
Calcitonin-Gene-Related Peptide in Migraine and Tension-Type Headache in Children During Interictal Period
 , , , , ,
, , , , ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Participants
2.2. Demographic and Clinical Characteristics
2.3. CGRP Determination
2.4. Statistical Analysis
3. Results
3.1. Study Population
3.2. Serum CGRP Levels in the Migraine Group, Tension-Type Group, and Healthy Controls
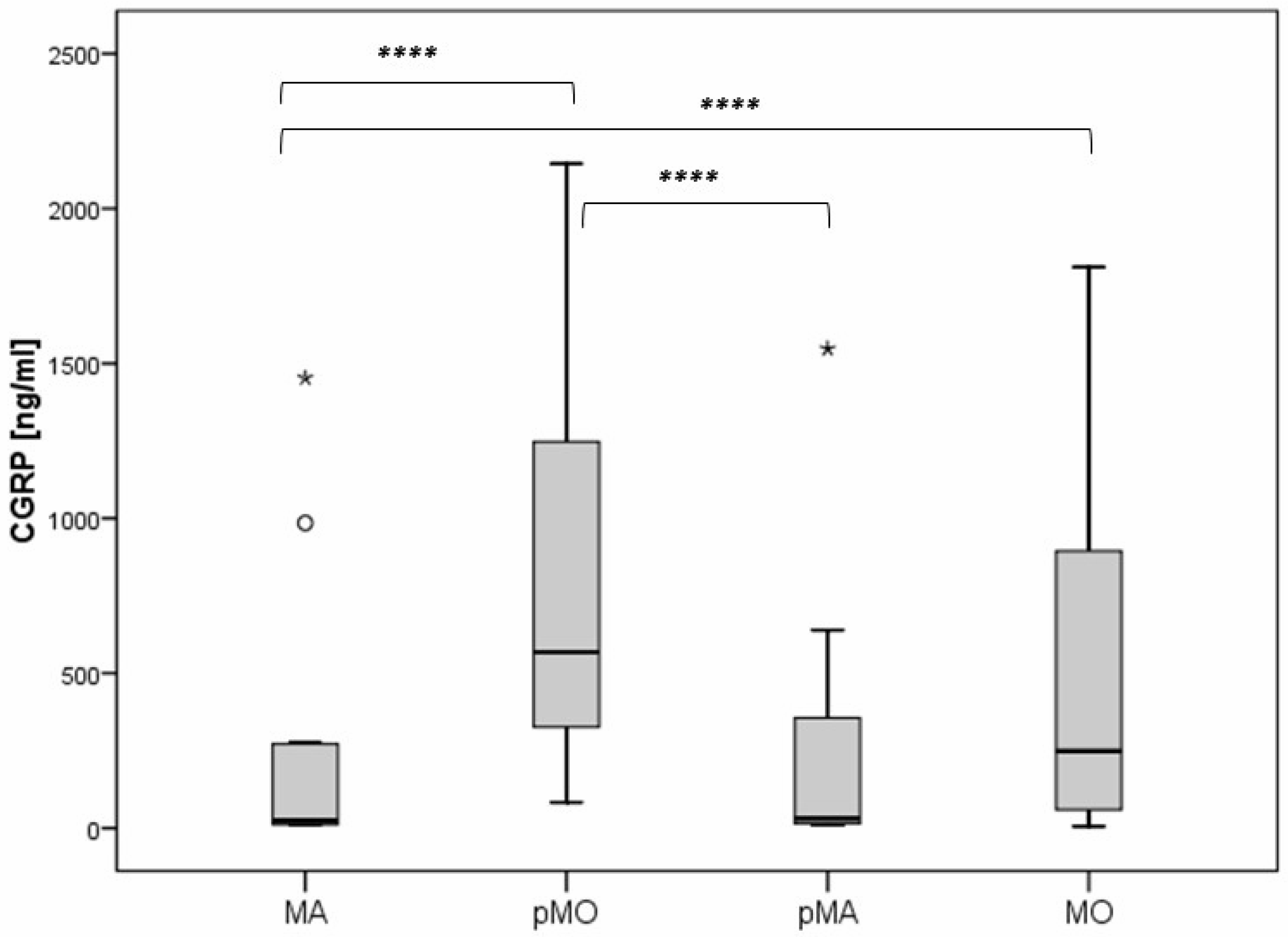
3.3. Plasma CGRP Levels in Pediatric Migraine Without Aura, Migraine with Aura, Probable Migraine Without Aura, and Probable Migraine with Aura
3.4. The Correlation of CGRP with Clinical Characteristics and Association of CGRP and the Diagnosis of Pediatric Migraine
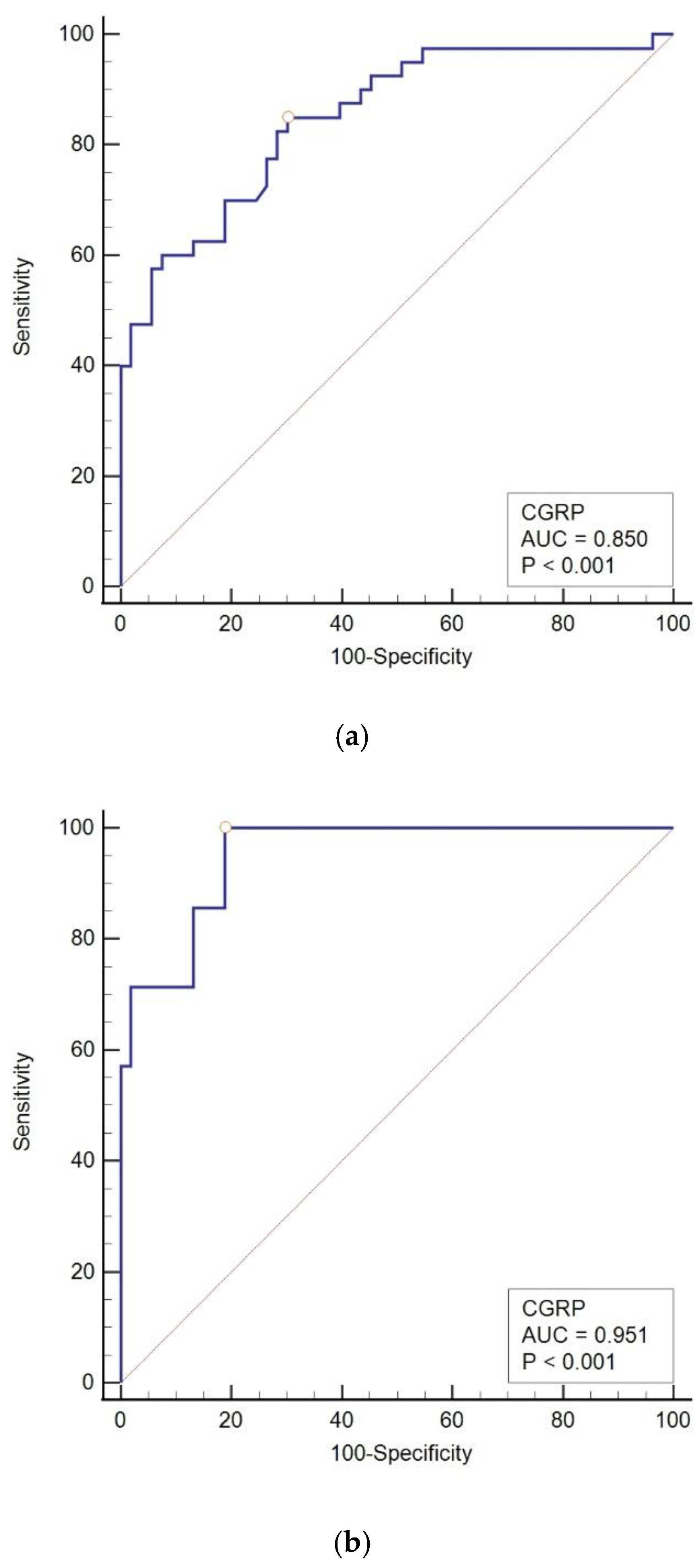
3.5. The Diagnostic Value of CGRP in Pediatric Migraine
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Philipp, J.; Zeiler, M.; Wöber, C.; Wagner, G.; Karwautz, A.F.K.; Steiner, T.J.; Wöber-Bingöl, Ç. Prevalence and burden of headache in children and adolescents in Austria—A nationwide study in a representative sample of pupils aged 10–18 years. J. Headache Pain 2019, 20, 101. [Google Scholar] [CrossRef] [PubMed]
- Arruda, M.A.; Bigal, M.E. Behavioral and emotional symptoms and primary headaches in children: A population-based study. Cephalalgia 2012, 32, 1093–1100. [Google Scholar] [CrossRef] [PubMed]
- Onofri, A.; Olivieri, L.; Silva, P.; Bernassola, M.; Tozzi, E. Correlation between primary headaches and learning disabilities in children and adolescents. Minerva Pediatr. 2022, 74, 1–6. [Google Scholar] [CrossRef]
- Guidetti, V.; Galli, F. Evolution of headache in childhood and adolescence: An 8-year follow-up. Cephalalgia 1998, 18, 449–454. [Google Scholar] [CrossRef]
- Law, E.F.; Blume, H.; Palermo, T.M. Longitudinal Impact of Parent Factors in Adolescents With Migraine and Tension-Type Headache. Headache 2020, 60, 1722–1733. [Google Scholar] [CrossRef]
- Abu-Arafeh, I.; Gelfand, A.A. The childhood migraine syndrome. Nat. Rev. Neurol. 2021, 17, 449–458. [Google Scholar] [CrossRef] [PubMed]
- Onofri, A.; Pensato, U.; Rosignoli, C.; Wells-Gatnik, W.; Stanyer, E.; Ornello, R.; Chen, H.Z.; De Santis, F.; Torrente, A.; Mikulenka, P.; et al. Primary headache epidemiology in children and adolescents: A systematic review and meta-analysis. J. Headache Pain 2023, 24, 8. [Google Scholar] [CrossRef] [PubMed]
- Stovner, L.J.; Hagen, K.; Linde, M.; Steiner, T.J. The global prevalence of headache: An update, with analysis of the influences of methodological factors on prevalence estimates. J. Headache Pain 2022, 23, 34. [Google Scholar] [CrossRef]
