
CBCT-Based Anthropometric Evaluation of Edentulous Alveolar Crest Lengths

Abstract
1. Introduction
2. Methods
2.1. Study Population
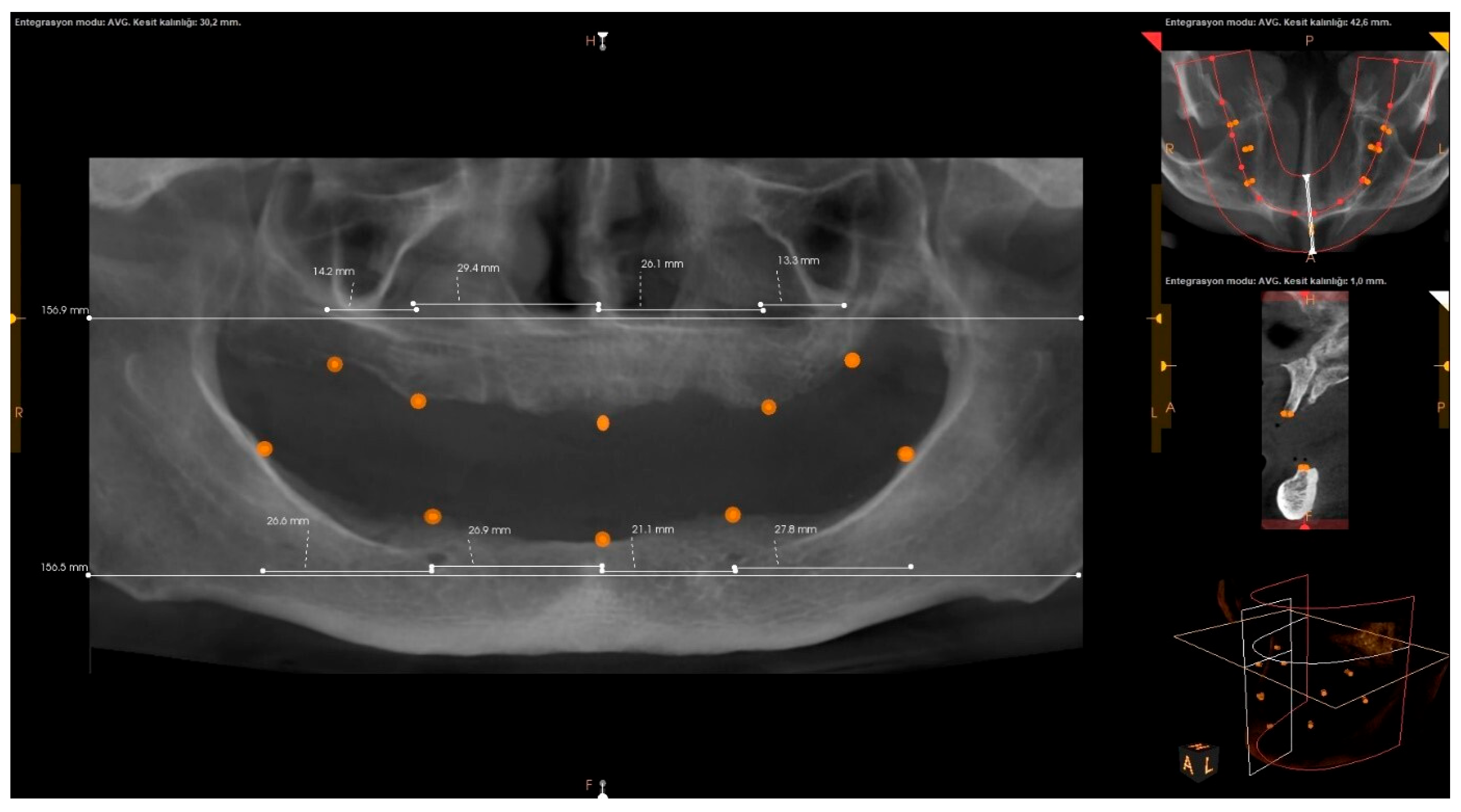
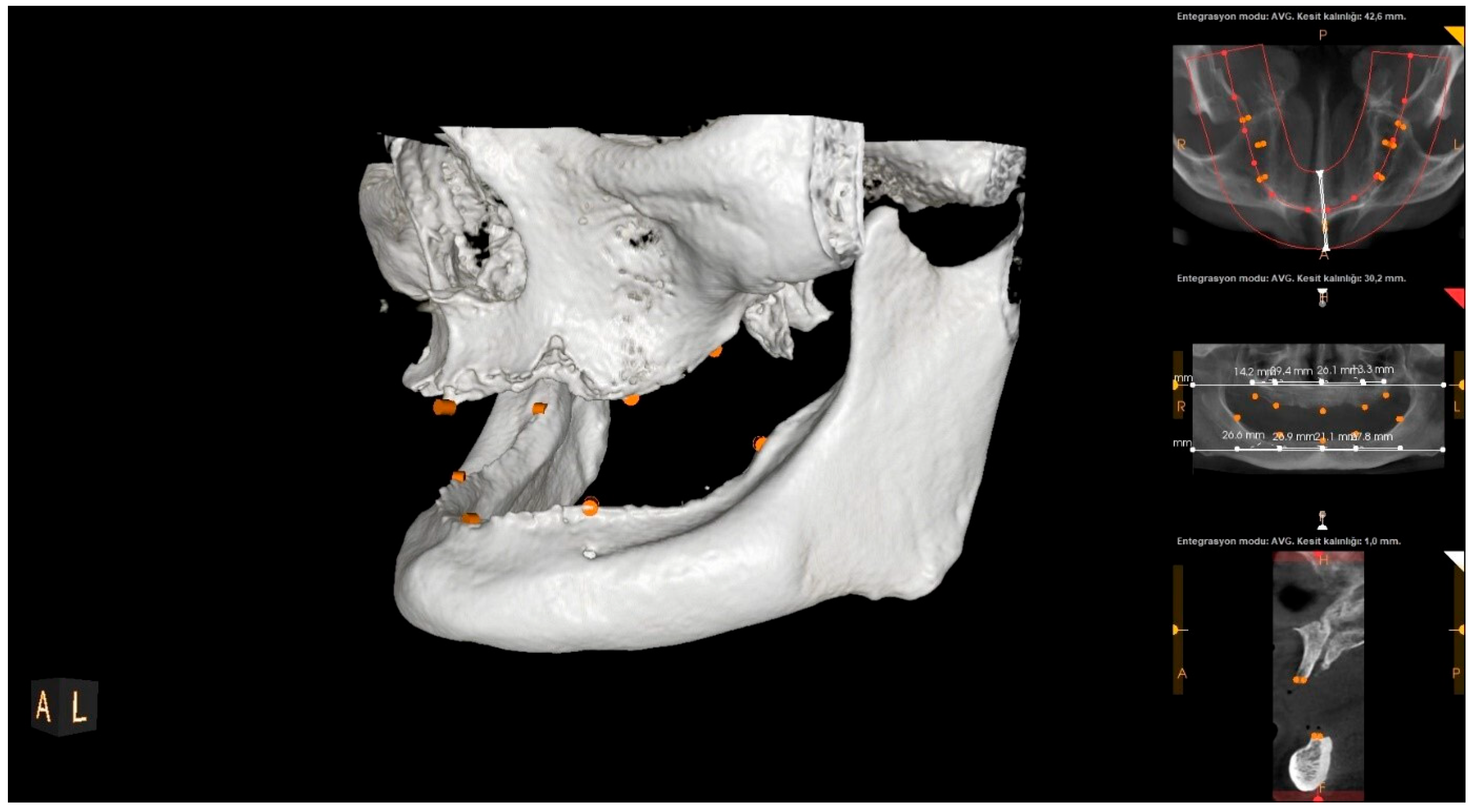
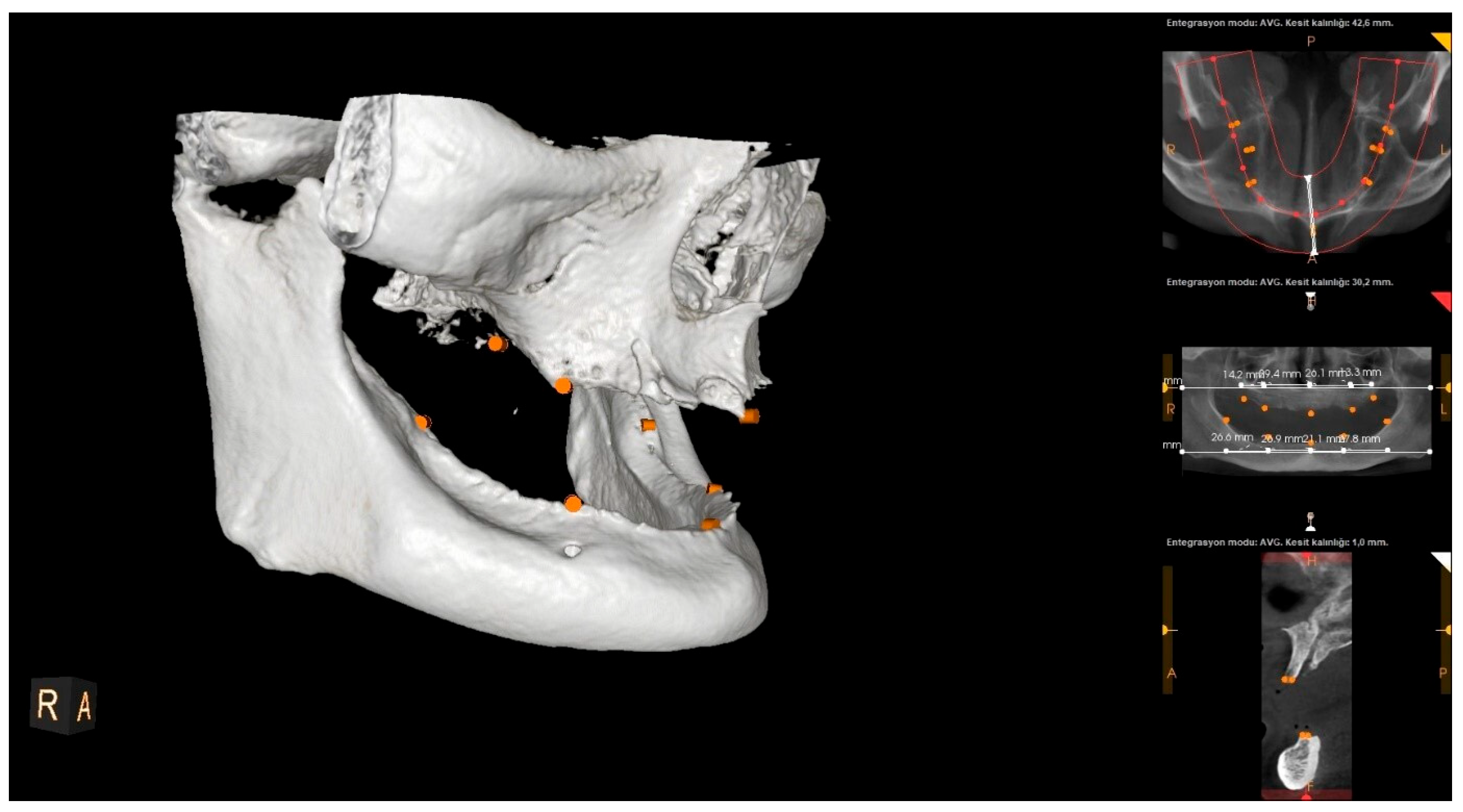
2.2. Processing of CBCT Scans and Radiographic Measurements
2.3. Statistical Analysis
2.3.1. Data Analysis
2.3.2. Sample Size
2.3.3. Intraobserver Repeatability
2.4. Compliance with Reporting Guidelines
2.5. Ethical Approval
3. Results
3.1. Study Population
3.2. Radiographic Measurements
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Arı, I.; Acar, G.; Tosun, E.; Muhtaroğulları, M. Assessment of different treatment alternatives for patients with total maxillectomy. J. Prosthodont. 2024. online ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Acar, G.; Ari, I.; Tosun, E. Biomechanical evaluation of implant options for unilateral maxillary defects: A finite element analysis. BMC Oral. Health 2024, 24, 1338. [Google Scholar] [CrossRef] [PubMed]
- Padhye, N.M.; Bhatavadekar, N.B. Quantitative Assessment of the Edentulous Posterior Maxilla for Implant Therapy: A Retrospective Cone Beam Computed Tomographic Study. J. Maxillofac. Oral. Surg. 2020, 19, 125–130. [Google Scholar] [CrossRef]
- Şeker, B.K.; Orhan, K.; Şeker, E.; Ustaoğlu, G.; Ozan, O.; Bağiş, N. Cone Beam CT Evaluation of Maxillary Sinus Floor and Alveolar Crest Anatomy for the Safe Placement of Implants. Curr. Med Imaging 2020, 16, 913–920. [Google Scholar] [CrossRef]
- Frost, H.M. Perspectives: A proposed general model of the “Mechanostat” (Suggestions from a new skeletal-biologic paradigm). Anat. Rec. 1996, 244, 139–147. [Google Scholar] [CrossRef]
- Saeed, T.A.; Alansy, A.S.; Abdu, Z.A.; Almaqtari, O.; Yu, Z. Dentulous versus edentulous mandibles: CBCT-based morphometric assessment of mandibular canal and alveolar bone. J. Clin. Exp. Dent. 2022, 14, e986–e993. [Google Scholar] [CrossRef] [PubMed]
