

The Surgical Treatment of Infective Endocarditis: A Comprehensive Review

 ,
, 
 , ,
, ,  ,
, 
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
2. Materials and Methods
3. Results
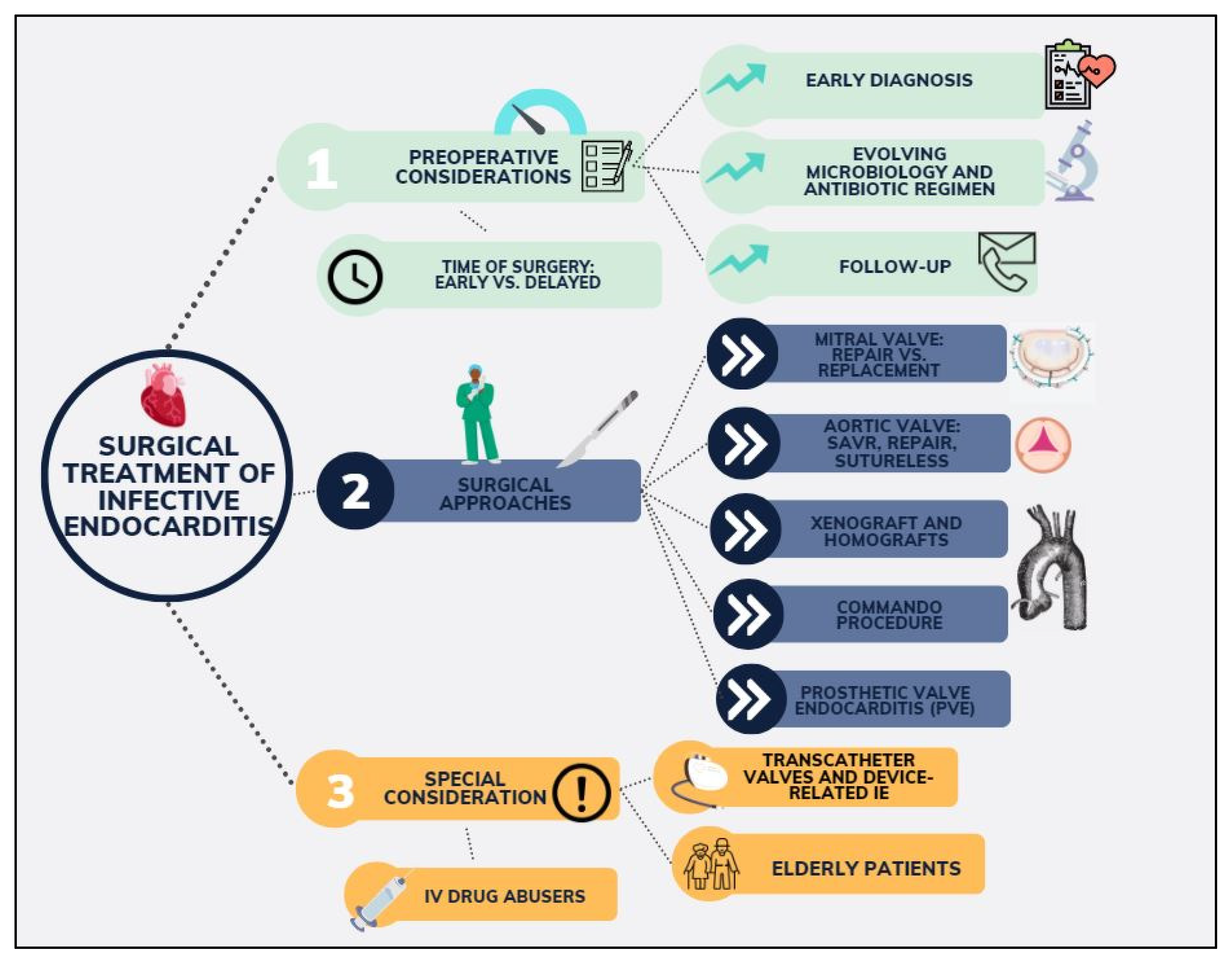
3.1. Preoperative Considerations
3.1.1. Treating the Patient, Not the Disease: Aetiology, Diagnosis, Antimicrobial Treatment, and Follow-Up
3.1.2. Shifting Microbiology in IE
3.1.3. Time of Surgery
3.2. Surgical Approaches to Infective Endocarditis
3.2.1. Isolated Valve: Valve Repair or Replacement?
Mitral Valve
Aortic Valve
3.2.2. Sutureless Valves: An Option Yet to Explore
3.2.3. Aortic Homograft in IE
3.2.4. Stentless Xenografts for IE
3.2.5. Extensive Aortic Root or Mitral Valve Infective Endocarditis: Commando
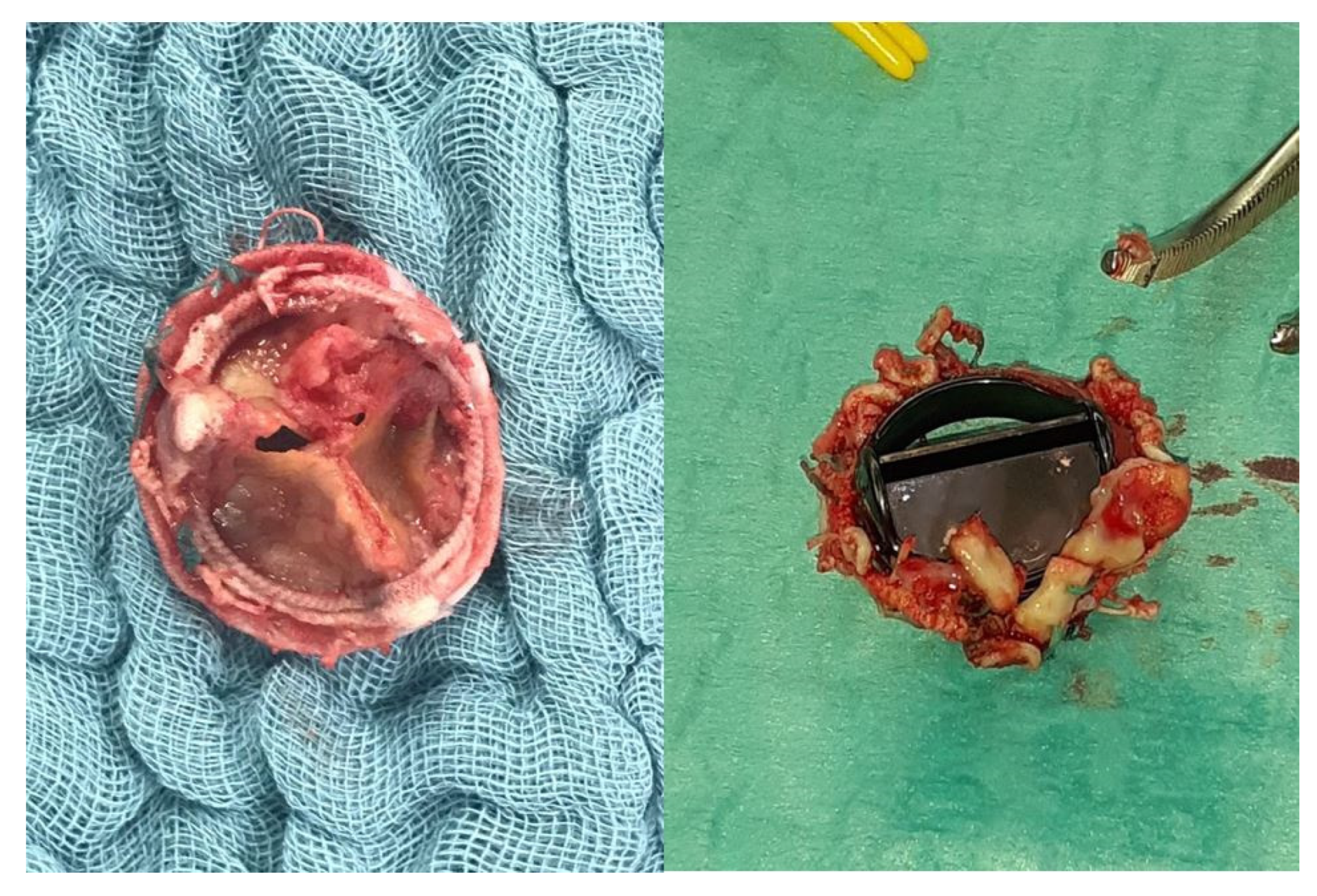
3.2.6. Prosthetic Valve Endocarditis
Transcatheter Valves, New Friends to an Old Problem for Cardiac Surgeons
Cardiac Implantable Electronic Devices Infective Endocarditis
3.3. Considerations in High-Risk Groups
3.3.1. IV Drug Abusers
3.3.2. Surgery in the Elderly
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Dayer, M.J.; Jones, S.; Prendergast, B.; Baddour, L.M.; Lockhart, P.B.; Thornhill, M.H. Incidence of infective endocarditis in England, 2000–13: A secular trend, interrupted time-series analysis. Lancet 2015, 385, 1219–1228. [Google Scholar] [CrossRef]
- Prendergast, B.D.; Tornos, P. Surgery for infective endocarditis: Who and when? Circulation 2010, 121, 1141–1152. [Google Scholar] [CrossRef]
- Mylonakis, E.; Calderwood, S.B. Infective Endocarditis in Adults. N. Engl. J. Med. 2001, 345, 1318–1330. [Google Scholar] [CrossRef] [PubMed]
- Habib, G.; Lancellotti, P.; Antunes, M.J.; Bongiorni, M.G.; Casalta, J.-P.; Del Zotti, F.; Dulgheru, R.; El Khoury, G.; Erba, P.A.; Iung, B.; et al. 2015 ESC Guidelines for the management of infective endocarditis: The Task Force for the Management of Infective Endocarditis of the European Society of Cardiology (ESC). Endorsed by: European Association for Cardio-Thoracic Surgery (EACTS), the European Association of Nuclear Medicine (EANM). Eur. Heart J. 2015, 36, 3075–3128. [Google Scholar] [CrossRef] [PubMed]
- Pettersson, G.B.; Coselli, J.S.; Hussain, S.T.; Griffin, B.; Blackstone, E.H.; Gordon, S.M.; LeMaire, S.A.; Woc-Colburn, L.E. 2016 The American Association for Thoracic Surgery (AATS) consensus guidelines: Surgical treatment of infective endocarditis: Executive summary. J. Thorac. Cardiovasc. Surg. 2017, 153, 1241–1258.e29. [Google Scholar] [CrossRef] [PubMed]
- Habib, G.; Lancellotti, P.; Erba, P.-A.; Sadeghpour, A.; Meshaal, M.; Sambola, A.; Furnaz, S.; Citro, R.; Ternacle, J.; Donal, E.; et al. The ESC-EORP EURO-ENDO (European Infective Endocarditis) registry. Eur. Heart J. Qual. Care Clin. Outcomes 2019, 5, 202–207. [Google Scholar] [CrossRef] [PubMed]
