AI-Assisted X-ray Fracture Detection in Residency Training: Evaluation in Pediatric and Adult Trauma Patients

 , , ,
, , ,  , and
, and
Abstract
1. Introduction
2. Materials and Methods
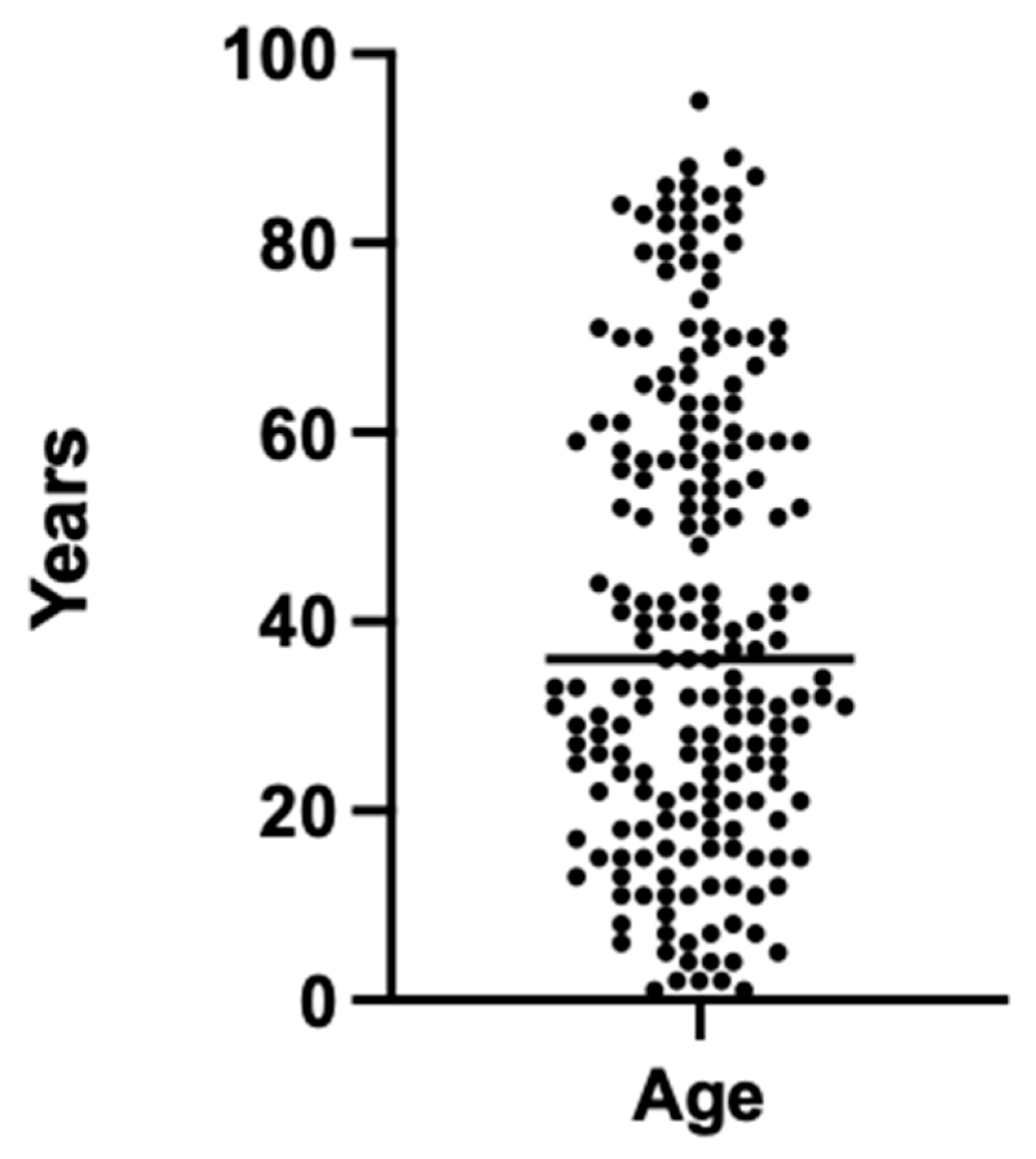
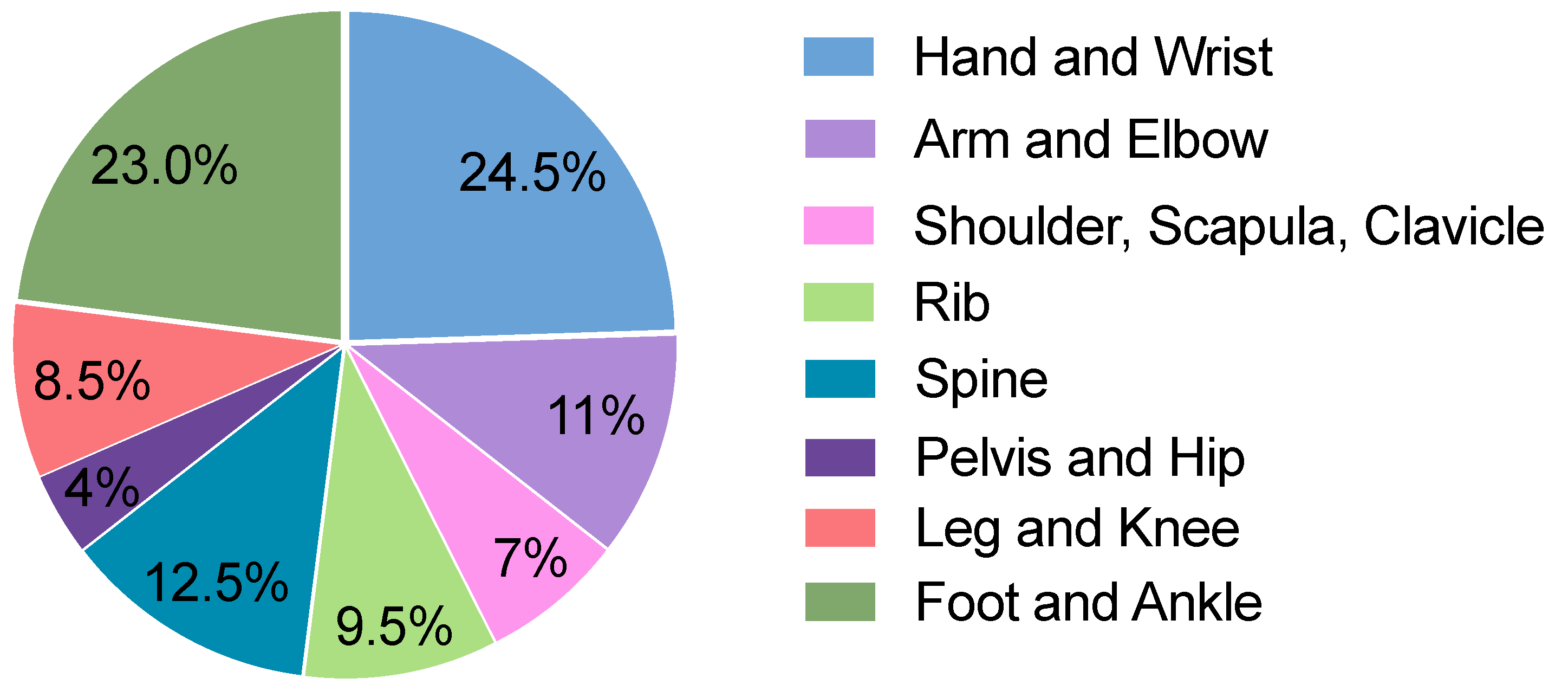
2.1. Study Population and Design
2.2. Ground Truth
2.3. Algorithm
2.4. Ethics Statement
2.5. Statistical Analysis
- True positive (TP): a fracture was detected when a fracture was present.
- False negative (FN): no fracture was detected when a fracture was present.
- False positive (FP): a fracture was detected when no fracture was present.
