
The Impact of IL1B rs1143634 and DEFB1 rs11362 Variants on Periodontitis Risk in Phenylketonuria and Type 1 Diabetes Mellitus Patients in a Latvian Population

 , , , and
, , , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Ethics
2.2. Study Subjects
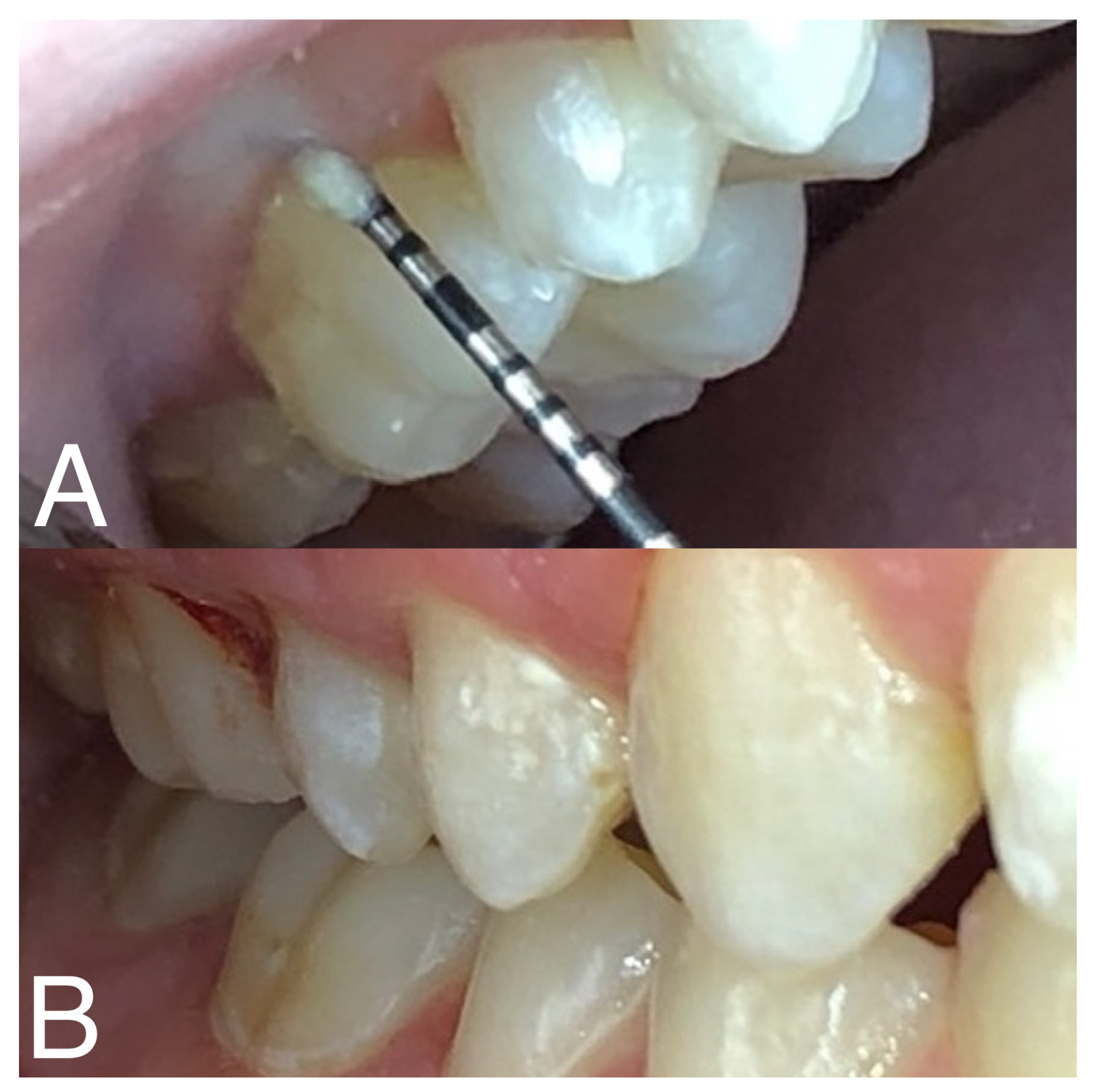
2.3. Oral Health Assessment
2.4. Genotyping
2.5. Statistical Analysis
3. Results
3.1. Oral Hygiene Assessment
3.2. Genetic Analysis Results
3.3. DEFB1 rs11362
3.4. IL1B rs1143634
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kwon, T.H.; Lamster, I.B.; Levin, L. Current Concepts in the Management of Periodontitis. Int. Dent. J. 2021, 71, 462–476. [Google Scholar] [CrossRef] [PubMed]
- Brodzikowska, A.; Górski, B.; Bogusławska-Kapała, A. Association between IL-1 Gene Polymorphisms and Stage III Grade B Periodontitis in Polish Population. Int. J. Environ. Res. Public. Health 2022, 19, 14687. [Google Scholar] [CrossRef] [PubMed]
- Kinane, D.F.; Stathopoulou, P.G.; Papapanou, P.N. Periodontal diseases. Nat. Rev. Dis. Primers 2017, 3, 17038. [Google Scholar] [CrossRef]
- Tonetti, M.S.; Greenwell, H.; Kornman, K.S. Staging and grading of periodontitis: Framework and proposal of a new classification and case definition. J. Clin. Periodontol. 2018, 45, S149–S161. [Google Scholar] [CrossRef] [PubMed]
- Räisänen, I.T.; Aji, N.R.A.S.; Sakellari, D.; Grigoriadis, A.; Rantala, I.; Pätilä, T.; Heikkilä, P.; Gupta, S.; Sorsa, T. Active Matrix Metalloproteinase-8 (aMMP-8) Versus Total MMP-8 in Periodontal and Peri-Implant Disease Point-of-Care Diagnostics. Biomedicines 2023, 11, 2885. [Google Scholar] [CrossRef] [PubMed]
- Sorsa, T.; Alassiri, S.; Grigoriadis, A.; Räisänen, I.T.; Pärnänen, P.; Nwhator, S.O.; Gieselmann, D.-R.; Sakellari, D. Active MMP-8 (AMMP-8) as a grading and staging biomarker in the periodontitis classification. Diagnostics 2020, 10, 61. [Google Scholar] [CrossRef] [PubMed]
- de Alencar, J.B.; Zacarias, J.M.V.; Tsuneto, P.Y.; Souza, V.H.D.; Silva, C.D.O.E.; Visentainer, J.E.L.; Sell, A.M. Influence of inflammasome NLRP3, and IL1B and IL2 gene polymorphisms in periodontitis susceptibility. PLoS ONE 2020, 15, e0227905. [Google Scholar] [CrossRef]
- Brodzikowska, A.; Górska, R.; Kowalski, J. Interleukin-1 Genotype in Periodontitis. Arch. Immunol. Ther. Exp. 2019, 67, 367–373. [Google Scholar] [CrossRef]
- da Silva, F.; Guimaraes-Vasconcelos, A.; De-Carvalho-Franca, L.; Di-Lenardo, D.; Rodrigues, L.; Barreto-Do-Nascimento, M.; Vasconcelos, D. Relationship between -889 C/T polymorphism in interleukin-1A gene and risk of chronic periodontitis: Evidence from a meta-analysis with new published findings. Med. Oral Patol. Oral Cir. Bucal 2017, 22, e7–e14. [Google Scholar] [CrossRef]
