
“It Soothes Your Heart”: A Multimethod Study Exploring Acceptability of Point-of-Care Viral Load Testing among Ugandan Pregnant and Postpartum Women Living with HIV

 ,
,
Abstract
:1. Background
2. Methods
2.1. Study Design and Population
2.2. Data Collection
2.3. Data Analysis
2.4. Ethical Approvals
3. Results
3.1. Study Participant Characteristics
3.2. Pregnancy and Treatment Outcomes
3.3. Qualitative Sample Characteristics
3.4. Exploring Acceptability of POC VL Testing among Ugandan PWLHIV
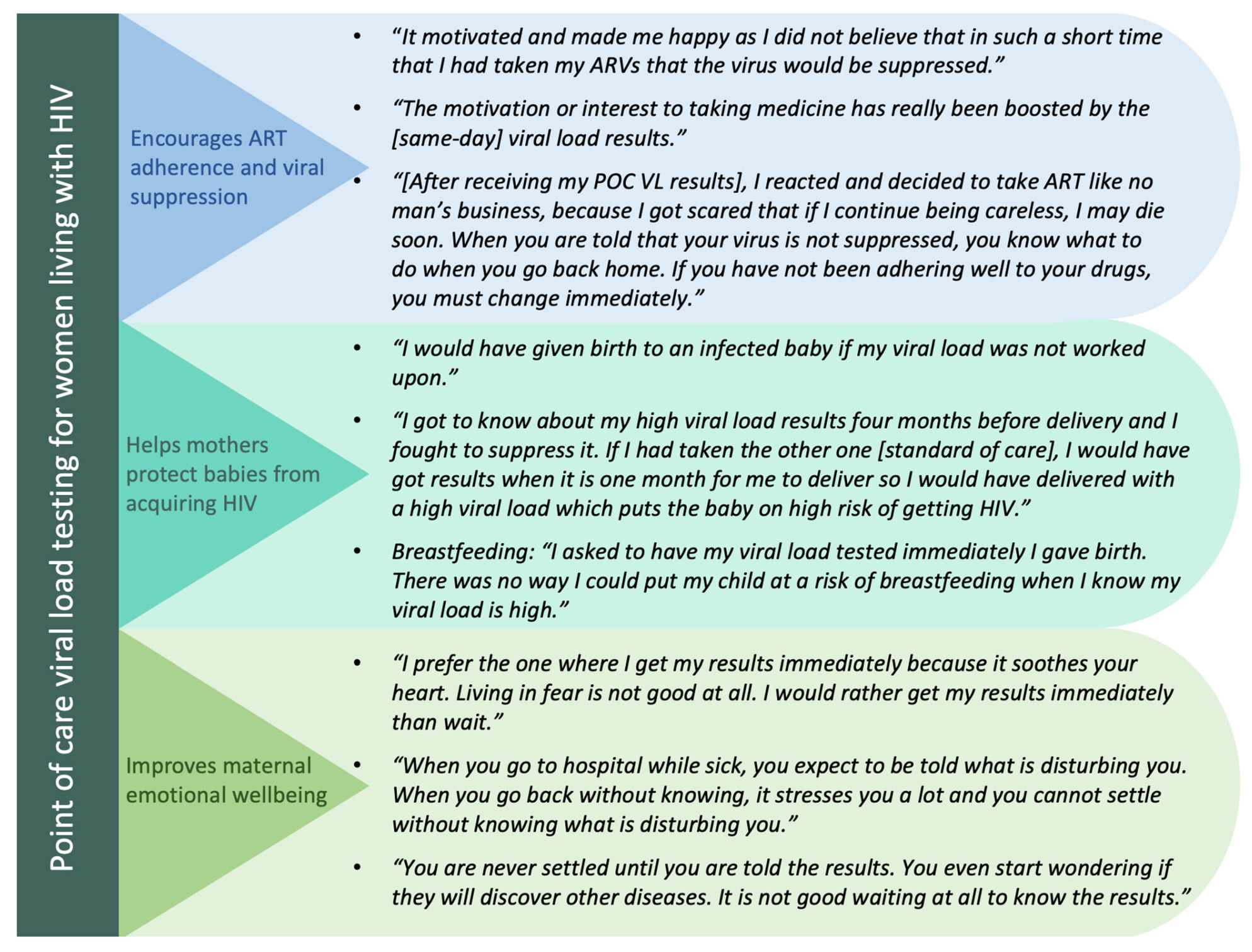
3.4.1. Category 1: POC VL Testing Encourages Maternal ART Adherence and Viral Suppression
“[After receiving my POC VL results], I reacted and decided to take ART like no man’s business, because I got scared that if I continue being careless, I may die soon. When you are told that your virus is not suppressed, you know what to do when you go back home. If you have not been adhering well to your drugs, you have to change immediately. This is not the case when you leave hospital without knowing your results. You cannot know if you are not adhering well to your drugs until when you go back to your next visit.” PWLHIV, 25 years old.
