
Dedifferentiated Leiomyosarcoma of the Uterine Corpus with Heterologous Component: Clinicopathological Analysis of Five Consecutive Cases from a Single Institution and Comprehensive Literature Review


Abstract
1. Introduction
2. Materials and Methods
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Asano, H.; Isoe, T.; Ito, Y.M.; Nishimoto, N.; Watanabe, Y.; Yokoshiki, S.; Watari, H. Status of the current treatment options and potential future targets in uterine leiomyosarcoma: A Review. Cancers 2022, 14, 1180. [Google Scholar] [CrossRef]
- Devaud, N.; Vornicova, O.; Abdul Razak, A.R.; Khalili, K.; Demicco, E.G.; Mitric, C.; Bernardini, M.Q.; Gladdy, R.A. Leiomyosarcoma: Current clinical management and future horizons. Surg. Oncol. Clin. N. Am. 2022, 31, 527–546. [Google Scholar] [CrossRef]
- Yu, S.; Hornick, J.L. Malignant mesenchymoma revisited: A clinicopathologic study of leiomyosarcomas with osteosarcomatous differentiation. Am. J. Surg. Pathol. 2022, 46, 1430–1435. [Google Scholar] [CrossRef] [PubMed]
- Penel, N.; Coindre, J.M.; Giraud, A.; Terrier, P.; Ranchere-Vince, D.; Collin, F.; Guellec, S.L.E.; Bazille, C.; Lae, M.; de Pinieux, G.; et al. Presentation and outcome of frequent and rare sarcoma histologic subtypes: A study of 10,262 patients with localized visceral/soft tissue sarcoma managed in reference centers. Cancer 2018, 124, 1179–1187. [Google Scholar] [CrossRef] [PubMed]
- Gronchi, A.; Strauss, D.C.; Miceli, R.; Bonvalot, S.; Swallow, C.J.; Hohenberger, P.; Van Coevorden, F.; Rutkowski, P.; Callegaro, D.; Hayes, A.J.; et al. Variability in patterns of recurrence after resection of primary retroperitoneal sarcoma (RPS): A report on 1007 patients from the multi-institutional collaborative RPS Working Group. Ann. Surg. 2016, 263, 1002–1009. [Google Scholar] [CrossRef] [PubMed]
- Buzinskiene, D.; Mikenas, S.; Drasutiene, G.; Mongirdas, M. Uterine sarcoma: A clinical case and a literature review. Acta Med. Litu. 2018, 25, 206–218. [Google Scholar] [CrossRef] [PubMed]
- Abeler, V.M.; Royne, O.; Thoresen, S.; Danielsen, H.E.; Nesland, J.M.; Kristensen, G.B. Uterine sarcomas in Norway. A histopathological and prognostic survey of a total population from 1970 to 2000 including 419 patients. Histopathology 2009, 54, 355–364. [Google Scholar] [CrossRef]
- D’Angelo, E.; Prat, J. Uterine sarcomas: A review. Gynecol. Oncol. 2010, 116, 131–139. [Google Scholar] [CrossRef] [PubMed]
- Hosh, M.; Antar, S.; Nazzal, A.; Warda, M.; Gibreel, A.; Refky, B. Uterine sarcoma: Analysis of 13,089 cases based on Surveillance, Epidemiology, and End Results Database. Int. J. Gynecol. Cancer 2016, 26, 1098–1104. [Google Scholar] [CrossRef]
- Toro, J.R.; Travis, L.B.; Wu, H.J.; Zhu, K.; Fletcher, C.D.; Devesa, S.S. Incidence patterns of soft tissue sarcomas, regardless of primary site, in the Surveillance, Epidemiology and End Results Program, 1978–2001: An analysis of 26,758 cases. Int. J. Cancer 2006, 119, 2922–2930. [Google Scholar] [CrossRef]
- Sparic, R.; Andjic, M.; Babovic, I.; Nejkovic, L.; Mitrovic, M.; Stulic, J.; Pupovac, M.; Tinelli, A. Molecular insights in uterine leiomyosarcoma: A systematic review. Int. J. Mol. Sci. 2022, 23, 9728. [Google Scholar] [CrossRef]
- Roberts, M.E.; Aynardi, J.T.; Chu, C.S. Uterine leiomyosarcoma: A review of the literature and update on management options. Gynecol. Oncol. 2018, 151, 562–572. [Google Scholar] [CrossRef] [PubMed]
- Juhasz-Boss, I.; Gabriel, L.; Bohle, R.M.; Horn, L.C.; Solomayer, E.F.; Breitbach, G.P. Uterine leiomyosarcoma. Oncol. Res. Treat. 2018, 41, 680–686. [Google Scholar] [CrossRef] [PubMed]
