

Preoperative Assessment of Medication-Related Osteonecrosis of the Jaw Using [18F]fluoride Positron Emission Tomography (PET)/CT and [18F]fluorodeoxyglucose PET/MRI in Correlation with Histomorphometry and Micro-CT—A Prospective Comparative Study

 , , , ,
, , , ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Patient Cohort
2.2. Study Protocol
2.3. [18F]FDG PET/MRI
2.4. [18F]fluoride PET/CT
2.5. Image Analysis
2.6. Bone Specimens
2.7. Surgical Technique
2.8. Micro-CT and Histomorphometric Analysis
2.9. Statistics
3. Results
3.1. Patient Characteristics
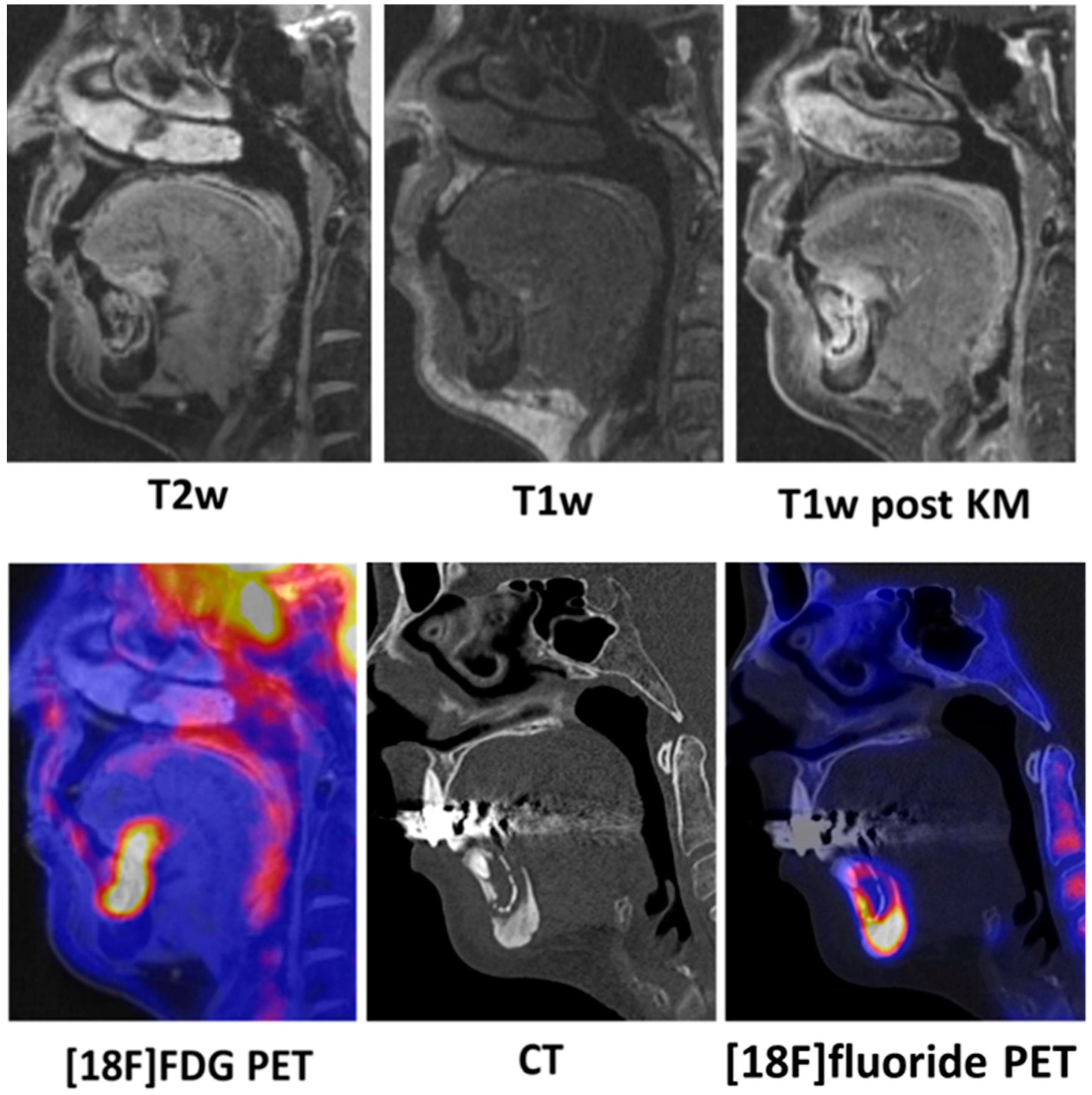
3.2. Qualitative Imaging
3.3. Quantitative Imaging
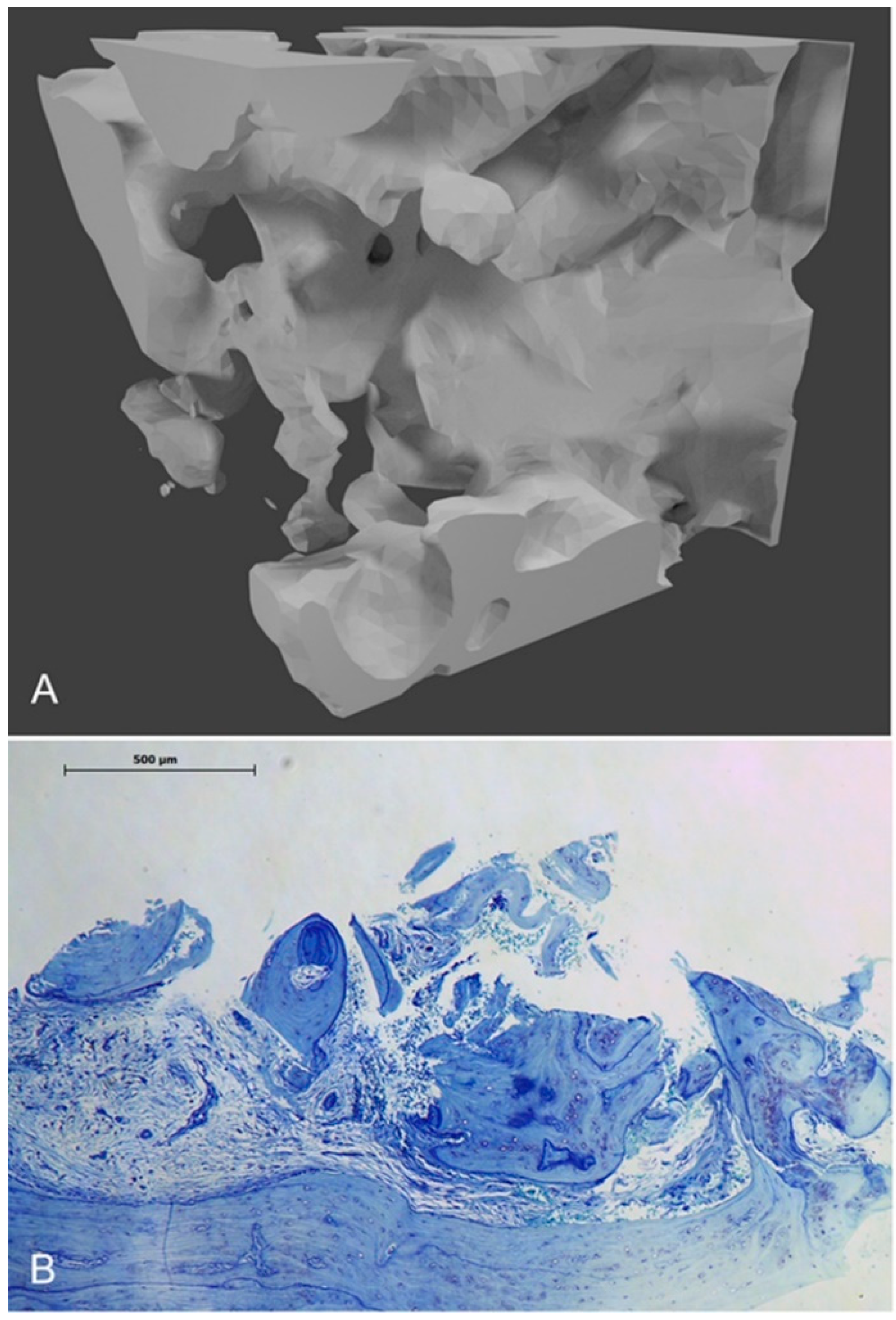
3.4. Microarchitecture
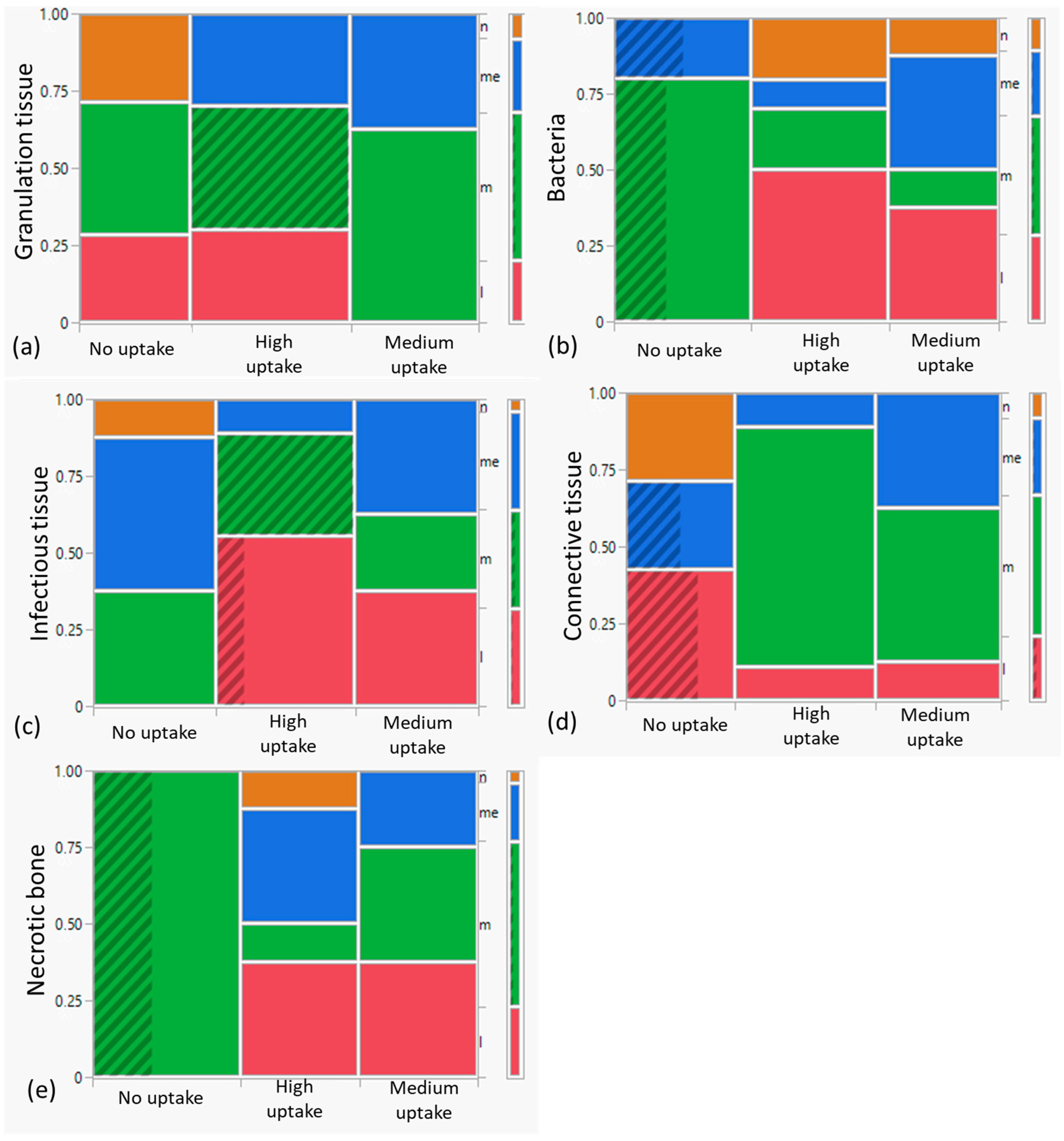
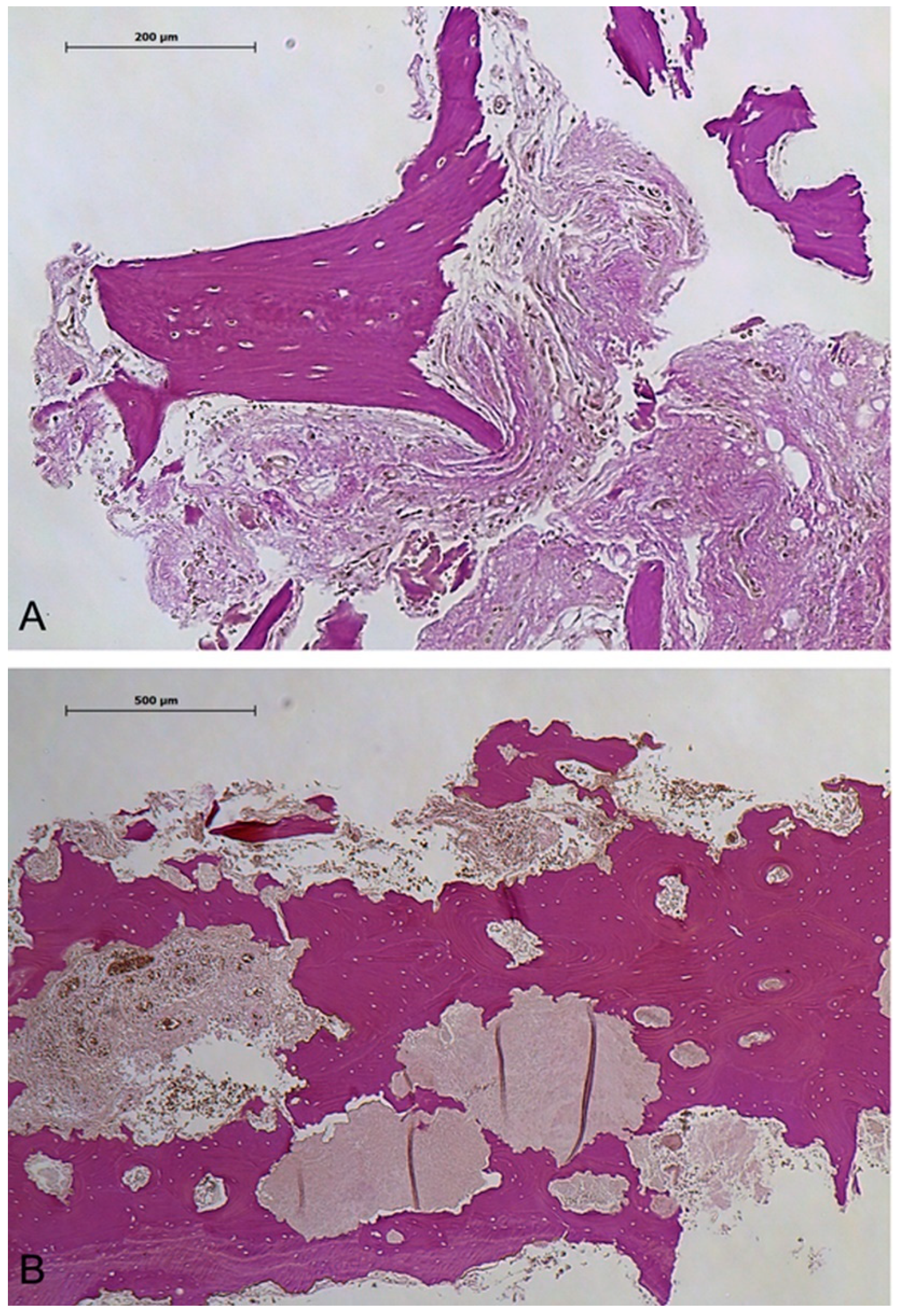
3.5. Histomorphometry
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Vanpoecke, J.; Verstraete, L.; Smeets, M.; Ferri, J.; Nicot, R.; Politis, C. Medication-related osteonecrosis of the jaw (MRONJ) stage III: Conservative and conservative surgical approaches versus an aggressive surgical intervention: A systematic review. J. Cranio-Maxillofac. Surg. 2020, 48, 435–443. [Google Scholar] [CrossRef]
