Comparison of Intensive Care Scoring Systems in Predicting Overall Mortality of Sepsis

 , , , , , , and
, , , , , , and
Abstract
1. Introduction
2. Materials and Methods
Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wang, X.; Jiao, J.; Wei, R.; Feng, Y.; Ma, X.; Li, Y.; Du, Y. A new method to predict hospital mortality in severe community acquired pneumonia. Eur. J. Intern. 2017, 40, 56–63. [Google Scholar] [CrossRef] [PubMed]
- Carmo, T.A.; Ferreira, I.B.; Menezes, R.C.; Telles, G.P.; Otero, M.L.; Arriaga, M.B.; Fukutani, K.F.; Neto, L.P.; Agareno, S.; Filho, N.M.F.; et al. Derivation and validation of a novel severity scoring system for pneumonia at intensive care unit admission. Clin. Infect. Dis. 2021, 72, 942–949. [Google Scholar] [CrossRef] [PubMed]
- Rapsang, A.G.; Shyam, D.C. Scoring systems in the intensive care unit: A compendium. Indian J. Crit. Care Med. 2014, 18, 220–228. [Google Scholar] [CrossRef] [PubMed]
- Liengswangwong, W.; Siriwannabhorn, R.; Leela-Amornsin, S.; Yuksen, C.; Sanguanwit, P.; Duangsri, C.; Kusonkhum, N.; Saelim, P. Comparison of Modified Early Warning Score (MEWS), Simplified Acute Physiology Score II (SAPS II), Sequential Organ Failure Assessment (SOFA), and Acute Physiology and Chronic Health Evaluation II (APACHE II) for early prediction of septic shock in diabetic patients in Emergency Departments. BMC Emerg. Med. 2024, 24, 161. [Google Scholar]
- Ion, R.; Kimidi, J.S.S.K.; Kalapala, C.; FNU, O.; Chandrababu, V.R.; Desireddygari, O.R.; Grigras, M.L.; Rosca, O.; Bratosin, F.; Cioca, F.; et al. Evaluating the Utility of Clinical Scores APACHE, CURB, SOFA, and NEWS2 at Admission and 5-Days after Symptom Onset in Predicting Severe COVID-19 in Patients with Diabetes. J. Pers. Med. 2024, 14, 868. [Google Scholar] [CrossRef]
- Mishra, S.; Swain, A.K.; Tharwani, S.; Kumar, D.; Meshram, S.; Shukla, A. Comparison of Four Severity Assessment Scoring Systems in Critically Ill Patients for Predicting Patient Outcomes: A Prospective Observational Study from a Single Tertiary Center in Central India. Cureus 2024, 16, e66268. [Google Scholar] [CrossRef]
- Afessa, B.; Gajic, O.; Keegan, M.T. Severity of illness and organ failure assessment in adult intensive care units. Crit. Care Clin. 2007, 23, 639–658. [Google Scholar] [CrossRef]
- Minne, L.; Abu-Hanna, A.; de Jonge, E. Evaluation of SOFA-based models for predicting mortality in the ICU: A systematic review. Crit. Care 2008, 12, 1–13. [Google Scholar] [CrossRef]