“[After receiving my POC VL results], I felt good and happy because it felt like as if I had cured [myself] of HIV (she laughs). I was strong because I knew that I was adhering well to my drugs and there was no way the results would show otherwise. I did not have any fears at all.” PWLHIV, 30 years old.
“[Without POC testing] I think we could have died. Can you imagine living without knowing what is happening in your body? The viral load test is very important because it helps you to know whether you are adhering well to your drugs or not and also it helps the health workers to know if the drugs they are giving you are working well. For example, when I did my third viral load test, I was told that my virus was not suppressed and the health worker decided to change the regimen for me. If the test was not done, the health worker would not have known that the drugs are no longer working well for me.” PWLHIV, 27 years old.
3.4.2. Category 2: POC VL Testing Helps Mothers Protect Their Babies from Acquiring HIV
“I got to know about my high viral load results four months before delivery and I fought to suppress it. If I had taken the other one [SOC testing], I would have got results when it is one month for me to deliver so I would have delivered with a high viral load which puts the baby on high risk of getting HIV. I wouldn’t have known and I wouldn’t have reacted the way I reacted. The other thing is the joy of having an HIV negative child. I was scared to miss that joy because I brought my first baby on earth when is negative and I was happy so I thought about that joy and I said I should take ART to avoid transmitting HIV to my unborn baby.” PWLHIV, 25 years old.
“I am sure the effort I put in taking ART helped me so much to give birth to a negative baby because you never know, I would have given birth to an infected baby if my viral load was not worked upon.” PWLHIV, 23 years old.
“Once you have the results then you can decide whether to breastfeed the child or not. It was the reason why I asked to have my viral load tested immediately I gave birth. There was no way I could put my child at a risk of breastfeeding when I know my viral load is high. The chance of the baby getting HIV would be high but now I started breastfeeding when I am comfortable that my baby will not get HIV from me since my viral load was suppressed. At that time, I was thinking about protecting my baby and that is why I asked for viral load test so that I decide well.” PWLHIV, 25 years old.
3.4.3. Category 3: POC VL Testing Improves Mothers’ Emotional Wellbeing
“(Respondent chuckles). [I prefer receiving my results] that same day. When you go to hospital while sick, you expect to be told what is disturbing you. When you go back without knowing, it stresses you a lot and you cannot settle without knowing what is disturbing you. It is important for one to know because it helps you to know what to do next. When you are not told whether your viral load is suppressed or not, you keep wondering what the results will be whereas if you know the results, you go back home knowing whether to continue adhering well or improve adherence if you have not been adhering well to your drugs.” PWLHIV, 37 years old
“I prefer the one where I get my results immediately because it soothes your heart. The viral load test where you have to get the results on your next visit is not good because you are always worried about the results that you will be given. You always wonder what the health workers will tell you when the viral load is not suppressed. You are always looking at the phone to see if maybe a health worker will call you and when he/she calls, you still wonder what the health worker will tell you. Living in fear is not good at all. I would rather get my results immediately than wait.” PWLHIV, 28 years old
“[POC VL testing] makes me happy because I do not worry about that all the time… for the standard VL test, I could spend much time worried thinking: “I wonder what the results will be like? I wonder what the VL is?” and yet remember that the more you worry, the more your CD4 count lowers. Yet, for the quick test when you learn your results early, it makes you happy.” PWLHIV, 23 years old.