- True negative (TN): no fracture was detected when no fracture was present.
- Sensitivity: the proportion of true positive cases correctly identified as fractures by the radiology residents.
- Specificity: the proportion of true negative cases correctly identified as non-fractures by the radiology residents.
- Positive predictive value (PPV): the proportion of cases identified as fractures by the radiology residents that were confirmed as true fractures.
- Negative predictive value (NPV): the proportion of cases identified as non-fractures by the radiology residents that were confirmed as true non-fractures.
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Arasu, V.A.; Abujudeh, H.H.; Biddinger, P.D.; Noble, V.E.; Halpern, E.F.; Thrall, J.H.; Novelline, R.A. Diagnostic Emergency Imaging Utilization at an Academic Trauma Center from 1996 to 2012. J. Am. Coll. Radiol. 2015, 12, 467–474. [Google Scholar] [CrossRef] [PubMed]
- Lendrum, R.A.; Lockey, D.J. Trauma System Development. Anaesthesia 2013, 68, 30–39. [Google Scholar] [CrossRef] [PubMed]
- Regnard, N.-E.; Lanseur, B.; Ventre, J.; Ducarouge, A.; Clovis, L.; Lassalle, L.; Lacave, E.; Grandjean, A.; Lambert, A.; Dallaudière, B.; et al. Assessment of Performances of a Deep Learning Algorithm for the Detection of Limbs and Pelvic Fractures, Dislocations, Focal Bone Lesions, and Elbow Effusions on Trauma X-rays. Eur. J. Radiol. 2022, 154, 110447. [Google Scholar] [CrossRef] [PubMed]
- Canoni-Meynet, L.; Verdot, P.; Danner, A.; Calame, P.; Aubry, S. Added Value of an Artificial Intelligence Solution for Fracture Detection in the Radiologist’s Daily Trauma Emergencies Workflow. Diagn. Interv. Imaging 2022, 103, 594–600. [Google Scholar] [CrossRef]
- Harvey, H.B.; Tomov, E.; Babayan, A.; Dwyer, K.; Boland, S.; Pandharipande, P.V.; Halpern, E.F.; Alkasab, T.K.; Hirsch, J.A.; Schaefer, P.W.; et al. Radiology Malpractice Claims in the United States From 2008 to 2012: Characteristics and Implications. J. Am. Coll. Radiol. 2016, 13, 124–130. [Google Scholar] [CrossRef]
- Blüthgen, C.; Becker, A.S.; Vittoria de Martini, I.; Meier, A.; Martini, K.; Frauenfelder, T. Detection and Localization of Distal Radius Fractures: Deep Learning System versus Radiologists. Eur. J. Radiol. 2020, 126, 108925. [Google Scholar] [CrossRef]
- Xue, L.; Yan, W.; Luo, P.; Zhang, X.; Chaikovska, T.; Liu, K.; Gao, W.; Yang, K. Detection and Localization of Hand Fractures Based on GA_Faster R-CNN. Alex. Eng. J. 2021, 60, 4555–4562. [Google Scholar] [CrossRef]
- Kim, D.H.; MacKinnon, T. Artificial Intelligence in Fracture Detection: Transfer Learning from Deep Convolutional Neural Networks. Clin. Radiol. 2018, 73, 439–445. [Google Scholar] [CrossRef]