- Zhang, F.; Liu, Y.; Quan, Q.; Meng, Y.; Mu, X. Diagnostic value of preoperative CA125, LDH and HE4 for leiomyosarcoma of the female reproductive system. Cancer Manag. Res. 2021, 13, 4657–4664. [Google Scholar] [CrossRef] [PubMed]
- Henricks, W.H.; Chu, Y.C.; Goldblum, J.R.; Weiss, S.W. Dedifferentiated liposarcoma: A clinicopathological analysis of 155 cases with a proposal for an expanded definition of dedifferentiation. Am. J. Surg. Pathol. 1997, 21, 271–281. [Google Scholar] [CrossRef]
- Chapel, D.B.; Maccio, L.; Bragantini, E.; Zannoni, G.F.; Quade, B.J.; Parra-Herran, C.; Nucci, M.R. Dedifferentiated leiomyosarcoma of the uterus: A clinicopathologic and immunohistochemical analysis of 23 cases. Histopathology 2023, 82, 812–825. [Google Scholar] [CrossRef] [PubMed]
- Shmookler, B.M.; Lauer, D.H. Retroperitoneal leiomyosarcoma. A clinicopathologic analysis of 36 cases. Am. J. Surg. Pathol. 1983, 7, 269–280. [Google Scholar] [PubMed]
- Dekanic, A.; Jonjic, N.; Savic Vukovic, A. Dedifferentiated leiomyosarcoma of the auricle with heterologous osteosarcoma component: Case report and literature review. Case Rep. Otolaryngol. 2022, 2022, 3684461. [Google Scholar] [CrossRef]
- Gaeta, R.; Matera, D.; Muratori, F.; Roselli, G.; Baldi, G.; Campanacci, D.A.; Franchi, A. Dedifferentiated soft tissue leiomyosarcoma with heterologous osteosarcoma component: Case report and review of the literature. Clin. Sarcoma Res. 2020, 10, 6. [Google Scholar] [CrossRef]
- Chen, E.; O’Connell, F.; Fletcher, C.D. Dedifferentiated leiomyosarcoma: Clinicopathological analysis of 18 cases. Histopathology 2011, 59, 1135–1143. [Google Scholar] [CrossRef]
- Nicolas, M.M.; Tamboli, P.; Gomez, J.A.; Czerniak, B.A. Pleomorphic and dedifferentiated leiomyosarcoma: Clinicopathologic and immunohistochemical study of 41 cases. Hum. Pathol. 2010, 41, 663–671. [Google Scholar] [CrossRef] [PubMed]
- Matsuda, K.; Akazawa, Y.; Yamaguchi, Y.; Mussazhanova, Z.; Kurohama, H.; Ueki, N.; Kohno, M.; Fukushima, A.; Kajimura, I.; Hiraki, H.; et al. Immunofluorescence analysis of DNA damage response protein p53-binding protein 1 in a case of uterine dedifferentiated leiomyosarcoma arising from leiomyoma. Pathol. Res. Pract. 2019, 215, 152640. [Google Scholar] [CrossRef] [PubMed]
- Zuo, X.; Wu, W.L.; Shi, P.; Liu, T.M.; Yu, N.; Li, L. A case report of recurrent leiomyosarcoma with chondrosarcoma differentiation in the abdominal wall and a review of the literature. Pathol. Oncol. Res. 2023, 29, 1611109. [Google Scholar] [CrossRef] [PubMed]
- Park, S.; Park, E.; Kim, H.S. Mesonephric-like carcinosarcoma of the uterine corpus: Clinicopathological, molecular and prognostic characteristics in comparison with uterine mesonephric-like adenocarcinoma and conventional endometrial carcinosarcoma. Cancer Genom. Proteom. 2022, 19, 747–760. [Google Scholar] [CrossRef] [PubMed]
- Chu, J.; Yeo, M.K.; Lee, S.H.; Lee, M.Y.; Chae, S.W.; Kim, H.S.; Do, S.I. Clinicopathological and prognostic significance of programmed death ligand-1 SP142 expression in 132 patients with triple-negative breast cancer. In Vivo 2022, 36, 2890–2898. [Google Scholar] [CrossRef]
- Sohn, J.; Lee, Y.; Kim, H.S. Endometrioid carcinomas of the ovaries and endometrium involving endocervical polyps: Comprehensive clinicopathological analyses. Diagnostics 2022, 12, 2339. [Google Scholar] [CrossRef] [PubMed]
- Chung, Y.; Kim, S.; Kim, H.S.; Do, S.I. High receptor-interacting serine/threonine-protein kinase 3 (RIP3) expression serves as an independent poor prognostic factor for triple-negative breast carcinoma. Anticancer. Res. 2022, 42, 2753–2761. [Google Scholar] [CrossRef]
- Koh, H.H.; Park, E.; Kim, H.S. Mesonephric-like adenocarcinoma of the ovary: Clinicopathological and molecular characteristics. Diagnostics 2022, 12, 326. [Google Scholar] [CrossRef]