- Ding, C.; Zhao, L.; Sun, Y.; Li, L.; Xu, Y. Interleukin-1 receptor antagonist polymorphism (rs2234663) and periodontitis susceptibility: A meta-analysis. Arch. Oral. Biol. 2012, 57, 585–593. [Google Scholar] [CrossRef]
- Ma, L.; Chu, W.M.; Zhu, J.; Wu, Y.N.; Wang, Z.L. Interleukin-1β (3953/4) C→T polymorphism increases the risk of chronic periodontitis in Asians: Evidence from a meta-analysis of 20 case-control studies. Arch. Med. Sci. 2015, 11, 267–273. [Google Scholar] [CrossRef] [PubMed]
- Dahash, S.A.; Hussein, K.L. Interleukin-1β rs1143634 Polymorphism and Susceptibility to Periodontitis in the Iraqi Population. Arch. Razi Inst. 2023, 78, 751–756. [Google Scholar] [CrossRef] [PubMed]
- Abdellatif, H.M.; Binshabaib, M.S.; Shawky, H.A.; Alharthi, S.S. Association between periodontitis and genetic polymorphisms in interleukins among patients with diabetes mellitus. Dent. J. 2021, 9, 45. [Google Scholar] [CrossRef] [PubMed]
- Yin, W.T.; Pan, Y.P.; Lin, L. Association between IL-1α rs17561 and IL-1β rs1143634 polymorphisms and periodontitis: A meta-analysis. Genet. Mol. Res. 2016, 15, 15017325. [Google Scholar] [CrossRef]
- Ślebioda, Z.; Szponar, E.; Kowalska, A. Defensins and their role in the maintenance of the oral cavity homeostasis—A literature review. Cent.-Eur. J. Immunol. 2013, 38, 111–117. [Google Scholar] [CrossRef]
- Ślebioda, Z.; Woźniak, T.; Dorocka-Bobkowska, B.; Woźniewicz, M.; Kowalska, A. Beta-defensin 1 gene polymorphisms in the pathologies of the oral cavity—Data from meta-analysis: Association only with rs1047031 not with rs1800972, rs1799946, and rs11362. J. Oral. Pathol. Med. 2021, 50, 22–31. [Google Scholar] [CrossRef]
- Zupin, L.; Robino, A.; Navarra, C.O.; Pirastu, N.; Di Lenarda, R.; Gasparini, P.; Crovella, S.; Bevilacqua, L. LTF and DEFB1 polymorphisms are associated with susceptibility toward chronic periodontitis development. Oral Dis. 2017, 23, 1001–1008. [Google Scholar] [CrossRef]
- Ballikaya, E.; Yildiz, Y.; Sivri, H.S.; Tokatli, A.; Dursun, A.; Olmez, S.; Coskun, T.; Tekcicek, M.U. Oral health status of children with phenylketonuria. J. Pediatr. Endocrinol. Metab. 2020, 33, 361–365. [Google Scholar] [CrossRef]
- DiMeglio, L.A.; Evans-Molina, C.; Oram, R.A. Type 1 diabetes. Lancet 2018, 391, 2449–2462. [Google Scholar] [CrossRef]
- Ismail, A.F.; McGrath, C.P.; Yiu, C.K.Y. Oral health of children with type 1 diabetes mellitus: A systematic review. Diabetes Res. Clin. Pract. 2015, 108, 369–381. [Google Scholar] [CrossRef]
- Ramfjord, S.P. Indices for Prevalence and Incidence of Periodontal Disease. J. Periodontol. 1959, 30, 51–59. [Google Scholar] [CrossRef]
