; Peng, J. Prognostic significance of the systemic immune-inflammation index in pancreatic carcinoma patients: A meta-analysis. Biosci. Rep. 2021, 41, BSR20204401. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Zhao, P.; Wu, Z.; Wang, Z.; Wu, C.; Huang, X.; Tian, B. Prognostic role of the prognostic nutritional index in patients with pancreatic cancer who underwent curative resection without preoperative neoadjuvant treatment: A systematic review and meta-analysis. Front. Surg. 2022, 9, 992641. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Sanchez-Escamilla, M.; Flynn, J.; Devlin, S.; Maloy, M.; Fatmi, S.A.; Tomas, A.A.; Escribano-Serrat, S.; Ponce, D.; Sauter, C.S.; Giralt, S.A.; et al. EASIX score predicts inferior survival after allogeneic hematopoietic cell transplantation. Bone Marrow Transplant. 2023, 58, 498–505. [Google Scholar] [CrossRef] [PubMed]
- Pedraza, A.; Salas, M.Q.; Rodríguez-Lobato, L.G.; Escribano-Serrat, S.; Suárez-Lledo, M.; Martínez-Cebrian, N.; Solano, M.T.; Arcarons, J.; Rosiñol, L.; Gutiérrez-García, G.; et al. Easix Score Correlates With Endothelial Dysfunction Biomarkers and Predicts Risk of Acute Graft-Versus-Host Disease After Allogeneic Transplantation. Transplant. Cell Ther. 2024, 30, 187.e1–187.e12. [Google Scholar] [CrossRef]
- Park, S.; Go, S.I.; Lee, G.W. The Endothelial Activation and Stress Index (EASIX) score is an independent prognostic factor in patients with diffuse large B-cell lymphoma. BMC Cancer 2022, 22, 816. [Google Scholar] [CrossRef]
- Ilic, M.; Ilic, I. Epidemiology of pancreatic cancer. World J. Gastroenterol. 2016, 22, 9694–9705. [Google Scholar] [CrossRef] [PubMed]
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef]
- Tas, F.; Sen, F.; Odabas, H.; Kılıc, L.; Keskin, S.; Yıldız, I. Performance status of patients is the major prognostic factor at all stages of pancreatic cancer. Int. J. Clin. Oncol. 2013, 18, 839–846. [Google Scholar] [CrossRef] [PubMed]
- Park, J.K.; Yoon, Y.B.; Kim, Y.T.; Ryu, J.K.; Yoon, W.J.; Lee, S.H. Survival and prognostic factors of unresectable pancreatic cancer. J. Clin. Gastroenterol. 2008, 42, 86–91. [Google Scholar] [CrossRef]
- Mai, S.; Inkielewicz-Stepniak, I. Pancreatic Cancer and Platelets Crosstalk: A Potential Biomarker and Target. Front. Cell Dev. Biol. 2021, 9, 749689. [Google Scholar] [CrossRef]
- Ghanavat, M.; Ebrahimi, M.; Rafieemehr, H.; Maniati, M.; Behzad, M.M.; Shahrabi, S. Thrombocytopenia in solid tumors: Prognostic significance. Oncol. Rev. 2019, 13, 413. [Google Scholar] [CrossRef]