- Straube, A.; Andreou, A. Primary headaches during lifespan. J. Headache Pain 2019, 20, 35. [Google Scholar] [CrossRef]
- Li, X.Y.; Yang, C.H.; Lv, J.J.; Liu, H.; Zhang, L.Y.; Yin, M.Y.; Guo, Z.-L.; Zhang, R.-H. Global, regional, and national epidemiology of migraine and tension-type headache in youths and young adults aged 15-39 years from 1990 to 2019: Findings from the global burden of disease study 2019. J. Headache Pain 2023, 24, 126. [Google Scholar] [CrossRef]
- Chen, Z.F.; Kong, X.M.; Yang, C.H.; Li, X.Y.; Guo, H.; Wang, Z.W. Global, regional, and national burden and trends of migraine among youths and young adults aged 15-39 years from 1990 to 2021: Findings from the global burden of disease study 2021. J. Headache Pain 2024, 25, 131. [Google Scholar] [CrossRef]
- Kawatu, N.; Wa Somwe, S.; Ciccone, O.; Mukanzu, M.; Uluduz, D.; Şaşmaz, T.; Yalçın, B.N.B.; Wöber, C.; Steiner, T.J. The prevalence of primary headache disorders in children and adolescents in Zambia: A schools-based study. J. Headache Pain 2022, 23, 118. [Google Scholar] [CrossRef] [PubMed]
- Agbetou Houessou, M.; Adoukonou, T.; Tchuenga Fokom, W.; Dovoedo, N.; Şaşmaz, T.; Bozdağ, F.; Uluduz, D.; Steiner, T.J. The prevalence of headache disorders in children and adolescents in Benin: A schools-based study. J. Headache Pain 2024, 25, 135. [Google Scholar] [CrossRef] [PubMed]
- Togha, M.; Rafiee, P.; Haghdoost, F.; Rafie, S.; Paknejad, S.M.H.; Amouian, S.; Şaşmaz, T.; Kale, D.; Uluduz, D.; Steiner, T.J. The burdens attributable to primary headache disorders in children and adolescents in Iran: Estimates from a schools-based study. J. Headache Pain 2024, 25, 86. [Google Scholar] [CrossRef]
- Zewde, Y.Z.; Zebenigus, M.; Demissie, H.; Tekle-Haimanot, R.; Uluduz, D.; Şaşmaz, T.; Bozdag, F.; Steiner, T.J. The burden attributable to primary headache disorders in children and adolescents in Ethiopia: Estimates from a national schools-based study. J. Headache Pain 2024, 25, 47. [Google Scholar] [CrossRef] [PubMed]
- Headache Classification Committee of the International Headache Society (IHS). The International Classification of Headache Disorders, 3rd edition. Cephalalgia 2018, 38, 1–211. [Google Scholar] [CrossRef]
- Maytal, J.; Young, M.; Shechter, A.; Lipton, R.B. Pediatric migraine and the International Headache Society (IHS) criteria. Neurology 1997, 48, 602–607. [Google Scholar] [CrossRef]
- Metsähonkala, L.; Sillanpää, M. Migraine in children—An evaluation of the IHS criteria. Cephalalgia 1994, 14, 285–290. [Google Scholar] [CrossRef]
- Mortimer, M.J.; Kay, J.; Jaron, A. Childhood migraine in general practice: Clinical features and characteristics. Cephalalgia 1992, 12, 238–243; discussion 186. [Google Scholar] [CrossRef]