- Cheng, C.-T.; Ho, T.-Y.; Lee, T.-Y.; Chang, C.-C.; Chou, C.-C.; Chen, C.-C.; Chung, I.-F.; Liao, C.-H. Application of a Deep Learning Algorithm for Detection and Visualization of Hip Fractures on Plain Pelvic Radiographs. Eur. Radiol. 2019, 29, 5469–5477. [Google Scholar] [CrossRef]
- Chung, S.W.; Han, S.S.; Lee, J.W.; Oh, K.-S.; Kim, N.R.; Yoon, J.P.; Kim, J.Y.; Moon, S.H.; Kwon, J.; Lee, H.-J.; et al. Automated Detection and Classification of the Proximal Humerus Fracture by Using Deep Learning Algorithm. Acta Orthop. 2018, 89, 468–473. [Google Scholar] [CrossRef]
- Cohen, M.; Puntonet, J.; Sanchez, J.; Kierszbaum, E.; Crema, M.; Soyer, P.; Dion, E. Artificial Intelligence vs. Radiologist: Accuracy of Wrist Fracture Detection on Radiographs. Eur. Radiol. 2023, 33, 3974–3983. [Google Scholar] [CrossRef] [PubMed]
- Lindsey, R.; Daluiski, A.; Chopra, S.; Lachapelle, A.; Mozer, M.; Sicular, S.; Hanel, D.; Gardner, M.; Gupta, A.; Hotchkiss, R.; et al. Deep Neural Network Improves Fracture Detection by Clinicians. Proc. Natl. Acad. Sci. USA 2018, 115, 11591–11596. [Google Scholar] [CrossRef] [PubMed]
- Dupuis, M.; Delbos, L.; Veil, R.; Adamsbaum, C. External Validation of a Commercially Available Deep Learning Algorithm for Fracture Detection in Children. Diagn. Interv. Imaging 2022, 103, 151–159. [Google Scholar] [CrossRef] [PubMed]
- Duron, L.; Ducarouge, A.; Gillibert, A.; Lainé, J.; Allouche, C.; Cherel, N.; Zhang, Z.; Nitche, N.; Lacave, E.; Pourchot, A.; et al. Assessment of an AI Aid in Detection of Adult Appendicular Skeletal Fractures by Emergency Physicians and Radiologists: A Multicenter Cross-Sectional Diagnostic Study. Radiology 2021, 300, 120–129. [Google Scholar] [CrossRef]
- Guermazi, A.; Tannoury, C.; Kompel, A.J.; Murakami, A.M.; Ducarouge, A.; Gillibert, A.; Li, X.; Tournier, A.; Lahoud, Y.; Jarraya, M.; et al. Improving Radiographic Fracture Recognition Performance and Efficiency Using Artificial Intelligence. Radiology 2022, 302, 627–636. [Google Scholar] [CrossRef]
- Nguyen, T.; Maarek, R.; Hermann, A.-L.; Kammoun, A.; Marchi, A.; Khelifi-Touhami, M.R.; Collin, M.; Jaillard, A.; Kompel, A.J.; Hayashi, D.; et al. Assessment of an Artificial Intelligence Aid for the Detection of Appendicular Skeletal Fractures in Children and Young Adults by Senior and Junior Radiologists. Pediatr. Radiol. 2022, 52, 2215–2226. [Google Scholar] [CrossRef]
- Wu, Y.; Kirillov, A.; Massa, F.; Lo, W.-Y.; Girshick, R. Detectron2 2019. Available online: https://github.com/facebookresearch/detectron2 (accessed on 26 May 2023).
