
The Impact of Sarcopenia in the Long-Term Survival of Patients following Complex Endovascular Aortic Surgery for Thoracoabdominal Aortic Aneurysms

 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
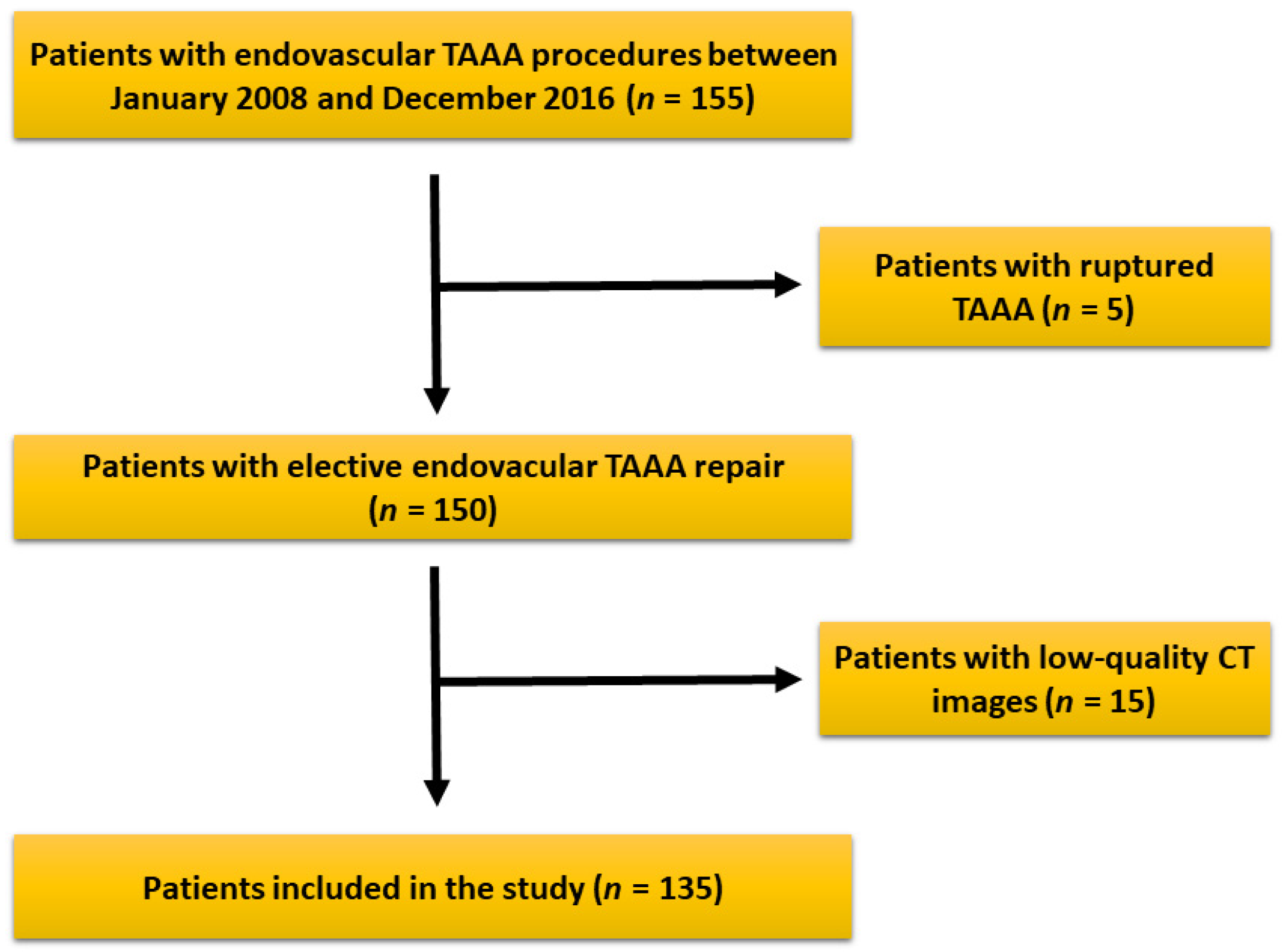
2.1. Patient Cohort
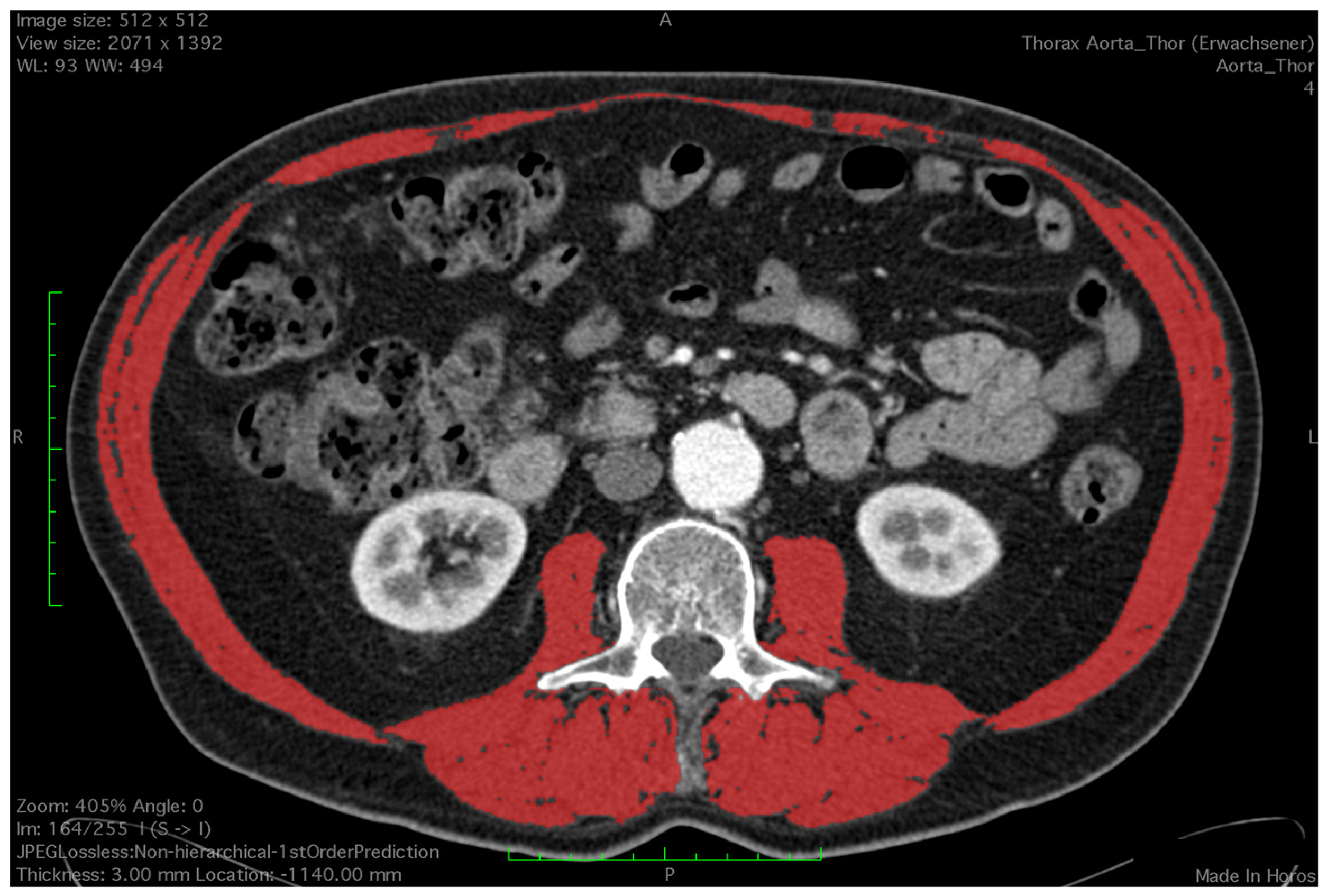
2.2. Assessment of Skeletal Muscle
2.3. Study Endpoints
2.4. Statistical Analysis
3. Results
3.1. Cohort Characteristics
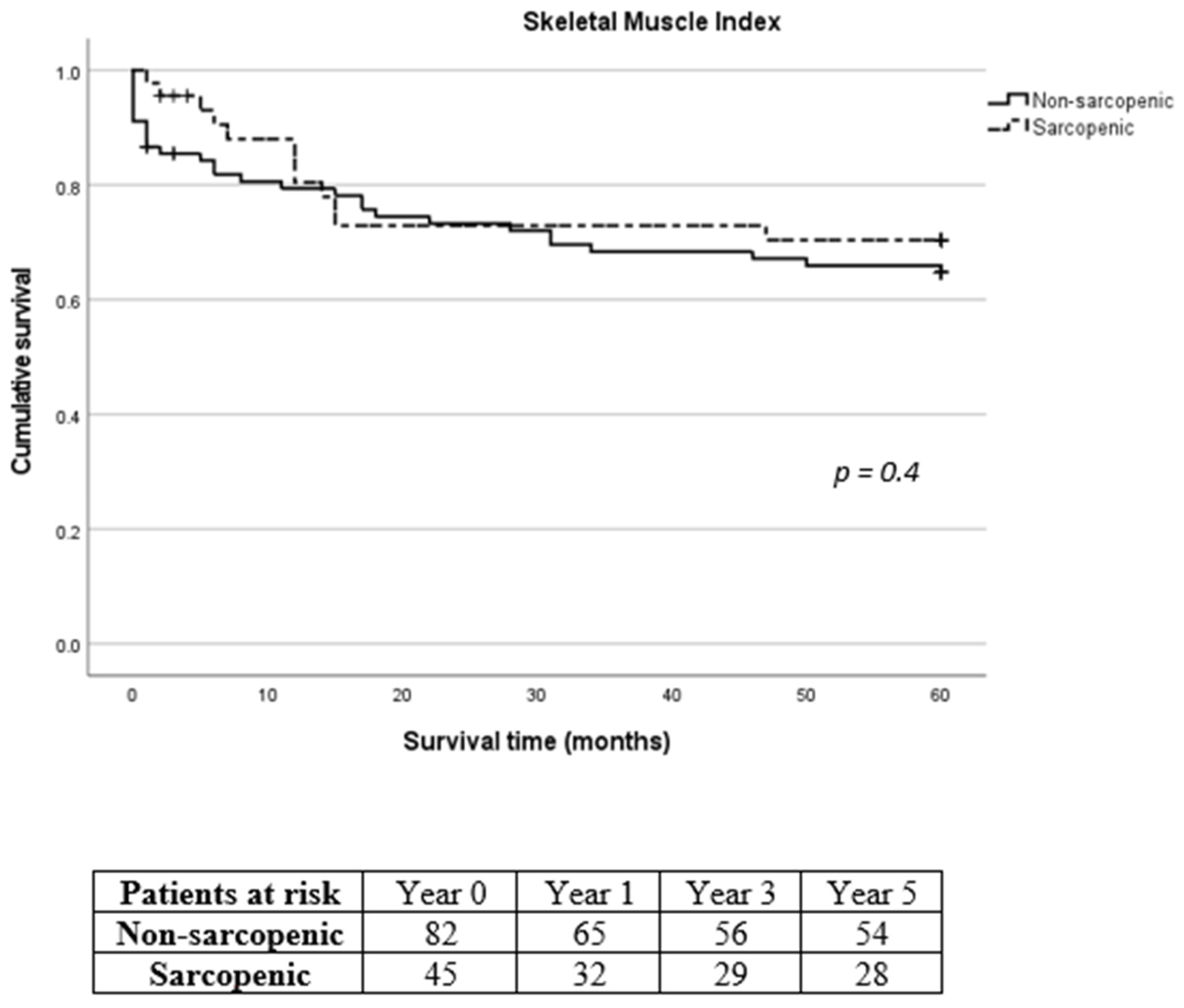
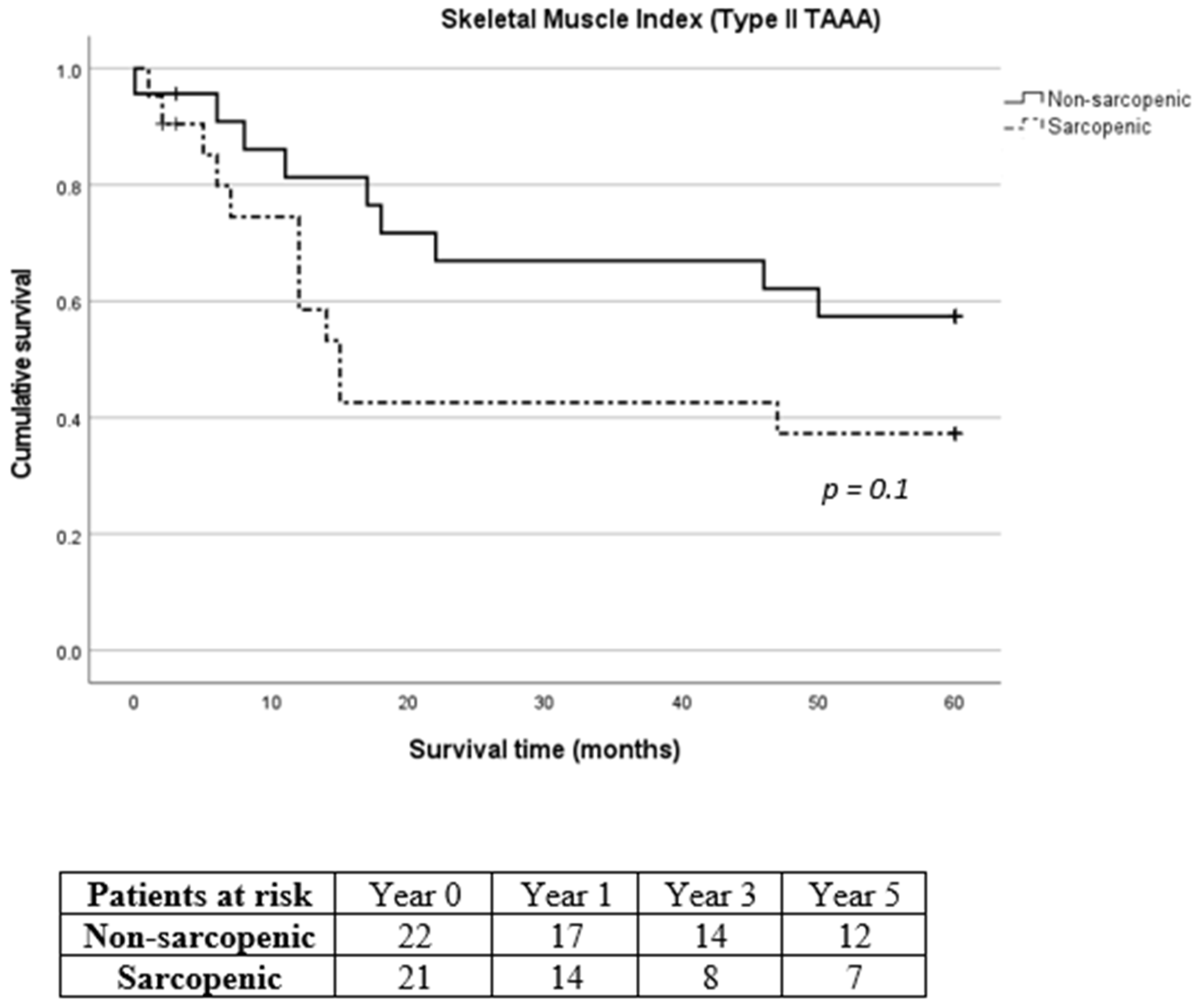
3.2. Primary Endpoints
3.3. Secondary Endpoints
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Santilli, V.; Bernetti, A.; Mangone, M.; Paoloni, M. Clinical definition of sarcopenia. Clin. Cases Miner. Bone Metab. 2014, 11, 177–180. [Google Scholar] [CrossRef]
- Sayer, A.A.; Syddall, H.; Martin, H.; Patel, H.; Baylis, D.; Cooper, C. The developmental origins of sarcopenia. J. Nutr. Health Aging 2008, 12, 427–432. [Google Scholar] [CrossRef]
- Manabe, T.; Ogawa, C.; Takuma, K.; Nakahara, M.; Oura, K.; Tadokoro, T.; Fujita, K.; Tani, J.; Shibatoge, M.; Morishita, A.; et al. Usefulness of the Measurement of Psoas Muscle Volume for Sarcopenia Diagnosis in Patients with Liver Disease. Diagnostics 2023, 13, 1245. [Google Scholar] [CrossRef] [PubMed]
- Tan, B.H.; Birdsell, L.A.; Martin, L.; Baracos, V.E.; Fearon, K.C. Sarcopenia in an overweight or obese patient is an adverse prognostic factor in pancreatic cancer. Clin. Cancer Res. 2009, 15, 6973–6979. [Google Scholar] [CrossRef]
- Jones, S.E.; Maddocks, M.; Kon, S.S.; Canavan, J.L.; Nolan, C.M.; Clark, A.L.; Man, W.D. Sarcopenia in COPD: Prevalence, clinical correlates and response to pulmonary rehabilitation. Thorax 2015, 70, 213–218. [Google Scholar] [CrossRef] [PubMed]