- Yoo, H.; Kim, H.S. Clinicopathological and prognostic values of telomerase reverse transcriptase (TERT) promoter mutations in ovarian clear cell carcinoma for predicting tumor recurrence, platinum resistance and survival. Cancer Genom. Proteom. 2023, 20, 626–636. [Google Scholar] [CrossRef]
- Park, S.; Cho, Y.; Kim, H.S. Mesonephric-like adenocarcinoma of the uterine corpus: Clinicopathological and prognostic significance of L1 cell adhesion molecule (L1CAM) over-expression. Anticancer. Res. 2023, 43, 4559–4571. [Google Scholar] [CrossRef]
- Koh, H.H.; Park, E.; Kim, H.S. Mesonephric-like adenocarcinoma of the uterine corpus: Genomic and immunohistochemical profiling with comprehensive clinicopathological analysis of 17 consecutive cases from a single institution. Biomedicines 2023, 11, 2269. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.; Kim, H.S. Mesonephric-like adenocarcinoma of the uterine corpus: Comparison between mismatch repair protein immunostaining and microsatellite instability testing. Anticancer Res. 2023, 43, 1785–1795. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.; Oh, Y.L. Thyroid pathology, a clue to PTEN hamartoma tumor syndrome. J. Pathol. Transl. Med. 2023, 57, 178–183. [Google Scholar] [CrossRef] [PubMed]
- Park, S.; Kim, J.; Jang, W.; Kim, K.M.; Jang, K.T. Clinicopathologic significance of the delta-like ligand 4, vascular endothelial growth factor, and hypoxia-inducible factor-2alpha in gallbladder cancer. J. Pathol. Transl. Med. 2023, 57, 113–122. [Google Scholar] [CrossRef]
- Chang, S.; Choi, Y.L.; Shim, H.S.; Lee, G.K.; Ha, S.Y.; Korean Cardiopulmonary Pathology Study Group. Usefulness of BRAF VE1 immunohistochemistry in non-small cell lung cancers: A multi-institutional study by 15 pathologists in Korea. J. Pathol. Transl. Med. 2022, 56, 334–341. [Google Scholar] [CrossRef] [PubMed]
- Koh, H.H.; Oh, Y.L. Papillary and medullary thyroid carcinomas coexisting in the same lobe, first suspected based on fine-needle aspiration cytology: A case report. J. Pathol. Transl. Med. 2022, 56, 301–308. [Google Scholar] [CrossRef]
- Kim, H.; Na, K.; Bae, G.E.; Kim, H.S. Mesonephric-like adenocarcinoma of the uterine corpus: Comprehensive immunohistochemical analyses using markers for mesonephric, endometrioid and serous tumors. Diagnostics 2021, 11, 2042. [Google Scholar] [CrossRef]
- Kobel, M.; Ronnett, B.M.; Singh, N.; Soslow, R.A.; Gilks, C.B.; McCluggage, W.G. Interpretation of p53 immunohistochemistry in endometrial carcinomas: Toward increased reproducibility. Int. J. Gynecol. Pathol. 2019, 38, S123–S131. [Google Scholar] [CrossRef]
- Oda, Y.; Miyajima, K.; Kawaguchi, K.; Tamiya, S.; Oshiro, Y.; Hachitanda, Y.; Oya, M.; Iwamoto, Y.; Tsuneyoshi, M. Pleomorphic leiomyosarcoma: Clinicopathologic and immunohistochemical study with special emphasis on its distinction from ordinary leiomyosarcoma and malignant fibrous histiocytoma. Am. J. Surg. Pathol. 2001, 25, 1030–1038. [Google Scholar] [CrossRef]
- Demicco, E.G.; Boland, G.M.; Brewer Savannah, K.J.; Lusby, K.; Young, E.D.; Ingram, D.; Watson, K.L.; Bailey, M.; Guo, X.; Hornick, J.L.; et al. Progressive loss of myogenic differentiation in leiomyosarcoma has prognostic value. Histopathology 2015, 66, 627–638. [Google Scholar] [CrossRef]
- Nosaka, K.; Komatsu, H.; Oishi, T.; Horie, Y.; Harada, T.; Umekita, Y. A Case of dedifferentiated leiomyosarcoma of the uterus. Int. J. Pathol. Clin. Res. 2016, 2, 49. [Google Scholar] [CrossRef]
- WHO. WHO Classification of Tumours: Female Genital Tumours, 5th ed.; WHO Classification of Tumors Editorial Board, Ed.; WHO: Lyon, France, 2020. [Google Scholar]