- Zhang, D.X.; Dai, Y.D.; Yuan, S.X.; Tao, L. Prognostic factors in patients with pancreatic cancer. Exp. Ther. Med. 2012, 3, 423–432. [Google Scholar] [CrossRef]
- Warburg, O. On the origin of cancer cells. Science 1956, 123, 309–314. [Google Scholar] [CrossRef] [PubMed]
- Hirschhaeuser, F.; Sattler, U.G.A.; Mueller-Klieser, W. Lactate: A metabolic key player in cancer. Cancer Res. 2011, 71, 6921–6925. [Google Scholar] [PubMed]
- Tas, F.; Aykan, F.; Alici, S.; Kaytan, E.; Aydiner, A.; Topuz, E. Prognostic factors in pancreatic carcinoma: Serum LDH levels predict survival in metastatic disease. Am. J. Clin. Oncol. 2001, 24, 547–550. [Google Scholar] [CrossRef]
- Stocken, D.D.; Hassan, A.B.; Altman, D.G.; Billingham, L.J.; Bramhall, S.R.; Johnson, P.J.; Freemantle, N. Modelling prognostic factors in advanced pancreatic cancer. Br. J. Cancer 2008, 99, 883–893. [Google Scholar] [CrossRef] [PubMed]
- Haas, M.; Heinemann, V.; Kullmann, F.; Laubender, R.P.; Klose, C.; Bruns, C.J.; Holdenrieder, S.; Modest, D.P.; Schulz, C.; Boeck, S. Prognostic value of CA 19-9, CEA, CRP, LDH and bilirubin levels in locally advanced and metastatic pancreatic cancer: Results from a multicenter, pooled analysis of patients receiving palliative chemotherapy. J. Cancer Res. Clin. Oncol. 2013, 139, 681–689. [Google Scholar] [CrossRef]
- Bower, J.E.; Lamkin, D.M. Inflammation and cancer-related fatigue: Mechanisms, contributing factors, and treatment implications. Brain Behav. Immun. 2013, 30, S48–S57. [Google Scholar] [CrossRef]
- Kintzel, P.E. Anticancer drug-induced kidney disorders. Drug Saf. 2001, 24, 19–38. [Google Scholar] [CrossRef]
- Terwoord, J.D.; Beyer, A.M.; Gutterman, D.D. Endothelial dysfunction as a complication of anti-cancer therapy. Pharmacol. Ther. 2022, 237, 108116. [Google Scholar] [CrossRef]
- Palumbo, J.S. Mechanisms linking tumor cell-associated procoagulant function to tumor progression. J. Thromb. Haemost. 2009, 7 (Suppl. S1), 117–120. [Google Scholar] [CrossRef]
- Mizrahi, J.D.; Surana, R.; Valle, J.W.; Shroff, R.T. Pancreatic cancer. Lancet 2020, 395, 2008–2020. [Google Scholar]
- Burke, E.E.; Marmor, S.; Virnig, B.A.; Tuttle, T.M.; Jensen, E.H. Lymph node evaluation for pancreatic adenocarcinoma and its value as a quality metric. J. Gastrointest. Surg. 2015, 19, 2162–2170. [Google Scholar] [PubMed]