- Jensen, A.D.; Østergaard, L.; Petersen, J.K.; Graversen, P.; Butt, J.H.; Bundgaard, H.; Moser, C.; Smerup, M.H.; Modrau, I.S.; Iversen, K.; et al. Surgical treatment of patients with infective endocarditis: Changes in temporal use, patient characteristics, and mortality—A nationwide study. BMC Cardiovasc. Disord. 2022, 22, 338. [Google Scholar] [CrossRef] [PubMed]
- Pettersson, G.B.; Hussain, S.T. Current AATS guidelines on surgical treatment of infective endocarditis. Ann. Cardiothorac. Surg. 2019, 8, 630–644. [Google Scholar] [CrossRef] [PubMed]
- Butchart, E.G.; Gohlke-Bärwolf, C.; Antunes, M.J.; Tornos, P.; De Caterina, R.; Cormier, B.; Prendergast, B.; Iung, B.; Bjornstad, H.; Leport, C.; et al. Recommendations for the management of patients after heart valve surgery. Eur. Heart J. 2005, 26, 2463–2471. [Google Scholar] [CrossRef]
- Holland, T.L.; Baddour, L.M.; Bayer, A.S.; Hoen, B.; Miro, J.M.; Fowler, V.G., Jr. Infective endocarditis. Nat. Rev. Dis. Primers 2016, 2, 16059. [Google Scholar] [CrossRef]
- Fournier, P.; Thuny, F.; Richet, H.; Lepidi, H.; Casalta, J.; Arzouni, J.; Maurin, M.; Célard, M.; Mainardi, J.; Caus, T.; et al. Comprehensive Diagnostic Strategy for Blood Culture–Negative Endocarditis: A Prospective Study of 819 New Cases. Clin. Infect. Dis. 2010, 51, 131–140. [Google Scholar] [CrossRef]
- Østergaard, L.; Voldstedlund, M.; Bruun, N.E.; Bundgaard, H.; Iversen, K.; Køber, N.; Christensen, J.J.; Rosenvinge, F.S.; Jarløv, J.O.; Moser, C.; et al. Temporal Changes, Patient Characteristics, and Mortality, According to Microbiological Cause of Infective Endocarditis: A Nationwide Study. J. Am. Heart Assoc. 2022, 11, e025801. [Google Scholar] [CrossRef]
- Revilla, A.; López, J.; Vilacosta, I.; Villacorta, E.; Rollán, M.J.; Echevarría, J.R.; Carrascal, Y.; Di Stefano, S.; Fulquet, E.; Rodríguez, E.; et al. Clinical and prognostic profile of patients with infective endocarditis who need urgent surgery. Eur. Heart J. 2007, 28, 65–71. [Google Scholar] [CrossRef]
- Nadji, G.; Rusinaru, D.; Rémadi, J.; Jeu, A.; Sorel, C.; Tribouilloy, C. Heart failure in left-sided native valve infective endocarditis: Characteristics, prognosis, and results of surgical treatment. Eur. J. Heart Fail. 2009, 11, 668–675. [Google Scholar] [CrossRef]
- Richardson, J.V.; Karp, R.B.; Kirklin, J.W.; Dismukes, W.E. Treatment of infective endocarditis: A 10-year comparative analysis. Circulation 1978, 58, 589–597. [Google Scholar] [CrossRef]
- Thuny, F.; Avierinos, J.-F.; Tribouilloy, C.; Giorgi, R.; Casalta, J.-P.; Milandre, L.; Brahim, A.; Nadji, G.; Riberi, A.; Collart, F.; et al. Impact of cerebrovascular complications on mortality and neurologic outcome during infective endocarditis: A prospective multicentre study. Eur. Heart J. 2007, 28, 1155–1161. [Google Scholar] [CrossRef]
- Kang, D.-H.; Kim, Y.-J.; Kim, S.-H.; Sun, B.J.; Kim, D.-H.; Yun, S.-C.; Song, J.-M.; Choo, S.J.; Chung, C.-H.; Song, J.-K.; et al. Early Surgery versus Conventional Treatment for Infective Endocarditis. N. Engl. J. Med. 2012, 366, 2466–2473. [Google Scholar] [CrossRef]