- Olczak, J.; Fahlberg, N.; Maki, A.; Razavian, A.S.; Jilert, A.; Stark, A.; Sköldenberg, O.; Gordon, M. Artificial Intelligence for Analyzing Orthopedic Trauma Radiographs. Acta Orthop. 2017, 88, 581–586. [Google Scholar] [CrossRef]
- Urakawa, T.; Tanaka, Y.; Goto, S.; Matsuzawa, H.; Watanabe, K.; Endo, N. Detecting Intertrochanteric Hip Fractures with Orthopedist-Level Accuracy Using a Deep Convolutional Neural Network. Skeletal. Radiol. 2019, 48, 239–244. [Google Scholar] [CrossRef]
- Yang, S.; Yin, B.; Cao, W.; Feng, C.; Fan, G.; He, S. Diagnostic Accuracy of Deep Learning in Orthopaedic Fractures: A Systematic Review and Meta-Analysis. Clin. Radiol. 2020, 75, 713.e17–713.e28. [Google Scholar] [CrossRef]
- Yoon, A.P.; Lee, Y.-L.; Kane, R.L.; Kuo, C.-F.; Lin, C.; Chung, K.C. Development and Validation of a Deep Learning Model Using Convolutional Neural Networks to Identify Scaphoid Fractures in Radiographs. JAMA Netw. Open 2021, 4, e216096. [Google Scholar] [CrossRef]
- Yamada, Y.; Maki, S.; Kishida, S.; Nagai, H.; Arima, J.; Yamakawa, N.; Iijima, Y.; Shiko, Y.; Kawasaki, Y.; Kotani, T.; et al. Automated Classification of Hip Fractures Using Deep Convolutional Neural Networks with Orthopedic Surgeon-Level Accuracy: Ensemble Decision-Making with Antero-Posterior and Lateral Radiographs. Acta Orthop. 2020, 91, 699–704. [Google Scholar] [CrossRef] [PubMed]
- Murata, K.; Endo, K.; Aihara, T.; Suzuki, H.; Sawaji, Y.; Matsuoka, Y.; Nishimura, H.; Takamatsu, T.; Konishi, T.; Maekawa, A.; et al. Artificial Intelligence for the Detection of Vertebral Fractures on Plain Spinal Radiography. Sci. Rep. 2020, 10, 20031. [Google Scholar] [CrossRef] [PubMed]
- Krogue, J.D.; Cheng, K.V.; Hwang, K.M.; Toogood, P.; Meinberg, E.G.; Geiger, E.J.; Zaid, M.; McGill, K.C.; Patel, R.; Sohn, J.H.; et al. Automatic Hip Fracture Identification and Functional Subclassification with Deep Learning. Radiol. Artif. Intell. 2020, 2, e190023. [Google Scholar] [CrossRef] [PubMed]
- Salhöfer, L.; Haubold, J.; Gutt, M.; Hosch, R.; Umutlu, L.; Meetschen, M.; Schuessler, M.; Forsting, M.; Nensa, F.; Schaarschmidt, B.M. The Importance of Educational Tools and a New Software Solution for Visualizing and Quantifying Report Correction in Radiology Training. Sci. Rep. 2024, 14, 1172. [Google Scholar] [CrossRef]
- Kalaria, A.D.; Filice, R.W. Comparison-Bot: An Automated Preliminary-Final Report Comparison System. J. Digit. Imaging 2016, 29, 325–330. [Google Scholar] [CrossRef]
- Sharpe, R.E.; Surrey, D.; Gorniak, R.J.T.; Nazarian, L.; Rao, V.M.; Flanders, A.E. Radiology Report Comparator: A Novel Method to Augment Resident Education. J. Digit. Imaging 2012, 25, 330–336. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Without AI Support | AI Supported | Difference | |
|---|---|---|---|
| Resident 1 | |||
| Sens (95% CI) | 81% (69–89) | 82% (72–89) | 1% |
| Spec (95% CI) | 82% (71–90) | 69% (56–79) | −13% |
| PPV (95% CI) | 81% (69–89) | 78% (68–85) | −3% |
| NPV (95% CI) | 82% (71–90) | 74% (61–84) | −8% |
| Resident 2 | |||
| Sens (95% CI) | 48% (36–61) | 70% (59–79) | 22% |
| Spec (95% CI) | 75% (64–84) | 77% (64–87) | 2% |
| PPV (95% CI) | 64% (49–76) | 82% (71–89) | 18% |