- Sadiq, Q.; Khan, F. High grade sarcoma with chondrosarcomatous differentiation in primary uterine leiomyosarcoma; A rare case and review of literature. Gynecol. Oncol. Rep. 2022, 39, 100905. [Google Scholar] [CrossRef] [PubMed]
- Rawish, K.R.; Fadare, O. Dedifferentiated leiomyosarcoma of the uterus with heterologous elements: A potential diagnostic pitfall. Case Rep. Obstet. Gynecol. 2012, 2012, 534634. [Google Scholar] [CrossRef]
- Parikh, P.; Maheshwari, A.; Rekhi, B. Two uncommon cases of uterine leiomyosarcomas displaying heterologous osteosarcomatous de-differentiation. J. Cancer Res. Ther. 2015, 11, 654. [Google Scholar] [CrossRef] [PubMed]
- Iihara, K.; Hirano, K.; Fujioka, Y.; Sakamoto, A. Leiomyosarcoma with dedifferentiation in a premenopausal patient discovered after uterine artery embolization. Pathol. Int. 2007, 57, 681–687. [Google Scholar] [CrossRef]
- Kousar, A.; Wald, A.I.; Heayn, M.; Cardillo, N.D.; Elishaev, E.; Bhargava, R. Dedifferentiated leiomyosarcoma: Morphology, immunohistochemistry, and molecular findings of a case and review of literature. Int. J. Gynecol. Pathol. 2023. online ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Cope, B.M.; Traweek, R.S.; Lazcano, R.; Keung, E.Z.; Lazar, A.J.; Roland, C.L.; Nassif, E.F. Targeting the molecular and immunologic features of leiomyosarcoma. Cancers 2023, 15, 2099. [Google Scholar] [CrossRef]
- Astolfi, A.; Nannini, M.; Indio, V.; Schipani, A.; Rizzo, A.; Perrone, A.M.; De Iaco, P.; Pirini, M.G.; De Leo, A.; Urbini, M.; et al. Genomic database analysis of uterine leiomyosarcoma mutational profile. Cancers 2020, 12, 2126. [Google Scholar] [CrossRef]
- Ciccarone, F.; Bruno, M.; De Paolis, E.; Piermattei, A.; De Bonis, M.; Lorusso, D.; Zannoni, G.F.; Normanno, N.; Minucci, A.; Scambia, G.; et al. Role of homologous recombination repair (HRR) genes in uterine leiomyosarcomas: A retrospective analysis. Cancers 2022, 14, 1934. [Google Scholar] [CrossRef]
- Beck, A.H.; Lee, C.H.; Witten, D.M.; Gleason, B.C.; Edris, B.; Espinosa, I.; Zhu, S.; Li, R.; Montgomery, K.D.; Marinelli, R.J.; et al. Discovery of molecular subtypes in leiomyosarcoma through integrative molecular profiling. Oncogene 2010, 29, 845–854. [Google Scholar] [CrossRef]
- Hass, R.; von der Ohe, J.; Ungefroren, H. The intimate relationship among EMT, MET and TME: A T(ransdifferentiation) E(nhancing) M(ix) to be exploited for therapeutic purposes. Cancers 2020, 12, 3674. [Google Scholar] [CrossRef]
- Varga, J.; Greten, F.R. Cell plasticity in epithelial homeostasis and tumorigenesis. Nat. Cell Biol. 2017, 19, 1133–1141. [Google Scholar] [CrossRef]
- Meacham, C.E.; Morrison, S.J. Tumour heterogeneity and cancer cell plasticity. Nature 2013, 501, 328–337. [Google Scholar] [CrossRef] [PubMed]
- Hammerlindl, H.; Schaider, H. Tumor cell-intrinsic phenotypic plasticity facilitates adaptive cellular reprogramming driving acquired drug resistance. J. Cell Commun. Signal. 2018, 12, 133–141. [Google Scholar] [CrossRef] [PubMed]
- Hass, R. Retrodifferentiation: A mechanism for cellular regeneration? Biol. Chem. 2009, 390, 409–416. [Google Scholar] [CrossRef] [PubMed]
- Hass, R. Retrodifferentiation and cell death. Crit. Rev. Oncog. 1994, 5, 359–371. [Google Scholar] [CrossRef] [PubMed]
- Cabillic, F.; Corlu, A. Regulation of transdifferentiation and retrodifferentiation by inflammatory cytokines in hepatocellular carcinoma. Gastroenterology 2016, 151, 607–615. [Google Scholar] [CrossRef]
- Lu, W.; Kang, Y. Epithelial-mesenchymal plasticity in cancer progression and metastasis. Dev. Cell 2019, 49, 361–374. [Google Scholar] [CrossRef]