- Gillinov, A.M.; Blackstone, E.H.; Nowicki, E.R.; Slisatkorn, W.; Al-Dossari, G.; Johnston, D.R.; George, K.M.; Houghtaling, P.L.; Griffin, B.; Sabik, J.F.; et al. Valve repair versus valve replacement for degenerative mitral valve disease. J. Thorac. Cardiovasc. Surg. 2008, 135, 885–893.e2. [Google Scholar] [CrossRef]
- Arjomandi Rad, A.; Naruka, V.; Vardanyan, R.; Viviano, A.; Salmasi, M.Y.; Magouliotis, D.; Kendall, S.; Casula, R.; Athanasiou, T. Mitral and tricuspid annuloplasty ring dehiscence: A systematic review with pooled analysis. Eur. J. Cardio Thorac. Surg. 2021, 60, 801–810. [Google Scholar] [CrossRef]
- Dreyfus, G.; Serraf, A.; Jebara, V.A.; Deloche, A.; Chauvaud, S.; Couetil, J.P.; Carpentier, A. Valve repair in acute endocarditis. Ann. Thorac. Surg. 1990, 49, 706–713. [Google Scholar] [CrossRef]
- Feringa, H.H.; Shaw, L.J.; Poldermans, D.; Hoeks, S.; van der Wall, E.E.; Dion, R.A.; Bax, J.J. Mitral valve repair and replacement in endocarditis: A systematic review of literature. Ann. Thorac. Surg. 2007, 83, 564–570. [Google Scholar] [CrossRef]
- Lee, H.-A.; Cheng, Y.-T.; Wu, V.C.-C.; Chou, A.-H.; Chu, P.-H.; Tsai, F.-C.; Chen, S.-W. Nationwide cohort study of mitral valve repair versus replacement for infective endocarditis. J. Thorac. Cardiovasc. Surg. 2018, 156, 1473–1483.e2. [Google Scholar] [CrossRef]
- Badhwar, V.; Vemulapalli, S.; Mack, M.A.; Gillinov, A.M.; Chikwe, J.; Dearani, J.A.; Grau-Sepulveda, M.V.; Habib, R.; Rankin, J.S.; Jacobs, J.P.; et al. Volume-Outcome Association of Mitral Valve Surgery in the United States. JAMA Cardiol. 2020, 5, 1092–1101. [Google Scholar] [CrossRef]
- Bonow, R.O.; Adams, D.H. The Time Has Come to Define Centers of Excellence in Mitral Valve Repair*. J. Am. Coll. Cardiol. 2016, 67, 499–501. [Google Scholar] [CrossRef]
- Ruttmann, E.; Legit, C.; Poelzl, G.; Mueller, S.; Chevtchik, O.; Cottogni, M.; Ulmer, H.; Pachinger, O.; Laufer, G.; Mueller, L.C. Mitral valve repair provides improved outcome over replacement in active infective endocarditis. J. Thorac. Cardiovasc. Surg. 2005, 130, 765–771. [Google Scholar] [CrossRef]
- Roudaut, R.; Serri, K.; Lafitte, S. Thrombosis of prosthetic heart valves: Diagnosis and therapeutic considerations. Heart 2007, 93, 137. [Google Scholar] [CrossRef] [PubMed]
- El Gabry, M.; Haidari, Z.; Mourad, F.; Nowak, J.; Tsagakis, K.; Thielmann, M.; Wendt, D.; Jakob, H.; Shehada, S.-E. Outcomes of mitral valve repair in acute native mitral valve infective endocarditis. Interact. Cardiovasc. Thorac. Surg. 2019, 29, 823–829. [Google Scholar] [CrossRef]
- Habib, G.; Badano, L.; Tribouilloy, C.; Vilacosta, I.; Zamorano, J.L.; Galderisi, M.; Voigt, J.-U.; Sicari, R.; Cosyns, B.; Fox, K.; et al. Recommendations for the practice of echocardiography in infective endocarditis. Eur. J. Echocardiogr. 2010, 11, 202–219. [Google Scholar] [CrossRef] [PubMed]
- Mayer, K.; Aicher, D.; Feldner, S.; Kunihara, T.; Schäfers, H.-J. Repair versus replacement of the aortic valve in active infective endocarditis. Eur. J. Cardio Thorac. Surg. 2012, 42, 122–127. [Google Scholar] [CrossRef] [PubMed]