- Song, H.; Xiao, X.; Liu, G.; Zhou, J. Sarcopenia as a novel prognostic factor in the patients of primary localized gastrointestinal stromal tumor. BMC Cancer 2022, 22, 179. [Google Scholar] [CrossRef]
- Friedman, J.; Lussiez, A.; Sullivan, J.; Wang, S.; Englesbe, M. Implications of sarcopenia in major surgery. Nutr. Clin. Pract. 2015, 30, 175–179. [Google Scholar] [CrossRef]
- Denison, H.J.; Cooper, C.; Sayer, A.A.; Robinson, S.M. Prevention and optimal management of sarcopenia: A review of combined exercise and nutrition interentions to improve muscle outcomes in older people. Clin. Interv. Aging 2015, 10, 859–869. [Google Scholar] [PubMed]
- Indrakusuma, R.; Zijlmans, J.L.; Jalalzadeh, H.; Planken, R.N.; Balm, R.; Koelemay, M.J.W. Psoas Muscle Area as a Prognostic Factor for Survival in Patients with an Asymptomatic Infrarenal Abdominal Aortic Aneurysm: A Retrospective Cohort Study. Eur. J. Vasc. Endovasc. Surg. 2018, 55, 83–91. [Google Scholar] [CrossRef]
- Waduud, M.A.; Wood, B.; Keleabetswe, P.; Manning, J.; Linton, E.; Drozd, M.; Hammond, C.J.; Scott, D.J.A. Influence of psoas muscle area on mortality following elective abdominal aortic aneurysm repair. Br. J. Surg. 2019, 106, 367–374. [Google Scholar] [CrossRef]
- Hale, A.L.; Twomey, K.; Ewing, J.A.; Langan, E.M., 3rd; Cull, D.L.; Gray, B.H. Impact of sarcopenia on long-term mortality following endovascular aneurysm repair. Vasc. Med. 2016, 21, 217–222. [Google Scholar] [CrossRef] [PubMed]