- Easwaran, H.; Tsai, H.C.; Baylin, S.B. Cancer epigenetics: Tumor heterogeneity, plasticity of stem-like states, and drug resistance. Mol. Cell 2014, 54, 716–727. [Google Scholar] [CrossRef]
- Yamada, Y.; Haga, H.; Yamada, Y. Concise review: Dedifferentiation meets cancer development: Proof of concept for epigenetic cancer. Stem Cells Transl. Med. 2014, 3, 1182–1187. [Google Scholar] [CrossRef]
- Dubois-Pot-Schneider, H.; Fekir, K.; Coulouarn, C.; Glaise, D.; Aninat, C.; Jarnouen, K.; Le Guevel, R.; Kubo, T.; Ishida, S.; Morel, F.; et al. Inflammatory cytokines promote the retrodifferentiation of tumor-derived hepatocyte-like cells to progenitor cells. Hepatology 2014, 60, 2077–2090. [Google Scholar] [CrossRef] [PubMed]
- Watts, F.; Stewart, P.; Gill, A.J.; Krishnaswamy, M. SDHA deficient dedifferentiated gastrointestinal stromal tumour with a smooth-muscle immunophenotype. Pathology 2023. online ahead of print. [Google Scholar] [CrossRef]
- Shah, V.I.; Morgan, S.E.; Kobel, M.; Lee, C.H.; McCluggage, W.G. Dedifferentiation in breast metastasis of endometrial carcinoma: A diagnostic dilemma. Int. J. Gynecol. Pathol. 2022, 41, 35–39. [Google Scholar] [CrossRef]
- Tan, N.J.H.; Sun, I.S.Y.; Low, S.W.; Kuick, C.H.; Chang, K.T.E.; Tan, C.L. A rapidly fatal intracranial anaplastic hemangiopericytoma with de-novo dedifferentiation: Emphasis on diagnostic recognition, molecular confirmation and discussion on treatment dilemma. Brain Tumor Pathol. 2019, 36, 20–26. [Google Scholar] [CrossRef] [PubMed]
- Pauwels, P.; Debiec-Rychter, M.; Stul, M.; De Wever, I.; Van Oosterom, A.T.; Sciot, R. Changing phenotype of gastrointestinal stromal tumours under imatinib mesylate treatment: A potential diagnostic pitfall. Histopathology 2005, 47, 41–47. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Antibody | Dilution | Clone | Company | Positive Control |
|---|---|---|---|---|
| Desmin | 1:200 | D33 | Agilent Technologies, Santa Clara, CA, USA | Normal myometrium |
| S100 protein | 1:5000 | polyclonal | Agilent Technologies, Santa Clara, CA, USA | Vulvar malignant melanoma |
| Myogenin | 1:50 | F5D | Cell marque, Rocklin, CA, USA | Uterine rhabdomyosarcoma |
| MyoD1 | 1:50 | EP212 | Cell marque, Rocklin, CA, USA | Uterine rhabdomyosarcoma |
| SATB2 | 1:2000 | EPNCIR130A | Abcam, Cambridge, UK | Colonic adenocarcinoma |
| p53 | 1:800 | DO-7 | Leica Biosystems, Deer Park, IL, USA | Ovarian HGSC |
| Retinoblastoma protein | 1:400 | 4H1 | Cell Signaling Technology, Beverly, MA, USA | Ocular retinoblastoma |
| Case No | 1 | 2 | 3 | 4 | 5 |
|---|---|---|---|---|---|
| Age (years) | 60 | 55 | 51 | 51 | 63 |
| Presenting symptoms | Abdominal discomfort, constipation | Uterine mass detected on routine examination | Uterine masses detected on routine examination | Uterine mass detected on routine examination | Abdominal discomfort and pain, palpable pelvic mass |
| Previous medical history | None | None | Thyroid cancer, umbilical hernia | Hyperthyroidism | None |
| Imaging findings of uterine tumor | NA | A large solid cystic mass | Multiple solid uterine masses measuring up to 8.9 cm | An 8.3 cm lobulated, heterogeneous mass with hypodense necrotic area | A 23.0 cm large heterogeneous mass with adnexal extension |
| Clinical impression | Uterine leiomyoma | Uterine leiomyoma | Uterine leiomyoma | Uterine leiomyoma | Uterine sarcoma |
| Surgical procedure for uterine tumor | TH | TH, BSO, PLND, PALND, OMT, APP | TH, bilateral salpingectomy | TH, BSO, OMT | Uterine mass excision, LO, LHC, left nephrectomy |
| Pathological diagnosis of uterine tumor | LMS | DDLMS | DDLMS-H | LMS | DDLMS-H |
| Greatest dimension of uterine tumor (cm) | NA | 27.8 | 8.9 | 8.3 | 23.0 |
| Adnexal extension | Absent | Absent | Absent | Absent | Present |