- Baldemir, R.; Doğanay, G.E.; Cirik, M.Ö.; Ülger, G.; Yurtseven, G.; Zengin, M. The relationship between acute physiology and chronic health evaluation-II, sequential organ failure assessment, Charlson comorbidity index and nutritional scores and length of intensive care unit stay of patients hospitalized in the intensive care unit due to chronic obstructive pulmonary disease. J. Health Sci. Med. 2022, 5, 1399–1404. [Google Scholar]
- Vincent, J.L.; Moreno, R.; Takala, J.; Willatts, S.; De Mendonça, A.; Bruining, H.; Reinhart, C.K.; Suter, P.; Thijs, L.G. The SOFA (Sepsis-Related Organ Failure Assessment) score to describe organ dysfunction/failure. Intensive Care Med. 1996, 22, 707–710. [Google Scholar] [CrossRef]
- Knaus, W.A.; Draper, E.A.; Wagner, D.P.; Zimmerman, J.E. APACHE II: A severity of disease classification system. Crit. Care Med. 1985, 13, 818–829. [Google Scholar] [CrossRef] [PubMed]
- Le Gall, J.R.; Lemeshow, S.; Saulnier, F. A new simplified acute physiology score (SAPS II) based on a European/North American multicenter study. JAMA J. Am. Med. Assoc. 1993, 270, 2957–2963. [Google Scholar] [CrossRef]
- Wang, L.; Zhang, Z.; Hu, T. Effectiveness of LODS, OASIS, and SAPS II to predict in-hospital mortality for intensive care patients with ST elevation myocardial infarction. Sci. Rep. 2021, 11, 23887. [Google Scholar] [CrossRef] [PubMed]
- Johnson, A.E.; Kramer, A.A.; Clifford, G.D. A new severity of illness scale using a subset of Acute Physiology And Chronic Health Evaluation data elements shows comparable predictive accuracy. Crit. Care Med. 2013, 41, 1711–1718. [Google Scholar] [CrossRef]
- Chen, Q.; Zhang, L.; Ge, S.; He, W.; Zeng, M. Prognosis predictive value of the Oxford Acute Severity of Illness Score for sepsis: A retrospective cohort study. PeerJ 2019, 7, e7083. [Google Scholar] [CrossRef]
- Qingui, C.; Wanmei, H.; Haichong, Z.; Lishan, Z.; Mian, Z. Comparison of predicitive value of SAPS II and OASIS scoring systems in ICU patients’ short-term outcomes. Chin. J. Crit. Care Intens. Care Med. 2018, 4, 159–163. [Google Scholar]
- Wang, X.; Xia, J.; Shan, Y.; Yang, Y.; Li, Y.; Sun, H. Predictive value of the Oxford Acute Severity of Illness Score in acute stroke patients with stroke-associated pneumonia. Front. Neurol. 2023, 14, 1251944. [Google Scholar] [CrossRef]
- Fan, S.; Ma, J. The value of five scoring systems in predicting the prognosis of patients with sepsis-associated acute respiratory failure. Sci. Rep. 2024, 14, 4760. [Google Scholar] [CrossRef]
