According to the Global Cancer Observatory, ovarian cancer is the eighth most common cancer in women, with 313.959 new cases and 207.252 new deaths worldwide in 2020 [
1]. In Italy, 5370 new cases and 3285 deaths were registered last year [
1]. Most cases, around 75% [
2], are diagnosed in advanced stages, thus making ovarian cancer a particularly lethal disease, named the “big silent killer”. This happens because of its rapid spread through the peritoneal surface, but also because of the lack of valid screening programs, in contrast to other gynecological diseases. For example, cervical cancer has finally become a preventable cancer nowadays, thanks to the Papanicolaou screening test, the Human Papilloma Virus (HPV) vaccination, and other effective interventions [
3]. Ultrasound and hysteroscopy are of paramount importance for the prevention and early detection of endometrial cancer, along with serum biomarkers CA125 and HE4, which could help in the diagnosis. Conversely, no method is really effective in detecting ovarian cancer at early stages, and its prognosis remains poor. Not even its signs and symptoms are reliable since they occur when the disease has already spread. In clinical practice, clinical examination, transvaginal ultrasound (US), and serum biomarkers, such as Carbohydrate Antigen 125 (CA125) and Human Epididymis Protein 4 (HE4) dosage, are used to investigate the presence of ovarian cancer (OC), with a sensitivity of 88% and 95% and a specificity of 84% and 76% respectively, but these data are not enough, and several early stages are missed [
4,
5,
6,
7]. The aim of transvaginal ultrasound is to observe both ovaries, calculate their volume, and report the presence of abnormal lesions. Any variation in morphology or increase in volume or vascularization needs to be further explored [
7]. Unfortunately, ultrasounds are extremely operator-dependent, and while CA125 may be elevated in OC, it may also be elevated in endometriosis or other benign diseases and thus has a low specificity [
5]. HE4 reaches a specificity of 86% [
5,
8,
9], and it is usually dosed with CA125. HE4 is approved by the Food and Drug Administration in the United States as a reliable tumor biomarker for ovarian cancer. Nonetheless, HE4 can also be elevated in renal diseases, and this again reduces its specificity. Therefore, it is clear that all these methods have several limitations; as a consequence, the great challenge now is to find an effective screening test for OC and develop a strong prevention. Many scientists have recently focused their attention on volatile organic compounds (VOCs). These are gaseous molecules easily collected from the breath because they pass from the bloodstream into the lungs and also from the blood into the urine. They might provide interesting information on several diseases, such as renal dysfunctions, asthma, and solid tumors [
10,
11,
12,
13,
14,
15]. The original idea was born in 2008: several studies by Horvath et al. demonstrated that human ovarian cancer has a specific odor that can be detected by a trained dog. In addition, the same dog was able to distinguish among several histopathological types and grades, as well as healthy control samples, with a sensitivity of 100% both in tissue and in blood tests and a specificity of 95% and 98% in tissue and blood tests, respectively. Unfortunately, dogs are not suitable for clinical practice [
16,
17,
18]. Based on their discovery, Horvath et al. used an electronic nose that can accomplish the same task, with a sensitivity of 84.4% and a specificity of 86.8% in tissue tests [
16,
17,
18]. This electronic nose was a combination of four gas sensors, operating at different temperatures, made of metal oxide to better differentiate between various gases. The nose produces some signals, which are reduced to numbers and analyzed through the Weka algorithm package [
16,
17,