- Solari, S.; Tamer, S.; Aphram, G.; Mastrobuoni, S.; Navarra, E.; Noirhomme, P.; Poncelet, A.; Astarci, P.; Rubay, J.; El Khoury, G.; et al. Aortic valve repair in endocarditis: Scope and results. Indian J. Thorac. Cardiovasc. Surg. 2020, 36, 104–112. [Google Scholar] [CrossRef] [PubMed]
- Zubarevich, A.; Arjomandi Rad, A.; Amanov, L.; Szczechowicz, M.; Osswald, A.; Torabi, S.; Schmack, B.; Ruhparwar, A.; Weymann, A. Sutureless aortic valve replacement in pure aortic regurgitation: Expanding the indications. J. Cardiothorac. Surg. 2022, 17, 198. [Google Scholar] [CrossRef]
- Zubarevich, A.; Szczechowicz, M.; Zhigalov, K.; Osswald, A.; Eynde, J.V.D.; Arjomandi Rad, A.; Vardanyan, R.; Wendt, D.; Schmack, B.; Ruhparwar, A.; et al. Sutureless aortic valve replacement in multivalve procedures. J. Thorac. Dis. 2021, 13, 3392–3398. [Google Scholar] [CrossRef]
- Zubarevich, A.; Arjomandi Rad, A.; Szczechowicz, M.; Ruhparwar, A.; Weymann, A. Sutureless aortic valve replacement in high-risk patients with active infective endocarditis. J. Thorac. Dis. 2022, 14, 3178–3186. [Google Scholar] [CrossRef]
- Musci, M.; Weng, Y.; Hübler, M.; Amiri, A.; Pasic, M.; Kosky, S.; Stein, J.; Siniawski, H.; Hetzer, R. Homograft aortic root replacement in native or prosthetic active infective endocarditis: Twenty-year single-center experience. J. Thorac. Cardiovasc. Surg. 2010, 139, 665–673. [Google Scholar] [CrossRef] [PubMed]
- Le, T.; Graham, N.J.; Naeem, A.; Clemence, J.; Caceres, J.; Wu, X.; Patel, H.J.; Kim, K.M.; Deeb, G.M.; Yang, B. Aortic valve endocarditis in patients with bicuspid and tricuspid aortic valves. JTCVS Open 2021, 8, 228–236. [Google Scholar] [CrossRef] [PubMed]
- Steffen, V.; Marsch, G.; Burgwitz, K.; Kuehn, C.; Teebken, O.E. Resistance to infection of long-term cryopreserved human aortic valve allografts. J. Thorac. Cardiovasc. Surg. 2016, 151, 1251–1259. [Google Scholar] [CrossRef]
- Kim, J.B.; Ejiofor, J.I.; Yammine, M.; Camuso, J.M.; Walsh, C.W.; Ando, M.; Melnitchouk, S.I.; Rawn, J.D.; Leacche, M.; MacGillivray, T.E.; et al. Are homografts superior to conventional prosthetic valves in the setting of infective endocarditis involving the aortic valve? J. Thorac. Cardiovasc. Surg. 2016, 151, 1239–1248.e2. [Google Scholar] [CrossRef] [PubMed]
- Arabkhani, B.; Bekkers, J.A.; Andrinopoulou, E.-R.; Roos-Hesselink, J.W.; Takkenberg, J.J.; Bogers, A.J. Allografts in aortic position: Insights from a 27-year, single-center prospective study Acquired: Aorta Arabkhani et al. J. Thorac. Cardiovasc. Surg. 2016, 152, 1572–1579.e3. [Google Scholar] [CrossRef] [PubMed]
- Fukushima, S.; Tesar, P.J.; Pearse, B.; Jalali, H.; Sparks, L.; Fraser, J.F.; Pohlner, P.G. Long-term clinical outcomes after aortic valve replacement using cryopreserved aortic allograft. J. Thorac. Cardiovasc. Surg. 2014, 148, 65–72.e2. [Google Scholar] [CrossRef] [PubMed]