- Chun, Y.S.; Pawlik, T.M.; Vauthey, J.N. 8th Edition of the AJCC Cancer Staging Manual: Pancreas and Hepatobiliary Cancers. Ann. Surg. Oncol. 2018, 25, 845–847. [Google Scholar] [CrossRef] [PubMed]
- Riediger, H.; Keck, T.; Wellner, U.; zur Hausen, A.; Adam, U.; Hopt, U.T.; Makowiec, F. The Lymph Node Ratio Is the Strongest Prognostic Factor After Resection of Pancreatic Cancer. J. Gastrointest. Surg. 2009, 13, 1337–1344. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.; Lin, P.; Yang, M.; Liu, W.; Fu, X.; Liu, D.; Tao, L.; Huo, Y.; Zhang, J.; Hua, R.; et al. Integrated Genomic and Transcriptomic Analysis Reveals Unique Characteristics of Hepatic Metastases and Pro-Metastatic Role of Complement C1q in Pancreatic Ductal Adenocarcinoma. Genome Biol. 2021, 22, 4. [Google Scholar] [CrossRef]
- Makohon-Moore, A.P.; Zhang, M.; Reiter, J.G.; Bozic, I.; Allen, B.; Kundu, D.; Chatterjee, K.; Wong, F.; Jiao, Y.; Kohutek, Z.A.; et al. Limited Heterogeneity of Known Driver Gene Mutations Among the Metastases of Individual Patients with Pancreatic Cancer. Nat. Genet. 2017, 49, 358–366. [Google Scholar] [CrossRef]
- Hawes, R.H.; Xiong, Q.; Waxman, I.; MacFadyen, B.; Varadarajulu, S.; Catalano, M.F.; Hoffman, B.J.; Chappo, J.; Wiersema, M.J.; Kopecky, K.K.; et al. A Multispecialty Approach to the Diagnosis and Management of Pancreatic Cancer. Am. J. Gastroenterol. 2000, 95, 17–31. [Google Scholar] [CrossRef]
- Meenk, H.G.; Incrocci, L.; Kazemier, G.; van Eijck, C.H.; van der Gaast, A.; van Tienhoven, G.; van Dekken, H.; van der Sangen, M.J.; van der Schelling, G.P.; van der Hoeven, J.J.; et al. Adjuvant 5-FU Based Chemoradiotherapy for Patients Undergoing R-1/R-2 Resections for Pancreatic Cancer. Dig. Surg. 2005, 22, 321–328. [Google Scholar] [CrossRef]
- Hatfield, D.R.; Leland, F.H.; Maruyama, Y. Skeletal Metastases in Pancreatic Carcinoma: Study by Isotopic Bone Scanning. Oncology 1976, 33, 44–47. [Google Scholar] [CrossRef]
- Iguchi, H.; Yasuda, M.; Matsuo, T.; Samii, T.; Funakoshi, A. Clinical Features and Management of Pancreatic Cancer with Bone Metastases. Nippon Shokakibyo Gakkai Zasshi 2004, 101, 872–878. [Google Scholar]
- Gasiorowska, A.; Talar-Wojnarowska, R.; Kaczka, A.; Borkowska, A.; Czupryniak, L.; Małecka-Panas, E. Subclinical Inflammation and Endothelial Dysfunction in Patients with Chronic Pancreatitis and Newly Diagnosed Pancreatic Cancer. Dig. Dis. Sci. 2016, 61, 1121–1129. [Google Scholar] [CrossRef]