- Yamada, S.-I.; Kurita, H.; Kondo, E.; Suzuki, S.; Nishimaki, F.; Yoshimura, N.; Morioka, M.; Ishii, S.; Kamata, T. Treatment outcomes and prognostic factors of medication-related osteonecrosis of the jaw: A case- and literature-based review. Clin. Oral Investig. 2019, 23, 3203–3211. [Google Scholar] [CrossRef]
- Khan, A.A.; Morrison, A.; Kendler, D.L.; Rizzoli, R.; Hanley, D.A.; Felsenberg, D.; McCauley, L.K.; O’Ryan, F.; Reid, I.R.; Ruggiero, S.L.; et al. Case-Based Review of Osteonecrosis of the Jaw (ONJ) and Application of the International Recommendations for Management From the International Task Force on ONJ. J. Clin. Densitom. 2017, 20, 8–24. [Google Scholar] [CrossRef] [PubMed]
- Allen, M.R.; Burr, D.B. Mandible Matrix Necrosis in Beagle Dogs After 3 Years of Daily Oral Bisphosphonate Treatment. J. Oral Maxillofac. Surg. 2008, 66, 987–994. [Google Scholar] [CrossRef] [PubMed]
- Ruggiero, S.L.; Dodson, T.B.; Fantasia, J.; Goodday, R.; Aghaloo, T.; Mehrotra, B.; O’Ryan, F. American Association of Oral and Maxillofacial Surgeons Position Paper on Medication-Related Osteonecrosis of the Jaw—2014 Update. J. Oral Maxillofac. Surg. 2014, 72, 1938–1956. [Google Scholar] [CrossRef] [PubMed]
- Yoneda, T.; Japanese Allied Committee on Osteonecrosis of the Jaw; Hagino, H.; Sugimoto, T.; Ohta, H.; Takahashi, S.; Soen, S.; Taguchi, A.; Nagata, T.; Urade, M.; et al. Antiresorptive agent-related osteonecrosis of the jaw: Position Paper 2017 of the Japanese Allied Committee on Osteonecrosis of the Jaw. J. Bone Miner. Metab. 2017, 35, 6–19. [Google Scholar] [CrossRef]
- Edwards, B.J.; Gounder, M.; McKoy, J.M.; Boyd, I.; Farrugia, M.; Migliorati, C.; Marx, R.; Ruggiero, S.; Dimopoulos, M.; Raisch, D.W.; et al. Pharmacovigilance and reporting oversight in US FDA fast-track process: Bisphosphonates and osteonecrosis of the jaw. Lancet Oncol. 2008, 9, 1166–1172. [Google Scholar] [CrossRef]