18]. At our university, Campus Bio-Medico of Rome, a new ongoing study is using the sensor array analysis (e-nose) to detect lung cancers, while a similar study on prostate cancer has already been published [
19]. The potential use of the e-nose has been tested in several other solid tumors, for example, in colorectal cancer [
12,
13,
20,
21], lung cancer [
11,
22], and breast cancer [
23]. Regarding ovarian cancer, there are at least a couple of articles to be mentioned. Haick et al., in 2014 [
24,
25], published a pilot study that aimed to detect ovarian cancer through exhaled breath samples. The nanoarray measured volatile organic compounds with a good sensitivity (79%) and a 100% specificity in detecting patients with ovarian cancer vs. controls. It also discriminated between early and advanced ovarian cancers with good accuracy. Inspired by these previous studies [
16,
17,
18,
26,
27], Raspagliesi et al. [
26] published in 2020 a prospective study demonstrating the ability of the e-nose to discriminate between breath samples from patients with ovarian cancer and controls. In addition, it identified four sensors involved in ovarian cancer detection that were also able to discriminate between early-stage and advanced-stage ovarian cancer [
26]. Along with the e-nose, another important discovery was the electronic tongue. The operating mechanism is similar. The e-tongue is a sensor array that produces an electrical response according to the material tasted, which serves as a fingerprint for the analyzed sample. This tool was used for various applications, first to classify food, wine, and milk or to detect impurities or pollutants in water [
27]. Then, its use was extended to detect other diseases including tumors, and it was tested on urine samples from male patients with bladder cancer [
28]. This study, by Lvova et al., suggested that the e-tongue could discriminate tumor samples from controls. However, the numbers were too low though (17 cancers and 10 controls), so further research was needed [
28]. In 2016, Pascual et al. introduced the usage of the e-tongue to detect patients with prostate cancer. This tool recognized an electrochemical fingerprint in urine samples with a sensitivity of 91% and a specificity of 73% [
29]. In particular, the e-tongue correctly classified 20 out of 22 samples of patients with prostate cancer and 11 out of 15 samples of controls. [
29] This specificity and sensibility were even higher than the prostate-specific antigen (PSA) test in blood, which was the main procedure to detect prostate cancer up to now. The PSA sensitivity and specificity are 34.9% and 63.1% respectively, when using a 4.0 ng/mL cutoff value [
30]. The e-tongue used by Pascual was an array of seven metal wire electrodes housed inside a steel cylinder. A Large Amplitude Pulse Voltammetry (LAPV) waveform was applied to each electrode, and the resulting currents versus time profile for each electrode was measured [
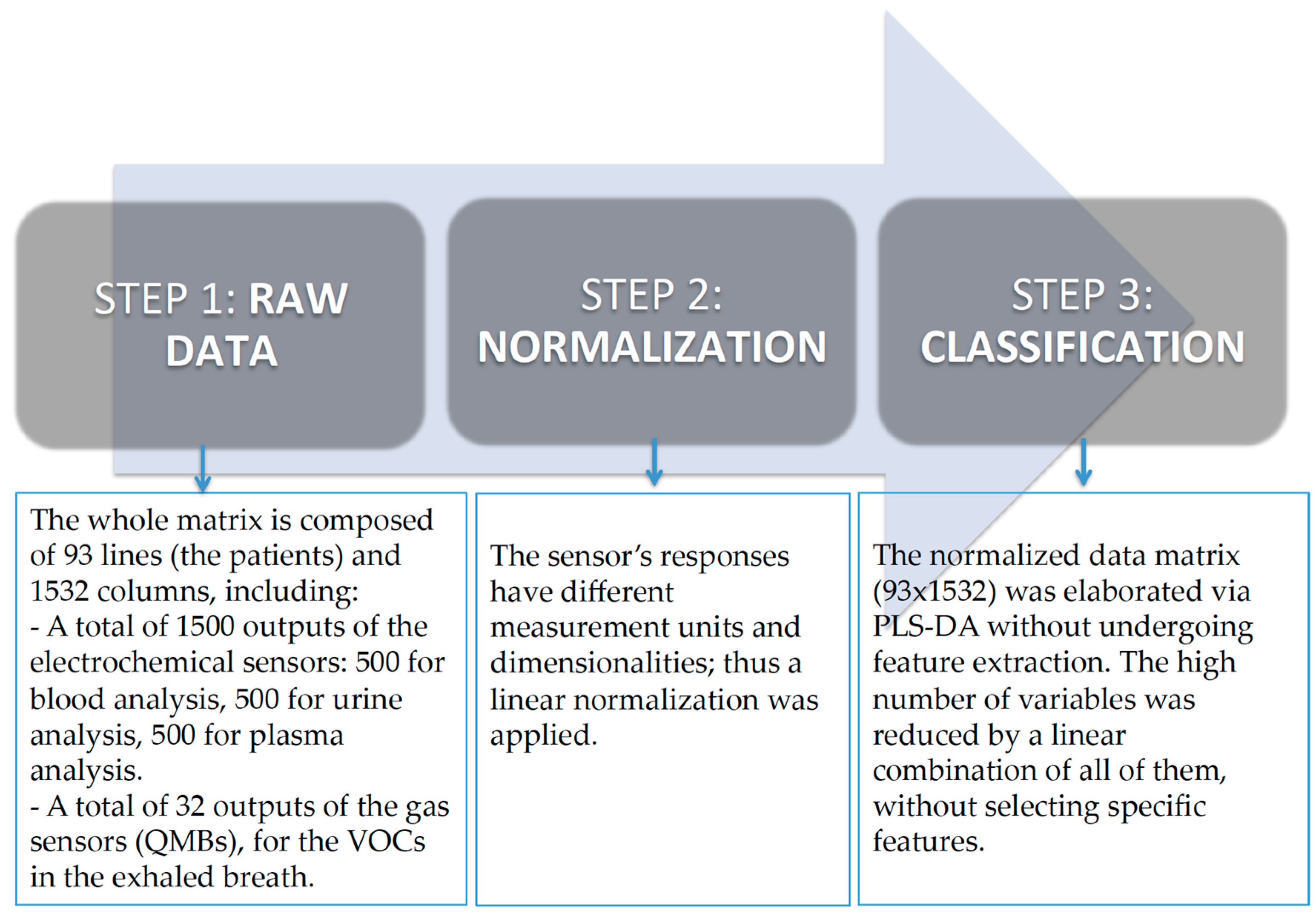
29]. Therefore, the e-tongue has been tested on urine samples from bladder and prostate cancer, as already mentioned, but it has never been tested on urine samples from ovarian cancer patients up to now. For the very first time in literature, we tested the e-tongue in this field. In our study, the electronic tongue was used not only on urine samples but also on blood and plasma samples from ovarian cancer women. In addition, we collected breath samples from the same patients to be analyzed by the electronic nose. To sum up, we merged the e-tongue data (made of 1500 sensors divided into three blocks of 500) with the e-nose data (made of 32 sensors) to increase the sensitivity and specificity for better detection of ovarian cancer. As a secondary endpoint, we correlated the fingerprints obtained from the e-nose and e-tongue with Carbohydrate Antigen 125 (CA125) and Human Epididymis Protein 4 (HE4) serum biomarkers collected before the surgical operation. This is also a first in the field of sensor arrays.




 ,
, 



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}