- Go, S.I.; Park, S.; Kang, M.H.; Kim, S.H.; Kim, Y.A.; Kim, Y.J.; Kim, H.G.; Kim, Y.H.; Lee, G.W. Endothelial Activation and Stress Index (EASIX) as a Predictive Biomarker in Small Cell Lung Cancer. Cancer Biomark. 2022, 35, 217–225. [Google Scholar] [CrossRef] [PubMed]
- Gu, J.S.; Ryu, J.W.; Yu, S.H.; Chung, H.S.; Hwang, J.E.; Bae, W.K.; Ku, J.Y.; Lee, C.H.; Ha, H.K.; Jung, S.I.; et al. Prognostic Value of the Endothelial Activation and Stress Index in Patients with Upper Tract Urothelial Cancer Undergoing Radical Nephroureterectomy. Investig. Clin. Urol. 2022, 63, 623–630. [Google Scholar] [CrossRef] [PubMed]
- Martin, S.D.; Bhuiyan, I.; Soleimani, M.; Wang, G. Biomarkers for Immune Checkpoint Inhibitors in Renal Cell Carcinoma. J. Clin. Med. 2023, 12, 4987. [Google Scholar] [CrossRef]

{kind=link}
| Min–Max | Median | Mean ± sd/n-% | ||||||
|---|---|---|---|---|---|---|---|---|
| Age (year) | 34.0 | – | 86.0 | 63.5 | 63.0 | ± | 9.4 | |
| Gender | Male | 126 | 61.8% | |||||
| Female | 78 | 38.2% | ||||||
| ECOG Score | 0 | 62 | 30.4% | |||||
| I | 119 | 58.3% | ||||||
| II | 17 | 8.3% | ||||||
| III | 6 | 2.9% | ||||||
| Lymphocyte-to-Monocyte Ratio | 0.3 | – | 13.0 | 2.8 | 3.3 | ± | 2.0 | |
| Neutrophil-to-Lymphocyte Ratio | 0.7 | – | 32.5 | 2.9 | 4.4 | ± | 4.4 | |
| White Blood Cell Count (×103/µL) | 1.0 | – | 162.3 | 7.5 | 11.4 | ± | 19.9 | |
| Hemoglobin (g/dL) | 7.2 | – | 18.7 | 12.1 | 12.0 | ± | 1.9 | |
| Platelet Count (×103/µL) | 45.0 | – | 919.0 | 263.0 | 269.2 | ± | 118.7 | |
| Urea (mg/dL) | 7.0 | – | 166.0 | 32.0 | 40.7 | ± | 26.0 | |
| Creatinine (mg/dL) | 0.26 | – | 1.78 | 0.72 | 0.79 | ± | 0.31 | |
| Lactate Dehydrogenase (U/L) | 101.0 | – | 615.0 | 213.0 | 235.5 | ± | 94.8 | |
| EASIX Score | 0.07 | – | 7.46 | 0.61 | 0.84 | ± | 0.93 | |
| Liver Metastasis | (−) | 117 | 57.4% | |||||
| (+) | 87 | 42.6% | ||||||
| Lymph Node Metastasis | (−) | 22 | 10.8% | |||||
| (+) | 182 | 89.2% | ||||||
| Bone Metastasis | (−) | 172 | 84.3% | |||||
| (+) | 32 | 15.7% | ||||||
| EASIX Score < 1.3 (n: 163) | EASIX Score ≥ 1.3 (n: 41) | p | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean ± sd/n-% | Median | Mean ± sd/n-% | Median | ||||||||
| Age | 62.8 | ± | 9.4 | 63.0 | 63.9 | ± | 9.5 | 66.0 | 0.437 | m | |
| Gender | Male | 98 | 60.1% | 28 | 68.3% | 0.336 | X2 | ||||
| Female | 65 | 39.9% | 13 | 31.7% | |||||||
| ECOG Score | 0 | 53 | 32.5% | 9 | 22.0% | 0.189 | X2 | ||||
| I | 92 | 56.4% | 27 | 65.9% | |||||||