| NPV (95% CI) | 62% (51–72) | 64% (52–75) | 2% |
| Resident 3 | |||
| Sens (95% CI) | 57% (46–68) | 78% (65–86) | 21% |
| Spec (95% CI) | 78% (65–87) | 89% (79–95) | 11% |
| PPV (95% CI) | 79% (66–87) | 88% (77–94) | 9% |
| NPV (95% CI) | 56% (45–67) | 80% (68–88) | 24% |
| Resident 4 | |||
| Sens (95% CI) | 49% (38–60) | 79% (67–88) | 30% |
| Spec (95% CI) | 71% (58–81) | 81% (69–89) | 10% |
| PPV (95% CI) | 69% (56–80) | 79% (67–88) | 10% |
| NPV (95% CI) | 51% (40–62) | 81% (69–89) | 30% |
| Residents 1–4 | |||
| Sens (95% CI) | 58% (52–64) | 77% (72–82) | 19% |
| Spec (95% CI) | 77% (71–81) | 79% (73–84) | 2% |
| PPV (95% CI) | 74% (67–79) | 81% (76–86) | 7% |
| NPV (95% CI) | 62% (56–67) | 75% (69–80) | 13% |
| Residents without AI Support | Residents with AI Support | AI | |
|---|---|---|---|
| Sens (95% CI) | 58% (52–64) | 77% (72–82) | 93% (87–96) |
| Spec (95% CI) | 77% (71–81) | 79% (73–84) | 77% (69–84) |
| PPV (95% CI) | 74% (67–79) | 81% (76–86) | 83% (77–88) |
| NPV (95% CI) | 62% (56–67) | 75% (69–80) | 89% (82–94) |
| RIS | AI | Difference | |
|---|---|---|---|
| Sens (95% CI) | 85% (78–90) | 93% (87–96) | 8% |
| Spec (95% CI) | 83% (75–89) | 77% (69–84) | −6% |
| PPV (95% CI) | 86% (79–91) | 83% (77–88) | −3% |
| NPV (95% CI) | 82% (74–88) | 89% (82–94) | 7% |
| Reporting Time | Reporting Time | Confidence | Confidence | |
|---|---|---|---|---|
| AI Supported | without AI Support | AI Supported | without AI Support | |
| Resident 1 | 45.8 s | 48.6 s | 1.53 | 1.55 |
| Resident 2 | 26.6 s | 25.2 s | 1.64 | 1.52 |
| Resident 3 | 23.1 s | 28.9 s | 1.48 | 2.14 |
| Resident 4 | 23.1 s | 26.1 s | 1.36 | 1.59 |
| Residents 1–4 | 29.6 s ± 19.8 s | 32.2 s ± 20.8 s | 1.53 ± 0.91 | 1.72 ± 1.02 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Meetschen, M.; Salhöfer, L.; Beck, N.; Kroll, L.; Ziegenfuß, C.D.; Schaarschmidt, B.M.; Forsting, M.; Mizan, S.; Umutlu, L.; Hosch, R.; et al. AI-Assisted X-ray Fracture Detection in Residency Training: Evaluation in Pediatric and Adult Trauma Patients. Diagnostics 2024, 14, 596. https://doi.org/10.3390/diagnostics14060596
Meetschen M, Salhöfer L, Beck N, Kroll L, Ziegenfuß CD, Schaarschmidt BM, Forsting M, Mizan S, Umutlu L, Hosch R, et al. AI-Assisted X-ray Fracture Detection in Residency Training: Evaluation in Pediatric and Adult Trauma Patients. Diagnostics. 2024; 14(6):596. https://doi.org/10.3390/diagnostics14060596
Chicago/Turabian StyleMeetschen, Mathias, Luca Salhöfer, Nikolas Beck, Lennard Kroll, Christoph David Ziegenfuß, Benedikt Michael Schaarschmidt, Michael Forsting, Shamoun Mizan, Lale Umutlu, René Hosch, and et al. 2024. "AI-Assisted X-ray Fracture Detection in Residency Training: Evaluation in Pediatric and Adult Trauma Patients" Diagnostics 14, no. 6: 596. https://doi.org/10.3390/diagnostics14060596
APA StyleMeetschen, M., Salhöfer, L., Beck, N., Kroll, L., Ziegenfuß, C. D., Schaarschmidt, B. M., Forsting, M., Mizan, S., Umutlu, L., Hosch, R., Nensa, F., & Haubold, J. (2024). AI-Assisted X-ray Fracture Detection in Residency Training: Evaluation in Pediatric and Adult Trauma Patients. Diagnostics, 14(6), 596. https://doi.org/10.3390/diagnostics14060596