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Musanhu, C.C.C.; Takarinda, K.C.; Shea, J.; Chitsike, I.; Eley, B. Viral load testing among pregnant women living with HIV in Mutare district of Manicaland province, Zimbabwe. AIDS Res. Ther. 2022, 19, 52. [Google Scholar] [CrossRef]
- Myer, L.; Phillips, T.K.; McIntyre, J.A.; Hsiao, N.; Petro, G.; Zerbe, A.; Ramjith, J.; Bekker, L.; Abrams, E. HIV viraemia and mother-to-child transmission risk after antiretroviral therapy initiation in pregnancy in Cape Town, South Africa. HIV Med. 2017, 18, 80–88. [Google Scholar] [CrossRef] [PubMed]
- Sha, B.E.; Tierney, C.; Cohn, S.E.; Sun, X.; Coombs, R.W.; Frenkel, L.M.; Kalams, S.A.; Aweeka, F.T.; Bastow, B.; Bardeguez, A.; et al. Postpartum viral load rebound in HIV-1-infected women treated with highly active antiretroviral therapy: AIDS Clinical Trials Group Protocol A5150. HIV Clin. Trials 2011, 12, 9–23. [Google Scholar] [CrossRef]
- Yoo-Jeong, M.; Schnall, R. Accuracy of Self-Reports of HIV Viral Load Status and Risk Factors for Inaccurate Reporting of Viral Suppression Among Racial/Ethnic Minority Persons Living with HIV. AIDS Patient Care STDs 2020, 34, 369–372. [Google Scholar] [CrossRef] [PubMed]
- Roberts, T.; Cohn, J.; Bonner, K.; Hargreaves, S. Scale-up of Routine Viral Load Testing in Resource-Poor Settings: Current and Future Implementation Challenges. Clin. Infect. Dis. 2016, 62, 1043–1048. [Google Scholar] [CrossRef] [PubMed]
- Bailey, H.; Zash, R.; Rasi, V.; Thorne, C. HIV treatment in pregnancy. Lancet HIV 2018, 5, e457–e467. [Google Scholar] [CrossRef]
- UNAIDS. 2021 UNAIDS Global AIDS Update—Confronting Inequalities—Lessons for Pandemic Responses from 40 Years of AIDS. Available online: https://www.unaids.org/en/resources/documents/2021/2021-global-aids-update (accessed on 21 June 2023).
- UNAIDS. Global HIV & Statistics—Fact Sheet. Available online: https://www.unaids.org/en/resources/fact-sheet (accessed on 21 June 2023).
- Bulterys, M.A.; Mujugira, A.; Nakyanzi, A.; Wyatt, M.A.; Kamusiime, B.; Kasiita, V.; Kakoola, G.N.; Nalumansi, A.; Twesigye, C.; Pisarski, E.E.; et al. “Him Leaving Me—That is My Fear Now”: A Mixed Methods Analysis of Relationship Dissolution Between Ugandan Pregnant and Postpartum Women Living with HIV and Their Male Partners. AIDS Behav. 2023, 27, 1776–1792. [Google Scholar] [CrossRef]
- Bulterys, M.A.; Naughton, B.; Mujugira, A.; Mugisha, J.; Nakyanzi, A.; Naddunga, F.; Boyer, J.; Ware, N.; Celum, C.; Sharma, M. Pregnant women and male partner perspectives on secondary distribution of HIV self-testing kits: A qualitative study. PLoS ONE 2023, 18, e0279781. [Google Scholar] [CrossRef]
- Muhumuza, S.; Akello, E.; Kyomugisha-Nuwagaba, C.; Baryamutuma, R.; Sebuliba, I.; Lutalo, I.M.; Kansiime, E.; Kisaakye, L.N.; Kiragga, A.N.; King, R.; et al. Retention in care among HIV-infected pregnant and breastfeeding women on lifelong antiretroviral therapy in Uganda: A retrospective cohort study. PLoS ONE 2017, 22, e0187605. [Google Scholar] [CrossRef]