| II | 12 | 7.4% | 5 | 12.2% | |||||||
| III | 6 | 3.7% | 0 | 0.0% | |||||||
| Lymphocyte-to-Monocyte Ratio | 3.3 | ± | 2.0 | 2.8 | 3.3 | ± | 2.0 | 2.9 | 0.936 | m | |
| Neutrophil-to-Lymphocyte Ratio | 4.3 | ± | 4.0 | 3.0 | 4.8 | ± | 5.9 | 2.7 | 0.605 | m | |
| White Blood Cell Count (×103/µL) | 12.2 | ± | 22.0 | 7.5 | 8.1 | ± | 4.4 | 7.3 | 0.454 | m | |
| Hemoglobin (g/dL) | 12.0 | ± | 1.9 | 12.0 | 12.1 | ± | 2.0 | 12.1 | 0.640 | t | |
| Platelet Count (×103/µL) | 284.4 | ± | 121.0 | 269.0 | 208.4 | ± | 86.4 | 200.0 | 0.000 | m | |
| Urea (mg/dL) | 37.6 | ± | 24.0 | 28.0 | 53.2 | ± | 29.8 | 42.0 | 0.000 | m | |
| Creatinine (mg/dL) | 0.71 | ± | 0.27 | 0.64 | 1.08 | ± | 0.30 | 1.04 | 0.000 | m | |
| Lactate Dehydrogenase (U/L) | 217.3 | ± | 84.0 | 204.0 | 307.9 | ± | 101.6 | 304.0 | 0.000 | m | |
| Liver Metastasis | (−) | 94 | 57.7% | 23 | 56.1% | 0.856 | X2 | ||||
| (+) | 69 | 42.3% | 18 | 43.9% | |||||||
| Lymph Node Metastasis | (−) | 17 | 10.4% | 5 | 12.2% | 0.745 | X2 | ||||
| (+) | 146 | 89.6% | 36 | 87.8% | |||||||
| Bone Metastasis | (−) | 138 | 84.7% | 34 | 82.9% | 0.785 | X2 | ||||
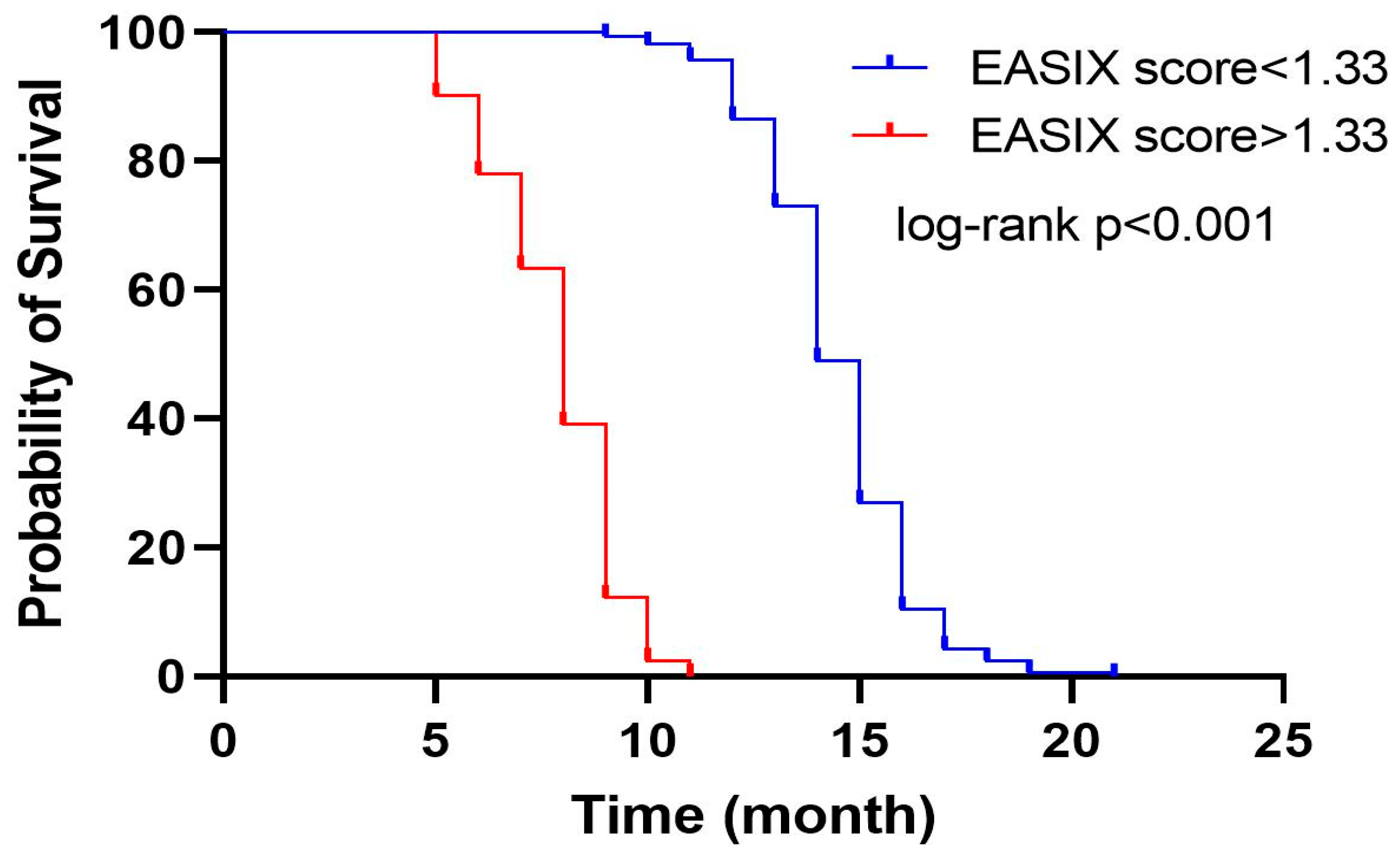
| OS (Month) Median (95%CI) | p | |
|---|---|---|
| EASIX score < 1.33 | 14 (13.66–14.33) | <0.001 |
| EASIX score > 1.33 | 8 (7.39–8.61) | |
| Overall | 14 (13.65–14.35) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cavdar, V.C.; Gokmen, Y.; Aric, M.; Altunkaya, T.; Erdem, C.G.; Gulturk, I.; Afsar, C.U. The Prognostic Value of the EASIX Score in Patients with Metastatic Pancreatic Cancer. Diagnostics 2025, 15, 1740. https://doi.org/10.3390/diagnostics15141740
Cavdar VC, Gokmen Y, Aric M, Altunkaya T, Erdem CG, Gulturk I, Afsar CU. The Prognostic Value of the EASIX Score in Patients with Metastatic Pancreatic Cancer. Diagnostics. 2025; 15(14):1740. https://doi.org/10.3390/diagnostics15141740
Chicago/Turabian StyleCavdar, Vahit Can, Yalcin Gokmen, Mert Aric, Tugba Altunkaya, Cennet Gizem Erdem, Ilkay Gulturk, and Cigdem Usul Afsar. 2025. "The Prognostic Value of the EASIX Score in Patients with Metastatic Pancreatic Cancer" Diagnostics 15, no. 14: 1740. https://doi.org/10.3390/diagnostics15141740
APA StyleCavdar, V. C., Gokmen, Y., Aric, M., Altunkaya, T., Erdem, C. G., Gulturk, I., & Afsar, C. U. (2025). The Prognostic Value of the EASIX Score in Patients with Metastatic Pancreatic Cancer. Diagnostics, 15(14), 1740. https://doi.org/10.3390/diagnostics15141740