- Hershey, A.D.; Winner, P.; Kabbouche, M.A.; Gladstein, J.; Yonker, M.; Lewis, D.; Pearlman, E.; Linder, S.L.; Rothner, A.D.; Powers, S.W. Use of the ICHD-II Criteria in the Diagnosis of Pediatric Migraine. Headache J. Head Face Pain 2005, 45, 1288–1297. [Google Scholar] [CrossRef]
- Özge, A.; Faedda, N.; Abu-Arafeh, I.; Gelfand, A.A.; Goadsby, P.J.; Cuvellier, J.C.; Valeriani, M.; Sergeev, A.; Barlow, K.; Uludüz, D.; et al. Experts’ opinion about the primary headache diagnostic criteria of the ICHD-3rd edition beta in children and adolescents. J. Headache Pain 2017, 18, 109. [Google Scholar] [CrossRef] [PubMed]
- Chakravarty, A.; Mukherjee, A.; Roy, D. Migraine pain location at onset and during established headaches in children and adolescents: A clinic-based study from eastern India. Cephalalgia 2007, 27, 1109–1114. [Google Scholar] [CrossRef] [PubMed]
- Chakravarty, A.; Mukherjee, A.; Roy, D. Migraine pain location: How do children differ from adults? J. Headache Pain 2008, 9, 375–379. [Google Scholar] [CrossRef] [PubMed]
- Powers, S.W.; Hershey, A.D.; Coffey, C.S.; Chamberlin, L.A.; Ecklund, D.J.; Sullivan, S.; Klingner, E.A.; Yankey, J.W.; Kashikar-Zuck, S.; Korbee, L.L.; et al. The Childhood and Adolescent Migraine Prevention (CHAMP) Study: A Report on Baseline Characteristics of Participants. Headache 2016, 56, 859–870. [Google Scholar] [CrossRef]
- Ashina, S.; Mitsikostas, D.D.; Lee, M.J.; Yamani, N.; Wang, S.J.; Messina, R.; Ashina, H.; Buse, D.C.; Pozo-Rosich, P.; Jensen, R.H.; et al. Tension-type headache. Nat. Rev. Dis. Primers 2021, 7, 24. [Google Scholar] [CrossRef]
- Dodick, D.W. A Phase-by-Phase Review of Migraine Pathophysiology. Headache 2018, 58 (Suppl. 1), 4–16. [Google Scholar] [CrossRef]
- Burstein, R.; Noseda, R.; Borsook, D. Migraine: Multiple processes, complex pathophysiology. J. Neurosci. 2015, 35, 6619–6629. [Google Scholar] [CrossRef] [PubMed]
- Leao, A.A.P. Spreading depression of activity in the cerebral cortex. J. Neurophysiol. 1944, 7, 359–390. [Google Scholar] [CrossRef]
- Charles, A.C.; Baca, S.M. Cortical spreading depression and migraine. Nat. Rev. Neurol. 2013, 9, 637–644. [Google Scholar] [CrossRef]
- Zhang, X.; Levy, D.; Noseda, R.; Kainz, V.; Jakubowski, M.; Burstein, R. Activation of meningeal nociceptors by cortical spreading depression: Implications for migraine with aura. J. Neurosci. 2010, 30, 8807–8814. [Google Scholar] [CrossRef]
- Bolay, H.; Reuter, U.; Dunn, A.K.; Huang, Z.; Boas, D.A.; Moskowitz, M.A. Intrinsic brain activity triggers trigeminal meningeal afferents in a migraine model. Nat. Med. 2002, 8, 136–142. [Google Scholar] [CrossRef] [PubMed]