- Chatterjee, S.; Shi, A.; Yoon, L.; Green, S.Y.; Zhang, Q.; Amarasekara, H.S.; Orozco-Sevilla, V.; Preventza, O.; LeMaire, S.A.; Coselli, J.S. Effect of sarcopenia on survival and spinal cord deficit outcomes after thoracoabdominal aortic aneurysm repair in patients 60 years of age and older. J. Thorac. Cardiovasc. Surg. 2023, 165, 1985–1996. [Google Scholar] [CrossRef]
- Ghaffarian, A.A.; Unangst, J.; Bartek, M.A.; Newhall, K.; Kang, P.C.; Shalhub, S.; Sweet, M.P. Sarcopenia predicts for long-term survival in patients with thoracoabdominal aortic aneurysms undergoing operative and nonoperative management. J. Vasc. Surg. 2022, 75, 343–347. [Google Scholar] [CrossRef] [PubMed]
- Pyun, A.J.; Ding, L.; Hong, Y.H.; Magee, G.A.; Tan, T.W.; Paige, J.K.; Weaver, F.A.; Han, S. Prospective assessment of dynamic changes in frailty and its impact on early clinical outcomes following physician-modified fenestrated-branched endovascular repair of complex abdominal and thoracoabdominal aortic aneurysms. J. Vasc. Surg. 2024, 79, 506–513.e1. [Google Scholar] [CrossRef] [PubMed]
- Mourtzakis, M.; Prado, C.; Lieffers, J.; Reinman, T.; McCargar, L.; Baracos, V.E. A practical and precise approach to quantification of body composition in cancer patients using computed tomography images acquired during routine care. Appl. Physiol. Nutr. Metab. 2008, 33, 997–1006. [Google Scholar] [CrossRef] [PubMed]
- Shen, W.; Punyanitya, M.; Wang, Z.; Gallagher, D.; St.-Onge, M.-P.; Albu, J.; Heymsfield, S.B.; Heshka, S. Total body skeletal muscle and adipose tissue volumes: Estimation from a single abdominal cross-sectional image. J. Appl. Phsyiol. 2004, 97, 2333–2338. [Google Scholar] [CrossRef] [PubMed]
