
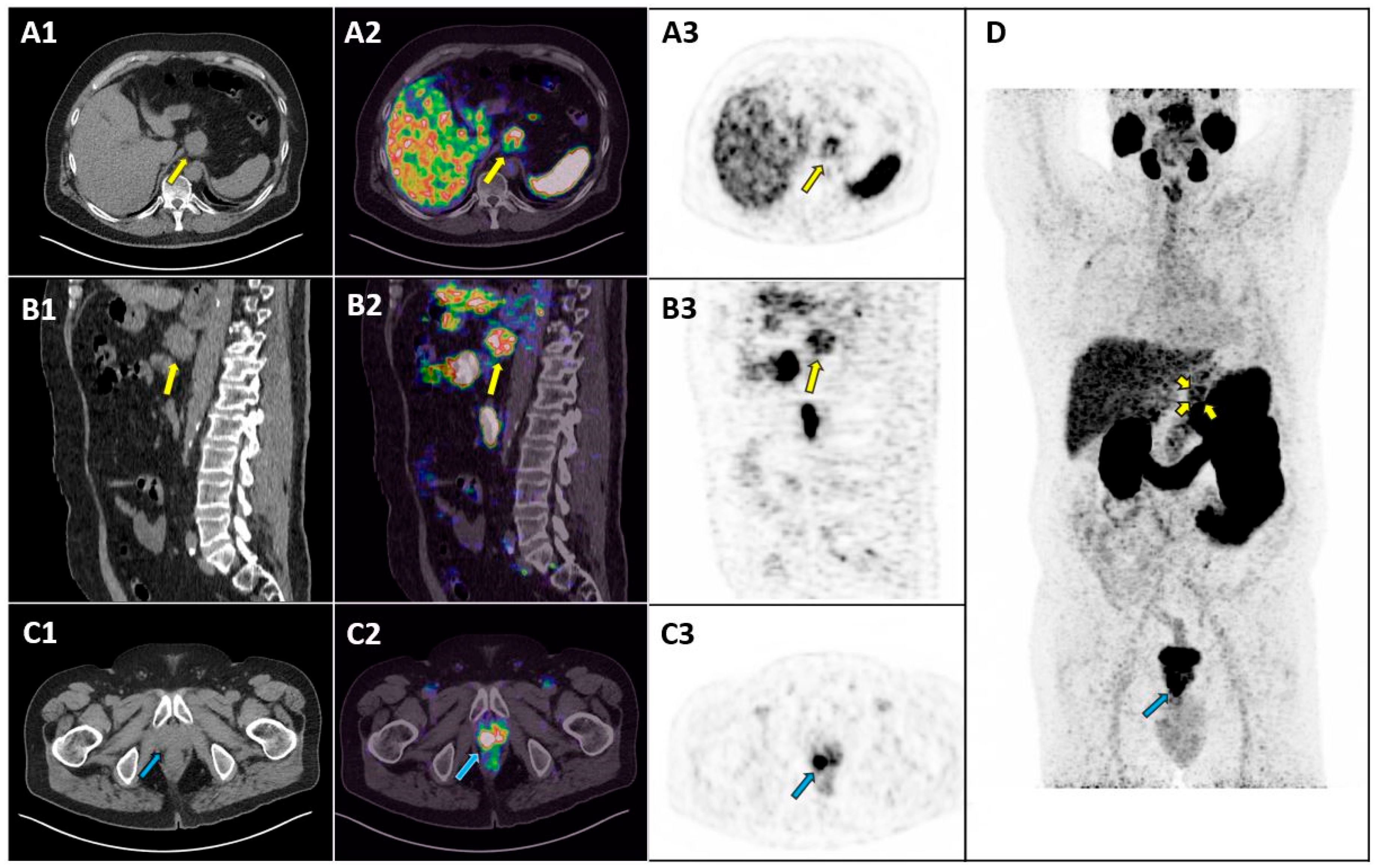
Gastric Adenocarcinoma Incidentally Detected by PET/CT with PSMA Ligands

 , ,
, ,  and
and 
{kind=link}
Abstract
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Oprea-Lager, D.E.; MacLennan, S.; Bjartell, A.; Briganti, A.; Burger, I.A.; de Jong, I.; De Santis, M.; Eberlein, U.; Emmett, L.; Fizazi, K.; et al. European Association of Nuclear Medicine Focus 5: Consensus on Molecular Imaging and Theranostics in Prostate Cancer. Eur. Urol. 2024, 85, 49–60. [Google Scholar] [CrossRef] [PubMed]
- Rizzo, A.; Dall’Armellina, S.; Pizzuto, D.A.; Perotti, G.; Zagaria, L.; Lanni, V.; Treglia, G.; Racca, M.; Annunziata, S. PSMA Radioligand Uptake as a Biomarker of Neoangiogenesis in Solid Tumours: Diagnostic or Theragnostic Factor? Cancers 2022, 14, 4039. [Google Scholar] [CrossRef] [PubMed]
- de Galiza Barbosa, F.; Queiroz, M.A.; Nunes, R.F.; Costa, L.B.; Zaniboni, E.C.; Marin, J.F.G.; Cerri, G.G.; Buchpiguel, C.A. Nonprostatic diseases on PSMA PET imaging: A spectrum of benign and malignant findings. Cancer Imaging 2020, 20, 23. [Google Scholar] [CrossRef] [PubMed]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Iacovitti, C.M.; Muoio, B.; Cuzzocrea, M.; Paone, G.; Treglia, G. Gastric Adenocarcinoma Incidentally Detected by PET/CT with PSMA Ligands. Diagnostics 2025, 15, 101. https://doi.org/10.3390/diagnostics15010101
Iacovitti CM, Muoio B, Cuzzocrea M, Paone G, Treglia G. Gastric Adenocarcinoma Incidentally Detected by PET/CT with PSMA Ligands. Diagnostics. 2025; 15(1):101. https://doi.org/10.3390/diagnostics15010101
Chicago/Turabian StyleIacovitti, Cesare Michele, Barbara Muoio, Marco Cuzzocrea, Gaetano Paone, and Giorgio Treglia. 2025. "Gastric Adenocarcinoma Incidentally Detected by PET/CT with PSMA Ligands" Diagnostics 15, no. 1: 101. https://doi.org/10.3390/diagnostics15010101
APA StyleIacovitti, C. M., Muoio, B., Cuzzocrea, M., Paone, G., & Treglia, G. (2025). Gastric Adenocarcinoma Incidentally Detected by PET/CT with PSMA Ligands. Diagnostics, 15(1), 101. https://doi.org/10.3390/diagnostics15010101