- Narmadha, C.; Ganesh, M.R.; Vardhan, B.G.H.; Gopal, S. CBCT Based Pre-Implant Assessment of Maxilla and Mandible—An Insight to Vital Anatomical Structures. Int. J. Res. Rev. 2023, 10, 514–525. [Google Scholar] [CrossRef]
- Bressan, E.; Ferrarese, N.; Pramstraller, M.; Lops, D.; Farina, R.; Tomasi, C. Ridge Dimensions of the Edentulous Mandible in Posterior Sextants: An Observational Study on Cone Beam Computed Tomography Radiographs. Implant. Dent. 2017, 26, 66–72. [Google Scholar] [CrossRef]
- Pramstraller, M.; Schincaglia, G.P.; Vecchiatini, R.; Farina, R.; Trombelli, L. Alveolar ridge dimensions in mandibular posterior regions: A retrospective comparative study of dentate and edentulous sites using computerized tomography data. Surg. Radiol. Anat. 2018, 40, 1419–1428. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Routledge: London, UK, 2013. [Google Scholar]
- Shemtov-Yona, K. Quantitative assessment of the jawbone quality classification: A meta-analysis study. PLoS ONE 2021, 16, e0253283. [Google Scholar] [CrossRef]
- Theunisse, H.J.; Joemai, R.M.; Maal, T.J.; Geleijns, J.; Mylanus, E.A.; Verbist, B.M. Cone-beam CT versus multi-slice CT systems for postoperative imaging of cochlear implantation--a phantom study on image quality and radiation exposure using human temporal bones. Otol. Neurotol. 2015, 36, 592–599. [Google Scholar] [CrossRef] [PubMed]
- Peker, I.; Alkurt, M.T.; Michcioglu, T. The use of 3 different imaging methods for the localization of the mandibular canal in dental implant planning. Int. J. Oral Maxillofac. Implant. 2008, 23, 463–470. [Google Scholar]
- Carlsson, G.E.; Persson, G. Morphologic changes of the mandible after extraction and wearing of dentures. A longitudinal, clinical, and x-ray cephalometric study covering 5 years. Odontol. Revy 1967, 18, 27–54. [Google Scholar]