- Dakis, K.; Nana, P.; Brodis, A.; Kouvelos, G.; Behrendt, C.-A.; Giannoukas, A.; Kölbel, T.; Spanos, K. Sarcopenia is a prognostic Biomarker for Long-Term Survival after Endovascular Aortic Aneurysm Repair: A Systematic Review and Meta-Analysis. Ann. Vasc. Surg. 2022, 2022, 358–368. [Google Scholar] [CrossRef] [PubMed]
- Kays, J.K.; Liang, T.W.; Zimmers, T.A.; Milgrom, D.P.; Abduljabar, H.; Young, A.; Kim, B.J.; Bell, T.M.; Fajardo, A.; Murphy, M.P.; et al. Sarcopenia is a Significant Predictor of Mortality After Abdominal Aortic Aneurysm Repair. JCSM Clin. Rep. 2018, 3, e00053. [Google Scholar] [CrossRef] [PubMed]
- Cheng, B.T.; Soult, M.C.; Helenowski, I.B.; Rodriguez, H.E.; Eskandari, M.K.; Joel, A.W. Sarcopenia predicts mortality and adverse outcomes after endovascular aneurysm repair and can be used to risk stratify patients. J. Vasc. Surg. 2019, 70, 1576–1584. [Google Scholar] [CrossRef]
- Nana, P.; Spanos, K.; Brotis, A.; Fabre, D.; Mastracci, T.; Haulon, S. Effect of Sarcopenia on Mortality and Spinal Cord Ischaemia After Complex Aortic Aneurysm Repair: Systematic Review and Meta-Analysis. Eur. J. Vasc. Endovasc. Surg. 2023, 65, 503–512. [Google Scholar] [CrossRef]
- Thurston, B.; Pena, G.N.; Howell, S.; Cowled, P.; Fitridge, R. Low total psoas area as scored in the clinic setting independently predicts midterm mortality after endovascular aneurysm repair in the male patients. J. Vasc. Surg. 2018, 67, 460–467. [Google Scholar] [CrossRef] [PubMed]
