

Study Design and Rationale of a Randomized Trial Comparing Aspirin–Sarpogrelate Combination Therapy with Aspirin Monotherapy: Effects on Blood Viscosity and Microcirculation in Cardiovascular Patients
 , ,
, ,  and
and
Abstract
1. Introduction
2. Methods
2.1. Study Design
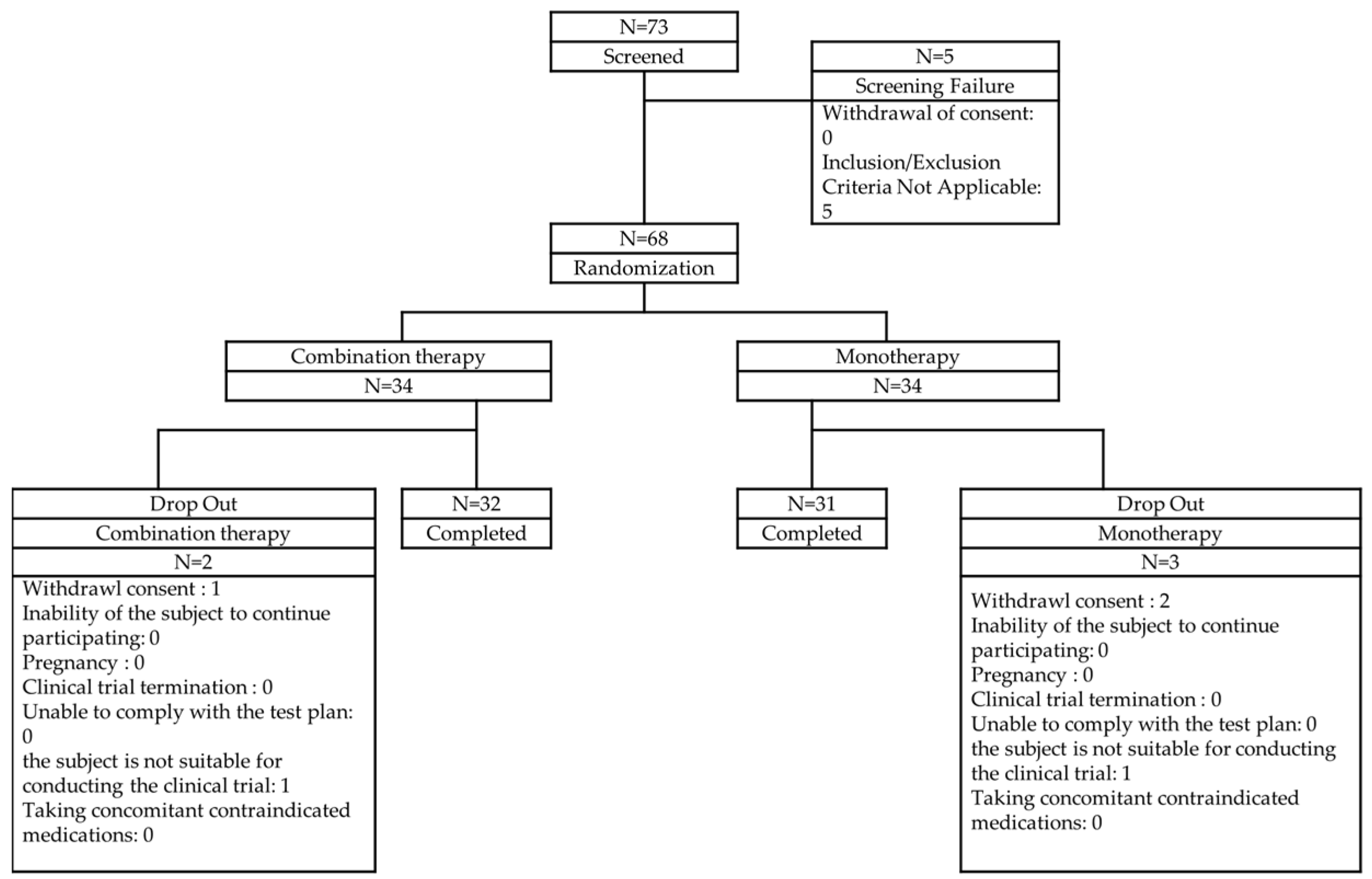
2.2. Recruitment and Screening
2.3. Sample Size
2.4. Demography
2.5. Randomization and Interventions
2.6. Outcome Measures
2.6.1. Primary and Secondary Outcomes
- Change in blood viscosity at week 4 compared to baseline.