- Van der Weijden, F.; Dell’Acqua, F.; Slot, D.E. Alveolar bone dimensional changes of post-extraction sockets in humans: A systematic review. J. Clin. Periodontol. 2009, 36, 1048–1058. [Google Scholar] [CrossRef]
- Pedrinaci, I.; Sun, T.C.; Sanz-Alonso, M.; Sanz-Esporrin, J.; Hamilton, A.; Gallucci, G.O. Implant survival in the anterior mandible: A retrospective cohort study. Clin. Oral Implant. Res. 2023, 34, 463–474. [Google Scholar] [CrossRef] [PubMed]
- Mangano, C.; Luongo, G.; Luongo, F.; Lerner, H.; Margiani, B.; Admakin, O.; Mangano, F. Custom-made computer-aided-design/computer-assisted-manufacturing (CAD/CAM) synthetic bone grafts for alveolar ridge augmentation: A retrospective clinical study with 3 years of follow-up. J. Dent. 2022, 127, 104323. [Google Scholar] [CrossRef] [PubMed]
- Mareque, S.; Castelo-Baz, P.; López-Malla, J.; Blanco, J.; Nart, J.; Vallés, C. Clinical and esthetic outcomes of immediate implant placement compared to alveolar ridge preservation: A systematic review and meta-analysis. Clin. Oral Investig. 2021, 25, 4735–4748. [Google Scholar] [CrossRef]
- Barone, A.; Ricci, M.; Mangano, F.; Covani, U. Morbidity associated with iliac crest harvesting in the treatment of maxillary and mandibular atrophies: A 10-year analysis. J. Oral Maxillofac. Surg. 2011, 69, 2298–2304. [Google Scholar] [CrossRef]
- Holtzclaw, D.; Toscano, N.; Eisenlohr, L.; Callan, D. The safety of bone allografts used in dentistry: A review. J. Am. Dent. Assoc. 2008, 139, 1192–1199. [Google Scholar] [CrossRef]
- Mehra, M.; Somohano, T.; Choi, M. Mandibular fibular graft reconstruction with CAD/CAM technology: A clinical report and literature review. J. Prosthet. Dent. 2016, 115, 123–128. [Google Scholar] [CrossRef]