- Martin, G.S.; Mannino, D.M.; Moss, M. The effect of age on the development and outcome of adult sepsis. Crit. Care Med. 2006, 34, 15–21. [Google Scholar] [CrossRef]
- Singer, M.; Deutschman, C.S.; Seymour, C.W.; Shankar-Hari, M.; Annane, D.; Bauer, M.; Bellomo, R.; Bernard, G.R.; Chiche, J.-D.; Coopersmith, C.M.; et al. The third international consensus definitions for sepsis and septic shock (Sepsis-3). Jama 2016, 315, 801–810. [Google Scholar] [CrossRef]
- Argyriou, G.; Vrettou, C.S.; Filippatos, G.; Sainis, G.; Nanas, S.; Routsi, C. Comparative evaluation of Acute Physiology and Chronic Health Evaluation II and Sequential Organ Failure Assessment scoring systems in patients admitted to the cardiac intensive care unit. J. Crit. Care 2015, 30, 752–757. [Google Scholar] [CrossRef] [PubMed]
- Park, S.K.; Chun, H.J.; Kim, D.W.; Im, T.H.; Hong, H.J.; Yi, H.J. Acute Physiology and Chronic Health Evaluation II and Simplified Acute Physiology Score II in predicting hospital mortality of neurosurgical intensive care unit patients. J. Korean Med. Sci. 2009, 24, 420–426. [Google Scholar] [CrossRef] [PubMed]
- Ari, M.; Ozyurek, B.A.; Yildiz, M.; Ozdemir, T.; Hosgun, D.; Ozdemirel, T.S.; Ensarioglu, K.; Erdogdu, M.H.; Doganay, G.E.; Doganci, M.; et al. Mean Platelet Volume-to-Platelet Count Ratio (MPR) in Acute Exacerbations of Idiopathic Pulmonary Fibrosis: A Novel Biomarker for ICU Mortality. Medicina 2025, 61, 244. [Google Scholar] [CrossRef]
- Jia, L.; Hao, L.; Li, X.; Jia, R.; Zhang, H.L. Comparing the predictive values of five scales for 4-year all-cause mortality in critically ill elderly patients with sepsis. Ann Palliat Med. 2021, 10, 2387–2397. [Google Scholar] [CrossRef] [PubMed]
- Lie, K.C.; Lau, C.Y.; Van Vinh Chau, N.; West, T.E.; Limmathurotsakul, D. Utility of SOFA score, management and outcomes of sepsis in Southeast Asia: A multinational multicenter prospective observational study. J. Intensive Care 2018, 6, 1–8. [Google Scholar] [CrossRef]
- Ferreira, F.L.; Bota, D.P.; Bross, A.; Mélot, C.; Vincent, J.L. Serial evaluation of the SOFA score to predict outcome in critically ill patients. Jama 2001, 286, 1754–1758. [Google Scholar] [CrossRef]
- Granholm, A.; Moller, M.H.; Krag, M.; Perner, A.; Hjortrup, P.B. Predictive performance of the simplified acute physiology score (SAPS) II and the initial sequential organ failure assessment (SOFA) score in acutely Ill intensive care patients: Post-hoc analyses of the SUP-ICU inception cohort study. PLoS ONE 2016, 11, e168948. [Google Scholar] [CrossRef]
