
Radiographic and Histopathological Characteristics of Chronic Nonbacterial Osteomyelitis of the Mandible in Pediatric Patients: Case Series

 , , , , , , and
, , , , , , and
Abstract
1. Introduction
2. Case Presentation
2.1. Case 1
2.1.1. History and Clinical Examination
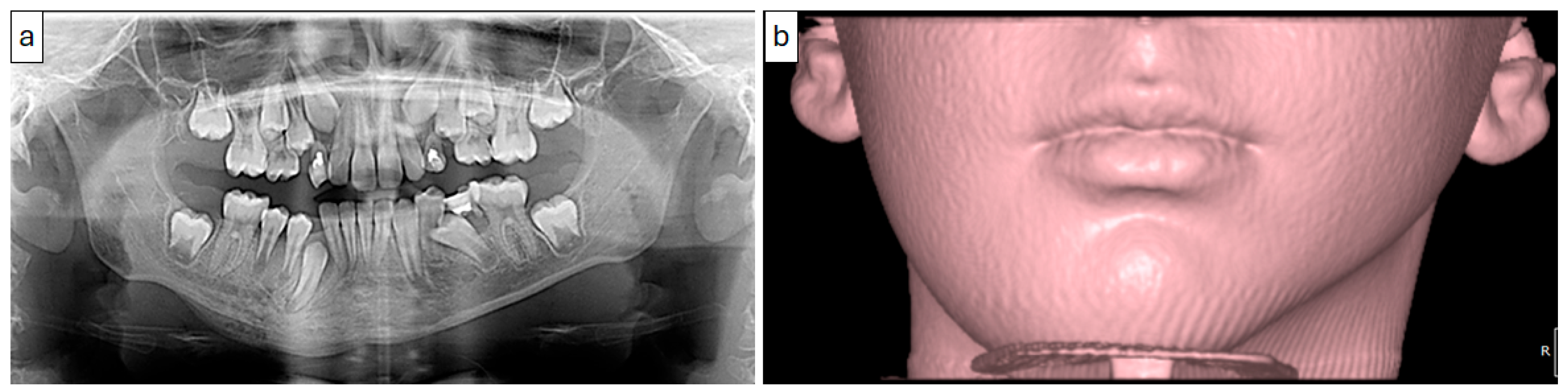
2.1.2. Radiographic Examination
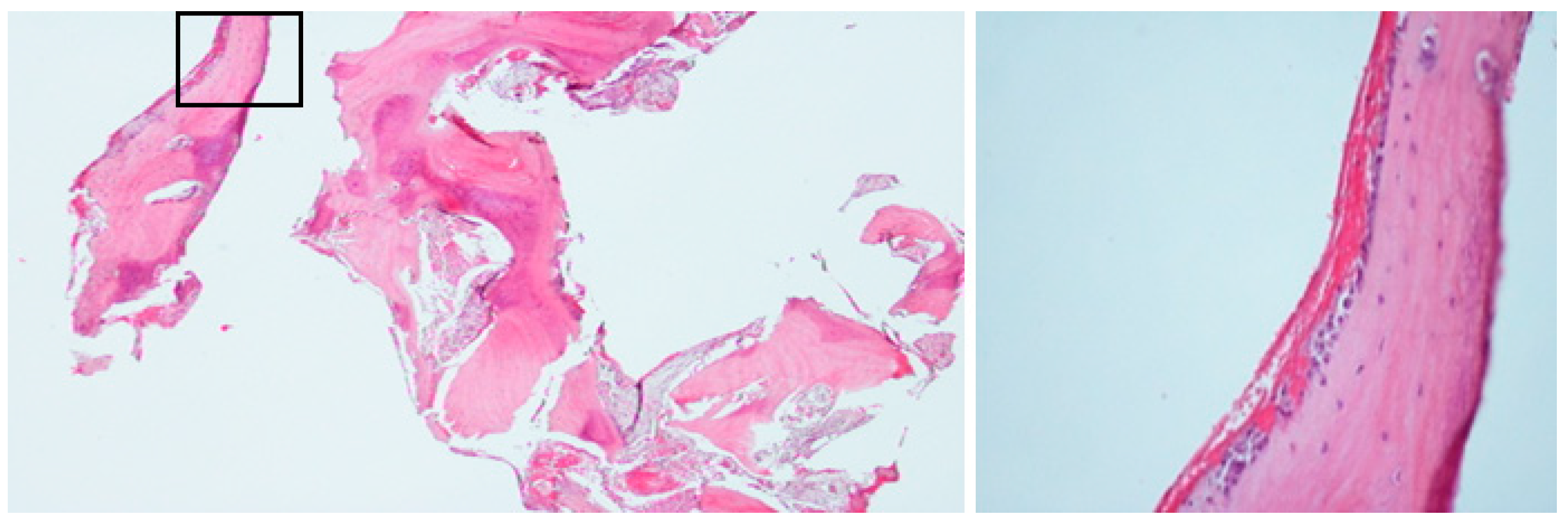
2.1.3. Histopathological Examination
2.1.4. Case Management and Differential Diagnosis
2.2. Case 2
2.2.1. History and Clinical Examination
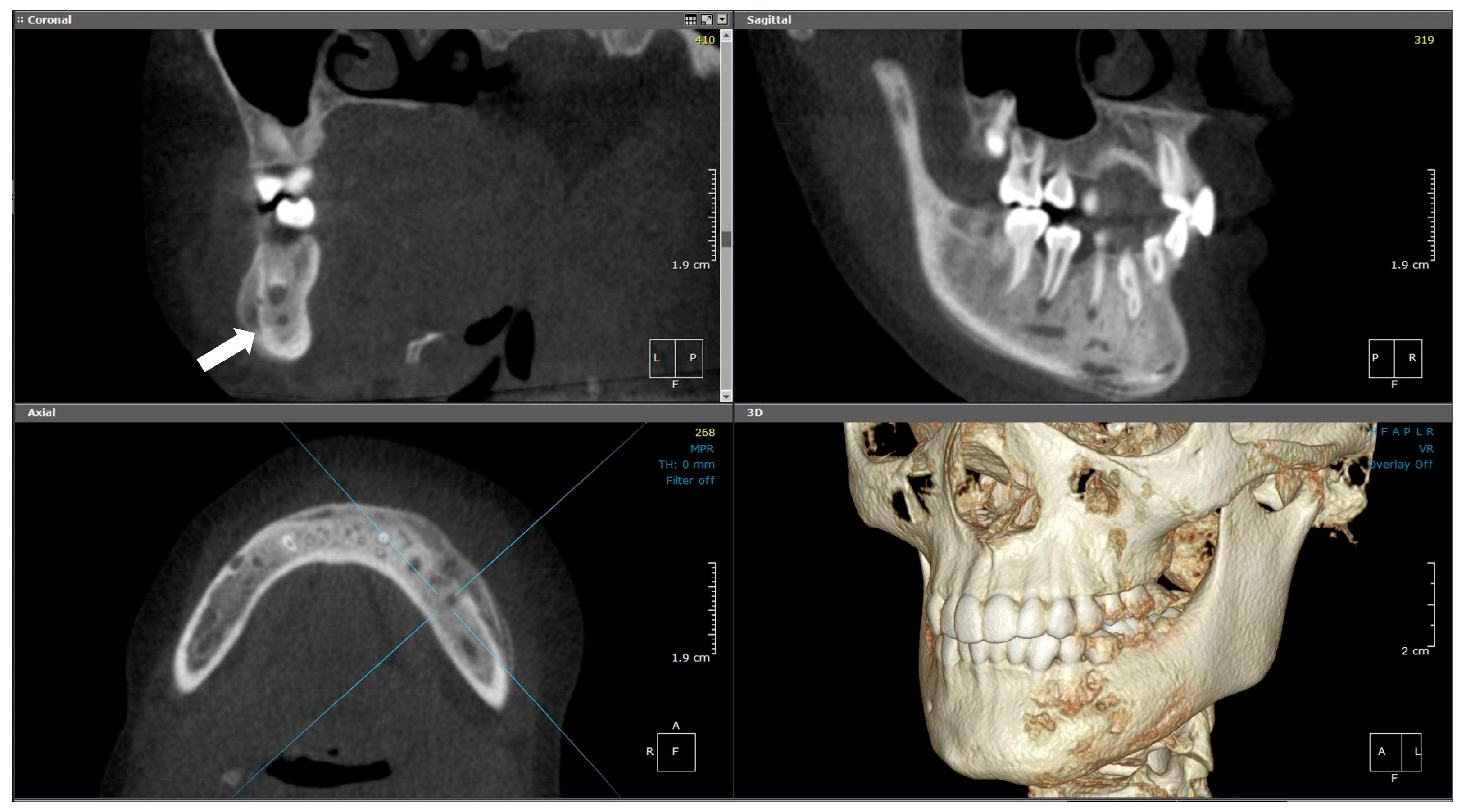
2.2.2. Radiographic Examination
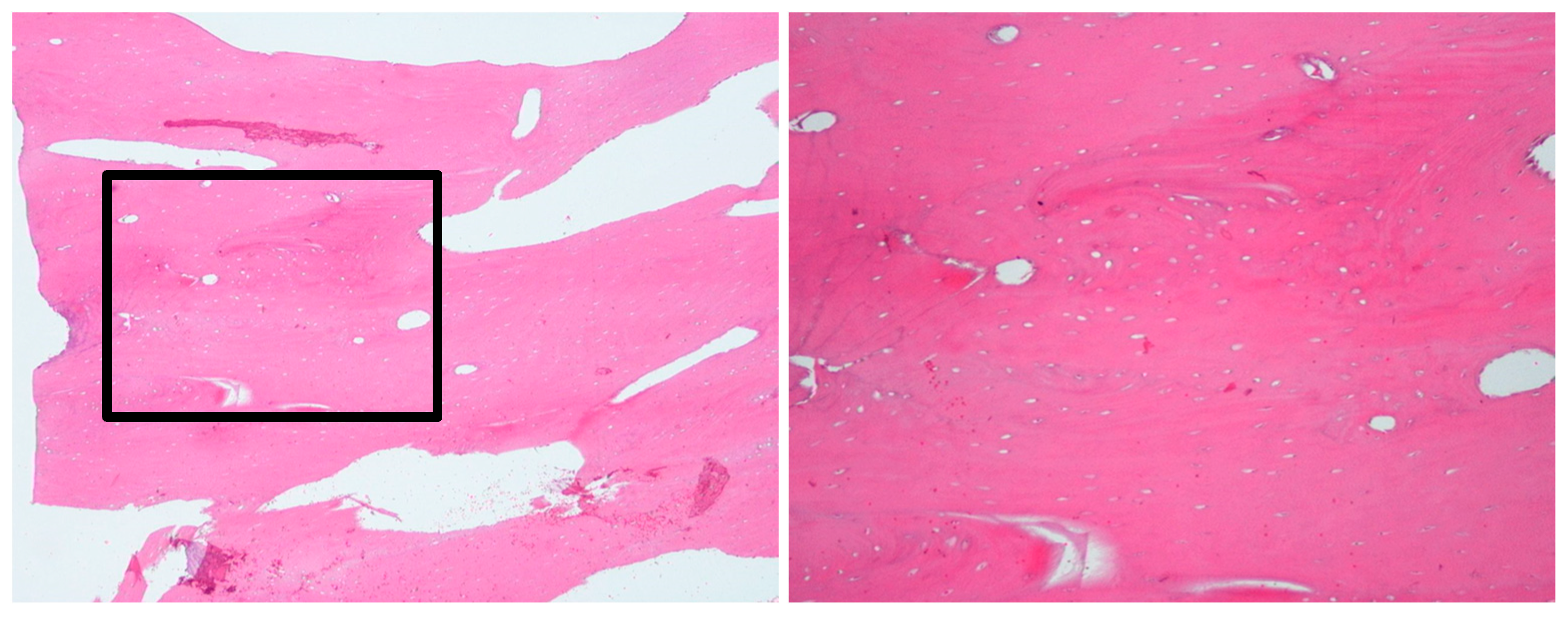
2.2.3. Histopathological Examination
2.2.4. Case Management and Differential Diagnosis
2.3. Case 3
2.3.1. History and Clinical Examination
2.3.2. Radiographic Examination
2.3.3. Histopathological Examination
2.3.4. Case Management and Differential Diagnosis
2.4. Case 4
2.4.1. History and Clinical Examination
2.4.2. Radiographic Examination
2.4.3. Histopathological Examination
2.4.4. Case Management and Differential Diagnosis
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| CNO | Chronic nonbacterial osteomyelitis |
| CRMO | Chronic recurrent multifocal osteomyelitis |
| FD | Fibrous dysplasia |
| NSAID | Non-steroidal anti-inflammatory drugs |
| DMARD | Disease-modifying antirheumatic drugs |
| CBCT | Cone-beam computed tomography |
| MPR | Multi-planar reformatted |
| MRI | Magnetic Resonance Imaging |
References
- Björkstén, B.; Gustavson, K.; Nordström, S.; Eriksson, B.; Lindholm, K. Chronic recurrent multifocal osteomyelitis and pustulosis palmoplantaris. J. Pediatr. 1978, 93, 227–231. [Google Scholar] [CrossRef] [PubMed]
- Buch, K.; Thuesen, A.C.B.; Brøns, C.; Schwarz, P. Chronic non-bacterial osteomyelitis: A review. Calcif. Tissue Int. 2019, 104, 544–553. [Google Scholar] [CrossRef]
