
New Surgical Criteria for Intraductal Papillary Mucinous Neoplasm Based on the Age-Adjusted Charlson Comorbidity Index Values and Presence of Solid Component
 , , , ,
, , , ,
Abstract
1. Introduction
2. Methods
2.1. Study Design and Patients
2.2. Classification of IPMN
2.3. Age-Adjusted Charlson Comorbidity Index: ACCI
2.4. Solid Component: SC
2.5. Outcomes
2.6. Statistical Analyses
3. Results
3.1. Characteristics of Included Studies
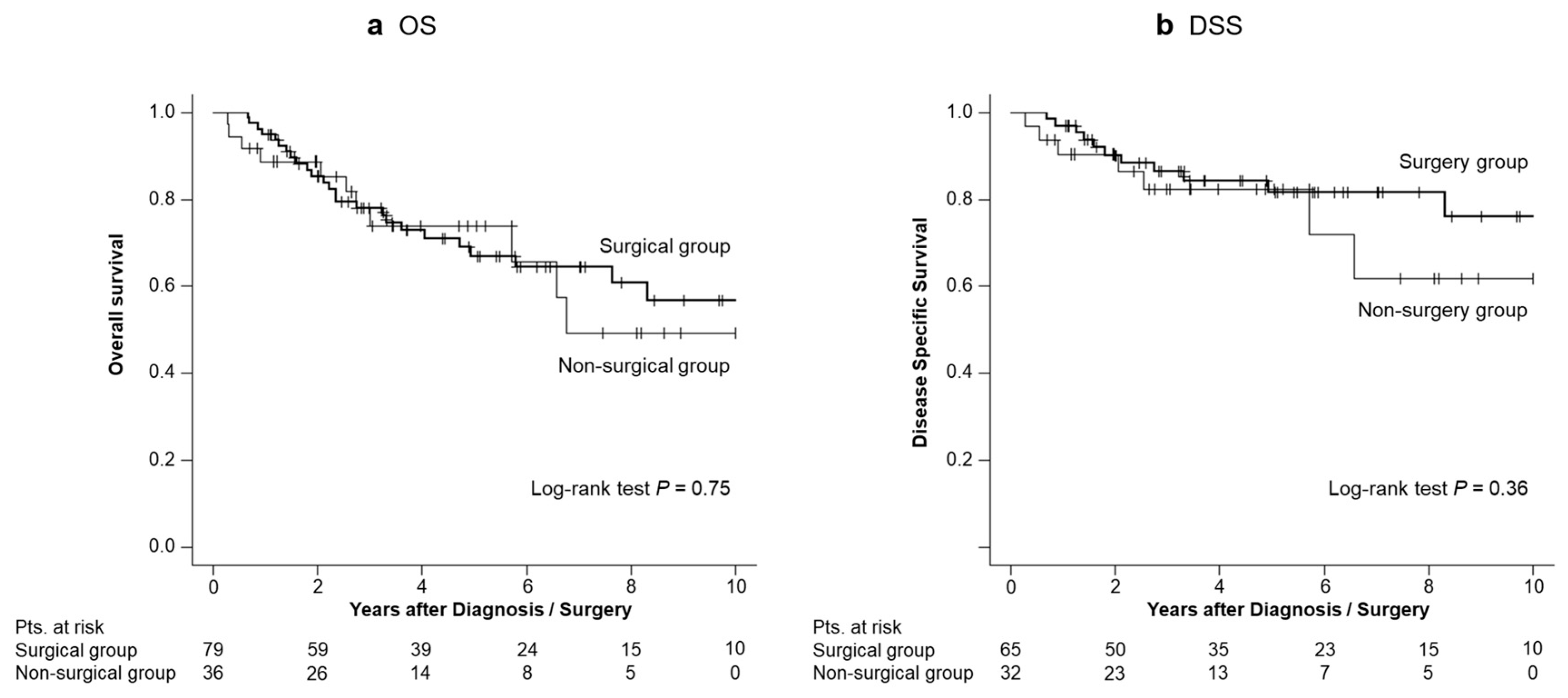
3.2. Comparison of Patient Survival Between the Surgical and Non-Surgical Groups
3.3. Factors Associated with Survival in Patients with IPMN Exhibiting HRS
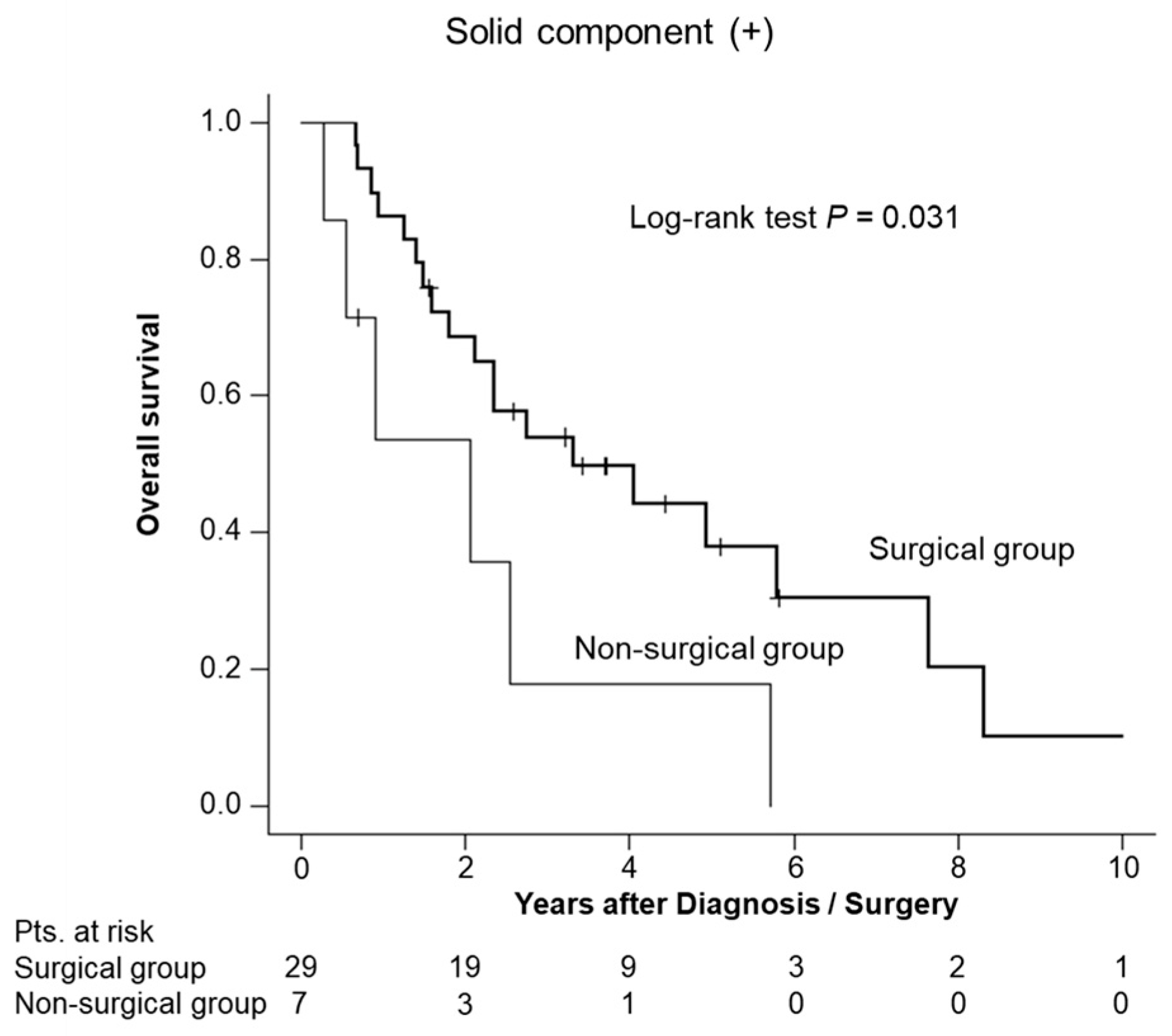
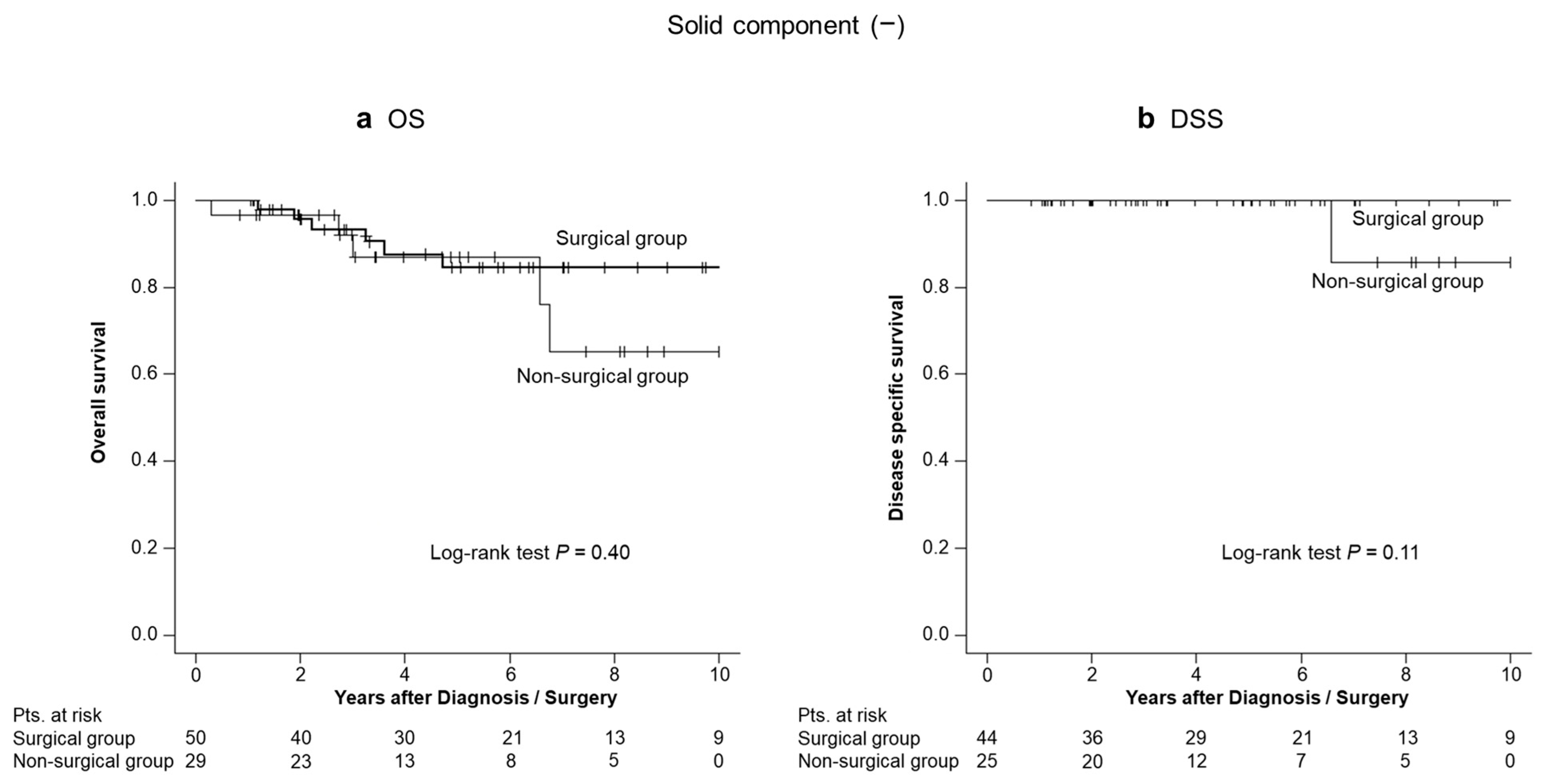
3.4. Survival Analyses Stratified by the Presence or Absence of an SC
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Oyama, H.; Tada, M.; Takagi, K.; Tateishi, K.; Hamada, T.; Nakai, Y.; Hakuta, R.; Ijichi, H.; Ishigaki, K.; Kanai, S.; et al. Long-Term Risk of Malignancy in Branch-Duct Intraductal Papillary Mucinous Neoplasms. Gastroenterology 2020, 158, 226–237.e5. [Google Scholar] [CrossRef] [PubMed]
- Lévy, P.; Jouannaud, V.; O’Toole, D.; Couvelard, A.; Vullierme, M.P.; Palazzo, L.; Aubert, A.; Ponsot, P.; Sauvanet, A.; Maire, F.; et al. Natural History of Intraductal Papillary Mucinous Tumors of the Pancreas: Actuarial Risk of Malignancy. Clin. Gastroenterol. Hepatol. 2006, 4, 460–468. [Google Scholar] [CrossRef]
- Nagata, N.; Kawazoe, A.; Mishima, S.; Wada, T.; Shimbo, T.; Sekine, K.; Watanabe, K.; Imbe, K.; Kojima, Y.; Kumazawa, K.; et al. Development of Pancreatic Cancer, Disease-Specific Mortality, and All-Cause Mortality in Patients with Nonresected IPMNs: A Long-Term Cohort Study. Radiology 2016, 278, 125–134. [Google Scholar] [CrossRef]