- Ari, M.; Haykir Solay, A.; Ozdemir, T.; Yildiz, M.; Mentes, O.; Tuten, O.F.; Tetik Manav, H.; Celik, D.; Doganci, M.; Eraslan Doganay, G.; et al. Neutrophil Percentage-to-Albumin Ratio as a Prognostic Marker in Pneumonia Patients Aged 80 and Above in Intensive Care. J. Clin. Med. 2025, 14, 3033. [Google Scholar] [CrossRef]
- Wang, N.; Wang, M.; Jiang, L.; Du, B.; Zhu, B.; Xi, X. The predictive value of the Oxford Acute Severity of Illness Score for clinical outcomes in patients with acute kidney injury. Ren. Fail. 2022, 44, 320–328. [Google Scholar] [CrossRef]
- Moreno-Torres, V.; Royuela, A.; Múñez, E.; Ortega, A.; Gutierrez, Á.; Mills, P.; Ramos-Martínez, A. Better prognostic ability of NEWS2, SOFA and SAPS-II in septic patients. Med. Clínica (Engl. Ed.) 2022, 159, 224–229. [Google Scholar] [CrossRef]
- Zhu, Y.; Zhang, R.; Ye, X.; Liu, H.; Wei, J. SAPS III is superior to SOFA for predicting 28-day mortality in sepsis patients based on Sepsis 3.0 criteria. Int. J. Infect. Dis. 2022, 114, 135–141. [Google Scholar] [CrossRef] [PubMed]
- Huang, W.C.; Xie, H.J.; Fan, H.T.; Yan, M.H.; Hong, Y.C. Comparison of prognosis predictive value of 4 disease severity scoring systems in patients with acute respiratory failure in intensive care unit: A STROBE report. Medicine 2021, 100, e27380. [Google Scholar] [CrossRef] [PubMed]
- Doganay, G.E.; Cirik, M.O. Determinants of prognosis in geriatric patients followed in respiratory ICU; either infection or malnutrition. Medicine 2021, 100, e27159. [Google Scholar] [CrossRef] [PubMed]
- Kao, K.-C.; Hsieh, M.-J.; Lin, S.-W.; Chuang, L.-P.; Chang, C.-H.; Hu, H.-C.; Wang, C.-H.; Li, L.-F.; Huang, C.-C.; Wu, H.-P. Survival predictors in elderly patients with acute respiratory distress syndrome: A prospective observational cohort study. Sci. Rep. 2018, 8, 13459. [Google Scholar] [CrossRef]
- Hu, C.; Hu, B.; Li, Z.; Yang, X.; Song, H.; Li, J. Comparison of four scoring systems for predicting ICU mortality in patients with sepsis. Nan Fang Yi Ke Da Xue Xue Bao = J. South. Med. Univ. 2020, 40, 513–518. [Google Scholar]
- Zhu, S.; Chen, H.; Li, X.; Gulifeire, T.; Wang, Y.; Yang, C.; Yu, X. Predictive value of six critical illness scores for 28-day death risk in comprehensive and specialized intensive care unit patients based on MIMIC-IV database. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue 2022, 34, 752–758. [Google Scholar]

{kind=link}
| Parameters (n, %) | Patients (n = 165) | |
|---|---|---|
| Gender | Male (%) | 110 (66.7) |
| Female (%) | 55 (33.3) | |
| Age (years, SD) | 70.38 (±15.85) | |