- Change in erythrocyte deformability and erythrocyte aggregation at weeks 4 and 12 compared to baseline.
- Change in flow-mediated dilation (FMD) at weeks 4 and 12 compared to baseline.
- Change in oxygen delivery index (tODI) at weeks 4 and 12 compared to baseline.
- Proportion of patients with a ≥20% improvement in tODI at weeks 4 and 12.
- Change in lipid profile, fasting plasma glucose (FPG), homeostatic model assessment for insulin resistance (HOMA-IR), and high-sensitivity C-reactive protein (hs-CRP) at weeks 4 and 12 compared to baseline.
- Change in patient-reported quality of life outcomes (SF-36 and VAS) at week 12 compared to baseline.
2.6.2. Blood Viscosity and Tissue Oxygen Delivery Index
2.6.3. RBC Deformability and Aggregation Test
2.6.4. Flow-Mediated Dilation
2.7. Safety Assessments
2.8. Statistical Analyses
2.8.1. Primary Efficacy Endpoint
2.8.2. Secondary Efficacy Endpoint
2.9. Regulatory and Ethical Approval
3. Discussion
3.1. Rationale of the Study and Outcome Measures
3.2. Limitations and Further Considerations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
| Procedure | Screening (<4 Weeks) | Randomization (Week 0) | Treatment (Week 4 ± 1 Week) | Treatment (Week 12 ± 1 Week) | Early Discontinuation |
|---|---|---|---|---|---|
| Visit | SV | Visit 1 | Visit 2 | Visit 3 | ED |
| Informed consent | ✓ | ||||
| Eligibility assessment | ✓ | ||||
| Medical history and demographics | ✓ | ||||
| Physical examination | ✓ | ✓ | ✓ | ✓ | ✓ |
| Vital signs | ✓ | ✓ | ✓ | ✓ | ✓ |
| Laboratory tests | ✓ | ✓ | ✓ | ✓ | ✓ |
| Randomization | ✓ | ||||
| Study drug administration | ✓ | ✓ | ✓ | ||
| Concomitant medication assessment | ✓ | ✓ | ✓ | ✓ | ✓ |
| Medication adherence assessment | ✓ | ✓ | ✓ | ||
| Adverse event monitoring | ✓ | ✓ | ✓ | ✓ | |
| Early discontinuation assessment | ✓ |
| Product Name | Manufacturer | Dosage Form and Appearance | Active Ingredient | Storage Conditions |
|---|---|---|---|---|
| Anplag SR Tablets 300 mg | Yuhan Corporation | White, film-coated, sustained-release tablet | Sarpogrelate hydrochloride 300 mg | Sealed container, store at 1–30 °C |
| Aspirin Protect Tablets 100 mg | Bayer Korea | White, round, film-coated tablet | Aspirin 100 mg | Sealed container, store at 1–25 °C |
Inclusion and Exclusion Criteria
- -
- Patients aged 19 years or older at the time of informed consent.
- -
- Individuals diagnosed with coronary artery stenosis of 10–75% confirmed by coronary angiography or coronary computed tomography angiography.
- -
- Individuals diagnosed with peripheral arterial disease (PAD) or exhibiting symptoms of PAD.
- -
- Individuals who have fully understood the study objectives, the characteristics and risks of the investigational drug, and have provided written informed consent after receiving a thorough explanation.
- -
- Individuals scheduled for surgery related to coronary artery disease or cerebrovascular disease.
- -
- Individuals who have taken aspirin within two weeks prior to randomization.
- -
- Individuals currently receiving or planning to receive antiplatelet agents or anticoagulants other than aspirin.