- Tanaka, M.; Fernández-del Castillo, C.; Kamisawa, T.; Jang, J.Y.; Levy, P.; Ohtsuka, T.; Salvia, R.; Shimizu, Y.; Tada, M.; Wolfgang, C.L. Revisions of International Consensus Fukuoka Guidelines for the Management of IPMN of the Pancreas. Pancreatology 2017, 17, 738–753. [Google Scholar] [CrossRef]
- Ohtsuka, T.; Fernandez-del Castillo, C.; Furukawa, T.; Hijioka, S.; Jang, J.Y.; Lennon, A.M.; Miyasaka, Y.; Ohno, E.; Salvia, R.; Wolfgang, C.L.; et al. International Evidence-Based Kyoto Guidelines for the Management of Intraductal Papillary Mucinous Neoplasm of the Pancreas. Pancreatology 2024, 24, 255–270. [Google Scholar] [CrossRef] [PubMed]
- Sultana, A.; Jackson, R.; Tim, G.; Bostock, E.; Psarelli, E.E.; Cox, T.F.; Sutton, R.; Ghaneh, P.; Raraty, M.G.T.; Neoptolemos, J.P.; et al. What Is the Best Way to Identify Malignant Transformation Within Pancreatic IPMN: A Systematic Review and Meta-Analyses. Clin. Transl. Gastroenterol. 2015, 6, e130. [Google Scholar] [CrossRef] [PubMed]
- Sho, M.; Murakami, Y.; Kawai, M.; Motoi, F.; Satoi, S.; Matsumoto, I.; Honda, G.; Uemura, K.; Yanagimoto, H.; Kurata, M.; et al. Prognosis after Surgical Treatment for Pancreatic Cancer in Patients Aged 80 Years or Older: A Multicenter Study. J. Hepatobiliary Pancreat. Sci. 2016, 23, 188–197. [Google Scholar] [CrossRef]
- Beger, H.G.; Mayer, B. Early Postoperative and Late Metabolic Morbidity after Pancreatic Resections: An Old and New Challenge for Surgeons-A Review. Am. J. Surg. 2018, 216, 131–134. [Google Scholar] [CrossRef]
- DeOliveira, M.L.; Winter, J.M.; Schafer, M.; Cunningham, S.C.; Cameron, J.L.; Yeo, C.J.; Clavien, P.A. Assessment of Complications after Pancreatic Surgery: A Novel Grading System Applied to 633 Patients Undergoing Pancreaticoduodenectomy. Ann. Surg. 2006, 244, 931–937. [Google Scholar] [CrossRef]