| Charlson Comorbidity Index (SD) | 6.88(±2.66) | |
| Hospital Admission Days | 12 (6–22) | |
| ICU Admission Days | 3 (1–6) | |
| Days on Mechanical Ventilation | 1 (0–5) | |
| Inotropic Support Requirement (%) | 71 (43) | |
| White Blood Cell (109/L) | 13.0 (7.9–19.7) | |
| Neutrophile (109/L) | 10.5 (5.6–15.8) | |
| Neutrophile (%, SD) | 83.8 (±16.25) | |
| Procalcitonin (ng/mL) | 4.9 (2.9–13.9) | |
| C-Reactive Protein (mg/L) | 15.6 (8.2–23.9) | |
| Mortality Scoring and Overall Mortality | ||
| APACHE II | 26.17 (±7.96) | |
| SOFA | 8.0 (±3.0) | |
| SAPS II | 56.73 (±14.53) | |
| OASIS | 34.38 (±10.0) | |
| 28-day Mortality (%) | 105 (63.6) | |
| Independent Samples t-Test | t | dF | p | 95% CI of the Difference | |
|---|---|---|---|---|---|
| Lower | Higher | ||||
| Gender | 2.015 | 112 | 0.046 * | 0.003 | 0.312 |
| Age (years) | −4.590 | 86 | 0.001 * | −17.675 | −6.992 |
| Charlson Comorbidity Index | −9.327 | 155 | 0.001 * | −3.716 | −2.417 |
| Hospital Admission Days | 3.950 | 94 | 0.001 * | 4.436 | 13.402 |
| ICU Admission Days | −2.270 | 160 | 0.025 * | −4.488 | −0.312 |
| Days on Mechanical Ventilation | −3.495 | 161 | 0.001 * | −6.104 | −1.696 |
| Inotropic Support Requirement | −8.428 | 161 | 0.001 | −0.641 | −0.397 |
| White Blood Cell (109/L) | −0.337 | 156 | 0.737 | −4.338 | 3.075 |
| Neutrophile (109/L) | −1.221 | 148 | 0.224 | −5.276 | 1.246 |
| Neutrophile (%) | −1.762 | 163 | 0.080 | −9.768 | 0.556 |
| Procalcitonin | −1.732 | 163 | 0.085 | −12.387 | 0.809 |
| C-Reactive Protein | 0.475 | 163 | 0.636 | −4.026 | 6.576 |
| APACHE II | −8.777 | 162 | 0.001 * | −10.401 | −6.580 |
| SOFA | −10.512 | 155 | 0.001 * | −4.231 | −2.893 |
| SAPS II | −10.637 | 163 | 0.001 * | −22.854 | −15.698 |
| OASIS | −10.553 | 163 | 0.001 * | −15.780 | −10.806 |
| Parameters | Pearson Correlation | APACHE II | SOFA | SAPS II | OASIS |
|---|---|---|---|---|---|
| Gender | Correlation | −0.106 | −0.178 a | −0.149 | −0.018 |
| p-value | 0.176 | 0.022 * | 0.057 | 0.823 | |
| Age | Correlation | 0.102 | 0.145 | 0.430 b | 0.360 b |
| p-value | 0.194 | 0.063 | 0.001 * | 0.001 * | |
| Charlson Comorbidity Index | Correlation | 0.340 b | 0.370 b | 0.613 b | 0.470 b |
| p-value | 0.001 * | 0.001 * | 0.001 * | 0.001 * | |
| Hospital Admission Days | Correlation | −0.169 a | −0.245 b | −0.226 b | −0.138 |
| p-value | 0.030 * | 0.002 * | 0.003 * | 0.077 | |
| ICU Admission Days | Correlation | −0.071 | −0.078 | 0.085 | 0.271 b |
| p-value | 0.365 | 0.320 | 0.280 | 0.001 * | |
