
Prediction of Seropositivity in Suspected Autoimmune Encephalitis by Use of Radiomics: A Radiological Proof-of-Concept Study
 , , and
, , and
Abstract
1. Introduction
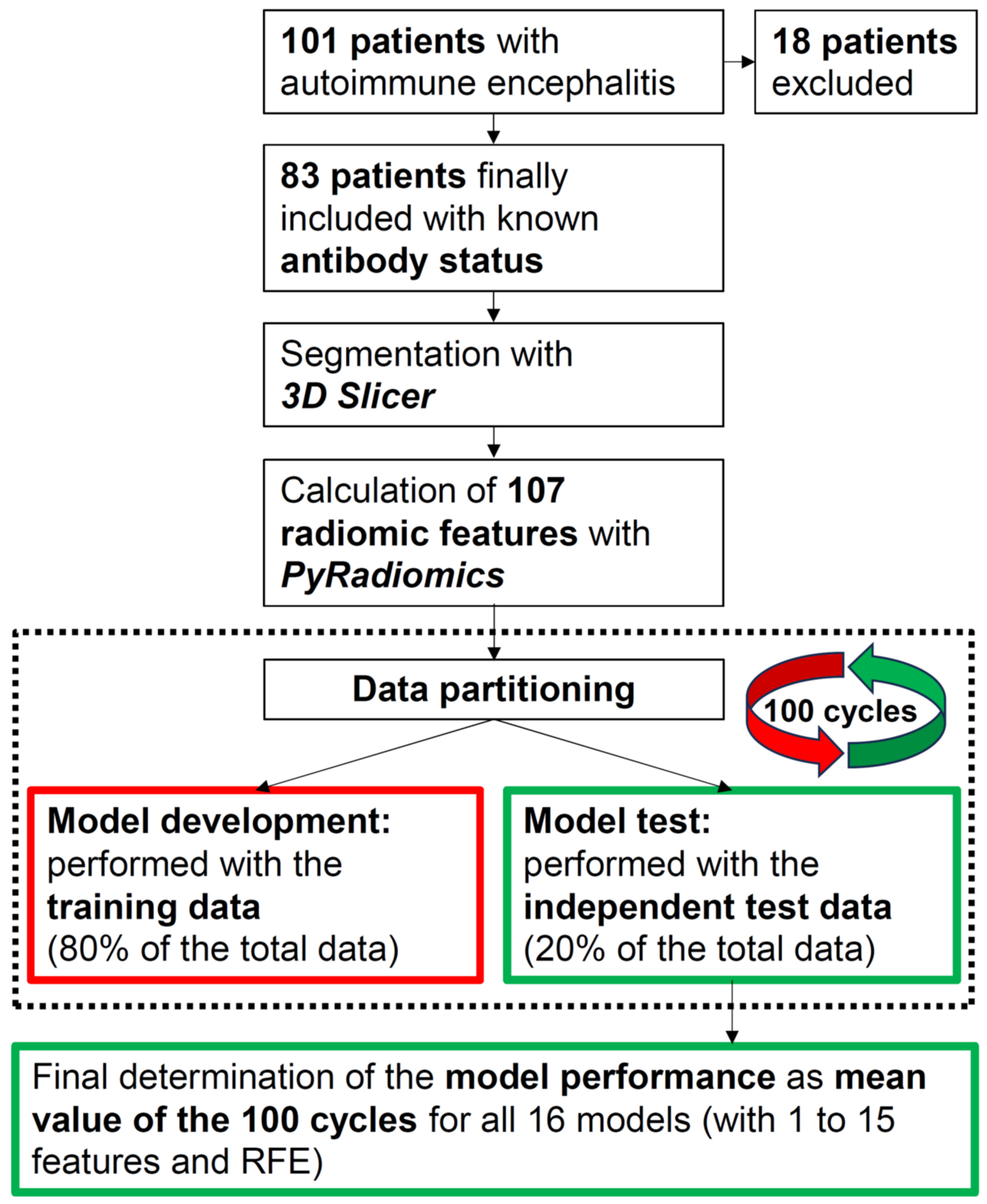
2. Materials and Methods
2.1. Radiomics
2.2. Statistical Analysis
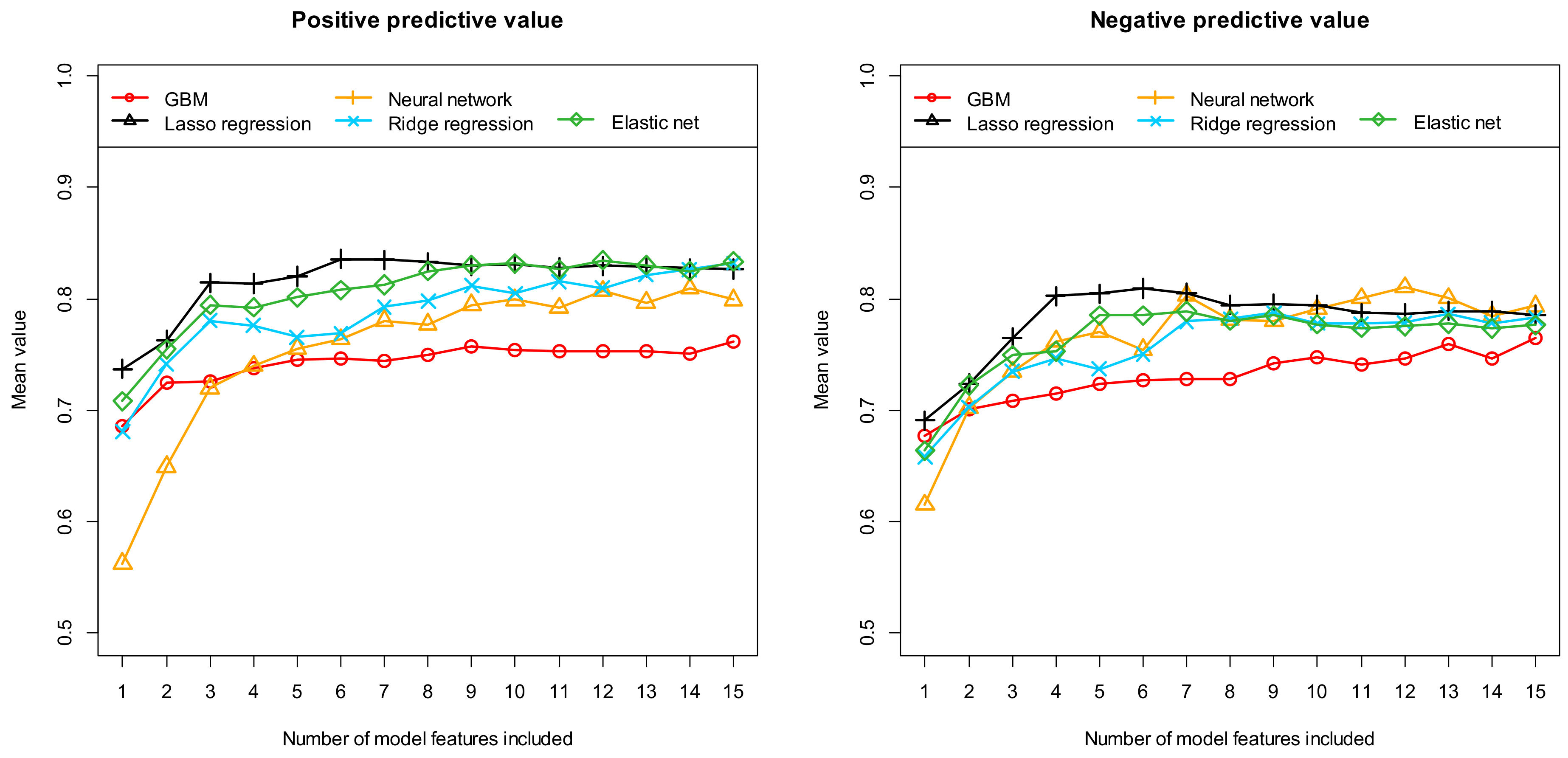
3. Results for Predicting Seropositivity in Suspected AE Using Machine Learning
4. Discussion
4.1. Limitations
4.2. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Dubey, D.; Pittock, S.J.; Kelly, C.R.; McKeon, A.; Lopez-Chiriboga, A.S.; Lennon, V.A.; Gadoth, A.; Smith, C.Y.; Bryant, S.C.; Klein, C.J.; et al. Autoimmune Encephalitis Epidemiology and a Comparison to Infectious Encephalitis: Autoimmune Encephalitis. Ann. Neurol. 2018, 83, 166–177. [Google Scholar] [CrossRef] [PubMed]
- Graus, F.; Titulaer, M.J.; Balu, R.; Benseler, S.; Bien, C.G.; Cellucci, T.; Cortese, I.; Dale, R.C.; Gelfand, J.M.; Geschwind, M.; et al. A Clinical Approach to Diagnosis of Autoimmune Encephalitis. Lancet Neurol. 2016, 15, 391–404. [Google Scholar] [CrossRef] [PubMed]
- Abboud, H.; Probasco, J.C.; Irani, S.; Ances, B.; Benavides, D.R.; Bradshaw, M.; Christo, P.P.; Dale, R.C.; Fernandez-Fournier, M.; Flanagan, E.P.; et al. Autoimmune Encephalitis: Proposed Best Practice Recommendations for Diagnosis and Acute Management. J. Neurol. Neurosurg. Psychiatry 2021, 92, 757–768. [Google Scholar] [CrossRef] [PubMed]
- Titulaer, M.J.; McCracken, L.; Gabilondo, I.; Armangué, T.; Glaser, C.; Iizuka, T.; Honig, L.S.; Benseler, S.M.; Kawachi, I.; Martinez-Hernandez, E.; et al. Treatment and Prognostic Factors for Long-Term Outcome in Patients with Anti-NMDA Receptor Encephalitis: An Observational Cohort Study. Lancet Neurol. 2013, 12, 157–165. [Google Scholar] [CrossRef] [PubMed]
- Dubey, D.; Singh, J.; Britton, J.W.; Pittock, S.J.; Flanagan, E.P.; Lennon, V.A.; Tillema, J.-M.; Wirrell, E.; Shin, C.; So, E.; et al. Predictive Models in the Diagnosis and Treatment of Autoimmune Epilepsy. Epilepsia 2017, 58, 1181–1189. [Google Scholar] [CrossRef] [PubMed]
- Dalmau, J.; Rosenfeld, M.R. Autoimmune Encephalitis Update. Neuro-Oncology 2014, 16, 771–778. [Google Scholar] [CrossRef] [PubMed]