- Sakai, A.; Masuda, A.; Eguchi, T.; Anami, T.; Nishi, K.; Furumatsu, K.; Okabe, Y.; Kakuyama, S.; Sato, Y.; Nishioka, C.; et al. Clinical Outcome of Conservatively Managed Pancreatic Intraductal Papillary Mucinous Neoplasms with Mural Nodules and Main Duct Dilation. J. Gastroenterol. 2021, 56, 285–292. [Google Scholar] [CrossRef]
- Vanella, G.; Crippa, S.; Archibugi, L.; Arcidiacono, P.G.; Delle Fave, G.; Falconi, M.; Capurso, G. Meta-Analysis of Mortality in Patients with High-Risk Intraductal Papillary Mucinous Neoplasms under Observation. Br. J. Surg. 2018, 105, 328–338. [Google Scholar] [CrossRef] [PubMed]
- Sharib, J.M.; Fonseca, A.L.; Swords, D.S.; Jaradeh, K.; Bracci, P.M.; Firpo, M.A.; Hatcher, S.; Scaife, C.L.; Wang, H.; Kim, G.E.; et al. Surgical Overtreatment of Pancreatic Intraductal Papillary Mucinous Neoplasms: Do the 2017 International Consensus Guidelines Improve Clinical Decision Making? Surgery 2018, 164, 1178–1184. [Google Scholar] [CrossRef] [PubMed]
- Watanabe, Y.; Endo, S.; Nishihara, K.; Ueda, K.; Mine, M.; Tamiya, S.; Nakano, T.; Tanaka, M. The Validity of the Surgical Indication for Intraductal Papillary Mucinous Neoplasm of the Pancreas Advocated by the 2017 Revised International Association of Pancreatology Consensus Guidelines. Surg. Today 2018, 48, 1011–1019. [Google Scholar] [CrossRef] [PubMed]
- Yamakawa, K.; Masuda, A.; Nakagawa, T.; Shiomi, H.; Toyama, H.; Takenaka, M.; Sakai, A.; Kobayashi, T.; Tsujimae, M.; Ashina, S.; et al. Evaluation of Efficacy of Pancreatic Juice Cytology for Risk Classification According to International Consensus Guidelines in Patients with Intraductal Papillary Mucinous Neoplasm; a Retrospective Study. Pancreatology 2019, 19, 424–428. [Google Scholar] [CrossRef]