- Masereka, E.M.; Ngabirano, T.D.; Osingada, C.P.; Wiltshire, C.S.; Castelnuovo, B.; Kiragga, A.N. Increasing retention of HIV positive pregnant and breastfeeding mothers on option-b plus by upgrading and providing full time HIV services at a lower health facility in rural Uganda. BMC Public Health 2019, 19, 950. [Google Scholar] [CrossRef]
- Lecher, S.; Williams, J.; Fonjungo, P.N.; Kim, A.A.; Ellenberger, D.; Zhang, G.; Toure, C.A.; Agolory, S.; Appiah-Pippim, G.; Beard, S.; et al. Progress with Scale-Up of HIV Viral Load Monitoring—Seven Sub-Saharan African Countries, January 2015–June 2016. MMWR Morb. Mortal Wkly. Rep. 2016, 65, 1332–1335. [Google Scholar] [CrossRef]
- Drain, P.K.; Dorward, J.; Violette, L.R.; Quame-Amaglo, J.; Thomas, K.K.; Samsunder, N.; Ngobese, H.; Mlisana, K.; Moodley, P.; Donnell, D.; et al. Point-of-care HIV viral load testing combined with task shifting to improve treatment outcomes (STREAM): Findings from an open-label, non-inferiority, randomised controlled trial. Lancet HIV 2020, 7, e229–e237. [Google Scholar] [CrossRef]
- Qian, S.R.W.; Hassan, S.A.; Scallon, A.J.; Oyaro, P.; Brown, E.; Wagude, J.; Mukui, I.; Kinywa, E.; Oluoch, F.; Odhiambo, F.; et al. “After viral load testing, I get my results so I get to know which path my life is taking me”: Qualitative insights on routine centralized and point-of-care viral load testing in western Kenya from the Opt4Kids and Opt4Mamas studies. BMC Health Serv. Res. 2022, 22, 1540. [Google Scholar] [CrossRef]
- World Health Organization (WHO). Updated Recommendations on HIV Prevention, Infant Diagnosis, Antiretroviral Initiation and Monitoring [Internet]. Geneva: World Health Organization; 3 March 2021, Clinical Guidelines: Diagnostics and Treatment Monitoring. Available online: https://www.ncbi.nlm.nih.gov/books/NBK569324/ (accessed on 1 June 2023).
- Cepheid Innovation I. Xpert HIV-1 Viral Load piS. Cepheid Innovation; Cepheid Innovation: Stockholm, Sweden, 2015. [Google Scholar]
- Moyo, S.; Mohammed, T.; Wirth, K.E.; Prague, M.; Bennett, K.; Holme, M.P.; Mupfumi, L.; Sebogodi, P.; Moraka, N.O.; Boleo, C.; et al. Point-of-Care Cepheid Xpert HIV-1 Viral Load Test in Rural African Communities Is Feasible and Reliable. J. Clin. Microbiol. 2016, 54, 3050–3055. [Google Scholar] [CrossRef] [PubMed]
- Msimango, L.; Gibbs, A.; Shozi, H.; Ngobese, H.; Humphries, H.; Drain, P.K.; Garrett, N.; Dorward, J. Acceptability of point-of-care viral load testing to facilitate differentiated care: A qualitative assessment of people living with HIV and nurses in South Africa. BMC Health Serv. Res. 2020, 20, 1081. [Google Scholar] [CrossRef] [PubMed]
- Joseph, J.; Boeke, C.E.; Makadzange, E.E.; Sithole, K.; Maparo, T.; Mangwendeza, P.M.; Peter, T.; Sacks, J.A.; Simbi, R.; Khan, S.; et al. Near-point-of-care viral load testing during pregnancy and viremia at delivery. AIDS 2022, 36, 711–719. [Google Scholar] [CrossRef] [PubMed]