- Titulaer, M.J.; Soffietti, R.; Dalmau, J.; Gilhus, N.E.; Giometto, B.; Graus, F.; Grisold, W.; Honnorat, J.; Sillevis Smitt, P.A.E.; Tanasescu, R.; et al. Screening for Tumours in Paraneoplastic Syndromes: Report of an EFNS Task Force: Screening for Tumours in PNS. Eur. J. Neurol. 2011, 18, 19-e3. [Google Scholar] [CrossRef] [PubMed]
- Dik, A.; Widman, G.; Schulte-Mecklenbeck, A.; Witt, J.-A.; Pitsch, J.; Golombeck, K.S.; Wagner, J.; Gallus, M.; Strippel, C.; Hansen, N.; et al. Impact of T Cells on Neurodegeneration in Anti-GAD65 Limbic Encephalitis. Ann. Clin. Transl. Neurol. 2021, 8, 2289–2301. [Google Scholar] [CrossRef]
- Roberts, W.K.; Darnell, R.B. Neuroimmunology of the Paraneoplastic Neurological Degenerations. Curr. Opin. Immunol. 2004, 16, 616–622. [Google Scholar] [CrossRef]
- Tanaka, K.; Ding, X.; Tanaka, M. Effects of Antineuronal Antibodies from Patients with Paraneoplastic Neurological Syndrome on Primary-Cultured Neurons. J. Neurol. Sci. 2004, 217, 25–30. [Google Scholar] [CrossRef]
- Hughes, E.G.; Peng, X.; Gleichman, A.J.; Lai, M.; Zhou, L.; Tsou, R.; Parsons, T.D.; Lynch, D.R.; Dalmau, J.; Balice-Gordon, R.J. Cellular and Synaptic Mechanisms of Anti-NMDA Receptor Encephalitis. J. Neurosci. 2010, 30, 5866–5875. [Google Scholar] [CrossRef] [PubMed]
- Dalmau, J.; Gleichman, A.J.; Hughes, E.G.; Rossi, J.E.; Peng, X.; Lai, M.; Dessain, S.K.; Rosenfeld, M.R.; Balice-Gordon, R.; Lynch, D.R. Anti-NMDA-Receptor Encephalitis: Case Series and Analysis of the Effects of Antibodies. Lancet Neurol. 2008, 7, 1091–1098. [Google Scholar] [CrossRef] [PubMed]
- Wang, B.; Wang, C.; Feng, J.; Hao, M.; Guo, S. Clinical Features, Treatment, and Prognostic Factors in Neuronal Surface Antibody-Mediated Severe Autoimmune Encephalitis. Front. Immunol. 2022, 13, 890656. [Google Scholar] [CrossRef] [PubMed]
- Saraya, A.W.; Worachotsueptrakun, K.; Vutipongsatorn, K.; Sonpee, C.; Hemachudha, T. Differences and Diversity of Autoimmune Encephalitis in 77 Cases from a Single Tertiary Care Center. BMC Neurol. 2019, 19, 273. [Google Scholar] [CrossRef] [PubMed]
