1. Introduction
In recent years, the study of lower-limb asymmetries in athletes has gained relevance in contemporary sports medicine research, particularly regarding their association with injury occurrence [
1,
2]. Despite this growing interest, emerging evidence suggests limited predictive validity of conventional asymmetry variables for stratifying injury risk [
3], highlighting the need for novel biomarkers. Among the proposed alternatives, kinetic performance indices derived from multiplanar power profiles have emerged as a promising approach to assess sport-specific neuromuscular function [
4,
5].
The hamstring-to-quadriceps (H/Q) ratio, traditionally measured using isokinetic dynamometry [
6], has been extensively studied in soccer populations [
7]. However, this method fails to replicate the multiplanar, high-velocity demands of soccer-specific movements. These actions frequently involve rapid transitions between eccentric and concentric contractions (i.e., stretch-shortening cycles) during directional changes and ball striking [
8]. As a result, there is growing agreement that sport-specific kinetic profiling requires assessment tools that better reflect functional movement patterns under ecologically valid loading conditions.
Rotational inertial devices offer superior ecological validity by quantifying concentric and eccentric power throughout the full range of motion [
9,
10]. These devices enable high-velocity, multiplanar movements that simulate soccer-specific tasks—key mechanisms behind non-contact injuries [
11]. This is particularly relevant for eccentric lower-limb strength, which governs deceleration during sprinting and cutting maneuvers [
12]. Conventional H/Q ratios, predominantly assessed via isokinetic dynamometry, focus on concentric strength and overlook eccentric control during high-risk tasks. Rotational inertial devices uniquely provide velocity-dependent resistance, requiring precise acceleration–deceleration modulation. This may offer greater sensitivity in detecting functional asymmetries than isokinetic methods [
13]. Despite their increasing application in elite sports, standardized evaluation protocols and sport-specific normative data for flywheel metrics remain underdeveloped [
14]. Given soccer players’ specific biomechanical demands, this population represents an ideal cohort for such research. However, power indices in professional soccer players remain largely unexplored, representing a critical gap in current knowledge [
8].
Ongoing debates around injury risk prediction continue to highlight the limitations of conventional biomechanical metrics, particularly those based on isolated movement phases that neglect kinetic interdependencies across the musculoskeletal chain [
8]. Although traditional H/Q ratio thresholds offer limited predictive value for hamstring injuries, their diagnostic capacity is further compromised by their inability to detect compensatory mechanisms across the kinetic chain, including the trunk, hips, ankles, and feet [
6,
15]. For example, athletes may present normal H/Q ratios yet remain vulnerable to ACL injuries due to insufficient adductor magnus activation during deceleration—allowing excessive femoral internal rotation [
16].
Positional demands in soccer add further complexity. Wide midfielders often tolerate greater Q/Q asymmetry without increased injury risk—likely as a neuromuscular adaptation to repetitive crossing motions. In contrast, central defenders exceeding 12% asymmetry show a 4.2-fold increase in ACL injury risk due to frequent high-load pivoting under defensive pressure [
17]. Compounding these challenges, isokinetic strength assessments have demonstrated poor discriminative validity in stratifying injury risk among soccer players [
18], underscoring the need for integrative profiling frameworks that reflect sport-specific kinetic chains. Although rotational inertial devices show promise for assessing neuromuscular function under ecological conditions [
14,
19], prospective validation of their derived indices as predictive biomarkers remains necessary in elite soccer cohorts.