- Solari, S.; Mastrobuoni, S.; De Kerchove, L.; Navarra, E.; Astarci, P.; Noirhomme, P.; Poncelet, A.; Jashari, R.; Rubay, J.; El Khoury, G. Over 20 years experience with aortic homograft in aortic valve replacement during acute infective endocarditis. Eur. J. Cardio Thorac. Surg. 2016, 50, 1158–1164. [Google Scholar] [CrossRef]
- Yankah, A.; Klose, H.; Petzina, R.; Musci, M.; Siniawski, H.; Hetzer, R. Surgical management of acute aortic root endocarditis with viable homograft: 13-year experience. Eur. J. Cardio Thorac. Surg. 2002, 21, 260–267. [Google Scholar] [CrossRef] [PubMed]
- Perrotta, S.; Jeppsson, A.; Fröjd, V.; Svensson, G. Surgical Treatment of Aortic Prosthetic Valve Endocarditis: A 20-Year Single-Center Experience. Ann. Thorac. Surg. 2016, 101, 1426–1432. [Google Scholar] [CrossRef] [PubMed]
- Preventza, O.; Mohamed, A.S.; Cooley, D.A.; Rodriguez, V.; Bakaeen, F.G.; Cornwell, L.D.; Omer, S.; Coselli, J.S. Homograft use in reoperative aortic root and proximal aortic surgery for endocarditis: A 12-year experience in high-risk patients. J. Thorac. Cardiovasc. Surg. 2014, 148, 989–994. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Jassar, A.S.; Bavaria, J.E.; Szeto, W.Y.; Moeller, P.J.; Maniaci, J.; Milewski, R.K.; Gorman, J.H., 3rd; Desai, N.D.; Gorman, R.C.; Pochettino, A. Graft selection for aortic root replacement in complex active endocarditis: Does it matter? Ann. Thorac. Surg. 2012, 93, 480–487. [Google Scholar] [CrossRef]
- O’Brien, M.F.; Harrocks, S.; Stafford, E.G.; Gardner, M.A.H.; Pohlner, P.G.; Tesar, P.J.; Stephens, F. The homograft aortic valve: A 29-year, 99.3% follow up of 1022 valve replacements. J. Heart Valve Dis. 2001, 10, 334–345. [Google Scholar] [PubMed]
- Sadowski, J.; Kapelak, B.; Bartus, K.; Podolec, P.; Rudzinski, P.; Myrdko, T.; Wierzbicki, K.; Dziatkowiak, A. Reoperation after fresh homograft replacement: 23 years’ experience with 655 patients. Eur. J. Cardio Thorac. Surg. 2003, 23, 996–1001. [Google Scholar] [CrossRef] [PubMed]
- Melina, G.; De Robertis, F.; Gaer, J.A.; Angeloni, E.; El-Hamamsy, I.; Bahrami, T.; Pepper, J.R.; Takkenberg, J.J.; Yacoub, M.H. Long-term survival after xenograft versus homograft aortic root replacement: Results from a prospective randomized trial. J. Thorac. Cardiovasc. Surg. 2021, 161, 57–65. [Google Scholar] [CrossRef]
- Clemence, J.; Caceres, J.; Ren, T.; Wu, X.; Kim, K.M.; Patel, H.J.; Deeb, G.M.; Yang, B. Treatment of aortic valve endocarditis with stented or stentless valve. J. Thorac. Cardiovasc. Surg. 2022, 164, 480–487.e1. [Google Scholar] [CrossRef]
- Easo, J.; Szczechowicz, M.; Hölzl, P.; Meyer, A.; Zhigalov, K.; Malik, R.; Thomas, R.P.; Weymann, A.; Dapunt, O.E. Stentless Root Replacement versus Tissue Valves in Infective Endocarditis—A Propensity-Score Matched Study. Braz. J. Cardiovasc. Surg. 2020, 35, 411. [Google Scholar] [CrossRef]