- Newton, D.H.; Kim, C.; Lee, N.; Wolfe, L.; Pfeifer, J.; Amendola, M. Sarcopenia predicts poor long-term survival in patients undergoing endovascular aortic aneurysm repair. J. Vasc. Surg. 2018, 67, 453–459. [Google Scholar] [CrossRef] [PubMed]
- Sündermann, S.H.; Bäck, C.; Bischoff-Ferrari, H.A.; Dehbi, H.M.; Szekely, A.; Völler, H.; Niebauer, J. Preinterventional frailty assessment in patients scheduled for cardiac surgery or transcatheter aortic valve implantation: A consensus statement of the European Association for Cardio-Thoracic Surgery (EACTS) and the European Association of Preventive Cardiology (EAPC) of the European Society of Cardiology (ECS). Eur. J. Cardiothorac. Surg. 2023, 64, ezad181. [Google Scholar]
- Cruz-Jentoft, A.J.; Bahat, G.; Bauer, J.; Boirie, Y.; Bruyere, O.; Cederholm, T.; Zamboni, M. Sarcopenia: Revised European consensus on definition and diagnosis. Age Ageing 2019, 48, 16–31. [Google Scholar] [CrossRef] [PubMed]
- Leong, D.P.; Teo, K.K.; Rangarajan, S.; Lopez-Jaramillo, P.; Avezum, A., Jr.; Orlandini, A. Prognostic value of grip strength: Findings from the Prospective Urban Rural Epidemiology (PURE) study. Lancet 2015, 386, 266–273. [Google Scholar] [CrossRef]
- Schaap, L.A.; Koster, A.; Visser, M. Adiposity, muscle mass, and muscle strength in relation to functional decline in older persons. Epidemiol. Rev. 2013, 35, 51–65. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Total No. (%) |
|---|---|
| Male/Female ratio | 86 (63.7%)/49 (36.3%) |
| Mean patient age (y.o ± SD) | 69.7 ± 8.6 |
| BMI (kg/m2 ± SD) | 26.9 ± 4.6 |
| ASA grading | |
| 17 (12.6%) |
| 104 (77%) |
| 14 (10.4%) |
| Type of TAAA | |
| 8 (5.9%) |
| 44 (32.6%) |
| 47 (34.8%) |
| 30 (22.2%) |
| 6 (4.4%) |