- Girschick, H.J.; Raab, P.; Surbaum, S.; Trusen, A.; Kirschner, S.; Schneider, P.; Papadopoulos, T.; Müller-Hermelink, H.K.; Lipsky, P.E. Chronic non-bacterial osteomyelitis in children. Ann. Rheum. Dis. 2005, 64, 279–285. [Google Scholar] [CrossRef] [PubMed]
- Hofmann, S.R.; Schnabel, A.; Rösen-Wolff, A.; Morbach, H.; Girschick, H.J.; Hedrich, C.M. Chronic nonbacterial osteomyelitis: Pathophysiological concepts and current treatment strategies. J. Rheumatol. 2016, 43, 1956–1964. [Google Scholar] [CrossRef]
- Jia, K.; Zhang, J.; Li, T.; Zhang, Y.; An, J. Comparison of the histopathological characteristics of diffuse sclerosing osteomyelitis of the mandible, chronic suppurative osteomyelitis, and craniofacial fibrous dysplasia. J. Oral. Pathol. Med. 2023, 52, 91–98. [Google Scholar] [CrossRef] [PubMed]
- Padwa, B.L.; Dentino, K.; Robson, C.D.; Woo, S.B.; Kurek, K.; Resnick, C.M. Pediatric chronic nonbacterial osteomyelitis of the jaw: Clinical, radiographic, and histopathologic features. J. Oral. Maxillofac. Surg. 2016, 74, 2393–2402. [Google Scholar] [CrossRef]
- Borzutzky, A.; Stern, S.; Reiff, A.; Zurakowski, D.; Steinberg, E.A.; Dedeoglu, F.; Sundel, R.P. Pediatric chronic nonbacterial osteomyelitis. Pediatrics 2012, 130, e1190–e1197. [Google Scholar] [CrossRef]
- Khanna, G.; Sato, T.S.; Ferguson, P. Imaging of chronic recurrent multifocal osteomyelitis. Radiographics 2009, 29, 1159–1177. [Google Scholar] [CrossRef]
- Zhao, D.Y.; McCann, L.; Hahn, G.; Hedrich, C.M. Chronic nonbacterial osteomyelitis (CNO) and chronic recurrent multifocal osteomyelitis (CRMO). J. Transl. Autoimmun. 2021, 4, 100095. [Google Scholar] [CrossRef]