- Marchegiani, G.; Andrianello, S.; Borin, A.; Dal Borgo, C.; Perri, G.; Pollini, T.; Romanò, G.; D’Onofrio, M.; Gabbrielli, A.; Scarpa, A.; et al. Systematic Review, Meta-Analysis, and a High-Volume Center Experience Supporting the New Role of Mural Nodules Proposed by the Updated 2017 International Guidelines on IPMN of the Pancreas. Surgery 2018, 163, 1272–1279. [Google Scholar] [CrossRef]
- Dias-Santos, D.; Ferrone, C.R.; Zheng, H.; Lillemoe, K.D.; Fernández-Del Castillo, C. The Charlson Age Comorbidity Index Predicts Early Mortality after Surgery for Pancreatic Cancer. Surgery 2015, 157, 881–887. [Google Scholar] [CrossRef] [PubMed]
- Asano, T.; Yamada, S.; Fujii, T.; Yabusaki, N.; Nakayama, G.; Sugimoto, H.; Koike, M.; Fujiwara, M.; Kodera, Y. The Charlson Age Comorbidity Index Predicts Prognosis in Patients with Resected Pancreatic Cancer. Int. J. Surg. 2017, 39, 169–175. [Google Scholar] [CrossRef]
- Tian, Y.; Jian, Z.; Xu, B.; Liu, H. Age-Adjusted Charlson Comorbidity Index Score as Predictor of Survival of Patients with Digestive System Cancer Who Have Undergone Surgical Resection. Oncotarget 2017, 8, 79453–79461. [Google Scholar] [CrossRef]
- Aoyama, T.; Yamamoto, N.; Kamiya, M.; Murakawa, M.; Tamagawa, H.; Sawazaki, S.; Numata, M.; Kobayashi, S.; Ueno, M.; Morimoto, M.; et al. The Age-Adjusted Charlson Comorbidity Index Is an Independent Prognostic Factor in Pancreatic Cancer Patients Who Receive Curative Resection Followed by Adjuvant Chemotherapy. J. Cancer Res. Ther. 2020, 16, S116–S121. [Google Scholar] [CrossRef]
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, C.R. A New Method of Classifying Prognostic Comorbidity in Longitudinal Studies: Development and Validation. J. Chronic Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef]