- -
- Individuals with the following laboratory test results at the time of screening:
- Hemoglobin level below 13 g/dL (or below 12 g/dL for females).
- Platelet count (PLT) below 60,000/µL.
- Severe renal impairment (eGFR < 30 mL/min/1.73 m2, based on the CKD-EPI equation).
- -
- Individuals with a history of cerebrovascular or cardiovascular complications (stroke, transient ischemic attack, myocardial infarction, unstable angina, coronary artery bypass grafting, or percutaneous coronary intervention) within the past six months.
- -
- Individuals with active bleeding disorders (including hemophilia, capillary fragility syndrome, gastric ulcer bleeding, urinary tract bleeding, hemoptysis, or vitreous hemorrhage).
- -
- Pregnant or lactating women, or those planning to become pregnant.
- -
- Individuals currently participating in another clinical trial involving investigational drugs.
- -
- Any other individuals deemed inappropriate for participation in this clinical trial by the investigator.
References
- Khalid, N.; Haider, S.; Abdullah, M.; Asghar, S.; Laghari, M.A.; Rajeswaran, Y. Trends and Disparities in Coronary Artery Disease Prevalence among U.S. Adults from 2019 to 2022. Curr. Probl. Cardiol. 2024, 49, 102645. [Google Scholar] [CrossRef] [PubMed]
- Libby, P.; Ridker, P.M.; Maseri, A. Inflammation and Atherosclerosis. Circulation 2002, 105, 1135–1143. [Google Scholar] [CrossRef] [PubMed]
- Sloop, G.; Holsworth, R.E.; Weidman, J.J.; Cyr, J.A. The Role of Chronic Hyperviscosity in Vascular Disease. Ther. Adv. Cardiovasc. Dis. 2015, 9, 19–25. [Google Scholar] [CrossRef]
- Cekirdekci, E.I.; Bugan, B. Whole Blood Viscosity in Microvascular Angina and Coronary Artery Disease: Significance and Utility. Rev. Port. Cardiol. 2020, 39, 17–23. [Google Scholar] [CrossRef]
- Lowe, G.D.O.; Forbes, C.D.; Prentice, C.R.M.; Drummond, M.M.; Barbenel, J.C.; Lorimer, A.R.; Hutton, I. Relation between Extent of Coronary Artery Disease and Blood Viscosity. Br. Med. J. 1980, 280, 673. [Google Scholar] [CrossRef]
- Baskurt, O.K.; Meiselman, H.J. Blood Rheology and Hemodynamics. Semin. Thromb. Hemost. 2023, 50, 902–915. [Google Scholar] [CrossRef]
- Gyawali, P.; Richards, R.S.; Hughes, D.L.; Tinley, P. Erythrocyte Aggregation and Metabolic Syndrome. Clin. Hemorheol. Microcirc. 2014, 57, 73–83. [Google Scholar] [CrossRef]
- Shin, S.; Ku, Y.H.; Ho, J.X.; Kim, Y.K.; Suh, J.S.; Singh, M. Progressive Impairment of Erythrocyte Deformability as Indicator of Microangiopathy in Type 2 Diabetes Mellitus. Clin. Hemorheol. Microcirc. 2007, 36, 253–261. [Google Scholar]
- Baigent, C.; Sudlow, C.; Collins, R.; Peto, R. Collaborative Meta-Analysis of Randomised Trials of Antiplatelet Therapy for Prevention of Death, Myocardial Infarction, and Stroke in High Risk Patients. Br. Med. J. 2002, 324, 71–86. [Google Scholar] [CrossRef]