- E Boeke, C.; Joseph, J.; Atem, C.; Banda, C.; Coulibaly, K.D.; Doi, N.; Gunda, A.; Kandulu, J.; Kiernan, B.; Kingwara, L.; et al. Evaluation of near point-of-care viral load implementation in public health facilities across seven countries in sub-Saharan Africa. J. Int. AIDS Soc. 2021, 24, e25663. [Google Scholar] [CrossRef] [PubMed]
- Habiyambere, V.; Nguimfack, B.D.; Vojnov, L.; Ford, N.; Stover, J.; Hasek, L.; Maggiore, P.; Low-Beer, D.; Gonzàlez, M.P.; Edgil, D.; et al. Forecasting the global demand for HIV monitoring and diagnostic tests: A 2016–2021 analysis. PLoS ONE 2018, 13, e0201341. [Google Scholar] [CrossRef] [PubMed]
- Ganesh, P.; Heller, T.; Chione, B.; Gumulira, J.; Gugsa, S.; Khan, S.; McGovern, S.; Nhlema, A.; Nkhoma, L.; Sacks, J.A.; et al. Near Point-of-Care HIV Viral Load: Targeted Testing at Large Facilities. J. Acquir. Immune Defic. Syndr. 2021, 86, 258–263. [Google Scholar] [CrossRef] [PubMed]
- Bulterys, M.A.; Oyaro, P.; Brown, E.; Yongo, N.; Karauki, E.; Wagude, J.; Kingwara, L.; Bowen, N.; Njogo, S.; Wagner, A.D.; et al. Costs of Point-of-Care Viral Load Testing for Adults and Children Living with HIV in Kenya. Diagnostics 2021, 11, 140. [Google Scholar] [CrossRef]
- Kufa, T.; Mazanderani, A.H.; Sherman, G.G.; Mukendi, A.; Murray, T.; Moyo, F.; Technau, K.; Carmona, S. Point-of-care HIV maternal viral load and early infant diagnosis testing around time of delivery at tertiary obstetric units in South Africa: A prospective study of coverage, results return and turn-around times. J. Int. AIDS Soc. 2020, 23, e25487. [Google Scholar] [CrossRef] [PubMed]
- Drain, P.K.; Dorward, J.; Bender, A.; Lillis, L.; Marinucci, F.; Sacks, J.; Bershteyn, A.; Boyle, D.S.; Posner, J.D.; Garrett, N. Point-of-Care HIV Viral Load Testing: An Essential Tool for a Sustainable Global HIV/AIDS Response. Clin. Microbiol. Rev. 2019, 32, e00097-18. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| Characteristic | POC VL, N = 77 | SOC VL, N = 74 | Overall, N = 151 |
|---|---|---|---|
| Employed | 38 (49%) | 34 (46%) | 72 (48%) |
| Education <7 years | 20 (26%) | 17 (23%) | 37 (25%) |
| Age (years) | 28.0 (25.0, 32.0) | 27.0 (24.0, 31.0) | 28.0 (24.0, 32.0) |
| Marital status | |||
| Married | 70 (91%) | 69 (93%) | 139 (92%) |
| Never married | 5 (6.5%) | 5 (6.8%) | 10 (6.6%) |
| Divorced/separated | 2 (2.6%) | 0 (0%) | 2 (1.3%) |
| Relationship is polygamous | 28 (36%) | 23 (31%) | 51 (34%) |
| Number of previous live births | |||
| None | 12 (20%) | 13 (25%) | 25 (23%) |
| 1–2 | 15 (25%) | 16 (31%) | 31 (28%) |
| 3+ | 32 (54%) | 23 (44%) | 55 (50%) |
| Knew she was living with HIV when she started this pregnancy | 55 (72%) | 57 (77%) | 112 (75%) |
| Time since HIV diagnosis (months) | |||
| ≤2 months | 12 (16%) | 13 (18%) | 25 (17%) |
| 3–24 months | 16 (22%) | 13 (18%) | 29 (20%) |
| 25+ months | 46 (62%) | 48 (65%) | 94 (64%) |
| On ART at enrollment | 75 (99%) | 72 (97%) | 147 (98%) |
| Number of days lapsed since last ART dose | |||
| 0 days (<24 h) | 45/75 (60%) | 41/73 (56%) | 86/148 (58%) |
| 1 day (24–48 h) | 30/75 (40%) | 30/73 (41%) | 60/148 (41%) |
| 2+ days | 0/75 (0%) | 2/73 (3%) | 2/148 (1%) |