- Greene, J.C.; Vermillion, J.R. The simplified oral hygiene index. J. Am. Dent. Assoc. 1964, 68, 7–13. [Google Scholar] [CrossRef] [PubMed]
- Hsieh, Y.J.; Chang, Y.C.; Huang, Y.H.; Chung, W.H.; Tsai, H.Y.; Hsu, L.A. A lack of association between genetic polymorphisms in beta-defensins and susceptibility of psoriasis in Taiwanese: A case-control study. Dermatol. Sin. 2016, 34, 78–82. [Google Scholar] [CrossRef]
- Meenakshi, P.; Ramya, S.; Shruthi, T.; Lavanya, J.; Mohammed, H.H.; Mohammed, S.A.; Vijayalakshmi, V.; Sumanlatha, G. Association of IL-1β +3954 C/T and IL-10-1082 G/A cytokine gene polymorphisms with susceptibility to tuberculosis. Scand. J. Immunol. 2013, 78, 92–97. [Google Scholar] [CrossRef] [PubMed]
- Purcell, S.; Neale, B.; Todd-Brown, K.; Thomas, L.; Ferreira, M.A.R.; Bender, D.; Maller, J.; Sklar, P.; de Bakker, P.I.W.; Daly, M.J.; et al. PLINK: A tool set for whole-genome association and population-based linkage analyses. Am. J. Hum. Genet. 2007, 81, 559–575. [Google Scholar] [CrossRef]
- Ajwani, S. Periodontal Disease in an Aged Population, and Its Role in Cardiovascular Mortality; University of Helsinki: Helsinki, Finland, 2003. [Google Scholar]
- Kinane, D.F.; Hart, T.C. Genes and gene polymorphisms associated with periodontal disease. Crit. Rev. Oral. Biol. Med. 2003, 14, 430–449. [Google Scholar] [CrossRef] [PubMed]
- Salvi, G.E.; Lawrence, H.P.; Offenbacher, S.; Beck, D. Influence of risk factors on the pathogenesis of periodontitis Risk factors. Periodontology 2000, 14, 173–201. [Google Scholar] [CrossRef] [PubMed]
- Lucas, V.S.; Contreras, A.; Loukissa, M.; Roberts, G.J. Dental disease indices and caries related oral microflora in children with phenylketonuria. ASDC J. Dent. Child. 2001, 68, 263–267. [Google Scholar]
- Singh-Hüsgen, P.; Meissner, T.; Bizhang, M.; Henrich, B.; Raab, W.H.M. Investigation of the oral status and microorganisms in children with phenylketonuria and type 1 diabetes. Clin. Oral. Investig. 2016, 20, 841–847. [Google Scholar] [CrossRef]
- Ikuta, T.; Inagaki, Y.; Tanaka, K.; Saito, T.; Nakajima, Y.; Bando, M.; Kido, J.-I.; Nagata, T. Gene polymorphism of β-defensin-1 is associated with susceptibility to periodontitis in Japanese. Odontology 2015, 103, 66–74. [Google Scholar] [CrossRef]
- Zhong, S.; Wang, C.; Gao, R.; Shu, S.; Shu, C. Association between DEFB1 polymorphisms and periodontitis: A meta-analysis. Pharmazie 2019, 74, 390–396. [Google Scholar] [CrossRef]
- Shao, J.; Zhang, M.; Wu, L.; Jia, X.W.; Jin, Y.H.; Zeng, X.T. DEFB1rs11362 polymorphism and risk of chronic periodontitis: A meta-analysis of unadjusted and adjusted data. Front. Genet. 2019, 10, 179. [Google Scholar] [CrossRef] [PubMed]