- Bhatt, D.L.; Topol, E.J. Scientific and Therapeutic Advances in Antiplatelet Therapy. Nat. Rev. Drug Discov. 2003, 2, 15–28. [Google Scholar] [CrossRef]
- Rosenson, R.S.; Wolff, D.; Green, D.; Boss, A.H.; Kensey, K.R. Aspirin. Aspirin Does Not Alter Native Blood Viscosity. J. Thromb. Haemost. 2004, 2, 340–341. [Google Scholar] [CrossRef] [PubMed]
- Rosenson, R.S. Treatment with Aspirin and Dipyridamole Is More Effective than Aspirin in Reducing Low Shear Blood Viscosity. Microcirculation 2008, 15, 615–620. [Google Scholar] [CrossRef] [PubMed]
- Saini, H.K.; Takeda, N.; Goyal, R.K.; Kumamoto, H.; Arneja, A.S.; Dhalla, N.S. Therapeutic Potentials of Sarpogrelate in Cardiovascular Disease. Cardiovasc. Drug Rev. 2004, 22, 27–54. [Google Scholar] [CrossRef]
- Satomura, K.; Takase, B.; Hamabe, A.; Ashida, K.; Hosaka, H.; Ohsuzu, F.; Kurita, A. Sarpogrelate, a Specific 5HT2-Receptor Antagonist, Improves the Coronary Microcirculation in Coronary Artery Disease. Clin. Cardiol. 2002, 25, 28–32. [Google Scholar] [CrossRef]
- Hayashi, T.; Sumi, D.; Matsui-Hirai, H.; Fukatsu, A.; Arockia, J.; Rani, P.R.; Kano, H.; Tsunekawa, T.; Iguchi, A. Sarpogrelate HCl, a Selective 5-HT2A Antagonist, Retards the Progression of Atherosclerosis through a Novel Mechanism. Atherosclerosis 2003, 168, 23–31. [Google Scholar] [CrossRef]
- Kajiwara, I.; Soejima, H.; Miyamoto, S.; Ogawa, H. Effects of Additional Treatment of Sarpogrelate to Aspirin Therapy on Platelet Aggregation and Plasma Plasminogen Activator Inhibitor Activity in Patients with Stable Effort Angina. Thromb. Res. 2011, 128, 547–551. [Google Scholar] [CrossRef] [PubMed]
- Han, A.; Lee, T.; Lee, J.; Song, S.W.; Lee, S.S.; Jung, I.M.; Kang, J.M.; Gwon, J.G.; Yun, W.S.; Cho, Y.P.; et al. A Multicenter, Randomized, Open-Labelled, Non-Inferiority Trial of Sustained-Release Sarpogrelate versus Clopidogrel after Femoropopliteal Artery Intervention. Sci. Rep. 2023, 13, 2502. [Google Scholar] [CrossRef]
- Celermajer, D.S.; Sorensen, K.E.; Gooch, V.M.; Miller, O.I.; Sullivan, I.D.; Lloyd, J.K.; Deanfield, J.E.; Spiegelhalter, D.J. Non-Invasive Detection of Endothelial Dysfunction in Children and Adults at Risk of Atherosclerosis. Lancet 1992, 340, 1111–1115. [Google Scholar] [CrossRef]
- Resch, K.L.; Ernst, E.; Matrai, A.; Paulsen, H.F. Fibrinogen and viscosity as risk factors for subsequent cardiovascular events in stroke sruvivors. Ann. Intern. Med. 1992, 117, 371–375. [Google Scholar] [CrossRef]
- Lee, A.J.; Mowbray, P.I.; Lowe, G.D.O.; Rumley, A.; Fowkes, F.G.R.; Allan, P.L. Blood Viscosity and Elevated Carotid Intima-Media Thickness in Men and Women: The Edinburgh Artery Study. Circulation 1998, 97, 1467–1473. [Google Scholar] [CrossRef]