- Kawamoto, S.; Lawler, L.P.; Horton, K.M.; Eng, J.; Hruban, R.H.; Fishman, E.K. MDCT of Intraductal Papillary Mucinous Neoplasm of the Pancreas: Evaluation of Features Predictive of Invasive Carcinoma. Am. J. Roentgenol. 2006, 186, 687–695. [Google Scholar] [CrossRef] [PubMed]
- Vullierme, M.-P.; Giraud-Cohen, M.; Hammel, P.; Sauvanet, A.; Couvelard, A.; O’Toole, D.; Levy, P.; Ruszniewski, P.; Vilgrain, V. Malignant Intraductal Papillary Mucinous Neoplasm of the Pancreas: In Situ versus Invasive Carcinoma Surgical Resectability. Radiology 2007, 245, 483–490. [Google Scholar] [CrossRef] [PubMed]
- Kobayashi, G.; Fujita, N.; Noda, Y.; Obana, T.; Takasawa, O. Ultrasonographic Findings and Natural History of Intraductal Papillary-Mucinous Neoplasms of the Pancreas. J. Med. Ultrason. 2008, 35, 85–96. [Google Scholar] [CrossRef] [PubMed]
- Walter, T.C.; Steffen, I.G.; Stelter, L.H.; Maurer, M.H.; Bahra, M.; Faber, W.; Klein, F.; Bläker, H.; Hamm, B.; Denecke, T.; et al. Implications of Imaging Criteria for the Management and Treatment of Intraductal Papillary Mucinous Neoplasms-Benign versus Malignant Findings. Eur. Radiol. 2015, 25, 1329–1338. [Google Scholar] [CrossRef]
- Yamao, K.; Ohashi, K.; Nakamura, T.; Suzuki, T.; Watanabe, Y.; Shimizu, Y.; Nakamura, Y.; Ozden, I. Evaluation of Various Imaging Methods in the Differential Diagnosis of Intraductal Papillary-Mucinous Tumor (IPMT) of the Pancreas. Hepato-Gastroenterology 2001, 48, 962–966. [Google Scholar]
- Nara, S.; Onaya, H.; Hiraoka, N.; Shimada, K.; Sano, T.; Sakamoto, Y.; Esaki, M.; Kosuge, T. Preoperative Evaluation of Invasive and Noninvasive Intraductal Papillary-Mucinous Neoplasms of the Pancreas: Clinical, Radiological, and Pathological Analysis of 123 Cases. Pancreas 2009, 38, 8–16. [Google Scholar] [CrossRef]