- Nicolatou-Galitis, O.; Papadopoulou, E.; Sarri, T.; Boziari, P.; Karayianni, A.; Kyrtsonis, M.-C.; Repousis, P.; Barbounis, V.; Migliorati, C.A. Osteonecrosis of the jaw in oncology patients treated with bisphosphonates: Prospective experience of a dental oncology referral center. Oral Surgery Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2011, 112, 195–202. [Google Scholar] [CrossRef]
- Ristow, O.; Rückschloß, T.; Müller, M.; Berger, M.; Kargus, S.; Pautke, C.; Engel, M.; Hoffmann, J.; Freudlsperger, C. Is the conservative non-surgical management of medication-related osteonecrosis of the jaw an appropriate treatment option for early stages? A long-term single-center cohort study. J. Cranio-Maxillofac. Surg. 2019, 47, 491–499. [Google Scholar] [CrossRef]
- Schiegnitz, E.; Al-Nawas, B.; Hoefert, S.; Otto, S.; Pautke, C.; Ristow, O.; Voss, P.; Grötz, K.A. S3-Leitlinie Antiresorptiva-assoziierte Kiefernekrosen 2017, AWMF Registernummer: 007-091. Available online: https://register.awmf.org/assets/guidelines/007-091l_S3_Antiresorptiva-assoziierte-Kiefernekrosen-AR-ONJ_2018-12.pdf (accessed on 29 December 2023).