- Ciocca, L.; Lizio, G.; Baldissara, P.; Sambuco, A.; Scotti, R.; Corinaldesi, G. Prosthetically CAD-CAM-Guided Bone Augmentation of Atrophic Jaws Using Customized Titanium Mesh: Preliminary Results of an Open Prospective Study. J. Oral Implantol. 2018, 44, 131–137. [Google Scholar] [CrossRef] [PubMed]
- Tsigarida, A.; Toscano, J.; de Brito Bezerra, B.; Geminiani, A.; Barmak, A.B.; Caton, J.; Papaspyridakos, P.; Chochlidakis, K. Buccal bone thickness of maxillary anterior teeth: A systematic review and meta-analysis. J. Clin. Periodontol. 2020, 47, 1326–1343. [Google Scholar] [CrossRef] [PubMed]
- Magat, G. Radiomorphometric analysis of edentulous posterior mandibular ridges in the first molar region: A cone-beam computed tomography study. J. Periodontal Implant. Sci. 2019, 50, 28–37. [Google Scholar] [CrossRef] [PubMed]
- Acharya, A.; Hao, J.; Mattheos, N.; Chau, A.; Shirke, P.; Lang, N.P. Residual ridge dimensions at edentulous maxillary first molar sites and periodontal bone loss among two ethnic cohorts seeking tooth replacement. Clin. Oral Implant. Res. 2014, 25, 1386–1394. [Google Scholar] [CrossRef]
- Zhou, X.; Gao, X.; Zhang, J. Bifid mandibular canals: CBCT assessment and macroscopic observation. Surg. Radiol. Anat. 2020, 42, 1073–1079. [Google Scholar] [CrossRef]
- Genç, T.; Duruel, O.; Kutlu, H.B.; Dursun, E.; Karabulut, E.; Tözüm, T.F. Evaluation of anatomical structures and variations in the maxilla and the mandible before dental implant treatment. Dent. Med Probl. 2018, 55, 233–240. [Google Scholar] [CrossRef]
- Couso-Queiruga, E.; Stuhr, S.; Tattan, M.; Chambrone, L.; Avila-Ortiz, G. Post-extraction dimensional changes: A systematic review and meta-analysis. J. Clin. Periodontol. 2021, 48, 126–144. [Google Scholar] [CrossRef]
- Al-Zubai, N.M. Dental arch asymmetry. Eur. J. Dent. 2014, 8, 224–228. [Google Scholar] [CrossRef]