- Zain-Alabdeen, E.; Abdelfattah, A.; Kordi, O.; Al-Sadhan, R. The dilemma of juvenile fibrous dysplasia versus chronic osteomyelitis of the posterior mandible: A case report. Clin. Case Rep. 2022, 10, e6379. [Google Scholar] [CrossRef]
- Monsour, P.; Dalton, J.B. Chronic recurrent multifocal osteomyelitis involving the mandible: Case reports and review of the literature. Dentomaxillofacial Radiol. 2010, 39, 184–190. [Google Scholar] [CrossRef] [PubMed]
- Beck, C.; Morbach, H.; Beer, M.; Stenzel, M.; Tappe, D.; Gattenlöhner, S.; Hofmann, U.; Raab, P.; Girschick, H.J. Chronic nonbacterial osteomyelitis in childhood: Prospective follow-up during the first year of anti-inflammatory treatment. Arthritis Res. Ther. 2010, 12, R74. [Google Scholar] [CrossRef]
- Taddio, A.; Ferrara, G.; Insalaco, A.; Pardeo, M.; Gregori, M.; Finetti, M.; Pastore, S.; Tommasini, A.; Ventura, A.; Gattorno, M. Dealing with chronic non-bacterial osteomyelitis: A practical approach. Pediatr. Rheumatol. 2017, 15, 87. [Google Scholar] [CrossRef] [PubMed]
- Schmitt, S.K. Osteomyelitis. Infect. Dis. Clin. 2017, 31, 325–338. [Google Scholar] [CrossRef] [PubMed]
- Gopal K, S.; Chandran, N.; Ramesh, S.; Ravi, P. Sclerosing Osteomyelitis of Jaw–A Case Series and Literature Review. Biomed. Res. Ther. 2024, 11, 6474–6481. [Google Scholar] [CrossRef]
- Mainville, G.N.; Turgeon, D.P.; Kauzman, A. Diagnosis and management of benign fibro-osseous lesions of the jaws: A current review for the dental clinician. Oral. Dis. 2017, 23, 440–450. [Google Scholar] [CrossRef]
- Jia, K.; Li, X.; An, J.; Zhang, Y. Comparing clinical and radiographic characteristics of chronic diffuse sclerosing osteomyelitis and craniofacial fibrous dysplasia in the mandible. J. Oral. Maxillofac. Surg. 2021, 79, 1053–1061. [Google Scholar] [CrossRef]