| Undetectable viral load (<50 copies/mL) at enrollment | 59 (86%) | 56 (80%) | 115 (83%) |
| Disclosed HIV status to partner by enrollment | 35 (45%) | 25 (34%) | 60 (40%) |
| Characteristic | POC VL, N = 77 | SOC VL, N = 74 | Overall, N = 151 |
|---|---|---|---|
| Birth outcome of this pregnancy | |||
| Liveborn | 64 (91%) | 61 (95%) | 125 (93%) |
| Stillborn/neonatal death/abortion | 6 (8.6%) | 3 (4.7%) | 9 (6.7%) |
| Mode of delivery | |||
| Vaginal birth | 68 (92%) | 55 (85%) | 123 (88%) |
| Planned c-section | 2 (2.7%) | 5 (7.7%) | 7 (5.0%) |
| Emergency c-section | 4 (5.4%) | 5 (7.7%) | 9 (6.5%) |
| Had separated with partner by postpartum visit | 4 (5.9%) | 8 (12%) | 12 (9.1%) |
| On ART at postpartum visit | 75 (99%) | 72 (97%) | 147 (98%) |
| Self-reported ART adherence at visit 3 months postpartum | |||
| Excellent | 40 (60%) | 47 (73%) | 87 (66%) |
| Good/very good | 24 (36%) | 16 (25%) | 40 (31%) |
| Fair/poor | 3 (4.5%) | 1 (1.6%) | 4 (3.1%) |
| Undetectable viral load (≤50 copies) at postpartum visit among participants with follow-up viral load data (n = 74) | 38/43 (88%) | 25/31 (81%) | 63/74 (85%) |
| POC VL results at the time of delivery (a subset of the POC VL arm only) (n = 29) | |||
| Undetectable viral load (≤50 copies) at delivery for mothers | 28/29 (96.6%) | - | - |
| Infant tested HIV negative at delivery | 29/29 (100%) | - | - |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nakyanzi, A.; Naddunga, F.; Bulterys, M.A.; Mujugira, A.; Wyatt, M.A.; Kamusiime, B.; Nalumansi, A.; Kasiita, V.; Peacock, S.; Celum, C.L.; et al. “It Soothes Your Heart”: A Multimethod Study Exploring Acceptability of Point-of-Care Viral Load Testing among Ugandan Pregnant and Postpartum Women Living with HIV. Diagnostics 2024, 14, 72. https://doi.org/10.3390/diagnostics14010072
Nakyanzi A, Naddunga F, Bulterys MA, Mujugira A, Wyatt MA, Kamusiime B, Nalumansi A, Kasiita V, Peacock S, Celum CL, et al. “It Soothes Your Heart”: A Multimethod Study Exploring Acceptability of Point-of-Care Viral Load Testing among Ugandan Pregnant and Postpartum Women Living with HIV. Diagnostics. 2024; 14(1):72. https://doi.org/10.3390/diagnostics14010072
Chicago/Turabian StyleNakyanzi, Agnes, Faith Naddunga, Michelle A. Bulterys, Andrew Mujugira, Monique A. Wyatt, Brenda Kamusiime, Alisaati Nalumansi, Vicent Kasiita, Sue Peacock, Connie L. Celum, and et al. 2024. "“It Soothes Your Heart”: A Multimethod Study Exploring Acceptability of Point-of-Care Viral Load Testing among Ugandan Pregnant and Postpartum Women Living with HIV" Diagnostics 14, no. 1: 72. https://doi.org/10.3390/diagnostics14010072
APA StyleNakyanzi, A., Naddunga, F., Bulterys, M. A., Mujugira, A., Wyatt, M. A., Kamusiime, B., Nalumansi, A., Kasiita, V., Peacock, S., Celum, C. L., & Ware, N. C. (2024). “It Soothes Your Heart”: A Multimethod Study Exploring Acceptability of Point-of-Care Viral Load Testing among Ugandan Pregnant and Postpartum Women Living with HIV. Diagnostics, 14(1), 72. https://doi.org/10.3390/diagnostics14010072