- Corretti, M.C.; Anderson, T.J.; Benjamin, E.J.; Celermajer, D.; Charbonneau, F.; Creager, M.A.; Deanfield, J.; Drexler, H.; Gerhard-Herman, M.; Herrington, D.; et al. Guidelines for the Ultrasound Assessment of Endothelial-Dependent Flow-Mediated Vasodilation of the Brachial Artery: A Report of the International Brachial Artery Reactivity Task Force. J. Am. Coll. Cardiol. 2002, 39, 257–265. [Google Scholar] [CrossRef] [PubMed]
- Ahn, Y.; Aung, N.; Ahn, H.S. A Comprehensive Review of Clinical Studies Applying Flow-Mediated Dilation. Diagnostics 2024, 14, 2499. [Google Scholar] [CrossRef] [PubMed]
- Shevkoplyas, S.S.; Yoshida, T.; Gifford, S.C.; Bitensky, M.W. Direct Measurement of the Impact of Impaired Erythrocyte Deformability on Microvascular Network Perfusion in a Microfluidic Device. Lab Chip 2006, 6, 914–920. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, Y.; Tateishi, N.; Soutani, M.; Maeda, N. Flow Behavior of Erythrocytes in Microvessels and Glass Capillaries: Effects of Erythrocyte Deformation and Erythrocyte Aggregation. Int. J. Microcirc. Exp. 1996, 16, 187–194. [Google Scholar] [CrossRef]
- Baskurt, O.K.; Meiselman, H.J. Erythrocyte Aggregation: Basic Aspects and Clinical Importance. Clin. Hemorheol. Microcirc. 2013, 53, 23–37. [Google Scholar] [CrossRef]
- Levy, B.I.; Schiffrin, E.L.; Mourad, J.J.; Agostini, D.; Vicaut, E.; Safar, M.E.; Struijker-Boudier, H.A.J. Impaired Tissue Perfusion a Pathology Common to Hypertension, Obesity, and Diabetes Mellitus. Circulation 2008, 118, 968–976. [Google Scholar] [CrossRef]
- Hara, H.; Kitajima, A.; Shimada, H.; Tamao, Y. Antithrombotic Effect of MCI-9042, a New Antiplatelet Agent on Experimental Thrombosis Models. Thromb. Haemost. 1991, 66, 484–488. [Google Scholar] [CrossRef]
- Yamashita, T.; Kitamori, K.; Hashimoto, M.; Watanabe, S.; Giddings, J.C.; Yamamoto, J. Conjunctive Effects of the 5HT2 Receptor Antagonist, Sarpogrelate, on Thrombolysis with Modified Tissue Plasminogen Activator in Different Laser-Induced Thrombosis Models. Haemostasis 2000, 30, 321–332. [Google Scholar] [CrossRef]
- Tamura, K.; Kanzaki, T.; Saito, Y.; Otabe, M.; Saito, Y.; Morisaki, N. Serotonin (5-Hydroxytryptamine, 5-HT) Enhances Migration of Rat Aortic Smooth Muscle Cells through 5-HT2 Receptors. Atherosclerosis 1997, 132, 139–143. [Google Scholar] [CrossRef]
- Shimokawa, H.; Vanhoutte, P.M. Angiographic Demonstration of Hyperconstriction Induced by Serotonin and Aggregating Platelets in Porcine Coronary Arteries with Regenerated Endothelium. J. Am. Coll. Cardiol. 1991, 17, 1197–1202. [Google Scholar] [CrossRef]
- Vikenes, K.; Farstad, M.; Nordrehaug, J.E. Serotonin Is Associated with Coronary Artery Disease and Cardiac Events. Circulation 1999, 100, 483–489. [Google Scholar] [CrossRef] [PubMed]
- Satoh, K.; Ozaki, Y.; Qi, R.; Yang, L.; Asazuma, N.; Yatomi, Y.; Kume, S. Factors That Affect the Size of Platelet Aggregates in Epinephrine-Induced Activation: A Study Using the Particle Counting Method Based upon Light Scattering. Thromb. Res. 1996, 81, 515–523. [Google Scholar] [CrossRef] [PubMed]