| Prior vascular surgery | 60 (44.4%) |
| 44 (32.6%) |
| 20(14.8%) |
| 5 (3.6%) |
| CAD | 59 (43.7%) |
| Hypertension | 129 (95.6%) |
| Stroke | 25 (18.5%) |
| COPD | 43 (31.9%) |
| Diabetes | 14 (10.4%) |
| Smoking | 56 (41.5%) |
| CKD | 53 (39.3%) |
| 40 (29.6%) |
| 13 (9.6%) |
| Variable | Skeletal Muscle Index (SMI) | Total Psoas Muscle Index (TPMI) | ||||
|---|---|---|---|---|---|---|
| Sarcopenic (n = 45) | Non Sarcopenic (n = 90) | p-Value | Sarcopenic (n = 45) | Non Sarcopenic (n = 90) | p-Value | |
| Male/Female ratio | 29 (64.4%)/16 (35.6%) | 57 (63.3%)/33 (36.7%) | 0.89 a | 29 (64.4%)/16 (35.6%) | 57 (63.3%)/33 (36.7%) | 0.89 a |
| Mean patient age (y.o ± SD) | 70.9 ± 8.5 | 69.1 ± 8.7 | 0.3 b | 70.6 ± 10.2 | 69.2 ± 7.7 | 0.15 b |
| BMI (kg/m2 ± SD) | 24.7 ± 4.2 | 28.1 ± 4.4 | 0.5 b | 24.9 ± 4.2 | 28 ± 4.4 | 0.39 b |
| ASA grading | 0.92 a | 0.34 a | ||||
| 5 (11.1%) | 12 (13.3%) | 3 (6.7%) | 14 (15.6%) | ||
| 35 (77.8%) | 69 (76.7%) | 37 (82.2%) | 67 (74.4%) | ||
| 5 (11.1%) | 9 (10%) | 5 (11.1%) | 9 (10%) | ||
| Type of TAAA | ||||||
| 1 (2.2%) | 7 (7.8%) | 0.19 c | 0 (0%) | 8 (8.9%) | 0.03c |
| 21 (46.7%) | 23 (25.6%) | 0.01a | 24 (53.3%) | 20 (22.2%) | <0.01a |
| 14 (31.1%) | 33 (36.7%) | 0.52 a | 13 (28.9%) | 34 (37.8%) | 0.3 a |
| 8 (17.8%) | 22 (24.4%) | 0.38 a | 7 (15.6%) | 23 (25.6%) | 0.18 a |
| 1 (2.2%) | 5 (5.6%) | 0.37 c | 1 (2.2%) | 5 (5.6%) | 0.37 c |
| Prior vascular surgery | 24 (53.3%) | 36 (40%) | 0.14 a | 25 (55.6%) | 35 (38.9%) | 0.66 a |
| 18 (40%) | 26 (28.9%) | 0.19 a | 19 (42.2%) | 25 (27.8%) | 0.91 a |
| 8 (17.8%) | 12 (13.3%) | 0.49 a | 6 (13.3%) | 14 (15.6%) | 0.73 a |