- Do, R.K.G.; Katz, S.S.; Gollub, M.J.; Li, J.; LaFemina, J.; Zabor, E.C.; Moskowitz, C.S.; Klimstra, D.S.; Allen, P.J. Interobserver Agreement for Detection of Malignant Features of Intraductal Papillary Mucinous Neoplasms of the Pancreas on MDCT. Am. J. Roentgenol. 2014, 203, 973–979. [Google Scholar] [CrossRef]
- Kanda, Y. Investigation of the Freely Available Easy-to-Use Software “EZR” for Medical Statistics. Bone Marrow Transplant. 2013, 48, 452–458. [Google Scholar] [CrossRef]
- Crippa, S.; Bassi, C.; Salvia, R.; Malleo, G.; Marchegiani, G.; Rebours, V.; Levy, P.; Partelli, S.; Suleiman, S.L.; Banks, P.A.; et al. Low Progression of Intraductal Papillary Mucinous Neoplasms with Worrisome Features and High-Risk Stigmata Undergoing Non-Operative Management: A Mid-Term Follow-up Analysis. Gut 2017, 66, 495–506. [Google Scholar] [CrossRef]
- Sahora, K.; Ferrone, C.R.; Brugge, W.R.; Morales-Oyarvide, V.; Warshaw, A.L.; Lillemoe, K.D.; Fernández-del Castillo, C. Effects of Comorbidities on Outcomes of Patients With Intraductal Papillary Mucinous Neoplasms. Clin. Gastroenterol. Hepatol. 2015, 13, 1816–1823. [Google Scholar] [CrossRef]
- Lee, B.S.; Nguyen, A.K.; Tekeste, T.F.; Chang, K.; Girgis, A.; Adeyemo, M.; Hanna, M.S.; Yao, J.F.; Kwok, K.K.; Giap, A.Q.; et al. Long-Term Follow-up of Branch-Duct Intraductal Papillary Mucinous Neoplasms with No Change in First 5 Years of Diagnosis. Pancreatology 2021, 21, 144–154. [Google Scholar] [CrossRef] [PubMed]
- Facciorusso, A.; Crinò, S.F.; Ramai, D.; Madhu, D.; Fugazza, A.; Carrara, S.; Spadaccini, M.; Mangiavillano, B.; Gkolfakis, P.; Mohan, B.P.; et al. Comparative Diagnostic Performance of Different Techniques for EUS-Guided Fine-Needle Biopsy Sampling of Solid Pancreatic Masses: A Network Meta-Analysis. Gastrointest. Endosc. 2023, 97, 839–848.e5. [Google Scholar] [CrossRef] [PubMed]