- Guerin, J.; Watson, R.E.; Carr, C.M.; Liebo, G.B.; Kotsenas, A.L. Autoimmune Epilepsy: Findings on MRI and FDG-PET. Br. J. Radiol. 2019, 92, 20170869. [Google Scholar] [CrossRef] [PubMed]
- Graus, F.; Saiz, A.; Lai, M.; Bruna, J.; López, F.; Sabater, L.; Blanco, Y.; Rey, M.J.; Ribalta, T.; Dalmau, J. Neuronal Surface Antigen Antibodies in Limbic Encephalitis: Clinical-Immunologic Associations. Neurology 2008, 71, 930–936. [Google Scholar] [CrossRef] [PubMed]
- Khan, N.L.; Jeffree, M.A.; Good, C.; Macleod, W.; Al-Sarraj, S. Histopathology of VGKC Antibody-Associated Limbic Encephalitis. Neurology 2009, 72, 1703–1705. [Google Scholar] [CrossRef] [PubMed]
- Van Griethuysen, J.J.M.; Fedorov, A.; Parmar, C.; Hosny, A.; Aucoin, N.; Narayan, V.; Beets-Tan, R.G.H.; Fillion-Robin, J.-C.; Pieper, S.; Aerts, H.J.W.L. Computational Radiomics System to Decode the Radiographic Phenotype. Cancer Res. 2017, 77, e104–e107. [Google Scholar] [CrossRef] [PubMed]
- Wagner, M.W.; Namdar, K.; Biswas, A.; Monah, S.; Khalvati, F.; Ertl-Wagner, B.B. Radiomics, Machine Learning, and Artificial Intelligence-What the Neuroradiologist Needs to Know. Neuroradiology 2021, 63, 1957–1967. [Google Scholar] [CrossRef]
- Huang, J.; Xin, B.; Wang, X.; Qi, Z.; Dong, H.; Li, K.; Zhou, Y.; Lu, J. Multi-Parametric MRI Phenotype with Trustworthy Machine Learning for Differentiating CNS Demyelinating Diseases. J. Transl. Med. 2021, 19, 377. [Google Scholar] [CrossRef]
- Salmanpour, M.R.; Shamsaei, M.; Saberi, A.; Hajianfar, G.; Soltanian-Zadeh, H.; Rahmim, A. Robust Identification of Parkinson’s Disease Subtypes Using Radiomics and Hybrid Machine Learning. Comput. Biol. Med. 2021, 129, 104142. [Google Scholar] [CrossRef] [PubMed]
- Han, Y.; Yang, Y.; Shi, Z.-S.; Zhang, A.-D.; Yan, L.-F.; Hu, Y.-C.; Feng, L.-L.; Ma, J.; Wang, W.; Cui, G.-B. Distinguishing Brain Inflammation from Grade II Glioma in Population without Contrast Enhancement: A Radiomics Analysis Based on Conventional MRI. Eur. J. Radiol. 2021, 134, 109467. [Google Scholar] [CrossRef] [PubMed]
- Xiang, Y.; Dong, X.; Zeng, C.; Liu, J.; Liu, H.; Hu, X.; Feng, J.; Du, S.; Wang, J.; Han, Y.; et al. Clinical Variables, Deep Learning and Radiomics Features Help Predict the Prognosis of Adult Anti-N-Methyl-D-Aspartate Receptor Encephalitis Early: A Two-Center Study in Southwest China. Front. Immunol. 2022, 13, 913703. [Google Scholar] [CrossRef] [PubMed]