- Szczechowicz, M.; Weymann, A.; Mkalaluh, S.; Mashhour, A.; Zhigalov, K.; Easo, J. Surgical Options for Aortic Root Replacement in Destructive Endocarditis. Braz. J. Cardiovasc. Surg. 2020, 35, 265. [Google Scholar] [CrossRef]
- Schaefer, A.; Dickow, J.; Schoen, G.; Westhofen, S.; Kloss, L.; Al-Saydali, T.; Reichenspurner, H.; Philipp, S.A.; Detter, C. Stentless vs. stented bioprosthesis for aortic valve replacement: A case matched comparison of long-term follow-up and subgroup analysis of patients with native valve endocarditis. PLoS ONE 2018, 13, e0191171. [Google Scholar] [CrossRef] [PubMed]
- Bavaria, J.E.; Griffith, B.; Heimansohn, D.A.; Rozanski, J.; Johnston, D.R.; Bartus, K.; Girardi, L.N.; Beaver, T.; Takayama, H.; Mumtaz, M.A.; et al. Five-year Outcomes of the COMMENCE Trial Investigating Aortic Valve Replacement with RESILIA Tissue. Ann. Thorac. Surg. 2023, 115, 1429–1436. [Google Scholar] [CrossRef] [PubMed]
- David, T.E.; Kuo, J.; Armstrong, S.; Carpentier, A.F.; Magotra, R.A. Aortic and mitral valve replacement with reconstruction of the intervalvular fibrous body. J. Thorac. Cardiovasc. Surg. 1997, 114, 766–771. [Google Scholar] [CrossRef]
- Davierwala, P.M.; Binner, C.; Subramanian, S.; Luehr, M.; Pfannmueller, B.; Etz, C.; Dohmen, P.; Misfeld, M.; Borger, M.A.; Mohr, F.W. Double valve replacement and reconstruction of the intervalvular fibrous body in patients with active infective endocarditis. Eur. J. Cardio Thorac. Surg. 2014, 45, 146–152. [Google Scholar] [CrossRef] [PubMed]
- Forteza, A.; Centeno, J.; Ospina, V.; Lunar, I.G.; Sánchez, V.; Pérez, E.; López, M.J.; Cortina, J. Outcomes in Aortic and Mitral Valve Replacement with Intervalvular Fibrous Body Reconstruction. Ann. Thorac. Surg. 2015, 99, 838–845. [Google Scholar] [CrossRef]
- David, T.E.; Lafreniere-Roula, M.; David, C.M.; Issa, H. Outcomes of combined aortic and mitral valve replacement with reconstruction of the fibrous skeleton of the heart. J. Thorac. Cardiovasc. Surg. 2022, 164, 1474–1484. [Google Scholar] [CrossRef] [PubMed]
- Zubarevich, A.; Zhigalov, K.; Osswald, A.; Arjomandi Rad, A.; Vardanyan, R.; Wendt, D.; Sá, M.P.B.O.; Schmack, B.; Ruhparwar, A.; Weymann, A. Essen—Commando: How we do it. J. Card. Surg. 2021, 36, 286–289. [Google Scholar] [CrossRef] [PubMed]
- Cahill, T.J.; Baddour, L.M.; Habib, G.; Hoen, B.; Salaun, E.; Pettersson, G.B.; Schäfers, H.J.; Prendergast, B.D. Challenges in Infective Endocarditis. J. Am. Coll. Cardiol. 2017, 69, 325–344. [Google Scholar] [CrossRef]
- David, T.E.; Gavra, G.; Feindel, C.M.; Regesta, T.; Armstrong, S.; Maganti, M.D. Surgical treatment of active infective endocarditis: A continued challenge. J. Thorac. Cardiovasc. Surg. 2007, 133, 144–149. [Google Scholar] [CrossRef]
- Wang, A.; Pappas, P.; Anstrom, K.J.; Abrutyn, E.; Fowler, V.G.; Hoen, B.; Miro, J.M.; Corey, G.R.; Olaison, L.; Stafford, J.A.; et al. The use and effect of surgical therapy for prosthetic valve infective endocarditis: A propensity analysis of a multicenter, international cohort. Am. Heart J. 2005, 150, 1086–1091. [Google Scholar] [CrossRef]