- Edvinsson, L. Tracing neural connections to pain pathways with relevance to primary headaches. Cephalalgia 2011, 31, 737–747. [Google Scholar] [CrossRef] [PubMed]
- Edvinsson, L.; Hara, H.; Uddman, R. Retrograde tracing of nerve fibers to the rat middle cerebral artery with true blue: Colocalization with different peptides. J. Cereb. Blood Flow Metab. 1989, 9, 212–218. [Google Scholar] [CrossRef]
- Edvinsson, L. The Trigeminovascular Pathway: Role of CGRP and CGRP Receptors in Migraine. Headache 2017, 57 (Suppl. 2), 47–55. [Google Scholar] [CrossRef]
- Messlinger, K.; Hanesch, U.; Baumgärtel, M.; Trost, B.; Schmidt, R.F. Innervation of the dura mater encephali of cat and rat: Ultrastructure and calcitonin gene-related peptide-like and substance P-like immunoreactivity. Anat. Embryol. 1993, 188, 219–237. [Google Scholar] [CrossRef]
- Messlinger, K.; Fischer, M.J.M.; Lennerz, J.K. Neuropeptide effects in the trigeminal system: Pathophysiology and clinical relevance in migraine. Keio J. Med. 2011, 60, 82–89. [Google Scholar] [CrossRef]
- Amin, F.M.; Hougaard, A.; Schytz, H.W.; Asghar, M.S.; Lundholm, E.; Parvaiz, A.I.; de Koning, P.J.H.; Andersen, M.R.; Larsson, H.B.W.; Fahrenkrug, J.; et al. Investigation of the pathophysiological mechanisms of migraine attacks induced by pituitary adenylate cyclase-activating polypeptide-38. Brain 2014, 137, 779–794. [Google Scholar] [CrossRef] [PubMed]
- Giffin, N.J.; Lipton, R.B.; Silberstein, S.D.; Olesen, J.; Goadsby, P.J. The migraine postdrome: An electronic diary study. Neurology 2016, 87, 309–313. [Google Scholar] [CrossRef]
- Bose, P.; Goadsby, P.J. The migraine postdrome. Curr. Opin. Neurol. 2016, 29, 299–301. [Google Scholar] [CrossRef]
- Kelman, L. The Postdrome of the Acute Migraine Attack. Cephalalgia 2006, 26, 214–220. [Google Scholar] [CrossRef]
- Ashina, M.; Bendtsen, L.; Jensen, R.; Schifter, S.; Jansen-Olesen, I.; Olesen, J. Plasma levels of calcitonin gene-related peptide in chronic tension-type headache. Neurology 2000, 55, 1335–1340. [Google Scholar] [CrossRef] [PubMed]
- Gupta, R.; Ahmed, T.; Banerjee, B.; Bhatia, M. Plasma calcitonin gene-related peptide concentration is comparable to control group among migraineurs and tension type headache subjects during inter-ictal period. J. Headache Pain 2009, 10, 161–166. [Google Scholar] [CrossRef] [PubMed]
- Ashina, M.; Bendtsen, L.; Jensen, R.; Schifter, S.; Olesen, J. Calcitonin gene-related peptide levels during nitric oxide-induced headache in patients with chronic tension-type headache. Eur. J. Neurol. 2001, 8, 173–178. [Google Scholar] [CrossRef]