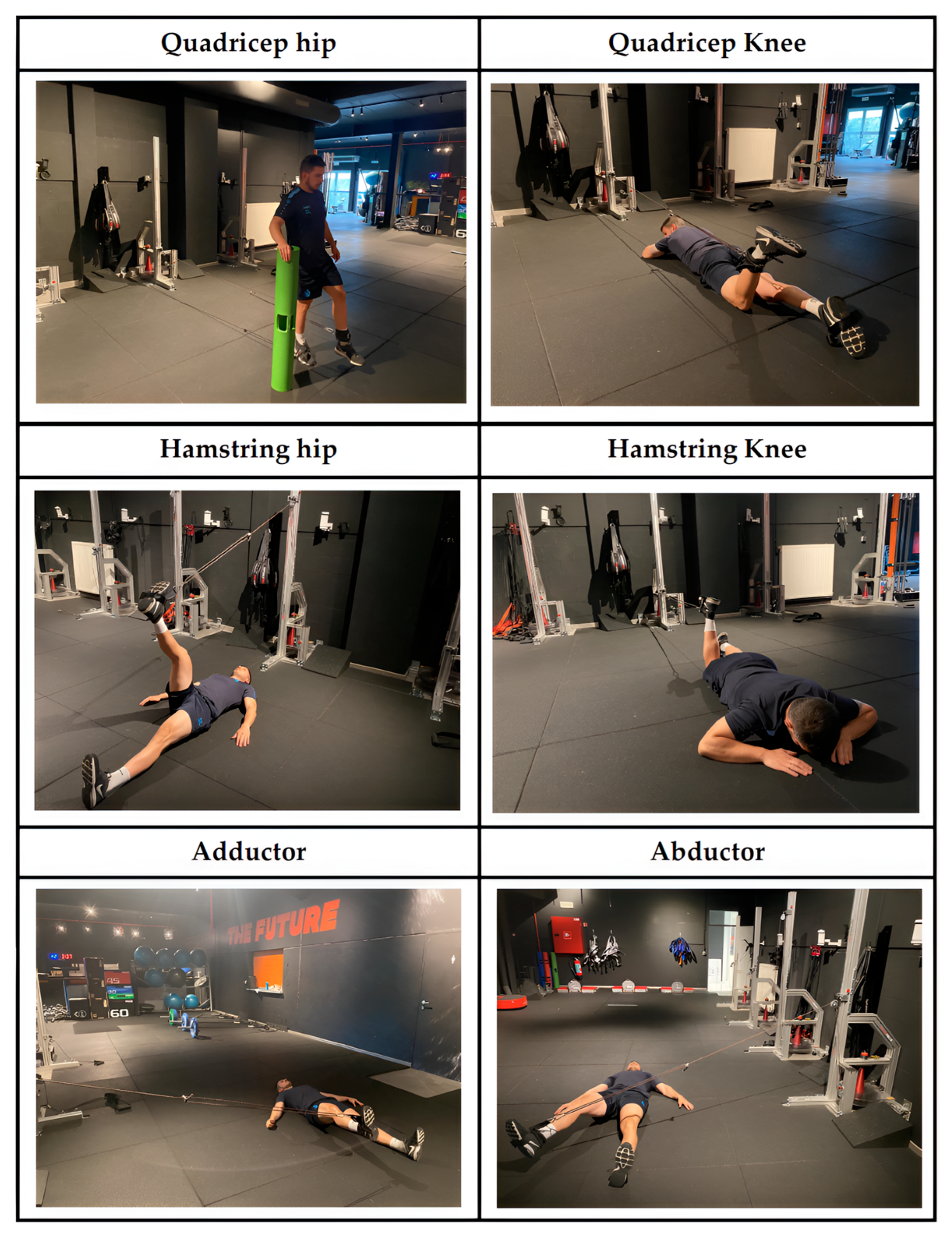
To address these gaps, this study employed a targeted monitoring protocol based on rotational inertial devices. Specifically, the study had three main aims: (1) to establish limb-specific normative values for inertial rotational devices’ power indices in professional soccer players, accounting for limb ability; (2) to map correlations between indices for each power variable; and (3) to compare power outcomes between injured and non-injured players within four months following assessment. Based on previous findings [
18,
19], we hypothesized that significant correlations would exist between exercise-specific power indices, and that these indices would differ between injured and non-injured players.
4. Discussion
The aim of this study was three-fold: (1) to establish limb-specific normative values for flywheel-derived power indices in professional soccer players, accounting for limb ability; (2) to map the intercorrelations between indices for each power variable; and (3) to compare the power outcomes related to these indices between injured and non-injured players within four months post-assessment. As a novel contribution, the study compared concentric and eccentric power indices across hip, knee, and stabilizer muscle movements. The main results revealed the following: firstly, there was no significant difference in any index between dominant and non-dominant limbs; secondly, there were moderate to large correlations between some indices across exercises; and finally, there were no differences in any power index between injured and non-injured players during the follow-up period.
4.1. Between Limbs’ Differences
The analysis of inter-limb power differences in soccer has diagnostic relevance due to the sport’s inherent biomechanical demands, which impose divergent functional roles on the lower extremities [
28]. The dominant leg predominantly executes high-velocity, precision-dependent actions such as ball striking and curved passing, while the non-dominant leg assumes a stabilizing role during weight-bearing tasks, including deceleration, pivoting, and dynamic postural control [
29]. This task-specific specialization could, in theory, lead to distinct neuromuscular adaptations, expressed as clinically relevant asymmetries in strength, in the rate of force development, or in eccentric-to-concentric force ratios [
30].