- Kugushev, A.; Lopatin, A.; Gra-chev, N.; Dagher, S.; Kotov, V. Clinical and Radiological Features of Primary Chronic Osteomyelitis and Fibrous Dysplasia of the Mandible. J. Clini-Cal Physiol. Pathol. (JISCPP) 2024, 3, 25–34. [Google Scholar] [CrossRef]
- Feller, L.; Wood, N.H.; Khammissa, R.A.; Lemmer, J.; Raubenheimer, E.J. The nature of fibrous dysplasia. Head. Face Med. 2009, 5, 22. [Google Scholar] [CrossRef]
- Gupta, V.; Jain, A.; Aggarwal, A. Chronic nonbacterial osteomyelitis from a tertiary care referral center. J. Postgrad. Med. 2018, 64, 170–173. [Google Scholar] [CrossRef]
- Seyhanli, D.; Alatas, S.O.; Guzin, A.C.; Mermer, E.T.K.; Aydin, T.; Cevizbas, S.; Oncel, E.K.; Sarioglu, F.C.; Belet, N. Multifocal Acute Osteomyelitis or Chronic Nonbacterial Osteomyelitis: Is It Always Easy to Diagnose? Pediatr. Infect. Dis. J. 2025, 44, e105–e106. [Google Scholar] [CrossRef] [PubMed]
- Costa-Reis, P.; Sullivan, K.E. Chronic recurrent multifocal osteomyelitis. J. Clin. Immunol. 2013, 33, 1043–1056. [Google Scholar] [CrossRef] [PubMed]
- Hu, M.; Zeng, W.; Zhang, J.; Yan, H.; Huang, F.; Xiong, H.; Fang, B.; Li, Y. Chronic recurrent multifocal osteomyelitis in pediatric patients: A Chinese single center observational study and literature review. Medicine 2024, 103, e40805. [Google Scholar] [CrossRef] [PubMed]
- Kubaszewski, Ł; Wojdasiewicz, P.; Rożek, M.; Słowińska, I.E.; Romanowska-Próchnicka, K.; Słowiński, R.; Poniatowski, ŁA.; Gasik, R. Syndromes with chronic non-bacterial osteomyelitis in the spine. Reumatol./Rheumatol. 2015, 53, 328–336. [Google Scholar] [CrossRef]
- Mathieu, D.; Marroni, A.; Kot, J. Tenth European Consensus Conference on Hyperbaric Medicine: Recommendations for accepted and non-accepted clinical indications and practice of hyperbaric oxygen treatment. Diving Hyperb. Med. 2017, 47, 24. [Google Scholar] [CrossRef]