- Navarra, C.O.; Robino, A.; Pirastu, N.; Bevilacqua, L.; Gasparini, P.; Di Lenarda, R.; Crovella, S. Caries and Innate Immunity: DEFB1 Gene Polymorphisms and Caries Susceptibility in Genetic Isolates from North-Eastern Italy. Caries Res. 2016, 50, 589–594. [Google Scholar] [CrossRef]
- Ozturk, A.; Famili, P.; Vieira, A.R. The antimicrobial peptide DEFB1 is associated with caries. J. Dent. Res. 2010, 89, 631–636. [Google Scholar] [CrossRef] [PubMed]
- Isaza-Guzmán, D.M.; Hernández-Viana, M.; Bonilla-León, D.M.; Hurtado-Cadavid, M.C.; Tobón-Arroyave, S.I. Determination of NLRP3 (rs4612666) and IL-1B (rs1143634) genetic polymorphisms in periodontally diseased and healthy subjects. Arch. Oral Biol. 2016, 65, 44–51. [Google Scholar] [CrossRef]
- Mesa, F.; Lanza, E.; García, L.; Marfil-Alvarez, R.; Magan-Fernandez, A. Polymorphism IL-1RN rs419598 reduces the susceptibility to generalized periodontitis in a population of European descent. PLoS ONE 2017, 12, e0186366. [Google Scholar] [CrossRef]
- da Silva, F.R.P.; Vasconcelos, A.C.C.G.; de Carvalho França, L.F.; Di Lenardo, D.; Nascimento, H.M.S.; Vasconcelos, D.F.P. Association between the rs1143634 polymorphism in interleukin-1B and chronic periodontitis: Results from a meta-analysis composed by 54 case/control studies. Gene 2018, 668, 97–106. [Google Scholar] [CrossRef] [PubMed]
- Azzola, L.G.; Fankhauser, N.; Srinivasan, M. Influence of the vegan, vegetarian and omnivore diet on the oral health status in adults: A systematic review and meta-analysis. Evid. Based Dent. 2023, 24, 43–44. [Google Scholar] [CrossRef]
- Atarbashi-Moghadam, F.; Moallemi-Pour, S.; Atarbashi-Moghadam, S.; Sijanivandi, S.; Baghban, A.A. Effects of raw vegan diet on periodontal and dental parameters. Tzu Chi Med. J. 2020, 32, 357–361. [Google Scholar] [CrossRef]
- Eberhard, J.; Ruiz, K.; Tan, J.; Jayasinghe, T.N.; Khan, S.; Eroglu, E.; Adler, C.; Simpson, S.J.; Le Couteur, D.G.; Raubenheimer, D.; et al. A randomized clinical trial to investigate the effect of dietary protein sources on periodontal health. J. Clin. Periodontol. 2022, 49, 388–400. [Google Scholar] [CrossRef]
- Hamdy, O.; Barakatun-Nisak, M.Y. Nutrition in Diabetes. Endocrinol. Metab. Clin. N. Am. 2016, 45, 799–817. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
| Genetic Variant | HGVS, Minor Allele | Primer Sequences | Restriction Enzyme |
|---|---|---|---|
| IL1B rs1143634 | NM_000576.3:c.315C > T p.(Phe105=), T (A *) | 5′-GTTGTCATCAGACTTTGACC-3′ 5′-TTCAGTTCATATGGACCAGA-3′ | Taq1 (fragments for A allele 250 bp, for G allele 135 and 115 bp) [24] |
| DEFB1 rs11362 | NM_005218.4:c.-20G > A p.(?), A (T *) | 5′-CAGGGGTTAGCGATTAG-3′ 5′-GCAGAGAGTAAACAGAAGGTA-3′ | BstnI (fragments for G allele 167 bp and 60 bp, for A allele 227 bp) [23] |