- Crinò, S.F.; Bernardoni, L.; Gabbrielli, A.; Capelli, P.; Salvia, R.; Rusev, B.C.; Scarpa, A.; Manfrin, E. Beyond Pancreatic Cyst Epithelium: Evidence of Ovarian-Like Stroma in EUS-Guided Through-the-Needle Micro-Forceps Biopsy Specimens. Am. J. Gastroenterol. 2018, 113, 1059–1060. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Surgical Group | Non-Surgical Group | p Value | |
|---|---|---|---|
| (n = 79) | (n = 36) | ||
| Median age, years (IQR) | 72 (65–77) | 81 (77–83) | <0.001 * |
| Male, n (%) | 51 (65) | 22 (61) | 0.88 |
| Median ACCI (IQR) | 4 (2–5) | 5 (4–5) | 0.001 * |
| MD/MIX type, n (%) | 55 (70) | 24 (67) | 0.92 |
| Median MPD, mm (IQR) | 7 (3.8–11) | 10 (3.8–11) | 0.70 |
| Median Mural nodule, mm (IQR) | 7 (3.5–11.5) | 6 (0–8) | 0.18 |
| Jaundice, n (%) | 5 (6) | 0 | 0.29 |
| Solid component, n (%) | 29 (37) | 7 (19) | 0.10 |
| Death, n (%) | 26 (32) | 11 (30) | 0.70 |
| IPMN-related death, n (%) | 12 (15) | 7 (19) | |
| IPMN-unrelated death, n (%) | 9 (11) | 3 (8) | |
| Unknown, n (%) | 5 (6) | 1 (3) | |
| Pathological diagnoses | |||
| low-grade dysplasia, n (%) | 29 (37) | ||
| high-grade dysplasia, n (%) | 21 (26) | ||
| IPMN-derived invasive carcinoma, n (%) | 29 (37) |
| Univariate Analysis | Multivariate Analysis | ||||||
|---|---|---|---|---|---|---|---|
| No. | 5-Year OS (%) | p Value | HR | 95% CI | p Value | ||
| Age | ≥75 | 60 | 64 | 0.018 | 1.73 | 0.85–3.52 | 0.13 |
| Sex | Male | 73 | 63 | 0.68 | |||
| ACCI | ≥5 | 41 | 55 | <0.001 | 2.27 | 1.11–4.64 | 0.025 * |
| IPMN type | MD/MIX | 79 | 68 | 0.35 | |||
| MPD | ≥10 mm | 53 | 64 | 0.65 | |||
| Mural nodule | ≥5 mm | 80 | 70 | 0.56 | |||
| Jaundice | Present | 5 | NA | 0.028 | 2.03 | 0.56–7.43 | 0.28 |