- Xiang, Y.; Zeng, C.; Liu, B.; Tan, W.; Wu, J.; Hu, X.; Han, Y.; Luo, Q.; Gong, J.; Liu, J.; et al. Deep Learning-Enabled Identification of Autoimmune Encephalitis on 3D Multi-Sequence MRI. J. Magn. Reson. Imaging 2022, 55, 1082–1092. [Google Scholar] [CrossRef] [PubMed]
- Piao, S.; Luo, X.; Bao, Y.; Hu, B.; Liu, X.; Zhu, Y.; Yang, L.; Geng, D.; Li, Y. An MRI-Based Joint Model of Radiomics and Spatial Distribution Differentiates Autoimmune Encephalitis from Low-Grade Diffuse Astrocytoma. Front. Neurol. 2022, 13, 998279. [Google Scholar] [CrossRef] [PubMed]
- Ernst, L.; David, B.; Gaubatz, J.; Domínguez-Narciso, I.; Lüchters, G.; Becker, A.J.; Weber, B.; Hattingen, E.; Elger, C.E.; Rüber, T. Volumetry of Mesiotemporal Structures Reflects Serostatus in Patients with Limbic Encephalitis. AJNR Am. J. Neuroradiol. 2019, 40, 2081–2089. [Google Scholar] [CrossRef] [PubMed]
- Pan, J.; Lv, R.; Wang, Q.; Zhao, X.; Liu, J.; Ai, L. Discrimination between Leucine-Rich Glioma-Inactivated 1 Antibody Encephalitis and Gamma-Aminobutyric Acid B Receptor Antibody Encephalitis Based on ResNet18. Vis. Comput. Ind. Biomed. Art. 2023, 6, 17. [Google Scholar] [CrossRef]
- World Medical Association. World Medical Association Declaration of Helsinki: Ethical Principles for Medical Research Involving Human Subjects. JAMA 2013, 310, 2191–2194. [Google Scholar] [CrossRef] [PubMed]
- Moore, M.; Hu, Y.; Woo, S.; O’Hearn, D.; Iordan, A.D.; Dolcos, S.; Dolcos, F. A Comprehensive Protocol for Manual Segmentation of the Medial Temporal Lobe Structures. J. Vis. Exp. 2014, 89, e50991. [Google Scholar] [CrossRef]
- LeDell, E.; Poirier, S. H2O AUTOML: Scalable Automatic Machine Learning. In Proceedings of the AutoML Workshop at ICML, San Diego, CA, USA, 18 July 2020. [Google Scholar]
- Darst, B.F.; Malecki, K.C.; Engelman, C.D. Using Recursive Feature Elimination in Random Forest to Account for Correlated Variables in High Dimensional Data. BMC Genet. 2018, 19, 65. [Google Scholar] [CrossRef]