However, our results showed no statistically significant differences (
p > 0.05) in concentric or eccentric power indices between limbs in any of the tested exercises. This aligns with recent evidence suggesting that functional limb dominance does not necessarily result in mechanical asymmetry in elite soccer players. One possible explanation lies in the sport’s training context: both legs are regularly exposed to high-intensity, multidirectional loads during drills (e.g., repeated sprints, cutting maneuvers) and matches, which may promote compensatory adaptations that equalize neuromuscular performance [
31]. For example, the stabilizing role of the non-dominant leg during kicking may require eccentric hamstring strength similar to the concentric quadriceps strength of the dominant leg, ultimately balancing mechanical output between limbs [
32]. These findings provide practical implications for performance testing in soccer players. Given the absence of significant differences, they suggest that performance evaluations might be conducted using only one leg. Nonetheless, future studies should classify limbs as “strong” or “weak” to draw more definitive conclusions.
4.2. Correlations Between Power Indices
The development of diagnostically robust assessment protocols in soccer is essential to understand how power indices relate across biomechanical variables and exercise modalities, especially within time-efficient, athlete-centered testing frameworks [
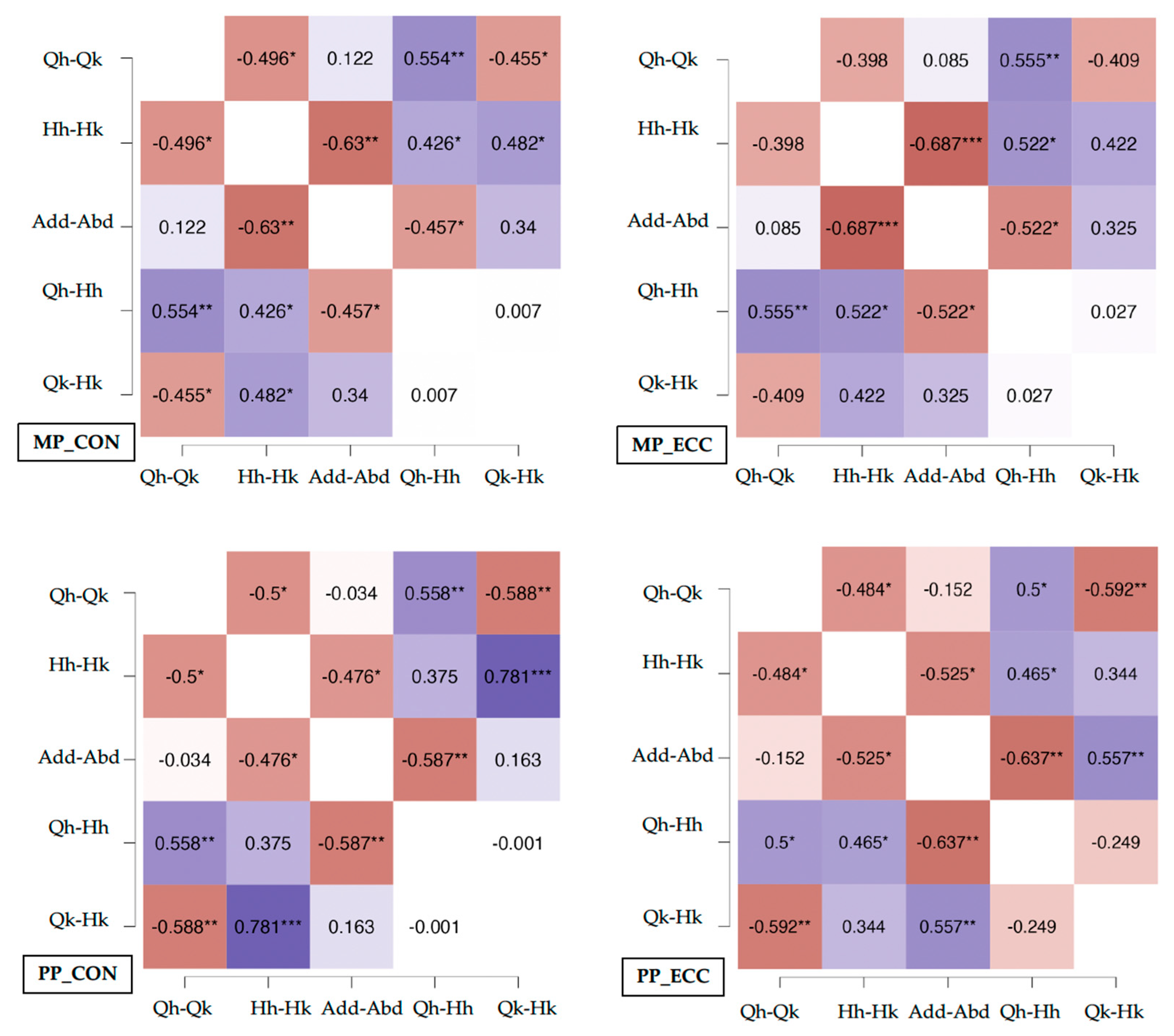
33]. Our findings reveal significant correlations between key power indices, most notably in concentric-phase quadriceps-to-hamstring ratios at the hip and knee joints (e.g., Qhip:Qknee and Hhip:Hknee ratios). These strong associations likely reflect the functional interdependence of these muscle groups during sport-specific movements such as sprint acceleration and deceleration, where coordinated hip–knee extension and flexion govern both force production (via concentric quadriceps action) and force absorption (via eccentric hamstring braking) [
34].