- Han, X.; Dong, Z.; Hou, L.; Wan, D.; Chen, M.; Tang, W.; Yu, S. Interictal plasma pituitary adenylate cyclase-activating polypeptide levels are decreased in migraineurs but remain unchanged in patients with tension-type headache. Clin. Chim. Acta 2015, 450, 151–154. [Google Scholar] [CrossRef]
- Edvinsson, L.; Fredholm, B.B.; Hamel, E.; Jansen, I.; Verrecchia, C. Perivascular peptides relax cerebral arteries concomitant with stimulation of cyclic adenosine monophosphate accumulation or release of an endothelium-derived relaxing factor in the cat. Neurosci. Lett. 1985, 58, 213–217. [Google Scholar] [CrossRef]
- Brain, S.D.; Williams, T.J.; Tippins, J.R.; Morris, H.R.; MacIntyre, I. Calcitonin gene-related peptide is a potent vasodilator. Nature 1985, 313, 54–56. [Google Scholar] [CrossRef] [PubMed]
- Hanko, J.; Hardebo, J.E.; Kåhrström, J.; Owman, C.; Sundler, F. Calcitonin gene-related peptide is present in mammalian cerebrovascular nerve fibres and dilates pial and peripheral arteries. Neurosci. Lett. 1985, 57, 91–95. [Google Scholar] [CrossRef]
- Holman, J.J.; Craig, R.K.; Marshall, I. Human alpha- and beta-CGRP and rat alpha-CGRP are coronary vasodilators in the rat. Peptides 1986, 7, 231–235. [Google Scholar] [CrossRef]
- Moskowitz, M.A. Neurogenic inflammation in the pathophysiology and treatment of migraine. Neurology 1993, 43 (Suppl. 3), S16–S20. [Google Scholar]
- Nakamura-Craig, M.; Gill, B.K. Effect of neurokinin A, substance P and calcitonin gene related peptide in peripheral hyperalgesia in the rat paw. Neurosci. Lett. 1991, 124, 49–51. [Google Scholar] [CrossRef]
- Iyengar, S.; Ossipov, M.H.; Johnson, K.W. The role of calcitonin gene–related peptide in peripheral and central pain mechanisms including migraine. Pain 2017, 158, 543–559. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Z.; Winborn, C.S.; Marquez de Prado, B.; Russo, A.F. Sensitization of calcitonin gene-related peptide receptors by receptor activity-modifying protein-1 in the trigeminal ganglion. J. Neurosci. 2007, 27, 2693–2703. [Google Scholar] [CrossRef]
- Goadsby, P.J.; Edvinsson, L. The trigeminovascular system and migraine: Studies characterizing cerebrovascular and neuropeptide changes seen in humans and cats. Ann. Neurol. 1993, 33, 48–56. [Google Scholar] [CrossRef] [PubMed]
- Goadsby, P.J.; Edvinsson, L.; Ekman, R. Release of vasoactive peptides in the extracerebral circulation of humans and the cat during activation of the trigeminovascular system. Ann. Neurol. 1988, 23, 193–196. [Google Scholar] [CrossRef]
- Goadsby, P.J.; Edvinsson, L.; Ekman, R. Vasoactive peptide release in the extracerebral circulation of humans during migraine headache. Ann. Neurol. 1990, 28, 183–187. [Google Scholar] [CrossRef]