- Alam, M.K.; Shahid, F.; Purmal, K.; Ahmad, B.; Khamis, M.F. Tooth Size and Dental Arch Dimension Measurement through Cone Beam Computed Tomography: Effect of Age and Gender. Res. J. Recent Sci. 2014, 3, 2277–2502. [Google Scholar]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Gender | n | Median (Min.–Max.) | Center ± S.s. | Test Statistic | p | |
|---|---|---|---|---|---|---|
| Age | Female | 259 | 61 (34–86) | 61.05 ± 9.79 | U = 21,489.500 | 0.014 * |
| Male | 192 | 59 (22–87) | 58.7 ± 9.57 |
| Measurement Fields | n | Median (Min.–Max.) | Center ± S.s. |
|---|---|---|---|
| U1 | 296 | 13 (6.6–29.6) | 13.47 ± 3.15 |
| U2 | 296 | 24.85 (11.6–36.5) | 25.02 ± 4.04 |
| U3 | 296 | 24.25 (9.6–35.8) | 24.41 ± 3.93 |
| U4 | 296 | 12.7 (5.7–29.3) | 13.05 ± 3.06 |
| L1 | 299 | 30.6 (16–45.1) | 30.74 ± 4.59 |
| L2 | 299 | 23.6 (12.2–33.3) | 23.2 ± 3.44 |
| L3 | 299 | 25.2 (9.5–36.8) | 24.97 ± 3.46 |
| L4 | 299 | 28.7 (16–41.6) | 28.49 ± 4.13 |
| Measurement Fields | Gender | n | Median (Min.–Max.) | Centrer ± S.s. | Test Statistic | p |
|---|---|---|---|---|---|---|
| U1 | Female | 165 | 12.9 (7–29.6) | 13.25 ± 2.89 | U = 10,201.500 | 0.407 |
| Male | 131 | 13.3 (6.6–25.4) | 13.73 ± 3.43 | |||
| U2 | Female | 165 | 24.9 (12.7–36.5) | 25.2 ± 3.88 | t = 0.877 | 0.381 |
| Male | 131 | 24.5 (11.6–35.8) | 24.79 ± 4.24 | |||
| U3 | Female | 165 | 24.2 (9.6–35.8) | 24.34 ± 3.87 | U = 10,479.000 | 0.653 |
| Male | 131 | 24.3 (10.7–35.2) | 24.49 ± 4.03 | |||
| U4 | Female | 165 | 12.7 (7.9–23.1) | 13.1 ± 2.88 | U = 10,278.500 | 0.469 |
| Male | 131 | 12.7 (5.7–29.3) | 12.99 ± 3.28 | |||
| L1 | Female | 176 | 30.05 (16–42.2) | 29.79 ± 4.3 | t = −4.386 | 0.000 * |
| Male | 123 | 31.5 (22–45.1) | 32.09 ± 4.66 | |||
| L2 | Female | 176 | 23.25 (12.2–33.1) | 22.85 ± 3.27 | t = −2.156 | 0.032 * |