| Pelvic extension | Absent | Absent | Present | Absent | Present |
| Abdominal extension | Absent | Absent | Absent | Absent | Present |
| LN metastasis | Absent | Absent | Present (para-aortic) | Present (left pelvic) | Absent |
| Initial stage | IB | IB | IIIC | IIIC | IVC |
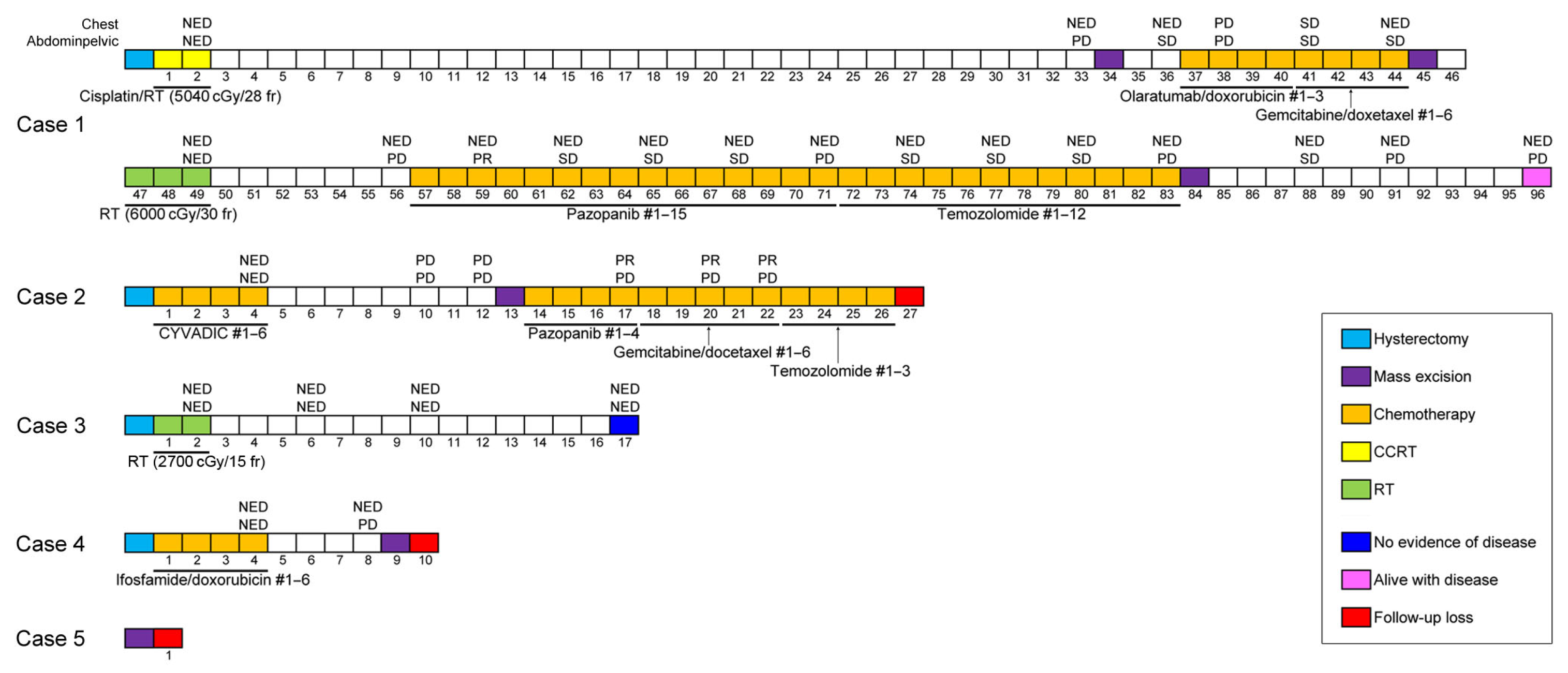
| Post-operative treatment | CCRT | Chemotherapy | RTx (interrupted) | Chemotherapy | NA (lost to follow-up) |
| Post-treatment recurrence | Present (ovary, colon, bladder, peritoneum, mesentery, omentum) | Present (vagina, bladder, peritoneum, lungs) | Absent | Present (left paracolic gutter) | NA (lost to follow-up) |
| Pathological diagnosis of recurrent tumor | Metastatic DDLMS-H | Metastatic DDLMS-H | None | Metastatic DDLMS-H | NA (lost to follow-up) |
| Treatment for recurrence | Excision, RTx, chemotherapy | Excision, chemotherapy | None | Excision | NA (lost to follow-up) |
| RFS (months) | 30 | 6 | 15 | 4 | NA (lost to follow-up) |
| Survival status | Alive with disease | NA (lost to follow-up) | No evidence of disease | NA (lost to follow-up) | NA (lost to follow-up) |
| OS (months) | 93 | NA (lost to follow-up) | 15 | NA (lost to follow-up) | NA (lost to follow-up) |
| Case No | 1 | 2 | 3 | 4 | 5 | |
|---|---|---|---|---|---|---|
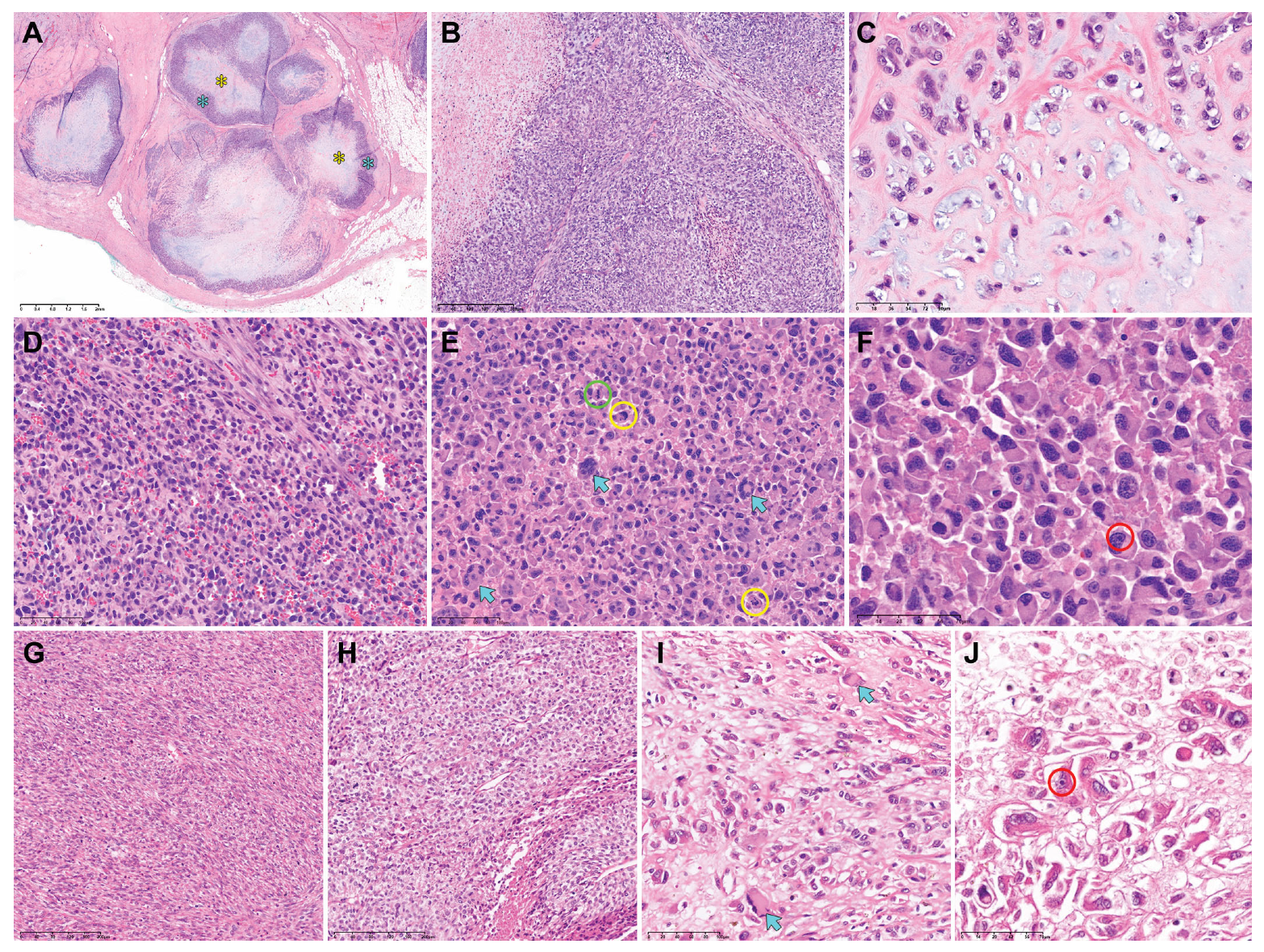
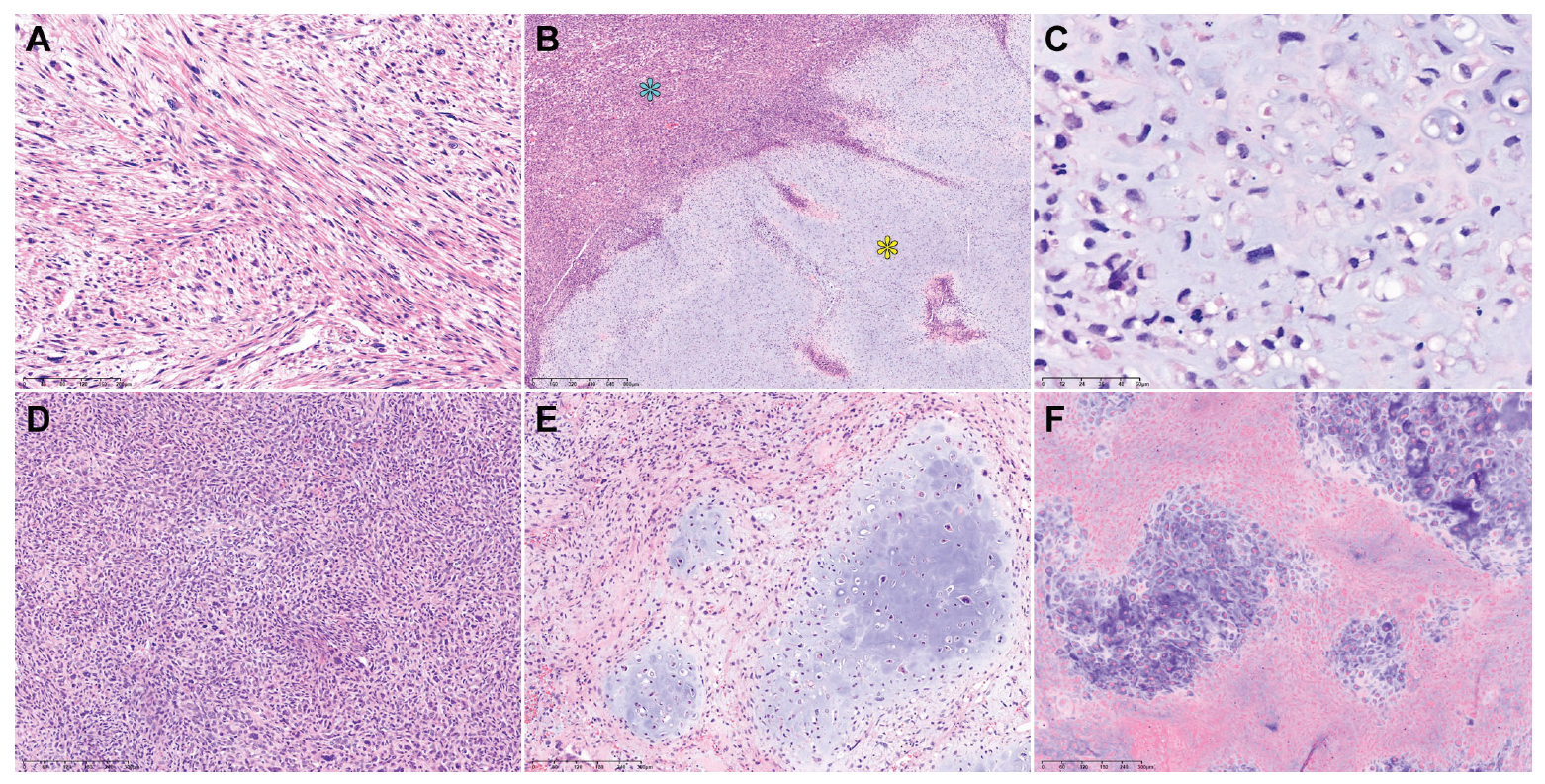
| Dominant morphology of differentiated component | Spindle cell and epithelioid LMS | Epithelioid LMS | Spindle cell and epithelioid LMS | Spindle cell LMS | Spindle cell and epithelioid LMS | |
| Nuclear pleomorphism | Severe | Severe | Severe | Severe | Severe | |
| Mitotic count per 10 HPFs | 23 | 40 | 46 | 22 | 21 | |
| Tumor cell necrosis | Present | Present | Present | Present | Present | |
| Tumor border | Infiltrative | Infiltrative | Infiltrative | Infiltrative | Infiltrative | |
| Lymphocytic infiltrate | Absent | Present | Present | Present | Absent | |
| Histological type and proportion of heterologous component | CSA (80%) | RMS (60%) | RMS (20%) | CSA (60%) | CSA (30%) | |
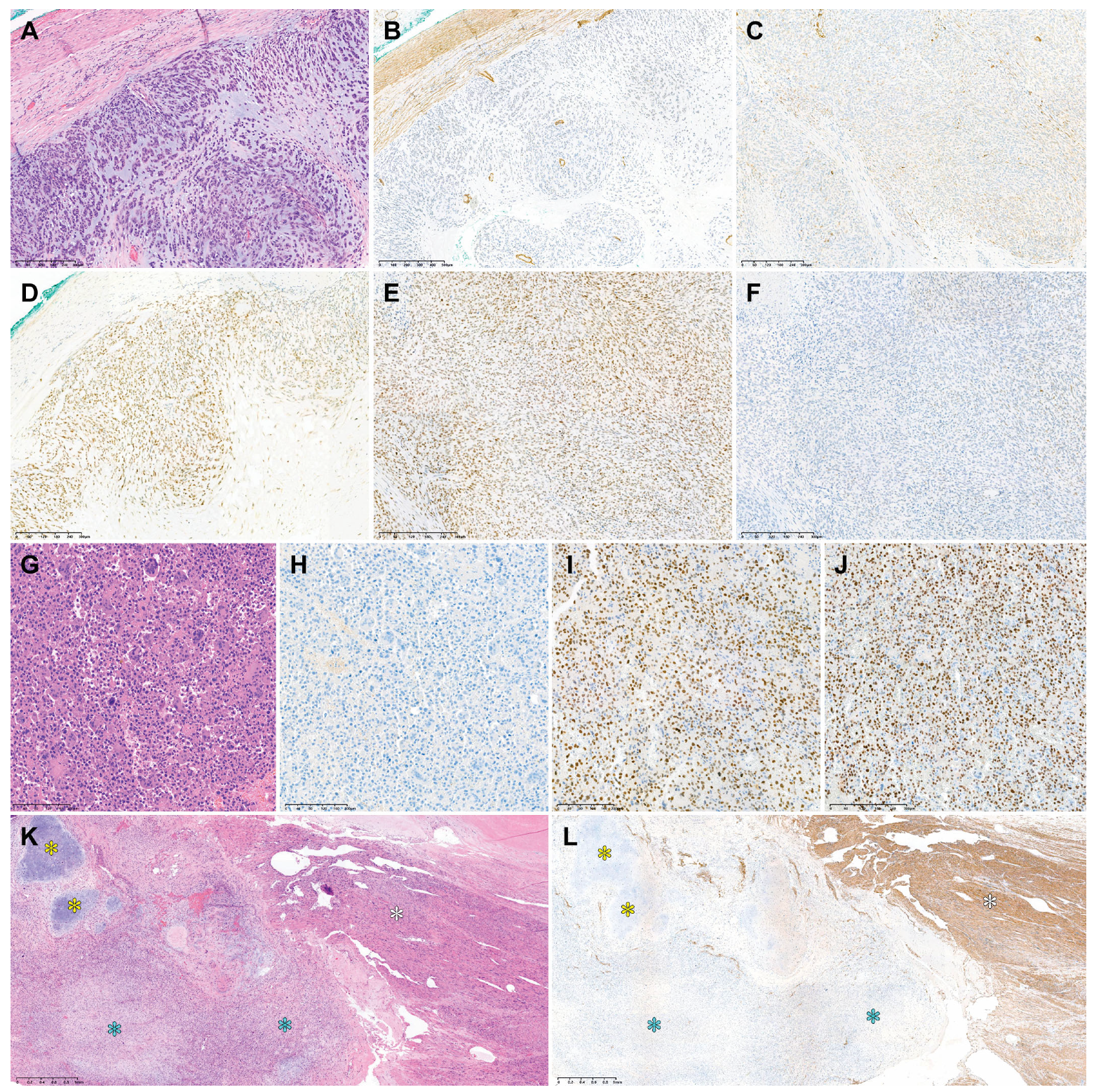
| Desmin | Differentiated | DMP | DSP | DSP | Negative | NA |
| Dedifferentiated | FWP | Negative | Negative | Negative | NA | |
| S100 protein | Differentiated | FWP | Negative | NA | Negative | NA |
| Dedifferentiated | DSP | Negative | NA | FSP | NA | |
| Myogenin | Differentiated | Negative | Negative | Negative | NA | NA |
| Dedifferentiated | Negative | Negative | FWP | NA | NA | |
| MyoD1 | Differentiated | Negative | Negative | Negative | NA | NA |
| Dedifferentiated | Negative | Negative | Negative | NA | NA | |
| SATB2 | Differentiated | FWP | Negative | NA | NA | NA |
| Dedifferentiated | Negative | DSP | NA | NA | NA | |
| p53 | Differentiated | WT | WT | WT | NA | NA |
| Dedifferentiated | WT | OE | WT | NA | NA | |
| RB protein | Differentiated | No loss | No loss | NA | NA | NA |
| Dedifferentiated | No loss | No loss | NA | NA | NA | |
| Authors (Year Published) | Case No | Age (Years) | Presenting Symptom | Initial Stage | Treatment | Recurrence | Distant Metastasis | DFS (Months) | Outcome | OS or DSS (Months) |
|---|---|---|---|---|---|---|---|---|---|---|
| Iihara et al., (2007) [46] | 1 | 48 | Hypermenorrhea for 4 years | IB | UAE, TH, CTx, GKRS | NA | Present (lungs, brain) | NA | DOD | 20 a |
| Chen et al., (2011) [20] | 2 | 59 | Pelvic pain | NA | TH, BSO | Absent | Absent | 28 | NED | 28 a |
| 3 | 80 | PMB | NA | Excision | NA | NA | NA | DOC | 12 a | |
| Rawish and Fadare (2012) [44] | 4 | 48 | NA | IA | SH, BSO, CTx | Present | Absent | 6 | AWD | 8 a |
| Parikh et al., (2015) [45] | 5 | 60 | Abdominal pain for 4 months | NA | TH, BS | NA | NA | NA | NA | NA |