- Sarchielli, P.; Alberti, A.; Codini, M.; Floridi, A.; Gallai, V. Nitric oxide metabolites, prostaglandins and trigeminal vasoactive peptides in internal jugular vein blood during spontaneous migraine attacks. Cephalalgia 2000, 20, 907–918. [Google Scholar] [CrossRef]
- Fusayasu, E.; Kowa, H.; Takeshima, T.; Nakaso, K.; Nakashima, K. Increased plasma substance P and CGRP levels, and high ACE activity in migraineurs during headache-free periods. Pain 2007, 128, 209–214. [Google Scholar] [CrossRef] [PubMed]
- Ashina, M.; Bendtsen, L.; Jensen, R.; Schifter, S.; Olesen, J. Evidence for increased plasma levels of calcitonin gene-related peptide in migraine outside of attacks. Pain 2000, 86, 133–138. [Google Scholar] [CrossRef]
- Lassen, L.H.; Haderslev, P.A.; Jacobsen, V.B.; Iversen, H.K.; Sperling, B.; Olesen, J. CGRP may play a causative role in migraine. Cephalalgia 2002, 22, 54–61. [Google Scholar] [CrossRef] [PubMed]
- Edvinsson, L.; Linde, M. New drugs in migraine treatment and prophylaxis: Telcagepant and topiramate. Lancet 2010, 376, 645–655. [Google Scholar] [CrossRef]
- Gallai, V.; Sarchielli, P.; Floridi, A.; Franceschini, M.; Codini, M.; Glioti, G.; Trequattrini, A.; Palumbo, R. Vasoactive peptide levels in the plasma of young migraine patients with and without aura assessed both interictally and ictally. Cephalalgia 1995, 15, 384–390. [Google Scholar] [CrossRef] [PubMed]
- Fan, P.C.; Kuo, P.H.; Chang, S.H.; Lee, W.T.; Wu, R.M.; Chiou, L.C. Plasma Calcitonin Gene-Related Peptide in Diagnosing and Predicting Paediatric Migraine. Cephalalgia 2009, 29, 883–890. [Google Scholar] [CrossRef] [PubMed]
- Fan, P.C.; Kuo, P.H.; Lee, M.T.; Chang, S.H.; Chiou, L.C. Plasma Calcitonin Gene-Related Peptide: A Potential Biomarker for Diagnosis and Therapeutic Responses in Pediatric Migraine. Front. Neurol. 2019, 10, 10. [Google Scholar] [CrossRef]
- Liu, J.; Wang, G.; Dan, Y.; Liu, X. CGRP and PACAP-38 play an important role in diagnosing pediatric migraine. J. Headache Pain 2022, 23, 68. [Google Scholar] [CrossRef] [PubMed]
- Hanci, F.; Kilinc, Y.B.; Kilinc, E.; Turay, S.; Dilek, M.; Kabakus, N. Plasma levels of vasoactive neuropeptides in pediatric patients with migraine during attack and attack-free periods. Cephalalgia 2021, 41, 166–175. [Google Scholar] [CrossRef]
- Kamm, K. CGRP and Migraine: What Have We Learned From Measuring CGRP in Migraine Patients So Far? Front. Neurol. 2022, 13, 930383. [Google Scholar] [CrossRef]
- Bertin Bioreagent CGRP (Human) ELISA Kit. Available online: http://content.bertin-bioreagent.com/spibio/docs/pdf/A05481.pdf (accessed on 14 October 2024).