- Wyngaert, T.V.D.; Claeys, T.; Huizing, M.T.; Vermorken, J.B.; Fossion, E. Initial experience with conservative treatment in cancer patients with osteonecrosis of the jaw (ONJ) and predictors of outcome. Ann. Oncol. 2009, 20, 331–336. [Google Scholar] [CrossRef]
- Tyndall, D.A.; Rathore, S. Cone-Beam CT Diagnostic Applications: Caries, Periodontal Bone Assessment, and Endodontic Applications. Dent. Clin. N. Am. 2008, 52, 825–841. [Google Scholar] [CrossRef] [PubMed]
- García-Ferrer, L.; Bagán, J.V.; Martínez-Sanjuan, V.; Hernandez-Bazan, S.; García, R.; Jiménez-Soriano, Y.; Hervas, V. MRI of Mandibular Osteonecrosis Secondary to Bisphosphonates. Am. J. Roentgenol. 2008, 190, 949–955. [Google Scholar] [CrossRef] [PubMed]
- Minami, Y.; Ogura, I. Comparison of maximum and mean standardized uptake values of jaw pathologies with bone SPECT/CT: An especial focus on medication-related osteonecrosis of the jaw. Nucl. Med. Commun. 2022, 43, 1188–1194. [Google Scholar] [CrossRef] [PubMed]
- Stockmann, P.; Hinkmann, F.M.; Lell, M.M.; Fenner, M.; Vairaktaris, E.; Neukam, F.-W.; Nkenke, E. Panoramic radiograph, computed tomography or magnetic resonance imaging. Which imaging technique should be preferred in bisphosphonate-associated osteonecrosis of the jaw? A prospective clinical study. Clin. Oral Investig. 2010, 14, 311–317. [Google Scholar] [CrossRef] [PubMed]
- Hong, C.M.; Ahn, B.-C.; Choi, S.-Y.; Kim, D.-H.; Lee, S.-W.; Kwon, T.-G.; Lee, J. Implications of Three-Phase Bone Scintigraphy for the Diagnosis of Bisphosphonate-Related Osteonecrosis of the Jaw. Nucl. Med. Mol. Imaging 2012, 46, 162–168. [Google Scholar] [CrossRef] [PubMed]
- Fleisher, K.E.; Raad, R.A.; Rakheja, R.; Gupta, V.; Chan, K.C.; Friedman, K.P.; Mourtzikos, K.A.; Janal, M.; Glickman, R.S. Fluorodeoxyglucose positron emission tomography with computed tomography detects greater metabolic changes that are not represented by plain radiography for patients with osteonecrosis of the jaw. J. Oral Maxillofac. Surg. 2014, 72, 1957–1965. [Google Scholar] [CrossRef] [PubMed]
- Lapa, P.; de Lima, J.P. Superiority of 18F-NaF PET/CT for the detection of bone metastases. Nucl. Med. Commun. 2018, 39, 344–345. [Google Scholar] [CrossRef] [PubMed]
- Agrawal, K.; Marafi, F.; Gnanasegaran, G.; Van der Wall, H.; Fogelman, I. Pitfalls and Limitations of Radionuclide Planar and Hybrid Bone Imaging. Semin. Nucl. Med. 2015, 45, 347–372. [Google Scholar] [CrossRef]
- Phal, P.M.; Myall, R.W.T.; Assael, L.A.; Weissman, J.L. Imaging Findings of Bisphosphonate-Associated Osteonecrosis of the Jaws. Am. J. Neuroradiol. 2007, 28, 1139–1145. [Google Scholar] [CrossRef]
- Leite, A.F.; Ogata, F.D.S.; de Melo, N.S.; Figueiredo, P.T.D.S. Imaging findings of bisphosphonate-related osteonecrosis of the jaws: A critical review of the quantitative studies. Int. J. Dent. 2014, 2014, 784348. [Google Scholar] [CrossRef]
- Guggenberger, R.; Fischer, D.; Metzler, P.; Andreisek, G.; Nanz, D.; Jacobsen, C.; Schmid, D. Bisphosphonate-Induced Osteonecrosis of the Jaw: Comparison of Disease Extent on Contrast-Enhanced MR Imaging, [18F] Fluoride PET/CT, and Conebeam CT imaging. Am. J. Neuroradiol. 2013, 34, 1242–1247. [Google Scholar] [CrossRef]
- Ruggiero, S.L.; Dodson, T.B.; Aghaloo, T.; Carlson, E.R.; Ward, B.B.; Kademani, D. American Association of Oral and Maxillofacial Surgeons’ Position Paper on Medication-Related Osteonecrosis of the Jaws—2022 Update. J. Oral Maxillofac. Surg. 2022, 80, 920–943. [Google Scholar] [CrossRef] [PubMed]
- Bennett, P.; Mintz, A.; Perry, B.; Vergara-Wentland, P.; Trout, A.T. Specialty Imaging: PET; Elsevier: Amsterdam, The Netherlands, 2017. [Google Scholar]
- Hoefert, S.; Eufinger, H. Relevance of a prolonged preoperative antibiotic regime in the treatment of bisphosphonate-related osteonecrosis of the jaw. J. Oral Maxillofac. Surg. 2011, 69, 362–380. [Google Scholar] [CrossRef] [PubMed]
- Fitzgibbons, P.L.; Dillon, D.A.; Alsabeh, R.; Berman, M.A.; Hayes, D.F.; Hicks, D.G.; Hughes, K.S.; Nofech-Mozes, S.; Patrick, L.; Fitzgibbons, M.D.; et al. Template for reporting results of biomarker testing of specimens from patients with carcinoma of the breast. Arch. Pathol. Lab. Med. 2014, 138, 595–601. [Google Scholar] [CrossRef] [PubMed]