| 6 | 38 | Infertility | NA | Myomectomy | NA | NA | NA | NA | NA | |
| Nosaka et al., (2016) [41] | 7 | 63 | Bloody vaginal discharge for 2 months | IVB | TH, BSO, CTx | NA | Present (lungs) | NA | NA | NA |
| Yu and Hornick (2022) [3] | 8 | 63 | NA | NA | Surgery, CTx | Present | Present (lungs, diaphragm, heart, SVC, kidney) | NA | DOD | 7.5 a |
| 9 | 40 | NA | NA | Surgery, CTx | Present | Present (colon, retroperitoneum) | NA | DOD | 18 a | |
| 10 | 48 | NA | NA | Surgery, CTx, RTx | Present | Present (lungs, liver, peritoneum, colon, small bowel) | NA | DOD | 6.5 a | |
| 11 | 55 | NA | NA | CTx | Absent | Present (pancreas, bone, lungs) | NA | DOD | NA | |
| 12 | 52 | NA | NA | Surgery, CTx | Present | Present (lungs, abdomen) | NA | AWD | 36 a | |
| 13 | 61 | NA | NA | Surgery, CTx, RTx | Present | Present (lungs, pleura) | NA | DOD | 17 a | |
| 14 | 53 | NA | NA | Surgery | Absent | NA | NA | DOD | 3.5 a | |
| 15 | 62 | NA | NA | NA | NA | NA | NA | NA | NA | |
| 16 | 43 | NA | NA | Surgery, CTx | Present | Present (small bowel) | NA | AWD | 32 a | |
| 17 | 52 | NA | NA | Surgery, CTx | Present | Present (liver, small bowel) | NA | AWD | 28 a | |
| Sadiq and Khan (2022) [43] | 18 | 68 | Vaginal bleeding | NA | TH, BSO | NA | NA | NA | NA | NA |
| Chapel et al., (2023) [16] | 19 | 88 | NA | IB | Surgery | NA | NA | 2 | DOD | 2 b |
| 20 | 66 | NA | IB | Surgery | NA | NA | 7 | DOD | 11 b | |
| 21 | 68 | NA | IB | Surgery, CTx | Present | NA | 3 | DOD | 20 b | |
| 22 | 42 | NA | IB | Surgery | NA | NA | NA | DOD | 23 b | |
| 23 | 61 | NA | IB | Surgery | NA | NA | NA | DOD | 5 b | |
| 24 | 57 | NA | IIIB | Surgery | NA | NA | NA | NA | NA | |
| 25 | 46 | NA | II | Surgery | NA | NA | 23 | DOD | 31 b | |
| 26 | 54 | NA | IB | Surgery | NA | NA | NA | DOD | 73 b | |
| 27 | 59 | NA | IB | CTx | NA | NA | 114 | NED | 114 b | |
| 28 | 50 | NA | IIIB | Surgery | NA | NA | 12 | AWD | 12 b | |
| 29 | 53 | NA | IA | Surgery | NA | NA | 21 | AWD | 50 b | |
| 30 | 63 | NA | IV | CTx | NA | Present | 8 | DOD | 16 b | |
| 31 | 53 | NA | IV | CTx | NA | Present | NA | DOD | 15 b | |
| 32 | 54 | NA | IV | Surgery | NA | Present | NA | DOD | 3 b | |
| 33 | 52 | NA | IV | CTx | NA | Present | NA | DOD | 10 b | |
| 34 | 57 | NA | IB | CTx for recurrence | Present | Present | 4 | NED | 109 b | |
| 35 | 90 | NA | II | Surgery | NA | NA | NA | NA | NA | |
| 36 | 54 | NA | II | CTx and RTx for recurrence | Present | NA | 2 | NED | 56 b | |
| 37 | 70 | NA | IB | RTx | NA | NA | 15 | AWD | 44 b | |
| 38 | 75 | NA | IB | Surgery | NA | NA | NA | NA | NA | |
| 39 | 55 | NA | IB | CTx for recurrence | Present | NA | 4 | AWD | 4 b | |
| 40 | 60 | NA | IB | CTx for recurrence | Present | NA | 8 | DOD | 13 b | |
| 41 | 63 | NA | II | Surgery | NA | NA | NA | NA | NA | |
| Kousar et al., (2023) [47] | 42 | 42 | Acute abdominal pain and vaginal bleeding | IV | Surgery, CTx | Present | Present (liver, peritoneum) | NA | NA | NA |
| Authors (Year Published) | Case No | Tumor Size (cm) | Dominant Morphology of Differentiated Component | Histological Type of Heterologous Component (Proportion) |
|---|---|---|---|---|
| Iihara et al., (2007) [46] | 1 | 14.0 | Spindle cell LMS | Mixed proliferation of scattered bizarre cells and spindle cells without specific structures (NA) |
| Chen et al., (2011) [20] | 2 | 6.8 | Spindle cell LMS | MFH-like morphology (NA) |
| 3 | 18.0 | Spindle cell LMS | MFH-like morphology (NA) | |
| Rawish and Fadare (2012) [44] | 4 | 18.0 | Spindle cell LMS | OSA (10%) |
| Parikh et al., (2015) [45] | 5 | 30.0 | Spindle cell LMS | Osteochondroid differentiation and MNGCs (NA) |