- Al-Khazali, H.M.; Ashina, H.; Christensen, R.H.; Wiggers, A.; Rose, K.; Iljazi, A.; Schytz, H.W.; Amin, F.M.; Ashina, M. An exploratory analysis of clinical and sociodemographic factors in CGRP-induced migraine attacks: A REFORM study. Cephalalgia 2023, 43, 3331024231206375. [Google Scholar] [CrossRef]
- Dhall, U.; Cowen, T.; Haven, A.J.; Burnstock, G. Perivascular noradrenergic and peptide-containing nerves show different patterns of changes during development and ageing in the guinea-pig. J. Auton. Nerv. Syst. 1986, 16, 109–126. [Google Scholar] [CrossRef]
- Fan, P.C.; Kuo, P.H.; Hu, J.W.; Chang, S.H.; Hsieh, S.T.; Chiou, L.C. Different trigemino-vascular responsiveness between adolescent and adult rats in a migraine model. Cephalalgia 2012, 32, 979–990. [Google Scholar] [CrossRef]
- Pérez-Pereda, S.; Toriello-Suárez, M.; Ocejo-Vinyals, G.; Guiral-Foz, S.; Castillo-Obeso, J.; Montes-Gómez, S.; Martínez-Nieto, R.M.; Iglesias, F.; González-Quintanilla, V.; Oterino, A. Serum CGRP, VIP, and PACAP usefulness in migraine: A case-control study in chronic migraine patients in real clinical practice. Mol. Biol. Rep. 2020, 47, 7125–7138. [Google Scholar] [CrossRef]
- Coppola, G.; Pierelli, F.; Schoenen, J. Is the cerebral cortex hyperexcitable or hyperresponsive in migraine? Cephalalgia 2007, 27, 1427–1439. [Google Scholar] [CrossRef] [PubMed]
- Iljazi, A.; Ashina, H.; Zhuang, Z.A.; Lopez Lopez, C.; Snellman, J.; Ashina, M.; Schytz, H.W. Hypersensitivity to calcitonin gene-related peptide in chronic migraine. Cephalalgia 2021, 41, 701–710. [Google Scholar] [CrossRef] [PubMed]
- Bille, B. A 40-year follow-up of school children with migraine. Cephalalgia 1997, 17, 488–491; discussion 487. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Migraine (n = 66) | Tension-Type Headache (n = 59) | Control (n = 53) | p-Value |
|---|---|---|---|---|
| Age (Years) | 13 (9–14) | 12 (9–16) | 13 (6–18) | 0.91 § |
| Gender (Male) | 30 (45%) | 20 (34%) | 31 (58%) | 0.03 † |
| Age at Onset | ||||
| <7 | 18 (27%) | 12 (20%) | 0.64 † | |
| 7–12 | 31 (47%) | 29 (49%) | ||
| >12 | 17 (26%) | 18 (31%) | ||
| Duration of Symptoms (Months) | 25 (11–49) | 12 (6–28) | - | 0.005 * |
| Attack duration (Hours) | 6 (3–12) | 4 (2–8) | - | 0.009 * |
| VAS | ||||
| Mild Pain | 0 | 2 (3%) | - | <0.001 † |
| Moderate Pain | 7 (11%) | 47 (80%) | - | |
| Severe Pain | 59 (89%) | 10 (17%) | - | |
| Frequency of Episodes | ||||
| Rare Episodic | 34 (52%) | 11 (19%) | - | <0.001 † |
| Frequent Episodic | 32 (48%) | 48 (81%) | - | |
| Activity-Related Aggravation | 62 (94%) | 10 (17%) | - | <0.001 † |
| Aura | 19 (29%) | - | - | - |
| Visual | 13 (20%) | - | - | - |
| Sensory | 10 (15%) | - | - | - |
| Speech | 7 (11%) | - | - | - |
| Motor | 1 (2%) | - | - | - |
| Brainstem | 1 (2%) | - | - | - |
| Concomitant Symptoms | ||||
| Nausea | 53 (80%) | 8 (14%) | - | <0.001 † |
| Vomiting | 42 (64%) | 2 (3%) | - | <0.001 † |
| Photophobia | 52 (79%) | 14 (24%) | - | <0.001 † |
| Phonophobia | 52 (79%) | 6 (10%) | - | <0.001 † |
| Location of Pain | ||||
| Unilateral | 25 (38%) | 7 (12%) | - | 0.001 † |
| Bilateral | 41 (62%) | 52 (88%) | - | - |
| Characteristics | MA (n = 19) | MO (n = 47) | p Value |
|---|---|---|---|
| Age (Years) | 14 (13–15) | 12 (9–14) | 0.001 * |
| Gender (M) | 7 (37%) | 23 (49%) | 0.37 † |
| Course (Months) | 12 (5–48) | 26 (12–50) | 0.04 * |