- Manne, M.B.; Shrestha, N.K.; Lytle, B.W.; Nowicki, E.R.; Blackstone, E.; Gordon, S.M.; Pettersson, G.; Fraser, T.G. Outcomes After Surgical Treatment of Native and Prosthetic Valve Infective Endocarditis. Ann. Thorac. Surg. 2012, 93, 489–493. [Google Scholar] [CrossRef]
- Sohail, M.R.; Martin, K.R.; Wilson, W.R.; Baddour, L.M.; Harmsen, W.S.; Steckelberg, J.M. Medical versus surgical management of Staphylococcus aureus prosthetic valve endocarditis. Am. J. Med. 2006, 119, 147–154. [Google Scholar] [CrossRef] [PubMed]
- Lecomte, R.; Laine, J.-B.; Issa, N.; Revest, M.; Gaborit, B.; Le Turnier, P.; Deschanvres, C.; Benezit, F.; Asseray, N.; Le Tourneau, T.; et al. Long-term Outcome of Patients with Nonoperated Prosthetic Valve Infective Endocarditis: Is Relapse the Main Issue? Clin. Infect. Dis. 2020, 71, 1316–1319. [Google Scholar] [CrossRef] [PubMed]
- Danneels, P.; Hamel, J.-F.; Picard, L.; Martinet, P.; Talarmin, J.-P.; Guimard, T.; Le Moal, G.; Brochard-Libois, J.; Beaudron, A.; Letheulle, J.; et al. Impact of Enterococcus faecalis Endocarditis Treatment on Risk of Relapse. Clin. Infect. Dis. 2023, 76, 281–290. [Google Scholar] [CrossRef] [PubMed]
- Stortecky, S.; Heg, D.; Tueller, D.; Pilgrim, T.; Muller, O.; Noble, S.; Jeger, R.; Toggweiler, S.; Ferrari, E.; Taramasso, M.; et al. Infective Endocarditis After Transcatheter Aortic Valve Replacement. J. Am. Coll. Cardiol. 2020, 75, 3020–3030. [Google Scholar] [CrossRef] [PubMed]
- Khan, A.; Aslam, A.; Satti, K.N.; Ashiq, S. Infective endocarditis post-transcatheter aortic valve implantation (TAVI), microbiological profile and clinical outcomes: A systematic review. PLoS ONE 2020, 15, e0225077. [Google Scholar] [CrossRef] [PubMed]
- Zhigalov, K.; Sá, M.P.B.O.; Kadyraliev, B.; Tsagakis, K.; Wendt, D.; Ruhparwar, A.; Weymann, A. Surgical treatment of infective endocarditis in the era of minimally invasive cardiac surgery and transcatheter approach: An editorial. J. Thorac. Dis. 2020, 12, 140. [Google Scholar] [CrossRef] [PubMed]
- Blomström-Lundqvist, C.; Traykov, V.; Erba, P.A.; Burri, H.; Nielsen, J.C.; Bongiorni, M.G.; Poole, J.; Boriani, G.; Costa, R.; Deharo, J.-C.; et al. European Heart Rhythm Association (EHRA) international consensus document on how to prevent, diagnose, and treat cardiac implantable electronic device infections—Endorsed by the Heart Rhythm Society (HRS), the Asia Pacific Heart Rhythm Society (APHRS), the Latin American Heart Rhythm Society (LAHRS), International Society for Cardiovascular Infectious Diseases (ISCVID) and the European Society of Clinical Microbiology and Infectious Diseases (ESCMID) in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS). EP Eur. 2020, 22, 515–549. [Google Scholar] [CrossRef]
- BHRS Standards for Lead Extraction (2018) British Heart Rhythm Society. Available online: https://bhrs.com/wp-content/uploads/2019/03/BHRS-Standards-Lead-Extraction-December-2018.pdf (accessed on 18 December 2023).