- Mader, J.T.; Brown, G.L.; Guckian, J.C.; Wells, C.H.; Reinarz, J.A. A mechanism for the amelioration by hyperbaric oxygen of experimental staphylococcal osteomyelitis in rabbits. J. Infect. Dis. 1980, 142, 915–922. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Case | Age | Lesion Location | Radiographic Appearance | Histopathology | Initial Management | Definitive Diagnosis | Final Treatment | Outcome |
|---|---|---|---|---|---|---|---|---|
| 1 | 11 | Left mandible (#32–#37) | Mixed sclerotic and lytic lesion with buccolingual expansion and “onion-skin” periosteal reaction | Irregular bone and fibrous tissue, sclerosis, no inflammation or bacteria | Long-term antibiotic course, NSAIDs | CNO confirmed by imaging, histology, and initial failure to respond to antibiotics | Conservative; antibiotics discontinued after improvement | Improved at 7 months; recurrence at 18 months; no further treatment needed |
| 2 | 9 | Right mandible (#33–#47, crossing midline) | Patchy sclerotic and radiolucent lesion, mandibular expansion, double cortex | Viable bone with osteoblastic rimming, no bacterial colonies | Multiple antibiotics, extractions, NSAIDs | CNO based on imaging, histology, and clinical course | NSAIDs only; progressive improvement | Gradual resolution with NSAIDs |
| 3 | 10 | Right mandible (#34–#47, crossing midline) | Granular sclerotic and radiolucent lesion, moth-eaten pattern, layered periosteal reaction | Normal viable bone, sterile | Empirical antibiotics, paracetamol, NSAIDs | CNO confirmed by imaging, CT, and sterile biopsy | NSAIDs only; no need for further escalation | Progressive improvement; under observation |