- Musigmann, M.; Akkurt, B.H.; Krähling, H.; Nacul, N.G.; Remonda, L.; Sartoretti, T.; Henssen, D.; Brokinkel, B.; Stummer, W.; Heindel, W.; et al. Testing the Applicability and Performance of Auto ML for Potential Applications in Diagnostic Neuroradiology. Sci. Rep. 2022, 12, 13648. [Google Scholar] [CrossRef] [PubMed]
- Yu, X.; Sun, X.; Wei, M.; Deng, S.; Zhang, Q.; Guo, T.; Shao, K.; Zhang, M.; Jiang, J.; Han, Y.; et al. Innovative Multivariable Model Combining MRI Radiomics and Plasma Indexes Predicts Alzheimer’s Disease Conversion: Evidence from a 2-Cohort Longitudinal Study. Research 2024, 7, 0354. [Google Scholar] [CrossRef] [PubMed]
- Yang, W.-S.; Liu, J.-Y.; Shen, Y.-Q.; Xie, X.-F.; Zhang, S.-Q.; Liu, F.-Y.; Yu, J.-L.; Ma, Y.-B.; Xiao, Z.-S.; Duan, H.-W.; et al. Quantitative Imaging for Predicting Hematoma Expansion in Intracerebral Hemorrhage: A Multimodel Comparison. J. Stroke Cerebrovasc. Dis. 2024, 107731. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Training Data | Independent Test Data | Total Data | |
|---|---|---|---|
| Number of patients (n) | 66 | 17 | 83 |
| Gender (in %): Female/Male | 50.55/49.45 | 50.82/49.18 | 50.60/49.40 |
| Mean age (in years) | 50.79 | 51.68 | 51.38 |
| Antibody detected (in %): Yes/No | 51.52/48.48 | 52.94/47.06 | 51.81/48.19 |
| Antibody detected (number): Yes/No | 34/32 | 9/8 | 43/40 |
| Performance Metric | Model Algorithm | ||||
|---|---|---|---|---|---|
| GBM | Neural Network | Lasso Regression | Ridge Regression | Elastic Net | |
| AUC | 0.808 [0.521:0.993] | 0.845 [0.556:1.000] | 0.863 [0.625:1.000] | 0.852 [0.539:1.000] | 0.850 [0.585:1.000] |
| Accuracy | 0.740 [0.529:0.941] | 0.784 [0.588:1.000] | 0.793 [0.501:0.941] | 0.785 [0.529:1.000] | 0.782 [0.560:0.941] |
| Sensitivity | 0.771 [0.392:1.000] | 0.804 [0.503:1.000] | 0.802 [0.392:1.000] | 0.773 [0.444:1.000] | 0.772 [0.444:1.000] |
| Specificity | 0.705 [0.375:1.000] | 0.761 [0.441:1.000] | 0.783 [0.500:1.000] | 0.799 [0.500:1.000] | 0.793 [0.500:1.000] |
| PPV | 0.756 [0.559:1.000] | 0.804 [0.613:1.000] | 0.811 [0.529:1.000] | 0.819 [0.586:1.000] | 0.813 [0.586:1.000] |
| NPV | 0.750 [0.500:1.000] | 0.792 [0.545:1.000] | 0.797 [0.482:1.000] | 0.774 [0.500:1.000] | 0.773 [0.524:1.000] |