| PKU Group (n = 43) | T1DM Group (n = 28) | Control Group (n = 63) | ||||
|---|---|---|---|---|---|---|
| Frequency of teeth brushing | ||||||
| Do not brush | 4 | 9% | 0 | 0% | 0 | 0% |
| Once per day | 13 | 30% | 12 | 43% | 2 | 3% |
| Twice per day | 26 | 60% | 16 | 57% | 61 | 97% |
| p * < 0.001 | p * < 0.001 | |||||
| Use of supplementary oral hygiene items | ||||||
| Do not use | 33 | 77% | 15 | 54% | 21 | 33% |
| Dental floss | 6 | 14% | 11 | 39% | 41 | 65% |
| Mouthwash | 4 | 9% | 2 | 7% | 1 | 2% |
| p * < 0.001 | p * = 0.048 | |||||
| PKU Group (n = 43) | T1DM Group (n = 28) | Control Group (n = 63) | ||||
|---|---|---|---|---|---|---|
| Calculus removal necessity | ||||||
| Not needed | 3 | 7% | 9 | 32% | 29 | 46% |
| Needed | 40 | 93% | 19 | 68% | 34 | 54% |
| p < 0.001 * | p = 0.156 * | |||||
| Silness–Löe index scores | ||||||
| 0 | 1 | 2% | 5 | 18% | 24 | 38% |
| 1 | 14 | 33% | 12 | 43% | 23 | 37% |
| 2 | 15 | 35% | 8 | 29% | 15 | 24% |
| 3 | 13 | 30% | 3 | 11% | 1 | 2% |
| p < 0.001 * | p = 0.088 * | |||||
| Greene–Vermillion index scores | ||||||
| 0 | 3 | 7% | 5 | 18% | 26 | 41% |
| 1 | 10 | 23% | 11 | 39% | 22 | 35% |
| 2 | 16 | 37% | 11 | 39% | 15 | 24% |
| 3 | 14 | 33% | 1 | 4% | 0 | 0% |
| p < 0.001 * | p = 0.069 * | |||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Emulina, D.E.; Abola, I.; Brinkmane, A.; Isakovs, A.; Skadins, I.; Moisejevs, G.; Gailite, L.; Auzenbaha, M. The Impact of IL1B rs1143634 and DEFB1 rs11362 Variants on Periodontitis Risk in Phenylketonuria and Type 1 Diabetes Mellitus Patients in a Latvian Population. Diagnostics 2024, 14, 192. https://doi.org/10.3390/diagnostics14020192
Emulina DE, Abola I, Brinkmane A, Isakovs A, Skadins I, Moisejevs G, Gailite L, Auzenbaha M. The Impact of IL1B rs1143634 and DEFB1 rs11362 Variants on Periodontitis Risk in Phenylketonuria and Type 1 Diabetes Mellitus Patients in a Latvian Population. Diagnostics. 2024; 14(2):192. https://doi.org/10.3390/diagnostics14020192
Chicago/Turabian StyleEmulina, Darta Elizabete, Iveta Abola, Anda Brinkmane, Aleksejs Isakovs, Ingus Skadins, Georgijs Moisejevs, Linda Gailite, and Madara Auzenbaha. 2024. "The Impact of IL1B rs1143634 and DEFB1 rs11362 Variants on Periodontitis Risk in Phenylketonuria and Type 1 Diabetes Mellitus Patients in a Latvian Population" Diagnostics 14, no. 2: 192. https://doi.org/10.3390/diagnostics14020192
APA StyleEmulina, D. E., Abola, I., Brinkmane, A., Isakovs, A., Skadins, I., Moisejevs, G., Gailite, L., & Auzenbaha, M. (2024). The Impact of IL1B rs1143634 and DEFB1 rs11362 Variants on Periodontitis Risk in Phenylketonuria and Type 1 Diabetes Mellitus Patients in a Latvian Population. Diagnostics, 14(2), 192. https://doi.org/10.3390/diagnostics14020192