In contrast, weaker correlations were observed in eccentric indices and in stabilizer muscle groups (e.g., adductor/abductor ratios). This may be due to the complexity of eccentric motor control, which involves greater proprioceptive input and more variable motor unit recruitment strategies [
35]. Additionally, adductor–abductor metrics may show higher variability between sessions because these muscles primarily respond to destabilizing forces rather than being involved in maximal force production, making them less suited to standardized assessments [
36]. From a practical diagnostic standpoint, the Qhip:Qknee and Hhip:Hknee concentric ratios appear to be clinically useful biomarkers for rapid screening. These indices condense complex neuromuscular information into simple metrics, allowing practitioners to assess overall mechanical output (e.g., power decline during repeated sprints) or detect compensatory strategies (e.g., reliance on knee-dominant mechanics) without the need for exhaustive testing protocols.
4.3. Differences Between Injured and Non-Injured Players
Identifying biomechanical precursors to sports injuries requires comparing power indices between injured and non-injured athletes, as these markers may reveal subclinical deficits in neuromuscular control or load tolerance [
37]. In this study, however, no statistically significant differences (
p > 0.05) were detected between groups across any mechanical index derived from flywheel testing, including eccentric/concentric ratios, impulse, or rate of force development. This null finding underscores the multifactorial etiology of sports injuries, wherein biomechanical factors interact dynamically with extrinsic loads (e.g., training volume, competition density), intrinsic vulnerabilities (e.g., unresolved prior injuries, collagen remodeling status), and psychosocial stressors (e.g., competitive anxiety, sleep quality) [
38].
Although rotational inertial devices provide high ecological validity due to their sport-specific resistance profiles and capacity to induce eccentric overload [
8], their predictive utility for injury remains limited due to methodological constraints. The eccentric phase, despite its clinical relevance to injury mechanisms (e.g., hamstring strains during terminal swing), exhibits high intra-subject variability, likely attributable to inconsistencies in braking mechanics, proprioceptive engagement, or motor unit synchronization during rapid deceleration [
39]. Such variability can mask subtle group differences in eccentric capacity, which may only become evident under fatigue or during unanticipated movements not captured in controlled testing conditions.
These findings support a shift toward integrative diagnostic models that combine flywheel-derived data with additional biomarkers, such as tissue-specific imaging (e.g., ultrasound of muscle architecture), biochemical stress indicators (e.g., cortisol, creatine kinase), and cognitive–motor tests (e.g., reactive balance assessments). Future studies should explore longitudinal evaluations using rotational inertial devices and develop protocols that simulate chaotic mechanical demands, such as unexpected inertial load changes or reactive directional shifts.
Despite certain methodological limitations, the results of the present study provide a valuable foundation for improving the understanding of the diagnostic potential of power indices obtained using flywheel devices in professional soccer players. First, a single team was involved in the study, which could have influenced the results, mainly related to correlations, due to the sample size. However, it is difficult to obtain larger samples for similar studies with professional soccer players. Second, no force-plates were used, which could have provided relevant information during inertial device assessments [
40]. Third, the experimental design employed a single assessment session, precluding longitudinal analysis of chronic neuromuscular adaptations or transient performance fluctuations associated with cumulative fatigue. Finally, the internal and external load during the follow-up period were not analyzed, which could impact injury occurrence [
41]. Advancing the diagnostic potential of inertial-based assessments will require longitudinal designs with broader, more diverse cohorts, as well as the inclusion of contextual factors like prior injury history, positional demands, and accumulated match exposure.

 ,
, 



{kind=link}
{kind=link}