| 4 | 12 | Left mandible (#37–#43, crossing midline) | Irregular mixed sclerotic/lytic lesion, periosteal reaction, buccolingual expansion | Viable bone with no bacterial colonies | Empirical antibiotics, paracetamol, NSAIDs | CNO confirmed based on recurrence, imaging, and histology | NSAIDs only; no additional therapy needed | Gradual clinical improvement; no recurrence noted |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Barayan, M.; Abdel Wahed, N.; Helal, N.; Komo, H.A.; Iskanderani, D.; Alansari, R.; Alhindi, N.A.; Alhelo, A.F.; Khalifa, H.; Sabban, H. Radiographic and Histopathological Characteristics of Chronic Nonbacterial Osteomyelitis of the Mandible in Pediatric Patients: Case Series. Diagnostics 2025, 15, 1549. https://doi.org/10.3390/diagnostics15121549
Barayan M, Abdel Wahed N, Helal N, Komo HA, Iskanderani D, Alansari R, Alhindi NA, Alhelo AF, Khalifa H, Sabban H. Radiographic and Histopathological Characteristics of Chronic Nonbacterial Osteomyelitis of the Mandible in Pediatric Patients: Case Series. Diagnostics. 2025; 15(12):1549. https://doi.org/10.3390/diagnostics15121549
Chicago/Turabian StyleBarayan, Mohammed, Nagla’a Abdel Wahed, Narmin Helal, Hisham Abbas Komo, Durer Iskanderani, Raghd Alansari, Nada A. Alhindi, Azza F. Alhelo, Hanadi Khalifa, and Hanadi Sabban. 2025. "Radiographic and Histopathological Characteristics of Chronic Nonbacterial Osteomyelitis of the Mandible in Pediatric Patients: Case Series" Diagnostics 15, no. 12: 1549. https://doi.org/10.3390/diagnostics15121549
APA StyleBarayan, M., Abdel Wahed, N., Helal, N., Komo, H. A., Iskanderani, D., Alansari, R., Alhindi, N. A., Alhelo, A. F., Khalifa, H., & Sabban, H. (2025). Radiographic and Histopathological Characteristics of Chronic Nonbacterial Osteomyelitis of the Mandible in Pediatric Patients: Case Series. Diagnostics, 15(12), 1549. https://doi.org/10.3390/diagnostics15121549