- Chu, V.H.; Park, L.P.; Athan, E.; Delahaye, F.; Freiberger, T.; Lamas, C.; Miro, J.M.; Mudrick, D.W.; Strahilevitz, J.; Tribouilloy, C.; et al. Association between surgical indications, operative risk, and clinical outcome in infective endocarditis: A prospective study from the International Collaboration on Endocarditis. Circulation 2015, 131, 131–140. [Google Scholar] [CrossRef]
- Zubarevich, A.; Szczechowicz, M.; Osswald, A.; Easo, J.; Arjomandi Rad, A.; Vardanyan, R.; Schmack, B.; Ruhparwar, A.; Zhigalov, K.; Weymann, A. Surgical treatment of infective endocarditis in intravenous drug abusers. J. Cardiothorac. Surg. 2021, 16, 97. [Google Scholar] [CrossRef]
- Bearpark, L.; Sartipy, U.; Franco-Cereceda, A.; Glaser, N. Surgery for Endocarditis in Intravenous Drug Users. Ann. Thorac. Surg. 2021, 112, 573–581. [Google Scholar] [CrossRef]
- Sultan, I.; Bianco, V.; Kilic, A.; Chu, D.; Navid, F.; Gleason, T.G. Aortic root replacement with cryopreserved homograft for infective endocarditis in the modern North American opioid epidemic. J. Thorac. Cardiovasc. Surg. 2019, 157, 45–50. [Google Scholar] [CrossRef] [PubMed]
- Luc, J.G.Y.; Choi, J.-H.; Kodia, K.; Weber, M.P.; Horan, D.P.; Maynes, E.J.; Carlson, L.A.; Massey, H.T.; Entwistle, J.W.; Morris, R.J.; et al. Valvectomy versus replacement for the surgical treatment of infective tricuspid valve endocarditis: A systematic review and meta-analysis. Ann. Cardiothorac. Surg. 2019, 8, 610–620. [Google Scholar] [CrossRef] [PubMed]
- Ansaripour, A.; Arjomandi Rad, A.; Koulouroudias, M.; Angouras, D.; Athanasiou, T.; Kourliouros, A. Sarcopenia Adversely Affects Outcomes following Cardiac Surgery: A Systematic Review and Meta-Analysis. J. Clin. Med. 2023, 12, 5573. [Google Scholar] [CrossRef] [PubMed]
- Durante Mangoni, E.; Bradley, S.; Selton Suty, C.; Tripodi, M.F.; Barsic, B.; Bouza, E.; Cabell, C.H.; de Oliveira Ramos, A.I.; Fowler, V., Jr.; Hoen, B.; et al. Current Features of Infective Endocarditis in Elderly Patients: Results of the International Collaboration on Endocarditis Prospective Cohort Study. Arch. Intern. Med. 2008, 168, 2095–2103. [Google Scholar] [CrossRef] [PubMed]
- Kiriyama, H.; Kaneko, H.; Itoh, H.; Kamon, T.; Morita, K.; Jo, T.; Fujiu, K.; Daimon, M.; Takeda, N.; Morita, H.; et al. Surgical treatment for infective endocarditis in the ageing society: A nationwide retrospective study in Japan. Open Heart 2021, 8, e001627. [Google Scholar] [CrossRef]
- Ragnarsson, S.; Salto-Alejandre, S.; Ström, A.; Olaison, L.; Rasmussen, M. Surgery is underused in elderly patients with left-sided infective endocarditis: A nationwide registry study. J. Am. Heart Assoc. 2021, 10, e020221. [Google Scholar] [CrossRef]




Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Arjomandi Rad, A.; Zubarevich, A.; Osswald, A.; Vardanyan, R.; Magouliotis, D.E.; Ansaripour, A.; Kourliouros, A.; Sá, M.P.; Rassaf, T.; Ruhparwar, A.; et al. The Surgical Treatment of Infective Endocarditis: A Comprehensive Review. Diagnostics 2024, 14, 464. https://doi.org/10.3390/diagnostics14050464
Arjomandi Rad A, Zubarevich A, Osswald A, Vardanyan R, Magouliotis DE, Ansaripour A, Kourliouros A, Sá MP, Rassaf T, Ruhparwar A, et al. The Surgical Treatment of Infective Endocarditis: A Comprehensive Review. Diagnostics. 2024; 14(5):464. https://doi.org/10.3390/diagnostics14050464
Chicago/Turabian StyleArjomandi Rad, Arian, Alina Zubarevich, Anja Osswald, Robert Vardanyan, Dimitrios E. Magouliotis, Ali Ansaripour, Antonios Kourliouros, Michel Pompeu Sá, Tienush Rassaf, Arjang Ruhparwar, and et al. 2024. "The Surgical Treatment of Infective Endocarditis: A Comprehensive Review" Diagnostics 14, no. 5: 464. https://doi.org/10.3390/diagnostics14050464
APA StyleArjomandi Rad, A., Zubarevich, A., Osswald, A., Vardanyan, R., Magouliotis, D. E., Ansaripour, A., Kourliouros, A., Sá, M. P., Rassaf, T., Ruhparwar, A., Sardari Nia, P., Athanasiou, T., & Weymann, A. (2024). The Surgical Treatment of Infective Endocarditis: A Comprehensive Review. Diagnostics, 14(5), 464. https://doi.org/10.3390/diagnostics14050464