| 6 | 12.5 | Spindle cell LMS | OSA (NA) | |
| Nosaka et al., (2016) [41] | 7 | 14.0 | Spindle cell LMS | Undifferentiated pleomorphic sarcoma (NA) |
| Yu and Hornick (2022) [3] | 8 | 11.7 | Spindle cell LMS | OSA (NA) |
| 9 | NA | Spindle cell LMS | OSA (NA) | |
| 10 | 12.0 | Spindle cell LMS | OSA (NA) | |
| 11 | 9.0 | Spindle cell LMS | OSA (NA) | |
| 12 | 20.0 | Spindle cell LMS | OSA (NA) | |
| 13 | 18.0 | Spindle cell LMS | OSA (NA) | |
| 14 | 16.0 | Spindle cell LMS | OSA (NA) | |
| 15 | 18.0 | Spindle cell LMS | OSA (NA) | |
| 16 | 17.0 | Spindle cell LMS | OSA (NA) | |
| 17 | 18.8 | Spindle cell LMS | OSA (NA) | |
| Sadiq and Khan (2022) [43] | 18 | Up to 4.0 | Spindle cell LMS | CSA (NA) |
| Chapel et al., (2023) [16] | 19 | NA | Spindle cell LMS | MFH-like morphology (30%) |
| 20 | 6.5 | Spindle cell LMS | MFH-like morphology (20%) | |
| 21 | 8.5 | Spindle cell LMS and CLM | MFH-like morphology (40%) | |
| 22 | 10.0 | CLM | MFH-like morphology (50%) | |
| 23 | 7.0 | Epithelioid LMS | MFH-like morphology (5%) | |
| 24 | 12.0 | Spindle cell LMS | MFH-like morphology (15%) | |
| 25 | 12.1 | Spindle cell LMS | MFH-like morphology and OSA (20%) | |
| 26 | 8.2 | Spindle cell LMS | MFH-like morphology (10%) | |
| 27 | 6.8 | Spindle cell LMS | MFH-like morphology (40%) | |
| 28 | 3.0 | Spindle cell LMS | MFH-like morphology (50%) | |
| 29 | 4.5 | STUMP | MFH-like morphology (30%) | |
| 30 | 11.7 | Spindle cell LMS | MFH-like morphology and OSA (10%) | |
| 31 | 8.0 | Spindle cell LMS | MFH-like morphology (25%) | |
| 32 | 25.0 | Spindle cell LMS | MFH-like morphology (20%) | |
| 33 | 20.0 | Spindle cell LMS | MFH-like morphology, OSA, and CSA (70%) | |
| 34 | 9.0 | CLM | MFH-like morphology (50%) | |
| 35 | 20.0 | LBN | MFH-like morphology (50%) | |
| 36 | 14.5 | CLM | MFH-like morphology (20%) | |
| 37 | 11.0 | STUMP | MFH-like morphology (40%) | |
| 38 | 6.1 | Spindle cell LMS | MFH-like morphology (70%) | |
| 39 | 10.0 | Spindle cell LMS | MFH-like morphology (40%) | |
| 40 | 14.3 | LM, LBM, and spindle cell LMS | MFH-like morphology (10%) | |
| 41 | 7.7 | Spindle cell LMS | MFH-like morphology (70%) | |
| Kousar et al., (2023) [47] | 42 | 10.5, 6.7 (fundus); 1.7 (body) | LM-like areas, STUMP, and frank LMS | Areas showing extreme hypercellularity and large polygonal cells with significant cytological atypia and brisk mitotic activity |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, S.; Bae, H.; Kim, H.-S. Dedifferentiated Leiomyosarcoma of the Uterine Corpus with Heterologous Component: Clinicopathological Analysis of Five Consecutive Cases from a Single Institution and Comprehensive Literature Review. Diagnostics 2024, 14, 160. https://doi.org/10.3390/diagnostics14020160
Kim S, Bae H, Kim H-S. Dedifferentiated Leiomyosarcoma of the Uterine Corpus with Heterologous Component: Clinicopathological Analysis of Five Consecutive Cases from a Single Institution and Comprehensive Literature Review. Diagnostics. 2024; 14(2):160. https://doi.org/10.3390/diagnostics14020160
Chicago/Turabian StyleKim, Suyeon, Hyunsik Bae, and Hyun-Soo Kim. 2024. "Dedifferentiated Leiomyosarcoma of the Uterine Corpus with Heterologous Component: Clinicopathological Analysis of Five Consecutive Cases from a Single Institution and Comprehensive Literature Review" Diagnostics 14, no. 2: 160. https://doi.org/10.3390/diagnostics14020160
APA StyleKim, S., Bae, H., & Kim, H.-S. (2024). Dedifferentiated Leiomyosarcoma of the Uterine Corpus with Heterologous Component: Clinicopathological Analysis of Five Consecutive Cases from a Single Institution and Comprehensive Literature Review. Diagnostics, 14(2), 160. https://doi.org/10.3390/diagnostics14020160