| Solid component | Present | 36 | 35 | <0.001 | 6.92 | 3.30–14.5 | <0.001 * |
| Pancreatectomy | Yes | 79 | 67 | 0.75 | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hasegawa, H.; Fukasawa, M.; Takano, S.; Kawakami, S.; Kuratomi, N.; Harai, S.; Yoshimura, D.; Imagawa, N.; Okuwaki, T.; Kuno, T.; et al. New Surgical Criteria for Intraductal Papillary Mucinous Neoplasm Based on the Age-Adjusted Charlson Comorbidity Index Values and Presence of Solid Component. Diagnostics 2024, 14, 2582. https://doi.org/10.3390/diagnostics14222582
Hasegawa H, Fukasawa M, Takano S, Kawakami S, Kuratomi N, Harai S, Yoshimura D, Imagawa N, Okuwaki T, Kuno T, et al. New Surgical Criteria for Intraductal Papillary Mucinous Neoplasm Based on the Age-Adjusted Charlson Comorbidity Index Values and Presence of Solid Component. Diagnostics. 2024; 14(22):2582. https://doi.org/10.3390/diagnostics14222582
Chicago/Turabian StyleHasegawa, Hiroyuki, Mitsuharu Fukasawa, Shinichi Takano, Satoshi Kawakami, Natsuhiko Kuratomi, Shota Harai, Dai Yoshimura, Naoto Imagawa, Tetsuya Okuwaki, Toru Kuno, and et al. 2024. "New Surgical Criteria for Intraductal Papillary Mucinous Neoplasm Based on the Age-Adjusted Charlson Comorbidity Index Values and Presence of Solid Component" Diagnostics 14, no. 22: 2582. https://doi.org/10.3390/diagnostics14222582
APA StyleHasegawa, H., Fukasawa, M., Takano, S., Kawakami, S., Kuratomi, N., Harai, S., Yoshimura, D., Imagawa, N., Okuwaki, T., Kuno, T., Suzuki, Y., Yoshida, T., Kobayashi, S., Sato, M., Maekawa, S., Hosomura, N., Kawaida, H., Ichikawa, D., & Enomoto, N. (2024). New Surgical Criteria for Intraductal Papillary Mucinous Neoplasm Based on the Age-Adjusted Charlson Comorbidity Index Values and Presence of Solid Component. Diagnostics, 14(22), 2582. https://doi.org/10.3390/diagnostics14222582