| 1 (2.2%) | 4 (4.4%) | 0.51 | 1 (2.2%) | 4 (4.4%) | 0.51 |
| CAD | 20 (44.4%) | 39 (43.3%) | 0.9 | 21 (46.7%) | 38 (42.2%) | 0.62 |
| Hypertension | 44 (97.8%) | 85 (94.4%) | 0.37 | 44 (97.8%) | 85 (94.4%) | 0.37 |
| Stroke | 11 (24.4%) | 14 (15.6%) | 0.21 | 11 (24.4%) | 14 (15.6%) | 0.21 |
| COPD | 14 (31.1%) | 29 (32.2%) | 0.89 | 13 (28.9%) | 30 (33.3%) | 0.6 |
| Diabetes | 6 (13.3%) | 8 (8.9%) | 0.42 | 4 (8.9%) | 10 (11.1%) | 0.69 |
| Smoking | 15 (33.3%) | 41 (45.6%) | 0.17 | 15 (33.3%) | 41 (45.6%) | 0.17 |
| CKD | 18 (40%) | 35 (38.9%) | 0.9 | 17 (37.8%) | 36 (40%) | 0.8 |
| 15 (33.3%) | 25 (27.8%) | 14 (31.1%) | 26 (28.9%) | ||
| 3 (6.7%) | 10 (11.1%) | 3 (6.7%) | 10 (11.1%) | ||
| Skeletal Muscle Index HR 1.77, 95% CI 0.86–3.6, p = 0.11 | Total Psoas Muscle Index HR 0.82, 95% CI 0.43–1.56, p = 0.55 | |||||
|---|---|---|---|---|---|---|
| Variable | HR | 95% CI | p-Value | HR | 95% CI | p-Value |
| Age | 1.07 | 1.02–1.12 | 0.003 | 1.08 | 1.02–1.12 | 0.003 |
| Body mass index | 0.93 | 0.86–1 | 0.07 | 0.95 | 0.89–1.02 | 0.2 |
| CAD | 0.73 | 0.37–1.43 | 0.36 | 0.7 | 0.36–1.34 | 0.28 |
| COPD | 0.62 | 0.31–1.24 | 0.18 | 0.63 | 0.32–1.25 | 0.18 |
| Diabetes | 0.95 | 0.32–2.84 | 0.93 | 1.03 | 0.35–3.07 | 0.94 |
| Smoking | 0.94 | 0.48–1.83 | 0.86 | 0.87 | 0.45–1.71 | 0.7 |
| CKD | 1.71 | 0.86–3.41 | 0.12 | 1.71 | 0.86–3.38 | 0.12 |
| Skeletal Muscle Index | Total Psoas Muscle Index | ||||||
|---|---|---|---|---|---|---|---|
| Postoperative Complications | Total No. (%) | Sarcopenic (n = 45) | Non-Sarcopenic (n = 90) | p Value | Sarcopenic (n = 45) | Non-Sarcopenic (n = 90) | p Value |