- Bisdas, S.; Pinho, N.C.; Smolarz, A.; Sader, R.; Vogl, T.; Mack, M. Biphosphonate-induced osteonecrosis of the jaws: CT and MRI spectrum of findings in 32 patients. Clin. Radiol. 2008, 63, 71–77. [Google Scholar] [CrossRef] [PubMed]
- Chiandussi, S.; Biasotto, M.; Dore, F.; Cavalli, F.; Cova, M.; Di Lenarda, R. Clinical and diagnostic imaging of bisphosphonate-associated osteonecrosis of the jaws. Dentomaxillofac. Radiol. 2006, 35, 236–243. [Google Scholar] [CrossRef] [PubMed]
- Estilo, C.L.; Van Poznak, C.H.; Wiliams, T.; Bohle, G.C.; Lwin, P.T.; Zhou, Q.; Riedel, E.R.; Carlson, D.L.; Schoder, H.; Farooki, A.; et al. Osteonecrosis of the Maxilla and Mandible in Patients with Advanced Cancer Treated with Bisphosphonate Therapy. Oncologist 2008, 13, 911–920. [Google Scholar] [CrossRef] [PubMed]
- Allen, M.R.; Burr, D.B. Bisphosphonate effects on bone turnover, microdamage, and mechanical properties: What we think we know and what we know that we don’t know. Bone 2011, 49, 56–65. [Google Scholar] [CrossRef] [PubMed]
- Saad, F.; Brown, J.E.; Van Poznak, C.; Ibrahim, T.; Stemmer, S.M.; Stopeck, A.T.; Diel, I.J.; Takahashi, S.; Shore, N.; Henry, D.H.; et al. Incidence, risk factors, and outcomes of osteonecrosis of the jaw: Integrated analysis from three blinded active-controlled phase III trials in cancer patients with bone metastases. Ann. Oncol. 2012, 23, 1341–1347. [Google Scholar] [CrossRef]
- Arce, K.; Assael, L.A.; Weissman, J.L.; Markiewicz, M.R. Imaging Findings in Bisphosphonate-Related Osteonecrosis of Jaws. J. Oral Maxillofac. Surg. 2009, 67, 75–84. [Google Scholar] [CrossRef]
- Hutchinson, M.; O’Ryan, F.; Chavez, V.; Lathon, P.V.; Sanchez, G.; Hatcher, D.C.; Indresano, A.T.; Lo, J.C. Radiographic Findings in Bisphosphonate-Treated Patients With Stage 0 Disease in the Absence of Bone Exposure. J. Oral Maxillofac. Surg. 2010, 68, 2232–2240. [Google Scholar] [CrossRef]
- Schoenhof, R.; Munz, A.; Yuan, A.; ElAyouti, A.; Boesmueller, H.; Blumenstock, G.; Reinert, S.; Hoefert, S. Microarchitecture of medication-related osteonecrosis of the jaw (MRONJ); a retrospective micro-CT and morphometric analysis. J. Cranio-Maxillofac. Surg. 2021, 49, 508–517. [Google Scholar] [CrossRef]
- Yuan, A.; Munz, A.; Reinert, S.; Hoefert, S. Histologic analysis of medication-related osteonecrosis of the jaw compared with antiresorptive-exposed bone and other infectious, inflammatory, and necrotic jaw diseases. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2020, 129, 133–140. [Google Scholar] [CrossRef] [PubMed]
- Bedogni, A.; Blandamura, S.; Lokmic, Z.; Palumbo, C.; Ragazzo, M.; Ferrari, F.; Tregnaghi, A.; Pietrogrande, F.; Procopio, O.; Saia, G.; et al. Bisphosphonate-associated jawbone osteonecrosis: A correlation between imaging techniques and histopathology. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2008, 105, 358–364. [Google Scholar] [CrossRef] [PubMed]
- Wilde, F.; Heufelder, M.; Lorenz, K.; Liese, S.; Liese, J.; Helmrich, J.; Schramm, A.; Hemprich, A.; Hirsch, E.; Winter, K. Prevalence of cone beam computed tomography imaging findings according to the clinical stage of bisphosphonate-related osteonecrosis of the jaw. Oral Surgery Oral Med. Oral Pathol. Oral Radiol. 2012, 114, 804–811. [Google Scholar] [CrossRef] [PubMed]
- Grant, F.D.; Fahey, F.H.; Packard, A.B.; Davis, R.T.; Alavi, A.; Treves, S.T. Skeletal PET with 18F-fluoride: Applying new technology to an old tracer. J. Nucl. Med. 2008, 49, 68–78. [Google Scholar] [CrossRef] [PubMed]
- Schär, M.; Ma, R.; Demange, M.; Morgan, M.; Chen, T.; Ballon, D.J.; Dyke, J.P.; Deng, X.-H.; A Rodeo, S. Use of small animal PET-CT imaging for in vivo assessment of tendon-to-bone healing: A pilot study. J. Orthop. Surg. 2022, 30, 23094990221076654. [Google Scholar] [CrossRef] [PubMed]
- Rahmim, A.; Zaidi, H. PET versus SPECT: Strengths, limitations and challenges. Nucl. Med. Commun. 2008, 29, 193–207. [Google Scholar] [CrossRef] [PubMed]
- A Sims, N.; Martin, T.J. Coupling the activities of bone formation and resorption: A multitude of signals within the basic multicellular unit. BoneKEy Rep. 2014, 3, 481. [Google Scholar] [CrossRef] [PubMed]