- Nemecek, G.M.; Coughlin, S.R.; Handley, D.A.; Moskowitz, M.A. Stimulation of Aortic Smooth Muscle Cell Mitogenesis by Serotonin. Proc. Natl. Acad. Sci. USA 1986, 83, 674–678. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.L.; Wang, W.W.; Moore, B.J.; Fanburg, B.L. Dual Effect of Serotonin on Growth of Bovine Pulmonary Artery Smooth Muscle Cells in Culture. Circ. Res. 1991, 68, 1362–1368. [Google Scholar] [CrossRef]
- Yum, K.S.; Kang, S.G.; Lee, J.W.; Cho, Y.I. Effects of Sarpogrelate on Blood Viscosity. Microvasc. Res. 2023, 145, 104439. [Google Scholar] [CrossRef]
- Miyazaki, M.; Higashi, Y.; Goto, C.; Chayama, K.; Yoshizumi, M.; Sanada, H.; Orihashi, K.; Sueda, T. Sarpogrelate Hydrochloride, a Selective 5-HT2A Antagonist, Improves Vascular Function in Patients with Peripheral Arterial Disease. J. Cardiovasc. Pharmacol. 2007, 49, 221–227. [Google Scholar] [CrossRef]
- Hasegawa, Y.; Suehiro, A.; Higasa, S.; Namba, M.; Kakishita, E. Enhancing Effect of Advanced Glycation End Products on Serotonin-Induced Platelet Aggregation in Patients with Diabetes Mellitus. Thromb. Res. 2002, 107, 319–323. [Google Scholar] [CrossRef]


| Combination Group | Monotherapy Group | Total | p-Value | ||
|---|---|---|---|---|---|
| N = 34 | N = 34 | N = 68 | |||
| Gender | Total, n (%) | 34 (100.00) | 34 (100.00) | 68 (100.00) | 0.7794 † |
| Male, n (%) | 25 (73.53) | 26 (76.47) | 51 (75.00) | ||
| Female, n (%) | 9 (26.47) | 8 (23.53) | 17 (25.00) | ||
| Age | n (%) | 34 (100.00) | 34 (100.00) | 68 (100.00) | 0.5796 * |
| Mean ± SD | 65.53 ± 6.45 | 66.65 ± 9.75 | 66.09 ± 8.23 | ||
| Median | 66.00 | 68.00 | 66.00 | ||
| Min, Max | 51.00, 76.00 | 34.00, 85.00 | 34.00, 85.00 | ||
| Age ranges separated by 10 years | 10s, n (%) | 0 (0.00) | 0 (0.00) | 0 (0.00) | 0.1059 †† |
| 20s, n (%) | 0 (0.00) | 0 (0.00) | 0 (0.00) | ||
| 30s, n (%) | 0 (0.00) | 1 (2.94) | 1 (1.47) | ||
| 40s, n (%) | 0 (0.00) | 0 (0.00) | 0 (0.00) | ||
| 50s, n (%) | 6 (17.65) | 7 (20.59) | 13 (19.12) | ||
| 60s, n (%) | 20 (58.82) | 11 (32.35) | 31 (45.59) | ||
| Above 70s, n (%) | 8 (23.53) | 15 (44.12) | 23 (33.82) | ||
| Pregnancy/breastfeeding status | Total, n (%) | 9 (26.47) | 8 (23.53) | 17 (25.00) | - |
| Yes, n (%) | 0 (0.00) | 0 (0.00) | 0 (0.00) | ||
| No, n (%) | 9 (26.47) | 8 (23.53) | 17 (25.00) | ||
| Fertility | Total, n (%) | 9 (26.47) | 8 (23.53) | 17 (25.00) | - |
| Yes, n (%) | 0 (0.00) | 0 (0.00) | 0 (0.00) | ||
| No, n (%) | 9 (26.47) | 8 (23.53) | 17 (25.00) | ||
| Smoking | Total, n (%) | 34 (100.00) | 34 (100.00) | 68 (100.00) | 0.0244 † |
| Never, n (%) | 8 (23.53) | 13 (38.24) | 21 (30.88) | ||
| Current smoker, n (%) | 4 (11.76) | 10 (29.41) | 14 (20.59) | ||
| Ex-smoker, n (%) | 22 (64.71) | 11 (32.35) | 33 (48.53) | ||
| Amount of smoking (cigarette/day) | n (%) | 25 (73.53) | 21 (61.76) | 46 (67.65) | 0.0498 ** |