| MACE | 13 (9.6%) | 7 (15.6%) | 6 (6.7%) | 0.09 a | 6 (13.3%) | 7 (7.8%) | 0.3 a |
| Pulmonal | 28 (20.7%) | 12 (26.7%) | 16 (17.8%) | 0.23 a | 14 (31.3%) | 14 (15.6%) | 0.03a |
| AKI | 21 (15.6%) | 7 (15.6%) | 14 (15.6%) | 1 a | 9 (20%) | 12 (13.3%) | 0.45 a |
| Hemodialysis | 10 (7.4%) | 4 (8.9%) | 6 (6.7%) | 0.64 b | 5 (11.1%) | 5 (5.6%) | 0.24 b |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sachsamanis, G.; Stahl, J.; Pfister, K.; Schierling, W.; Betz, T.; Jage, S. The Impact of Sarcopenia in the Long-Term Survival of Patients following Complex Endovascular Aortic Surgery for Thoracoabdominal Aortic Aneurysms. Diagnostics 2024, 14, 751. https://doi.org/10.3390/diagnostics14070751
Sachsamanis G, Stahl J, Pfister K, Schierling W, Betz T, Jage S. The Impact of Sarcopenia in the Long-Term Survival of Patients following Complex Endovascular Aortic Surgery for Thoracoabdominal Aortic Aneurysms. Diagnostics. 2024; 14(7):751. https://doi.org/10.3390/diagnostics14070751
Chicago/Turabian StyleSachsamanis, Georgios, Judith Stahl, Karin Pfister, Wilma Schierling, Thomas Betz, and Simon Jage. 2024. "The Impact of Sarcopenia in the Long-Term Survival of Patients following Complex Endovascular Aortic Surgery for Thoracoabdominal Aortic Aneurysms" Diagnostics 14, no. 7: 751. https://doi.org/10.3390/diagnostics14070751
APA StyleSachsamanis, G., Stahl, J., Pfister, K., Schierling, W., Betz, T., & Jage, S. (2024). The Impact of Sarcopenia in the Long-Term Survival of Patients following Complex Endovascular Aortic Surgery for Thoracoabdominal Aortic Aneurysms. Diagnostics, 14(7), 751. https://doi.org/10.3390/diagnostics14070751