- Marx, R.E. Bisphosphonat-Induzierte Osteonekrose der Kiefer: Ätiologie, Prävention, Behandlung; Quintessenz Verlag: Berlin, Germany, 2013. [Google Scholar]
- Hanley, D.A.; Adachi, J.D.; Bell, A.; Brown, V. Denosumab: Mechanism of action and clinical outcomes. Int. J. Clin. Pract. 2012, 66, 1139–1146. [Google Scholar] [CrossRef]
- Aoki, K.; Matsunaga, S.; Ito, S.; Shibahara, T.; Nomura, T.; Matsuzaki, H.; Abe, S.; Yamaguchi, A. Persistent bone resorption lacunae on necrotic bone distinguish bisphosphonate-related osteonecrosis of jaw from denosumab-related osteonecrosis. J. Bone Miner. Metab. 2021, 39, 737–747. [Google Scholar] [CrossRef] [PubMed]
- Even-Sapir, E.; Mishani, E.; Flusser, G.; Metser, U. 18F-fluoride positron emission tomography and positron emission tomography/computed tomography. Semin. Nucl. Med. 2007, 37, 462–469. [Google Scholar] [CrossRef] [PubMed]
- Minami, Y.; Ogura, I. Comparison of single photon emission computed tomography-computed tomography, computed tomography and magnetic resonance imaging of osteonecrosis of jaw by new calculated parameters. Q. J. Nucl. Med. Mol. Imaging 2022. [Google Scholar] [CrossRef] [PubMed]
- Ruggiero, S.L.; Dodson, T.B.; Assael, L.A.; Landesberg, R.; Marx, R.E.; Mehrotra, B. American association of oral and maxillofacial surgeons position paper on bisphosphonate-related osteonecrosis of the jaws—2009 update. J. Oral Maxillofac. Surg. 2009, 67, 2–12. [Google Scholar] [CrossRef]
- Walter, C.; Al-Nawas, B.; Frickhofen, N.; Gamm, H.; Beck, J.; Reinsch, L.; Blum, C.; Grötz, K.A.; Wagner, W. Prevalence of bisphosphonate associated osteonecrosis of the jaws in multiple myeloma patients. Head Face Med. 2010, 6, 11. [Google Scholar] [CrossRef]
- Ristow, O.; Otto, S.; Geiß, C.; Kehl, V.; Berger, M.; Troeltzsch, M.; Koerdt, S.; Hohlweg-Majert, B.; Freudlsperger, C.; Pautke, C. Comparison of auto-fluorescence and tetracycline fluorescence for guided bone surgery of medication-related osteonecrosis of the jaw: A randomized controlled feasibility study. Int. J. Oral Maxillofac. Surg. 2017, 46, 157–166. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| (a) | |||||||||
| Patient | Sex; Age | Primary Diagnosis | Antiresorptive Drug; Application | Duration of Treatment # | Antibiotics | Duration of Antibiotic Treatment § | Clinical Outcome after Surgery | Follow Up | Clinical Outcome at Endpoint of Follow Up |
| 1 | male; 67 yr. | Prostate cancer | Zoledronate; iv | 79 months | Clindamycin; Moxifloxacin | 32 (25o; 7iv) | cured | 30 months | cured |
| 2 | female; 76 yr. | Breast cancer | Zoledronate; iv | 22 months | Cefuroxime; Moxifloxacin | 32 (25o; 7iv) | cured | 29 months | cured at origin; new necrosis at the upper jaw |
| 3 | female; 68 yr. | Breast cancer | Denosumab; sc | 48 months | Sultamicillin; Ampicillin/Sulbactam; Metronidazole; Cefuroxime | 29 (22o; 7iv) | cured | 40 months | cured |
| 4 | male; 65 yr. | Kidney cancer | Denosumab; sc | 6 months | Sultamicillin; Ampicillin/Sulbactam; Clindamycin | 32 (25o; 7iv) | cured | 18 months | cured |
| 5 | male; 65 yr. | Multiple myeloma | Zoledronate; iv | 13 months | Sultamicillin; Metronidazole | 40 (33o; 7iv) | cured | 10 months | cured |
| 6 | male; 79 yr. | Multiple myeloma | Zoledronate; iv Denosumab; sc | 24 months | Sultamicillin; Ampicillin/Sulbactam | 22 (15o; 7iv) | cured | 6 months | cured |
| 7 | male; 77 yr. | Multiple myeloma | Zoledronate; iv | 7 months | Sultamicillin; Ampicillin/Sulbactam; Metronidazole | 21 (14o; 7iv) | cured | 5 months | cured |
| (b) | |||||||||
| Patient | Sex; Age | Primary Diagnosis | Location of Necrosis | Antiresorptive Drug; Application | Duration of Treatment # | Antibiotics | Duration of Antibiotic Treatment * | Follow Up | Clinical Outcome at Endpoint of Follow Up |
| 8 | female; 53 yr. | Breast cancer | Lower jaw both sides | Denosumab (biannual) | 18 months | none | 60 months | spontaneous sequestrum; cured | |
| 9 | female; 76 yr. | Breast cancer | Lower jaw both sides | Ibandronate Denosumab | 138 months | Sultamicillin; Moxifloxacin | 87 (80o; 7iv) | 63 months | sequestrum; not cured |
| 10 | male; 68 yr. | Lung cancer | Lower jaw both sides | Denosumab | 29 months | Metronidazole (local application) | each visit | 7 months | sequestrum; not cured |