| Mean ± SD | 16.92 ± 12.91 | 25.76 ± 20.88 | 20.96 ± 17.39 | ||
| Median | 13.00 | 20.00 | 20.00 | ||
| Min, Max | 2.00, 60.00 | 3.00, 100.00 | 2.00, 100.00 | ||
| Alcohol | Total, n (%) | 34 (100.00) | 34 (100.00) | 68 (100.00) | 0.8584 † |
| Never, n (%) | 11 (32.35) | 9 (26.47) | 20 (29.41) | ||
| Current, n (%) | 18 (52.94) | 20 (58.82) | 38 (55.88) | ||
| Past, n (%) | 5 (14.71) | 5 (14.71) | 10 (14.71) | ||
| Alcohol (g/week) | n (%) | 23 (67.65) | 25 (73.53) | 48 (70.59) | 0.7178 ** |
| Mean ± SD | 84.35 ± 45.31 | 98.20 ± 99.18 | 91.56 ± 77.67 | ||
| Median | 70.00 | 70.00 | 70.00 | ||
| Min, Max | 20.00, 140.00 | 10.00, 420.00 | 10.00, 420.00 | ||
| Height (cm) | n (%) | 34 (100.00) | 34 (100.00) | 68 (100.00) | 0.4112 * |
| Mean ± SD | 164.41 ± 6.85 | 162.85 ± 8.62 | 163.63 ± 7.77 | ||
| Median | 165.50 | 162.00 | 164.25 | ||
| Min, Max | 150.00, 177.00 | 138.00, 180.00 | 138.00, 180.00 | ||
| Weight (kg) | n (%) | 34 (100.00) | 34 (100.00) | 68 (100.00) | 0.5487 * |
| Mean ± SD | 70.56 ± 8.16 | 68.95 ± 13.26 | 69.75 ± 10.96 | ||
| Median | 72.00 | 69.90 | 70.00 | ||
| Min, Max | 55.00, 84.00 | 48.00, 98.50 | 48.00, 98.50 | ||
| BMI (kg/m2) | n (%) | 34 (100.00) | 34 (100.00) | 68 (100.00) | 0.7415 * |
| Mean ± SD | 26.11 ± 2.82 | 25.85 ± 3.64 | 25.98 ± 3.24 | ||
| Median | 25.65 | 26.10 | 25.95 | ||
| Min, Max | 21.10, 33.30 | 19.10, 34.50 | 19.10, 34.50 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ahn, Y.; Jang, J.; Bu, S.; Aung, N.; Ahn, H.-S.; Yum, K.-S. Study Design and Rationale of a Randomized Trial Comparing Aspirin–Sarpogrelate Combination Therapy with Aspirin Monotherapy: Effects on Blood Viscosity and Microcirculation in Cardiovascular Patients. Diagnostics 2025, 15, 1373. https://doi.org/10.3390/diagnostics15111373
Ahn Y, Jang J, Bu S, Aung N, Ahn H-S, Yum K-S. Study Design and Rationale of a Randomized Trial Comparing Aspirin–Sarpogrelate Combination Therapy with Aspirin Monotherapy: Effects on Blood Viscosity and Microcirculation in Cardiovascular Patients. Diagnostics. 2025; 15(11):1373. https://doi.org/10.3390/diagnostics15111373
Chicago/Turabian StyleAhn, Yuran, Jaehyuk Jang, Seonghyeon Bu, Nay Aung, Hyo-Suk Ahn, and Keun-Sang Yum. 2025. "Study Design and Rationale of a Randomized Trial Comparing Aspirin–Sarpogrelate Combination Therapy with Aspirin Monotherapy: Effects on Blood Viscosity and Microcirculation in Cardiovascular Patients" Diagnostics 15, no. 11: 1373. https://doi.org/10.3390/diagnostics15111373
APA StyleAhn, Y., Jang, J., Bu, S., Aung, N., Ahn, H.-S., & Yum, K.-S. (2025). Study Design and Rationale of a Randomized Trial Comparing Aspirin–Sarpogrelate Combination Therapy with Aspirin Monotherapy: Effects on Blood Viscosity and Microcirculation in Cardiovascular Patients. Diagnostics, 15(11), 1373. https://doi.org/10.3390/diagnostics15111373