| Level of Importance | Feature Name | Number of Runs Included |
|---|---|---|
| 1 | firstorder_Minimum | 96 |
| 2 | shape_Flatness | 96 |
| 3 | gldm_DependenceNonUniformity | 82 |
| 4 | firstorder_Kurtosis | 73 |
| 5 | glszm_GrayLevelNonUniformity | 68 |
| 6 | glcm_Idn | 59 |
| 7 | glrlm_RunLengthNonUniformity | 15 |
| 8 | glszm_SizeZoneNonUniformityNormalized | 12 |
| 9 | glcm_InverseVariance | 11 |
| 10 | gldm_DependenceNonUniformityNormalized | 11 |
| Performance Metric | Different Features | Fixed Features |
|---|---|---|
| AUC | 0.878 [0.653:1.000] | 0.902 [0.757:1.000] |
| Accuracy | 0.811 [0.588:1.000] | 0.831 [0.619:1.000] |
| Sensitivity | 0.812 [0.444:1.000] | 0.840 [0.444:1.000] |
| Specificity | 0.809 [0.566:1.000] | 0.820 [0.625:1.000] |
| PPV | 0.836 [0.613:1.000] | 0.849 [0.684:1.000] |
| NPV | 0.809 [0.564:1.000] | 0.834 [0.586:1.000] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Stake, J.; Spiekers, C.; Akkurt, B.H.; Heindel, W.; Brix, T.; Mannil, M.; Musigmann, M. Prediction of Seropositivity in Suspected Autoimmune Encephalitis by Use of Radiomics: A Radiological Proof-of-Concept Study. Diagnostics 2024, 14, 1070. https://doi.org/10.3390/diagnostics14111070
Stake J, Spiekers C, Akkurt BH, Heindel W, Brix T, Mannil M, Musigmann M. Prediction of Seropositivity in Suspected Autoimmune Encephalitis by Use of Radiomics: A Radiological Proof-of-Concept Study. Diagnostics. 2024; 14(11):1070. https://doi.org/10.3390/diagnostics14111070
Chicago/Turabian StyleStake, Jacob, Christine Spiekers, Burak Han Akkurt, Walter Heindel, Tobias Brix, Manoj Mannil, and Manfred Musigmann. 2024. "Prediction of Seropositivity in Suspected Autoimmune Encephalitis by Use of Radiomics: A Radiological Proof-of-Concept Study" Diagnostics 14, no. 11: 1070. https://doi.org/10.3390/diagnostics14111070
APA StyleStake, J., Spiekers, C., Akkurt, B. H., Heindel, W., Brix, T., Mannil, M., & Musigmann, M. (2024). Prediction of Seropositivity in Suspected Autoimmune Encephalitis by Use of Radiomics: A Radiological Proof-of-Concept Study. Diagnostics, 14(11), 1070. https://doi.org/10.3390/diagnostics14111070