| Male | 123 | 24.1 (14.6–33.3) | 23.71 ± 3.63 | |||
| L3 | Female | 176 | 24.65 (9.5–36.2) | 24.67 ± 3.61 | t = −1.835 | 0.068 |
| Male | 123 | 25.6 (17.6–36.8) | 25.41 ± 3.21 | |||
| L4 | Female | 176 | 27.45 (16–41.6) | 27.58 ± 4.11 | t = −4.698 | 0.000 * |
| Male | 123 | 30.2 (19.8–39.7) | 29.78 ± 3.81 |
| Measurement Fields | Age | n | Median (Min.-Max.) | Center ± S.s. | Test Statistic | p | Bonferroni (p) |
|---|---|---|---|---|---|---|---|
| U1 | Under 50 years old | 45 | 12.9 (6.6–29.6) | 13.13 ± 3.43 | KW = 1.434 | 0.698 | - |
| 50–59 years old | 105 | 13.4 (7.9–25.4) | 13.50 ± 2.83 | ||||
| 60–69 years old | 110 | 12.8 (7–25.3) | 13.48 ± 3.27 | ||||
| 70 years old and above | 36 | 13.25 (7.6–22.3) | 13.75 ± 3.35 | ||||
| U2 | Under 50 years old | 45 | 25.4 (18.4–35.8) | 25.35 ± 3.77 | F = 1.868 | 0.135 | - |
| 50–59 years old | 105 | 24.9 (13.6–35.5) | 24.87 ± 3.76 | ||||
| 60–69 years old | 110 | 24.1 (11.6–34.6) | 24.59 ± 4.31 | ||||
| 70 years old and above | 36 | 26.45 (15.1–36.5) | 26.35 ± 4.19 | ||||
| U3 | Under 50 years old | 45 | 24 (17.3–34.3) | 24.27 ± 3.66 | KW = 1.740 | 0.628 | - |
| 50–59 years old | 105 | 24.3 (17.4–35.8) | 24.63 ± 3.87 | ||||
| 60–69 years olf | 110 | 23.85 (9.6–35.2) | 24.07 ± 4.09 | ||||
| 70 years old and above | 36 | 24.75 (14.7–35.2) | 24.99 ± 4.01 | ||||
| U4 | Under 50 years old | 45 | 12.6 (8.1–17.4) | 12.77 ± 2.21 | KW = 3.505 | 0.320 | - |
| 50–59 years old | 105 | 12.8 (7.3–22.9) | 13.12 ± 2.75 | ||||
| 60–69 years old | 110 | 12.6 (7.9–29.3) | 12.88 ± 3.49 | ||||
| 70 years old and above | 36 | 13.55 (5.7–20.9) | 13.75 ± 3.40 | ||||
| L1 | Under 50 years old | 35 | 31.1 (21.4–43.5) | 31.50 ± 4.93 | F = 0.774 | 0.509 | - |
| 50–59 years old | 91 | 30.5 (22.8–45.1) | 30.86 ± 4.14 | ||||
| 60–69 years old | 126 | 30.6 (17.8–42.2) | 30.72 ± 4.70 | ||||