| 11 | male; 76 yr. | Prostate cancer | Lower jaw left | Zoledronate | 18 months | Sultamicillin | 280 (o) | 12 months | died; not cured |
| 12 | female; 78 yr. | Breast cancer | Lower jaw both sides | Zoledronate Denosumab | 58 months | Sultamicillin Sulfamethoxazole/Trimetoprima | 263 (o) | 40 months | not cured |
| Imaging Markers | Affected Bone | Healthy Bone | SQI | p Value |
|---|---|---|---|---|
| T2w | 28 ± 19 | 40 ± 26 | 0.9 ± 0.4 | >0.05 |
| T1w | 140 ± 58 | 303 ± 124 | 0.5 ± 0.3 | 0.0005 |
| T1w post-contrast (bone) | 304 ± 143 | 281 ± 151 | 1.4 ± 0.7 | >0.05 |
| [18F]FDG PET SUVmean (bone) | 1.1 ± 0.4 | 0.6 ± 0.2 | 2.0 ± 1.1 | 0.003 |
| [18F]FDG PET SUVmean (soft tissue) | 4.1 ± 1.4 | 1.9 ± 0.3 | 2.2 ± 0.9 | 0.0004 |
| [18F]fluoride PET SUVmean (bone) | 21 ± 12 | 2.4 ± 0.8 | 8.9 ± 3.3 | 0.00001 |
| Hounsfield Units | 1085 ± 218 | 271 ± 136 | 6.5 ± 7.4 | 0.00001 |
| Micro-CT | Necrotic Bone | Medium [18F]fluoride Uptake | High [18F]fluoride Uptake | p Value |
|---|---|---|---|---|
| BV/TV | 0.24 ± 0.09 | 0.27 ± 0.14 | 0.33 ± 0.15 | >0.05 |
| (0.12–0.49) | (0.14–0.52) | (0.14–0.6) | ||
| BS/BV | 4.41 ± 2.97 | 5.34 ± 2.05 | 5.42 ± 1.88 | >0.05 |
| (2.3–10.48) | (2.78–8.61) | (2.78–8.61) | ||
| Tr.Th. (mm) | 0.48 ± 0.25 | 0.43 ± 0.17 | 0.41 ± 0.15 | >0.05 |
| (0.19–0.87) | (0.25–0.71) | (0.23–0.72) | ||
| Tr.N. (mm−1) | 0.59 ± 0.10 | 0.63 ± 0.12 | 0.86 ± 0.10 | >0.05 |
| (0.28–1.21) | (0.35–0.96) | (0.24–1.51) | ||
| Tr.Sp. (mm) | 1.62 ± 0.26 | 1.31 ± 0.31 | 1.14 ± 0.26 | >0.05 |
| (0.54–2.75) | (0.65–3.64) | (0.65–2.26) | ||
| Euler Index | 1.36 ± 1.86 | 1.28 ± 0.87 | 2.13 ± 2.35 | >0.05 |
| (0.19–5.69) | (0.31–2.97) | (0.13–8.10) | ||
| BMD (g·cm−3) | 656.0 ± 38.6 | 580.1 ± 46.1 | 750.0 ± 38.6 | >0.05 |
| (567.2–764.5) | (555.5–997.2) | (519.5–937.9) |
| Histological Samples | Necrotic Bone | Medium [18F]fluoride Uptake | High [18F]fluoride Uptake | p Value |
|---|---|---|---|---|
| Osteocytes/mm2 | 10.2 ± 48.2 | 164.4 ± 53.6 | 335.5 ± 48.2 | 0.0005 |
| Lacunae/mm2 | 347.5 ± 37.9 | 305.1 ± 42.3 | 444.3 ± 37.9 | 0.01 |
| Osteoblasts/mm | 24.5 ± 14.5 | 37.9 ± 8.9 | 42.9 ± 8.4 | >0.05 |
| Osteoclasts/mm | 1.5 ± 0.5 | 1.6 ± 0.3 | 1.6 ± 0.3 | >0.05 |
| Resorption lacunae, mean length (mm) | 0.033 ± 0.004 | 0.033 ± 0.004 | 0.025 ± 0.004 | >0.05 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Reinert, C.P.; Pfannenberg, C.; Gückel, B.; Dittmann, H.; la Fougère, C.; Nikolaou, K.; Reinert, S.; Schönhof, R.; Hoefert, S. Preoperative Assessment of Medication-Related Osteonecrosis of the Jaw Using [18F]fluoride Positron Emission Tomography (PET)/CT and [18F]fluorodeoxyglucose PET/MRI in Correlation with Histomorphometry and Micro-CT—A Prospective Comparative Study. Diagnostics 2024, 14, 428. https://doi.org/10.3390/diagnostics14040428
Reinert CP, Pfannenberg C, Gückel B, Dittmann H, la Fougère C, Nikolaou K, Reinert S, Schönhof R, Hoefert S. Preoperative Assessment of Medication-Related Osteonecrosis of the Jaw Using [18F]fluoride Positron Emission Tomography (PET)/CT and [18F]fluorodeoxyglucose PET/MRI in Correlation with Histomorphometry and Micro-CT—A Prospective Comparative Study. Diagnostics. 2024; 14(4):428. https://doi.org/10.3390/diagnostics14040428
Chicago/Turabian StyleReinert, Christian Philipp, Christina Pfannenberg, Brigitte Gückel, Helmut Dittmann, Christian la Fougère, Konstantin Nikolaou, Siegmar Reinert, Rouven Schönhof, and Sebastian Hoefert. 2024. "Preoperative Assessment of Medication-Related Osteonecrosis of the Jaw Using [18F]fluoride Positron Emission Tomography (PET)/CT and [18F]fluorodeoxyglucose PET/MRI in Correlation with Histomorphometry and Micro-CT—A Prospective Comparative Study" Diagnostics 14, no. 4: 428. https://doi.org/10.3390/diagnostics14040428
APA StyleReinert, C. P., Pfannenberg, C., Gückel, B., Dittmann, H., la Fougère, C., Nikolaou, K., Reinert, S., Schönhof, R., & Hoefert, S. (2024). Preoperative Assessment of Medication-Related Osteonecrosis of the Jaw Using [18F]fluoride Positron Emission Tomography (PET)/CT and [18F]fluorodeoxyglucose PET/MRI in Correlation with Histomorphometry and Micro-CT—A Prospective Comparative Study. Diagnostics, 14(4), 428. https://doi.org/10.3390/diagnostics14040428