| Days on Mechanical Ventilation | Correlation | 0.020 | 0.059 | 0.139 | 0.339 b |
| p-value | 0.796 | 0.454 | 0.076 | 0.001 * | |
| 28-day Mortality | Correlation | 0.515 b | 0.564 b | 0.640 b | 0.637 b |
| p-value | 0.001 * | 0.001 * | 0.001 * | 0.001 * |
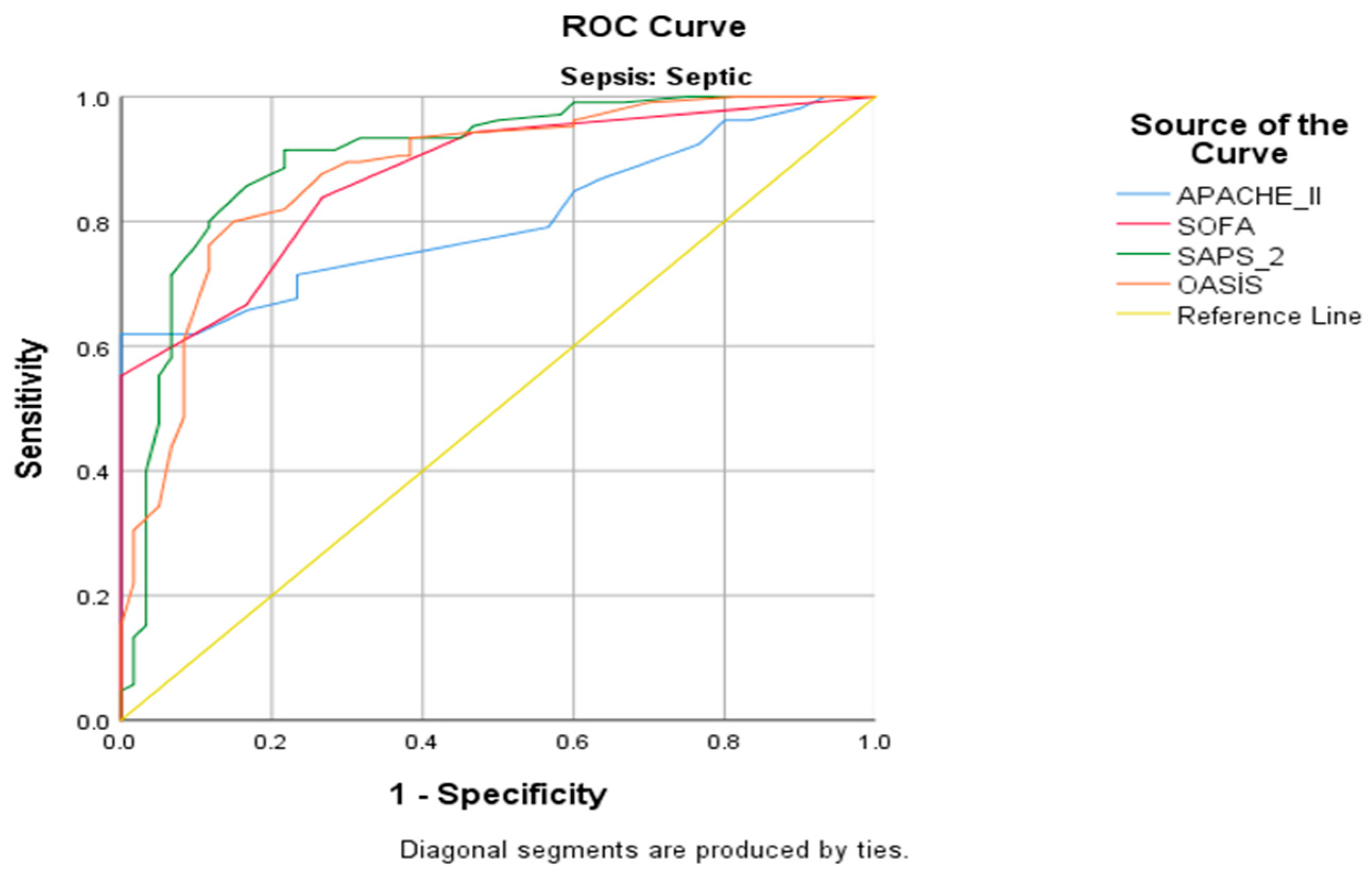
| Area Under Curve | Standard Error | p | %95 Confidence Interval | ||
|---|---|---|---|---|---|
| Lower Bound | Upper Bound | ||||
| APACHE II | 0.803 | 0.033 | 0.001 * | 0.738 | 0.868 |
| SOFA | 0.873 | 0.027 | 0.001 * | 0.821 | 0.925 |
| SAPS II | 0.902 | 0.027 | 0.001 * | 0.849 | 0.955 |
| OASIS | 0.879 | 0.028 | 0.001* | 0.823 | 0.935 |
| Test Pairs | AUC Difference | 95% Confidence Interval | Standard Score | Standard Error Difference 1 | p-Value | |
|---|---|---|---|---|---|---|
| Lower | Upper | |||||
| APACHE II—SOFA | −0.070 | −0.131 | −0.009 | −2.251 | 0.242 | 0.024 * |
| APACHE II—SAPS II | −0.099 | −0.176 | −0.023 | −2.557 | 0.245 | 0.011 * |
| APACHE II—OASIS | −0.076 | −0.152 | 0.000 | −1.957 | 0.247 | 0.049 * |
| SOFA—SAPS II | −0.030 | −0.092 | 0.033 | −0.921 | 0.230 | 0.357 |
| SOFA—OASIS | −0.006 | −0.066 | 0.054 | −0.200 | 0.233 | 0.841 |
| SAPS II—OASIS | 0.023 | −0.027 | 0.074 | 0.908 | 0.234 | 0.364 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cirik, M.O.; Doganay, G.E.; Doganci, M.; Ozdemir, T.; Yildiz, M.; Kahraman, A.; Hazer, S.; Tunc, M.; Ensarioglu, K.; Ozanbarci, A.; et al. Comparison of Intensive Care Scoring Systems in Predicting Overall Mortality of Sepsis. Diagnostics 2025, 15, 1660. https://doi.org/10.3390/diagnostics15131660
Cirik MO, Doganay GE, Doganci M, Ozdemir T, Yildiz M, Kahraman A, Hazer S, Tunc M, Ensarioglu K, Ozanbarci A, et al. Comparison of Intensive Care Scoring Systems in Predicting Overall Mortality of Sepsis. Diagnostics. 2025; 15(13):1660. https://doi.org/10.3390/diagnostics15131660
Chicago/Turabian StyleCirik, Mustafa Ozgur, Guler Eraslan Doganay, Melek Doganci, Tarkan Ozdemir, Murat Yildiz, Abdullah Kahraman, Seray Hazer, Mehtap Tunc, Kerem Ensarioglu, Azra Ozanbarci, and et al. 2025. "Comparison of Intensive Care Scoring Systems in Predicting Overall Mortality of Sepsis" Diagnostics 15, no. 13: 1660. https://doi.org/10.3390/diagnostics15131660
APA StyleCirik, M. O., Doganay, G. E., Doganci, M., Ozdemir, T., Yildiz, M., Kahraman, A., Hazer, S., Tunc, M., Ensarioglu, K., Ozanbarci, A., & Mentes, O. (2025). Comparison of Intensive Care Scoring Systems in Predicting Overall Mortality of Sepsis. Diagnostics, 15(13), 1660. https://doi.org/10.3390/diagnostics15131660