| 70 years old and above | 47 | 30.3 (16–42) | 29.98 ± 4.85 | ||||
| L2 | Under 50 years old | 35 | 23.7 (18.4–29.4) | 23.73 ± 2.64 | F = 1.433 | 0.233 | - |
| 50–59 years old | 91 | 23.7 (15.2–32.4) | 23.53 ± 3.10 | ||||
| 60–69 years old | 126 | 23.8 (12.2–33.3) | 23.12 ± 3.99 | ||||
| 70 years old and above | 47 | 22 (16.9–29.6) | 22.40 ± 2.90 | ||||
| L3 | Under 50 years old | 35 | 24.7 (18.9–31.9) | 24.35 ± 3.06 | F = 0.459 | 0.711 | - |
| 50–59 years old | 91 | 25.4 (16.8–35.7) | 25.07 ± 3.32 | ||||
| 60–69 years old | 126 | 25.25 (9.5–36.2) | 25.1 ± 3.62 | ||||
| 70 years old and above | 47 | 25 (17.7–36.8) | 24.9 ± 3.66 | ||||
| L4 | Under 50 years old (1) | 35 | 29.7 (22.5–39.5) | 29.45 ± 3.71 | F = 2.633 | 0.050 * | 4 < 1 (0.041 *) |
| 50–59 years old (2) | 91 | 29.10 (18.6–39.7) | 28.87 ± 3.65 | ||||
| 60–69 years old (3) | 126 | 28.45 (16–41.6) | 28.45 ± 4.58 | ||||
| 70 years old and above (4) | 47 | 26.70 (19.6–34.7) | 27.13 ± 3.80 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yildirim, O.; Izgi, E.; Ozturk, M.; Gulen, O. CBCT-Based Anthropometric Evaluation of Edentulous Alveolar Crest Lengths. Diagnostics 2025, 15, 1525. https://doi.org/10.3390/diagnostics15121525
Yildirim O, Izgi E, Ozturk M, Gulen O. CBCT-Based Anthropometric Evaluation of Edentulous Alveolar Crest Lengths. Diagnostics. 2025; 15(12):1525. https://doi.org/10.3390/diagnostics15121525
Chicago/Turabian StyleYildirim, Ozgun, Eda Izgi, Mustafa Ozturk, and Orhan Gulen. 2025. "CBCT-Based Anthropometric Evaluation of Edentulous Alveolar Crest Lengths" Diagnostics 15, no. 12: 1525. https://doi.org/10.3390/diagnostics15121525
APA StyleYildirim, O., Izgi, E., Ozturk, M., & Gulen, O. (2025). CBCT-Based Anthropometric Evaluation of Edentulous Alveolar Crest Lengths. Diagnostics, 15(12), 1525. https://doi.org/10.3390/diagnostics15121525