| Duration of Attacks (Hours) | 6 (3–10) | 4 (3–12) | 0.90 * |
| VAS (Visual Analog Scale) | |||
| Moderate Pain | 1 (5) | 6 (13) | 0.66 † |
| Severe Pain | 18 (95) | 41 (87) | |
| Frequency | |||
| Rare Episodic | 14 (74) | 20 (43) | 0.02 † |
| Frequent Episodic | 5 (26) | 27 (57) | |
| Activity-Related Aggravation | 19 (100) | 43 (92) | 0.32 † |
| Associated Symptoms | 9 (47) | 25 (88) | 0.67 † |
| Characteristic | CGRP Median (IQR) | p-Value |
|---|---|---|
| Age (years) | ||
| 0–7 | 250 (24.8–665.7) | 0.10 * |
| 7–12 | 276.7 (763.0–1030.8) | |
| 12–18 | 74.8 (19.6–646.5) | |
| Sex | ||
| Male | 274.8 (56.6–686.9) | 0.69 † |
| Female | 221.3 (23.3–932.5) | |
| Course (months) | ||
| 0–6 | 134.2 (24.4–912.1) | 0.95 * |
| 6–12 | 283.6 (54.5–990.5) | |
| 12–18 | 371.3 (56.6–813.4) | |
| 18–24 | 75.8 (56.9–559.6) | |
| >24 | 245.7 (23.3–686.9) | |
| Attack duration (hours) | ||
| 0–2 | 568.3 (91.3–1036.6) | 0.21 * |
| 2–4 | 88.3 (21.3–515.2) | |
| 4–6 | 73.3 (12–199.3) | |
| >6 | 288.7 (50.4–976.3) | |
| Frequency | ||
| Rare episodic | 96.1 (49.2–639.1) | 0.21 † |
| Frequent episodic | 303.2 (29.2–983.4) | |
| VAS (Visual Analog Scale) | ||
| Moderate pain | 617.6 (112.1–1404.7) | 0.17 † |
| Severe pain | 232.2 (31.2–771.7) | |
| Activity-related aggravation | ||
| Yes | 247.8 (49.2–813.4) | 0.47 † |
| No | 40.1 (18.1–834.2) | |
| Aura | ||
| Visual | 23.2 (11.6–359.6) | 0.009 † |
| Sensory | 31.2 (9–276.7) | 0.04 † |
| Speech | 266.4 (21.2–548.5) | 0.63 † |
| Motor | 8.7 (n = 1) | - |
| Brainstem | 266.4 (n = 1) | - |
| Concomitant symptoms | ||
| Nausea | 199.3 (32.7–671.0) | 0.34 † |
| Vomiting | 149.6 (24.8–686.9) | 0.35 † |
| Photophobia | 247.8 (23.3–806.7) | 0.65 † |
| Phonophobia | 247.8 (23.3–806.7) | 0.65 † |
| Pain localization | ||
| Unilateral | 199.3 (29.0–653.2) | 0.57 * |
| Bilateral | 247.6 (56.1–978.5) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sekelj Fures, J.; Duranovic, V.; Lenicek Krleza, J.; Katusic Bojanac, A.; Loncar, L.; Dakovic, I.; Pejic-Rosko, S.; Vulin, K.; Pilon-Far, A.; Simic Klaric, A. Calcitonin-Gene-Related Peptide in Migraine and Tension-Type Headache in Children During Interictal Period. Diagnostics 2024, 14, 2645. https://doi.org/10.3390/diagnostics14232645
Sekelj Fures J, Duranovic V, Lenicek Krleza J, Katusic Bojanac A, Loncar L, Dakovic I, Pejic-Rosko S, Vulin K, Pilon-Far A, Simic Klaric A. Calcitonin-Gene-Related Peptide in Migraine and Tension-Type Headache in Children During Interictal Period. Diagnostics. 2024; 14(23):2645. https://doi.org/10.3390/diagnostics14232645
Chicago/Turabian StyleSekelj Fures, Jadranka, Vlasta Duranovic, Jasna Lenicek Krleza, Ana Katusic Bojanac, Lana Loncar, Ivana Dakovic, Sanja Pejic-Rosko, Katarina Vulin, Andrijana Pilon-Far, and Andrea Simic Klaric. 2024. "Calcitonin-Gene-Related Peptide in Migraine and Tension-Type Headache in Children During Interictal Period" Diagnostics 14, no. 23: 2645. https://doi.org/10.3390/diagnostics14232645
APA StyleSekelj Fures, J., Duranovic, V., Lenicek Krleza, J., Katusic Bojanac, A., Loncar, L., Dakovic, I., Pejic-Rosko, S., Vulin, K., Pilon-Far, A., & Simic Klaric, A. (2024). Calcitonin-Gene-Related Peptide in Migraine and Tension-Type Headache in Children During Interictal Period. Diagnostics, 14(23), 2645. https://doi.org/10.3390/diagnostics14232645